

Abstract
Aims
This study examines gender differences in the pathway from childhood sexual abuse (CSA) to adult binge drinking.
Methods
Using longitudinal data on 313 males and females (31–41 years old, mean = 36.21) in the Lehigh Longitudinal Study, we test for gender differences in the pathway from CSA to adolescent drinking, norms and pro-alcohol peers, to adult binge drinking.
Results
Controlling for family history of alcohol problems, socioeconomic status (SES) and ethnicity, we found that for females there was a significant direct effect of CSA on adult binge drinking. For males there was no significant direct or indirect effect. Significant effects of family alcohol problems and SES were also moderated by gender.
Conclusion
There are gender differences in the impact of CSA on adult binge drinking. Service providers and program developers should pay special attention to the possibility that their female clients may have a history of sexual abuse which could have implications for the course of prevention and treatment services related to binge drinking. Early intervention could prevent alcohol-related risk in adolescence which in turn could reduce, but not eliminate, the binge drinking consequences of CSA for females.
INTRODUCTION
The misuse of alcohol, particularly patterns of excessive drinking, is a leading cause of preventable death in the USA for adults (Naimi et al., 2003a) and adolescents (Miller et al., 2007). Binge drinking, consuming a large volume of alcohol in a single episode, is linked to a variety of negative health outcomes, including violence and the transmission of sexual infections (Naimi et al., 2010). Although binge drinking is related to alcohol use disorder (AUD; American Psychatric Association, 2013), most people (73%) who report binge drinking are light to moderate drinkers (Naimi et al., 2003a), which suggests that binge drinking is a distinct form of alcohol use that may have a different etiology than AUD. It is estimated that 25 million men and 13 million women (17% of adults) in the USA report binge drinking in the past month, with most reporting binge drinking on more than one occasion (U.S. Department of Health and Human Services Office of Disease Prevention and Health Promotion, 2010). Men are twice as likely as women to report binge drinking (Centers for Disease Control and Prevention, 2012). However, women who binge drink face a higher incidence than men of rape, sexual assault and domestic violence (Naimi et al., 2003b). The gender differences in both the prevalence and consequences of binge drinking raise questions about underlying risk mechanisms and the degree to which its etiology is similar for males and females. Understanding gender differences in the risk factors for binge drinking as well as differences in developmental mechanisms that contribute to adult binge drinking could improve prevention efficacy and treatment success for binge drinking.
Childhood sexual abuse (CSA) has been identified as a risk factor for alcohol problems in adolescence (Shin et al., 2009; Tonmyr et al., 2010) and adulthood, and there is some evidence of a stronger risk effect for women compared to men. Bensley et al. (2000) found that gender moderated the effect of physical and sexual abuse on heavy drinking in adults. In this cross-sectional study, adult heavy drinking was defined as four or more binging events (five or more drinks on a single occasion) within the past month. For women, the combination of sexual and physical abuse significantly increased the odds of heavy drinking by over six times but was not a risk factor for men. Widom et al. (2007) examined the association between childhood maltreatment (a combination of substantiated cases of physical, emotional, or sexual abuse or neglect) and patterns of excessive adult drinking (a latent construct of the frequency and quantity of alcohol use). They found that child maltreatment significantly predicted adolescent alcohol abuse or dependence which in turn predicted adult excessive drinking at age 29 among women but not men.
Several gaps remain in the literature on adult binge drinking as an outcome of CSA. With few exceptions (Champion et al., 2004; Howard and Wang, 2005; Behnken et al., 2010), most studies have not distinguished sexual abuse from other forms of abuse, which limits our understanding of the distinct consequences of CSA. Furthermore, little attention has been given to the wide range of adolescent alcohol-related factors that may serve as mediating variables in the development of adult binge drinking as a consequence of CSA. Peer drinking behavior and alcohol norms have been found to be significant risk factors for alcohol use in adolescents (Marshal and Chassin, 2000) and in the transition to adulthood (Lee et al., 2014). Tonmyr et al. (2010) found that peer substance use was a key influencer of alcohol use trajectories.
