

Abstract
[Purpose] To investigate the relationships between toe flexor muscle strength with (TFS-5-toes) and without (TFS-4-toes) the contribution of the great toe, anatomical and physiological muscle cross-sectional areas (CSA) of intrinsic toe flexor muscle and physical performance were measured. [Subjects] Seventeen men (82% sports-active) and 17 women (47% sports-active), aged 20 to 35 years, volunteered. [Methods] Anatomical CSA was measured in two intrinsic toe flexor muscles (flexor digitorum brevis [FDB] and abductor hallucis) by ultrasound. Muscle volume and muscle length of the FDB were also estimated, and physiological CSA was calculated. [Results] Both TFS-5-toes and TFS-4-toes correlated positively with walking speed in men (r=0.584 and r=0.553, respectively) and women (r=0.748 and r=0.533, respectively). Physiological CSA of the FDB was significantly correlated with TFS-5-toes (r=0.748) and TFS-4-toes (r=0.573) in women. In men, physiological CSA of the FDB correlated positively with TFS-4-toes (r=0.536), but not with TFS-5-toes (r=0.333). [Conclusion] Our results indicate that physiological CSA of the FDB is moderately associated with TFS-4-toes while toe flexor strength correlates with walking performance.
Key words: Toe grasping, Physiological CSA, Walking speed
INTRODUCTION
Muscle morphological characteristics, such as anatomical muscle cross-sectional area (CSA), muscle length, and muscle volume (MV) are important physiological variables for assessing the functional capacity of a muscle. Although magnetic resonance imaging (MRI) and computed tomography scans are the gold standard for measuring anatomical CSA and MV, ultrasound is a utilizable technique that can be easily applied to clinical assessment and field surveys1). In a small muscle, anatomical CSA and MV can be measured using multiple images of individual muscles created by portable ultrasound. One study2) investigated the validity and reliability of MV measurements of the medial gastrocnemius using three-dimensional ultrasound, and reported that ultrasound overestimated MV by approximately 2 mL (1.1%) and underestimated muscle length by 3 mm (1.3%) across all joint angles compared to MRI-measured values. In addition, the same study reported excellent reliability for repeated measures of MV (intrarater correlation coefficient (ICC) = 0.99) and muscle length (ICC = 0.97). These results suggest that multiple ultrasound images of a small muscle can accurately measure muscle morphological variables.
The foot is the point of direct contact between the body and ground surface during standing and walking. Muscle forces generated by the toes and ankles may play an important role in maintaining balance because muscle strength is essential for posture and stability3, 4). A few studies have reported that toe flexor muscle strength is associated with postural control. For example, Handa et al.5) reported significant positive correlations between toe flexor strength and one-leg standing balance with the eyes open (r = 0.443, p < 0.01) as well as functional reach (r = 0.620, p < 0.01), in an analysis grouping men and women together. Kurihara et al.6) examined the relationships between toe flexor muscle strength and intrinsic and extrinsic foot muscle sizes in young men and women and found significant correlations between toe flexor muscle strength and MRI-measured anatomical CSA in the medial parts (r = 0.775, p < 0.01) and lateral parts (r = 0.739, p < 0.01) of foot intrinsic muscles. Recently, Abe et al.7) reported a significant positive association between toe flexor muscle strength and accelerometer-determined light and moderate physical activities and average step counts. The results of these previous studies suggest that bigger intrinsic foot muscles in active individuals may be associated with greater toe flexor strength as well as good postural control. In a previous MRI study6), however, only one MRI image was used to determine the anatomical CSA of individual intrinsic foot muscles, even though the foot has several toe flexor muscles with differing distributions among the toes. Therefore, the purpose of this study was to test the hypothesis that toe flexor muscle strength is related to the anatomical and physiological CSA of intrinsic toe flexor muscles and that these morphological and functional variables associate with physical performance.