The current investigation uses data from an extended longitudinal study to examine the association between CSA and frequency of adult binge drinking (mean age 36). Analyses test adolescent alcohol-related experiences (one's own and peers) as mediating variables to help establish the developmental pathway through which CSA may increase the risk for adult binge drinking. We hypothesize that CSA is a more salient risk factor for adult binge drinking for females than males, and that pro-alcohol peers and one's own drinking and alcohol norms during adolescence are developmental pathways from CSA to adult binge drinking. We model these relationships and test for gender differences while controlling for family alcohol problems, childhood socioeconomic status (SES) and racial minority status.
MATERIALS AND METHODS
Sample
Data are from the Lehigh Longitudinal Study, a prospective study of the causes and consequences of child maltreatment, which began in the 1970s with a sample of 457 children and their families (Herrenkohl et al., 2013). The sampling was originally designed to compare families with child welfare referrals to families without officially documented cases of abuse and neglect. To this end some of the families were selected into the study from child welfare agency caseloads. Others were selected from several group settings (Head Start, day care and nursery programs) in the same two-county area. The first ‘preschool’ wave of the study took place in 1976–1977 when children were 18 months to 6 years old. A second ‘school-age’ assessment was conducted in 1980–1982. In 1990–1992, a third ‘adolescent’ assessment was conducted (mean age 18). The ‘adult’ survey was collected in 2008–2010 (n = 357, 80% of those living) when participants were in their mid-30s.
The original child sample was gender balanced (54% males) and the racial and ethnic composition was homogeneous and consistent with the makeup of the area (80.7% White). Just over 7% (n = 33) self-identified as Hispanic or Latino. For a small percentage, 1.3% (n = 6), the ethnicity of the child was unknown. Most children were from two-parent households (86%). There were 142 families with more than one child in the study. Of these, 128 families had 2 children and 18 families had 3 or more children. Intraclass correlations for variables of interest indicated coefficients were generally similar and unaffected by clustering of children within families.
Of the 357 cases with adult data, 44 were excluded from the analysis due to missing data on one of the variables. With these exclusions, the sample remains gender balanced (53.7% male), and ∼20% of those represented in the analysis belong to a minority ethnic group. An analysis of the retained and full samples indicates no significant differences in gender, age, minority ethnicity or childhood SES, although more of the child welfare abuse group was lost to attrition (43% compared to about 20% in the child welfare neglect group and 20% in the nonreferred comparison group). See Table 1.
Table 1.
Descriptive statistics for total sample and by gender with test of gender differences
| Variable n |
Full sample 313 |
Males 168 |
Females 145 |
χ2 | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Minority | 64 | 20.4 | 29 | 17.3 | 35 | 24.1 | 2.26 (1), P = 0.16 |
| Child welfare referred | 150 | 47.9 | 84 | 50.0 | 66 | 45.5 | 0.63 (1), P = 0.50 |
| Childhood sexual abuse | 126 | 40.3 | 46 | 27.4 | 80 | 55.2 | 24.99 (1), P = 0.00 |
| Family alcohol problems | 108 | 34.5 | 64 | 38.1 | 44 | 30.3 | 2.07 (1), P = 0.16 |
| Mean | SD | Mean | SD | Mean | SD | t-value | |
| Childhood SES | 0.31 | 3.39 | 0.32 | 3.52 | 0.29 | 3.25 | −0.07 (311), P = 0.95 |
| Adolescent | |||||||
| Number of friends get drunk | 3.53 | 1.34 | 3.68 | 1.35 | 3.36 | 1.31 | −2.01 (279), P = 0.05 |
| Number of friends sell alcohol | 2.97 | 1.43 | 3.11 | 1.42 | 2.79 | 1.44 | −1.85 (279), P = 0.07 |
| Friends approve of my drinking | 3.20 | 1.19 | 3.34 | 1.16 | 3.03 | 1.20 | −2.18 (277), P = 0.03 |
| Number of friends use alcohol | 3.67 | 1.29 | 3.85 | 1.27 | 3.45 | 1.28 | −2.61 (279), P = 0.01 |
| 30-day frequency of drinking | 4.27 | 2.55 | 4.61 | 2.72 | 3.87 | 2.30 | −2.57 (311), P = 0.01 |
| OK for me to get drunk | 3.13 | 1.33 | 3.23 | 1.31 | 3.02 | 1.34 | −1.41 (311), P = 0.16 |
| OK for me to sell alcohol | 2.25 | 1.33 | 2.42 | 1.33 | 2.06 | 1.31 | −2.37 (311), P = 0.02 |
| Low discomfort with getting drunk | 3.49 | 1.42 | 3.61 | 1.35 | 3.34 | 1.49 | −1.67 (311), P = 0.10 |
| Adult | |||||||
| Frequency of binge drinking | 1.30 | 1.67 | 1.72 | 1.79 | 0.80 | 1.35 | −4.55 (252), P = 0.00 |
| Age | 36.21 | 2.12 | 36.08 | 2.06 | 36.36 | 2.17 | 1.15 (311), P = 0.25 |
Significant gender differences are highlighted with bold text.
Measures
Sexual abuse
Questions regarding child sexual abuse were not included in the preschool or school-age assessments. Two relevant questions were asked of youth participants in the adolescent assessment: ‘How many times has someone pressured or pushed you to do sexual things you didn't want to do?’ and ‘How many times have you been sexually attacked or raped or an attempt made to do so?’ In addition, some adolescents were asked directly whether they had been sexually abused. CSA was also documented in interview notes, case records and adult retrospective reports. In the adult assessment, participants indicated whether (a) they had ever been raped, and (b) they had ever been sexually assaulted. Definitions of rape and sexual assault were included in the questions. Follow-up questions asked, ‘How old were you when this happened the first time?’ In total, 126 people were coded as having experienced sexual abuse before the age of 18 based on one or more of these sources. Nine cases were included based only on a positive response to one of the adult interview questions and providing an age younger than 18 years for the first occurrence. Ten cases were reported at the adolescent interview, but the respondent was over 18 and no follow-up question about age was asked. The remaining 107 positive cases were identified before or during the adolescent interview when the participant was under 18. Women were more likely than men to report sexual abuse (55.2 vs. 30.3%, respectively).
Substantiated childhood maltreatment
A variable was included in the analyses to account for the over sampling of child welfare involved families, coded 1 if referred through child welfare and 0 if not. Participants from the referred group were more likely to report sexual abuse than those in the comparison group (50.7 vs. 30.6%, respectively).
Adolescent alcohol use and norms
Adolescent alcohol use behavior and pro-alcohol norms were modeled as a latent variable using four measured indicators from the interview conducted in adolescence: (a) In the last year how many times have you used alcohol (1 = never to 8 = 100 or more)? (b) How wrong do you think it is to get drunk once in a while (1 = very wrong to 5 = not wrong at all)? (c) How wrong do you think it is to give or sell alcohol to someone under 21 (1 = very wrong to 5 = not wrong at all)? (d) How much personal discomfort would you experience if you got drunk once in a while (1 = a great deal to 5 = very little)?
Peer alcohol norms and behavior
Peer alcohol norms and behavior were also modeled as a latent variable using four indicators of peer behavior. These questions about peers were asked of the respondent during the adolescent interview: (a) In the last year how many of your close friends used alcohol (1 = none of them to 5 = all of them)? (b) In the last year how many of your close friends got drunk once in a while (1 = none of them to 5 = all of them)? (c) In the last year how many of your close friends gave or sold alcohol to someone under 21 (1 = none of them to 5 = all of them)? (d) How would your close friends react if you used alcohol (1 = strongly disapprove to 5 = strongly approve)?
Binge drinking behavior in adulthood
The adult survey included one item on binge drinking: ‘In the past year, how many times did you have 5+ drinks in one sitting?’ The responses ranged from 0 to more than 365 and were coded into seven ordinal categories: 0 = no binge drinking in past year, 1 = 1–5 times, 2 = 6–11 times, 3 = 12–29 times, 4 = 30–44 times, 5 = 45–69 times, and 6 = 70+ times in the past year.
Covariates
Socioeconomic status
SES is based on mother's educational level, occupation, total rooms in the family home, and family income at the preschool assessment that was then standardized, resulting in a score with M = 0 and SD = 3.2. About 60% of the sample would be considered poor according to the income-to-needs ratio and poverty threshold in 1976 (http://www.census.gov/hhes/www/poverty/data/threshld/thresh76.html).