SUBJECTS AND METHODS
Thirty-four young adults aged 20 to 35 years (17 men and 17 women) were recruited through printed advertisements and by word of mouth. Before accepting their informed consent, a written description of the purpose and safety of the study was distributed to all of the potential subjects. All subjects were healthy and free of overt chronic disease (e.g., neuromuscular disorders, arthritic disorders, etc) as assessed by self-report. The rate of regular sports activity (at least twice a week), among the subjects was 65% (82% in men and 47% in women). The main types of sports activities were judo (29%), resistance exercise (21%), and soccer (21%) for men, and jogging/running (50%) and canoeing (25%) for women. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee for Human Experiments of the National Institute of Fitness and Sports in Kanoya, Japan.
Anatomical CSA was measured using B-mode ultrasound (Aloka Prosound α6, Tokyo, Japan) with a 7.5 MHz linear array transducer (76 mm wide) in two intrinsic toe flexor muscles, the flexor digitorum brevis (FDB) and abductor hallucis (AbH), as described previously8). All subjects lay in the prone position during scanning of the two muscles. Using anatomic landmarks described by Crofts et al.8), a linear transducer coated with water-soluble transmission gel was placed on the skin surface of the measurement sites, and cross sections of each muscle were imaged. Ultrasound images of each site were stored on a personal computer, and anatomical CSA was measured using Image-J software. The mean values (two images) of each site were used for data analysis. All ultrasound measurements were performed on the left (non-dominant) foot, and dominance was ascertained by asking each subject which foot they used to perform well-learned skills using a questionnaire9).
The muscle volume and muscle length of the FDB were estimated using multiple ultrasound images from the sole of the foot. After foot length (the distance between the tip of the great toe and the edge of the heel) measurements, all measurement sites were marked at 50% of the foot length as well as at contiguous 1-cm intervals from the point of 50% of the foot length in both the proximal and distal directions. Ultrasound images were obtained at each measurement site (Fig. 1) and the anatomical CSA of the FDB was measured using the procedure described above. Muscle volume was calculated by multiplying anatomical CSA by distance interval (1 cm). The distance between the most proximal image and the most distal image in which the FDB was visible was defined as the length of the FDB muscle. To calculate physiological CSA, the fiber length of the FDB was estimated using the ratio of fiber length to muscle length (average of the second, third, fourth toes) as reported by Kura et al10). The physiological CSA of the FDB was calculated by dividing muscle volume by fiber length. The test-retest reliability (ICC, SEM and minimal difference) was previously determined using the data of 7 young subjects (5 men and 2 women) scanned twice within 7 days (at least one day apart) for anatomical CSA of the FDB (0.924, 0.13 cm2, 0.36 cm2) and AbH (0.949, 0.21 cm2, 0.58 cm2) and muscle volume of FDB (0.971, 0.57 cm3, 1.57 cm3).
Fig. 1.
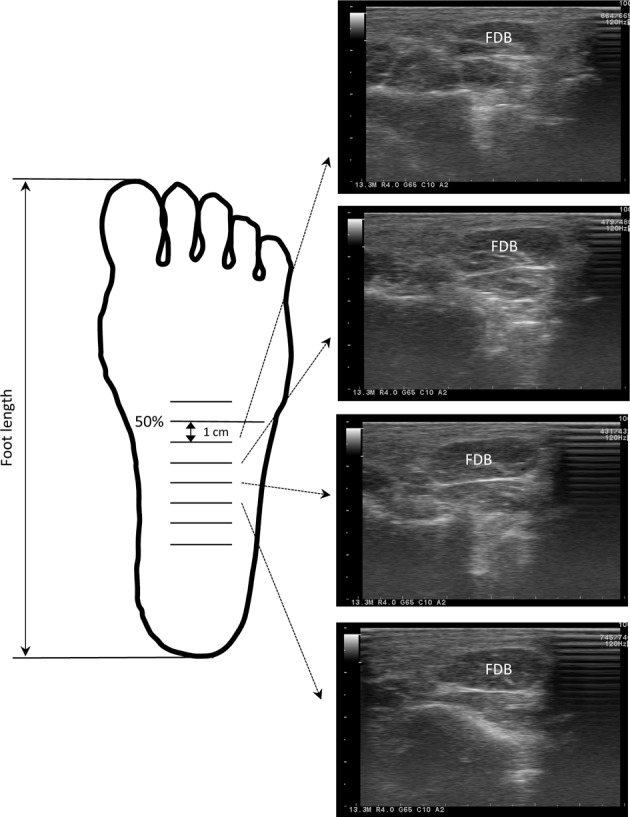
Before the start of ultrasound testing, foot length (the distance between the tip of the great toe and the edge of the heel) was measured and then all measurement sites were marked at 50% of the foot length as well as at contiguous 1-cm intervals from the point of 50% of the foot length in both the proximal and distal directions. Typical ultrasound images (young woman, 20 yr) revealing transverse scans of the foot at contiguous 1-cm intervals from the point of 50% of the foot length
FDB: flexor digitorum brevis