Race/ethnicity
Racial minority status was coded 1 (minority) or 0 (nonminority) based on parent report at the preschool assessment.
Family alcohol use
Teens were asked in the adolescent assessment, ‘In the last 2 years have you experienced a family member who drinks too much alcohol?’ Responses were coded 0 (no) and 1 (yes).
Analyses
A confirmatory factor analysis (CFA) was conducted to determine the adequacy of factor loadings and model fit for the two latent constructs together (adolescent alcohol use and norms, and peer behavior and norms) using Mplus version 7 (Muthén and Muthén, 2013). Several fit indices were considered to determine the goodness of fit of the model (Hu and Bentler, 1999). Recommendations for cutoffs on goodness of fit include the following: RMSEA ≤ 0.06, CFI ≥ 0.95 and TLI ≥ 0.95; and adequate fit: RMSEA ≤ 0.08, CFI ≥ 0.90 and TLI ≥ 0.90. To determine if the measurements of the latent constructs were equivalent for males and females, a multiple-group CFA was conducted comparing a model where all factor loadings were allowed to estimate without restriction to a model where parameters were constrained to be equal for males and females. Log-likelihood tests (LRT) of difference were calculated based on comparison of model fit. Multi-group structural equation models (MGSEM) were used to examine gender differences in causal relationships between CSA and later alcohol behaviors, accounting for family alcohol problems, child ethnicity and childhood socioeconomic status.
RESULTS
Confirmatory factor analyses
Based on model fit and factor loadings, a four-indicator CFA was the most parsimonious for both adolescent alcohol use and norms and peer alcohol norms and behavior. For females, the model fit adequately (χ2(19) 38.678, P = 0.0049, RMSEA = 0.08, CFI = 0.97, TLI = 0.96) and all indicators loaded onto the appropriate latent constructs significantly (P < 0.000), ranging from 0.59 to 0.99. For males, the model also fit adequately (χ2(19) 43.088, P = 0.0013, RMSEA = 0.09, CFI = 0.97, TLI = 0.96) and all indicators loaded onto the appropriate latent constructs significantly (P < 0.000), ranging from 0.54 to 0.96. The LRT chi-square test indicated that the latent factor models did not differ significantly by gender (χ2(1) 1138, P > 0.05). Mean-levels of the latent constructs did not significantly differ by gender.
Structural models
We estimated a model which allowed path coefficients to vary across gender (χ2(122) 201.989, P < 0.000, RMSEA = 0.07, CFI = 0.94, TLI = 0.93), and compared it to a model in which paths were constrained to be equal for males and females (χ2(160) 482.928, P < 0.000, RMSEA = 0.11, CFI = 0.80, TLI = 0.77). The LRT test of difference found a chi-square value of χ2(6) = 905.248, P < 0.0001, indicating that constraining the paths reduced the fit of the model significantly. See Table 2 for unstandardized and standardized paths and significance tests.
Table 2.
Estimated standardized effects of background and mediating factors on frequency of adult binge drinking
| Variable | Adolescent alcohol |
Peer alcohol |
Frequency adult binge |
|||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Males |
Females |
Males |
Females |
Males |
Females |
|||||||||||||
| β | st. β | P | β | st. β | P | β | st. β | P | β | st. β | P | β | st. β | P | β | st. β | P | |
| SES | 0.12 | 0.27 | 0.00 | −0.04 | −0.07 | 0.41 | −0.00 | −0.01 | 0.92 | −0.03 | −0.08 | 0.41 | 0.04 | 0.08 | 0.45 | 0.002 | 0.01 | 0.95 |
| Minority | 0.20 | 0.05 | 0.51 | 0.31 | 0.09 | 0.29 | 0.09 | 0.03 | 0.78 | 0.07 | 0.02 | 0.77 | 0.44 | 0.09 | 0.31 | −0.27 | −0.08 | 0.36 |
| Child welfare | 0.45 | 0.14 | 0.10 | −0.32 | −0.10 | 0.27 | −0.48 | −0.19 | 0.04 | −0.36 | −0.14 | 0.14 | 0.25 | 0.07 | 0.54 | 0.28 | 0.10 | 0.37 |
| Family alcohol problems | 0.53 | 0.16 | 0.03 | −0.61 | −0.18 | 0.04 | 0.69 | 0.26 | 0.00 | 0.43 | 0.16 | 0.06 | 0.42 | 0.11 | 0.24 | 0.49 | 0.17 | 0.19 |
| Childhood sexual abuse | −0.10 | −0.03 | 0.71 | 0.01 | 0.004 | 0.96 | 0.33 | 0.12 | 0.12 | 0.51 | 0.20 | 0.03 | 0.12 | 0.03 | 0.74 | 0.44 | 0.16 | 0.03 |
| Adolescent alcohol | – | – | – | – | – | – | – | – | – | – | – | – | 0.47 | 0.42 | 0.01 | 0.44 | 0.51 | 0.00 |
| Peer alcohol | – | – | – | – | – | – | – | – | – | – | – | – | −0.42 | −0.30 | 0.07 | −0.14 | −0.13 | 0.37 |
Significant effects are highlighted with bold text.
For females, the model fit the data well (χ2(55) 77.855, P = 0.023, RMSEA = 0.05, CFI = 0.97, TLI = 0.95). Figure 1 illustrates the paths that were statistically significant for females. Results indicate that sexual abuse significantly predicted binge drinking behavior in adulthood (standardized β = 0.16, P < 0.05), even after controlling for SES, race, family influences, and adolescent alcohol use and norms and peer alcohol norms and behavior. Sexual abuse also predicted having peers with more pro-alcohol behaviors and norms (β = 0.20, P < 0.05). For females, having a family member with alcohol use problems negatively predicted their own alcohol use and norms in adolescence (β = −0.18, P < 0.05). Alcohol use and norms in adolescence were a strong predictor of binge drinking in adulthood (β = 0.50, P < 0.001). For females, the indirect effects of CSA on adult binge drinking through adolescent factors were marginally significant (β = 0.069, P = 0.068). The indirect effect of family alcohol use on adult binge drinking through peers was also marginally significant (β = 0.105, P = 0.068).
Fig. 1.
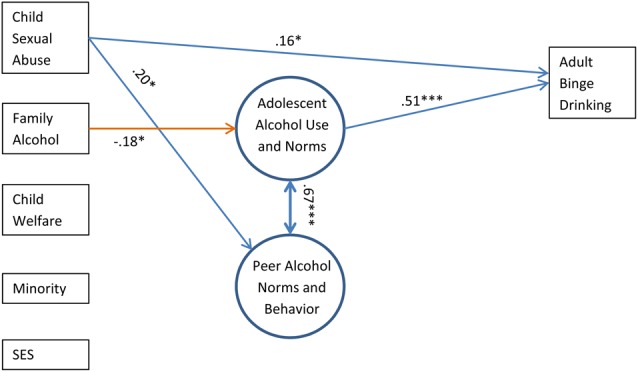
Females: Standardized path coefficients for model of CSA effects on alcohol-related behavior in adolescence and adulthood. *P < 0.05; **P < 0.01; ***P< 0.001.
For males, the model fit the data adequately (χ2(55) 106.215, P < 0.000, RMSEA = 0.07, CFI = 0.93, TLI = 0.90). Figure 2 illustrates the statistically significant paths for males (see Table 2 for path coefficients). Family alcohol use in childhood was a significant predictor of their own adolescent alcohol use and norms (β = 0.16, P < 0.05) and being involved with more pro-alcohol peers (β = 0.27, P < 0.001). Being in the referred group of the initial study was predictive of having peers with less alcohol use and pro-alcohol norms in adolescence (β = −0.19, P < 0.05). Alcohol use and beliefs in adolescence were a strong predictor of binge drinking in adulthood (β = 0.44, P < 0.01). The indirect pathway from family alcohol use through peer behavior to adolescent alcohol use was significant (β = 0.183, P < 0.001). The indirect effect of family alcohol use on adult binge drinking, through peer behavior and adolescent use, was also marginally significant (β = 0.077, P = 0.055). For males, unlike females, sexual abuse did not predict adolescent alcohol use and norms or peer alcohol norms and behavior directly or adult binge drinking directly or indirectly.
Fig. 2.

Males: Standardized path coefficients for model of CSA effects on alcohol-related behavior in adolescence and adulthood. *P < 0.05; **P < 0.01; ***P < 0.001.
DISCUSSION
This study focused on predictors and pathways from CSA to adult binge drinking through the potential developmental mechanisms of adolescent alcohol use, norms and pro-alcohol peers. We tested for gender moderation in these relationships based on previous research that suggested the link between CSA and adult binge drinking could be stronger for females than males, and that the pathway through adolescent alcohol-related factors may differ as well.
Consistent with our hypotheses, a direct relationship was confirmed from CSA to adult binge drinking for females, but not for males. The combination of a significant direct effect and trend level indirect effect for females suggests that female victims of CSA are particularly vulnerable to binge drinking well beyond the original abuse, and that these effects are not confined to the adolescent period.
Evidence suggests females are more likely to engage in self-harming behaviors as a result of early trauma, while males are more likely to engage in externalizing behaviors such as violence and delinquency (Herrenkohl et al., 2011). There is a small but growing body of literature that shows that problematic alcohol use is associated with more severe consequences for sexually abused women than for sexually abused men (i.e. Bensley et al., 2000; Widom et al., 2007). Thus, the use of excessive alcohol among sexually abused females may be further evidence of self-harm behavior.
Other gender differences were significant, although not always consistent with our hypotheses. Boys who had been child welfare referred for physical or emotional abuse or neglect were less likely to associate with pro-alcohol peers in adolescence, and were no more or less likely to engage in adolescent drinking or have pro-alcohol norms themselves, nor was there any direct effect on adult binge drinking. These results are not consistent with our hypothesis and previous research that found childhood physical abuse to positively predict later heavy drinking among men (Bensley et al., 2000).
An interesting finding was that for males, family alcohol problems positively predicted adolescent alcohol use and norms as expected, but for females this effect was in the opposite direction. Family alcohol use problems predicted lower adolescent drinking and norms among females. Our measure did not allow us to determine which family member or members had alcohol problems. It is possible that the girls in our sample were more likely to have a non-drinking parent than were the boys, and that a non-drinking parent's influence acted as a protective factor for girls, reducing their likelihood of using alcohol in adolescence (Marshal and Chassin, 2000). However, any protective effect did not extend to adult binge drinking.
Our measure of family alcohol problems is based on a single item reported by the teen during the adolescent interview. Unfortunately, this is the only indicator of family alcohol problems available in this study. The measure is limited to the teen's perception and their judgment of what constitutes a ‘problem’. Given the limitations of this measure we performed post hoc analyses omitting this variable and found no substantive differences in the results.
While we tested a model which stipulated that CSA leads to increased adolescent drinking and pro-alcohol norms and peer norms and drinking behavior, the directionality of these relationships is not guaranteed. It was possible for adolescent alcohol measures to be taken before any sexual abuse occurred. We deemed this unlikely because the preponderance of cases of sexual abuse was determined during or before the adolescent interview. Information about sexual abuse was gleaned from a variety of sources over the course of childhood and adolescence as well as responses to interview items in adulthood. Retrospective reporting has limitations (Widom and Morris, 1997). Research suggests females are more consistent across time in reporting lifetime sexual abuse compared to males (Okeke, 2014). However, the underreporting of sexual abuse to official agencies makes the use of official records alone problematic, and some evidence suggests that fears of reporter bias may be overstated (Fergusson et al., 2011). If females are more likely to report consistently, and consistency indicates a higher likelihood of accuracy, direct effects of CSA on adult binge drinking for females could reflect a stronger link for those with more accurate reporting rather than a real gender difference. Furthermore, we did not include certain details about CSA, such as the relationship to the perpetrator, penetration and co-occurring violence (Walsh et al., 2010). Gender differences in these factors (Molnar et al., 2001; Maikovich-Fong and Jaffee, 2010) could contribute to gender differences in the long-term outcomes of CSA (Hornor, 2010).
More cases were lost to attrition among the children referred for physical or emotional abuse. It could be that those cases were more likely to include sexual abuse than those retained, thus reducing our access to the full variety of CSA cases in the original sample. However, prospective data on maltreatment and alcohol behaviors and attitudes from childhood into adulthood are rare. This study was able to partially distinguish the experience of sexual abuse from other forms of maltreatment and neglect by controlling for substantiated reports of physical or emotional abuse and neglect at the beginning of the study. Although this variable may not capture all incidences of maltreatment (some of which occurred in the comparison sample), it is a strong indicator of other serious forms of early maltreatment and increases our confidence in our results.
Originally defined as the consumption of five or more drinks in a row (Miller et al., 2007), the definition of binge drinking was amended such that four or more drinks are considered binge drinking for women (National Institute on Alcohol Abuse and Alcoholism). A limitation of the current study is the measure of 5+ drinks for both males and females. The higher cutoff of 5+ drinks is likely to miss a subset of women who binge drink at slightly lower levels than those identified in this study.
We note the strong cross-sectional relationship between participants' reports of adolescent alcohol use and norms and their reports of peers' pro-alcohol norms and behaviors. Although the direction of the influence is impossible to disentangle in this study, theory and research indicate that peers have a strong influence over behavior during adolescence. A teen's behavior is influenced by peers, but it is one's own behavior (rather than peers' behavior) that predicts the frequency of one's own binge drinking more than two decades later. It is also entirely possible, and is also consistent with our findings, that the teen's own alcohol use and attitudes exert a strong impact on their report of their peers' drinking behavior and norms (If I drink, then I drink with my friends, and therefore my friends drink and obviously think it is a fine thing to do).
This study highlights that consequences of CSA can persist across developmental periods, which should be considered in intervention programming, especially for women. This finding suggests designing tailored interventions for women with sexual abuse experiences to include an alcohol/binge drinking prevention component. Brief interventions conducted by physicians have been found to be effective in significantly reducing the frequency of binge drinking (Fleming et al., 1997) and could be tailored to support initial screening of family dysfunction and experience of sexual abuse for adolescents and young adults. In addition, child welfare service providers who work with families who are often exposed to many risk factors explored in this study, such as child abuse, delinquent peers, and familial alcohol abuse, should utilize early screening for binge drinking among their clients (Tonmyr et al., 2010), even when there are no indications abuse or dependence.
FUNDING
This work was supported by the National Institute on Drug Abuse (R01DA032950) and the National Institute on Child Health and Human Development (RO1 HD049767), with co-funding from the Office of Behavioral and Social Sciences Research, all of the National Institutes of Health. The content of this paper is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
- American Psychatric Association. (2013) Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Association. [Google Scholar]
- Behnken MP, Le Y-CL, Temple JR et al. (2010) Forced sexual intercourse, suicidality, and binge drinking among adolescent girls. Addict Behav 35:507–9. doi: http://dx.doi.org/10.1016/j.addbeh.2009.12.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bensley LS, Van Eenwyk J, Simmons KW (2000) Self-reported childhood sexual and physical abuse and adult HIV-risk behaviors and heavy drinking. Am J Prev Med 18:151–8. doi: http://dx.doi.org/10.1016/S0749-3797(99)00084-7. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2012) Fact Sheets—Binge Drinking. Vitalsigns http://www.cdc.gov/alcohol/fact-sheets/binge-drinking.htm.
- Champion HLO, Foley KL, Durant RH et al. (2004) Adolescent sexual victimization, use of alcohol and other substances, and other health risk behaviors. J Adolesc Health 35:321–8. doi: http://dx.doi.org/10.1016/j.jadohealth.2003.09.023. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Horwood LJ, Boden JM (2011) Structural equation modeling of repeated retrospective reports of childhood maltreatment. Int J Methods Psychiatr Res 20:93–104. doi:10.1002/mpr.337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleming MF, Barry K, Manwell L et al. (1997) Brief physician advice for problem alcohol drinkers: a randomized controlled trial in community-based primary care practices. JAMA 277:1039–45. doi:10.1001/jama.1997.03540370029032. [PubMed] [Google Scholar]
- Herrenkohl TI, Aisenberg E, Williams JH et al. (2011) Violence in Context: Current Evidence on Risk, Protection, and Prevention. New York: Oxford University Press. [Google Scholar]
- Herrenkohl TI, Hong S, Klika JB et al. (2013) Developmental impacts of child abuse and neglect related to adult mental health, substance use, and physical health. J Fam Violence 28:191–9. doi:10.1007/s10896-012-9474-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hornor G. (2010) Child sexual abuse: consequences and implications. J Pediatr Health Care 24:358–64. doi: http://dx.doi.org/10.1016/j.pedhc.2009.07.003. [DOI] [PubMed] [Google Scholar]
- Howard DE, Wang MQ (2005) Psychosocial correlates of U.S. adolescents who report a history of forced sexual intercourse. J Adolesc Health 36:372–9. doi: http://dx.doi.org/10.1016/j.jadohealth.2004.07.007. [DOI] [PubMed] [Google Scholar]
- Hu LT, Bentler PM (1999) Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling 6:1–55. [Google Scholar]
- Lee JO, Hill KG, Guttmannova K et al. (2014) Childhood and adolescent predictors of heavy episodic drinking and alcohol use disorder at ages 21 and 33: a domain-specific cumulative risk model. J Stud Alcohol Drugs 75:684–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maikovich-Fong AK, Jaffee SR (2010) Sex differences in childhood sexual abuse characteristics and victims’ emotional and behavioral problems: findings from a national sample. Child Abuse Negl 34:429–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Chassin L (2000) Peer influence on adolescent alcohol use: the moderating role of parental support and discipline. Appl Dev Sci 4:80–8. doi:10.1207/S1532480XADS0402_3. [Google Scholar]
- Miller JW, Naimi TS, Brewer RD et al. (2007) Binge drinking and associated health risk behaviors among high school students. Pediatrics 119:76–85. doi:10.1542/peds.2006-1517. [DOI] [PubMed] [Google Scholar]
- Molnar BE, Buka SL, Kessler RC (2001) Child sexual abuse and subsequent psychopathology: results from the National Comorbidity Survey. Am J Public Health 91:753–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO (2013) Mplus User's Guide. Los Angeles: Muthen & Muthen. [Google Scholar]
- Naimi TS, Brewer RD, Mokdad A et al. (2003a) Binge drinking among US adults. JAMA 289:70–5. doi:10.1001/jama.289.1.70. [DOI] [PubMed] [Google Scholar]
- Naimi TS, Lipscomb LE, Brewer RD et al. (2003b) Binge drinking in the preconception period and the risk of unintended pregnancy: implications for women and their children. Pediatrics 111(Supplement 1):1136–41. [PubMed] [Google Scholar]
- Naimi TS, Nelson DE, Brewer RD (2010) The intensity of binge alcohol consumption among U.S. adults. Am J Prev Med 38:201–7. doi: http://dx.doi.org/10.1016/j.amepre.2009.09.039. [DOI] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism. Drinking levels defined. http://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking.
- Okeke NL. (2014) Sexual abuse and the life course: an analysis of factors linking child sexual abuse to adult sexual revictimization and perpetration. http://digitalcommons.library.tmc.edu/dissertations/AAI3689785.
- Shin SH, Edwards EM, Heeren T (2009) Child abuse and neglect: relations to adolescent binge drinking in the national longitudinal study of Adolescent Health (AddHealth) Study. Addict Behav 34:277–80. doi: http://dx.doi.org/10.1016/j.addbeh.2008.10.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tonmyr L, Thornton T, Draca J et al. (2010) A review of childhood maltreatment and adolescent substance use relationship. Curr Psychiatry Rev 6:223–34. [Google Scholar]
- U.S. Department of Health and Human Services Office of Disease Prevention and Health Promotion. (2010, December 2). Healthy People 2020—Improving the Health of Americans. http://www.healthypeople.gov/2020 (1 June 2012, date last accessed).
- Walsh K, Fortier MA, DiLillo D (2010) Adult coping with childhood sexual abuse: a theoretical and empirical review. Aggress Violent Behav 15:1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Widom CS, Morris S (1997) Accuracy of adult recollections of childhood victimization, Part 2: childhood sexual abuse. Psychol Assess 9:34–46. doi:10.1037/1040-3590.9.1.34. [Google Scholar]
- Widom CS, White HR, Czaja SJ (2007) Long-term effects of child abuse and neglect on alcohol use and excessive drinking in middle adulthood. J Stud Alcohol Drugs 68:317–26. [DOI] [PubMed] [Google Scholar]