Toe flexor muscle strength (TFS) was measured using a toe-grasp dynamometer (TKK3361, Takei, Tokyo, Japan), as described previously11, 12). While barefoot, subjects stood in front of a wall and the left foot was placed on the dynamometer. Then the subjects were instructed to lift the right foot and maintain a one-legged upright standing position on the dynamometer, with both hands on the wall in front of them, while holding the dynamometer grasp bar with their toes. The distance between the bar and the heel was adjusted to the foot size of the subjects so that the distal phalanges of the great toe and fifth toe and the middle phalanges of the second to fifth toes could be placed on the toe grasp bar. Subjects were allowed to perform one test trial, followed by two maximum effort trials (TFS-5-toes), and the best value of the left foot was used for the data analysis. The subjects also performed two maximum effort trials to measure toe flexor muscle strength without the contribution of the great toe (TFS-4-toes). In these trials, a small metal plate was placed between the great toe and the toe grasp bar during these measurements for preventing the great toe from grasping the toe grasp bar of the dynamometer. Maximal toe flexor strength divided by body weight was calculated to evaluate the relative toe flexor strength. The test-retest reliability of toe flexor strength (TFS-5-toes and TFS-4-toes) measurements using the ICC, SEM and minimal difference was previously determined using the data of 7 young subjects (5 men and 2 women) tested twice within 7 days (at least one day apart): 0.962, 1.2 kg and 3.3 kg for TFS-5-toes and 0.883, 1.1 kg and 3.1 kg for TFS-4-toes.
Maximum walking speed was measured by timing each subject as they walked along a 10-meter corridor with a ceramic floor surface. The total length of the marked corridor was 14 meters, allowing 2-meter acceleration and deceleration zones. The width of the corridor was constricted to 1 meter to encourage subjects to maintain a straight course. Subjects used their own footwear and had to start 2 meters before the beginning of the start line, and to continue until the 2 meters past the goal line. After one practice trial, subjects performed two maximum speed timed trials. Subjects were asked to walk down the corridor as fast as possible without running. Times were measured with an electronic timing system (nearest 0.01 s, Brower Timing System, Draper, USA). The best time was converted to a maximum speed measurement (unit, m/s) and the best value was used as the maximum walking speed. The test-retest reliability of this measurement using the ICC, SEM and minimal difference was previously determined using the procedure described above: 0.930, 0.14 m/s and 0.38 m/s, respectively.
The functional reach test was measured using the method described in a previously reported study4). Before the start of the test, subjects were instructed to stand with both feet touching a marked line and to maintain that foot position throughout testing. The subject then performed shoulder forward flexion with the right shoulder until an angle of 90 degrees was reached. The right arm was kept straight during shoulder forward flexion. Next, the subjects tried to extend their middle finger as far forward as possible without moving their feet and keeping their arm parallel to the ground. The distance moved by the end of the middle finger between the starting position and maximum forward position was measured using a horizontal line marker4). Subjects performed two trials, and the best value was used for the functional reach test. The test-retest reliability of this measurement using the ICC, SEM and minimal difference was previously determined fusing the procedure described above: 0.889, 2 cm and 5 cm, respectively.
The results are expressed as the mean and standard deviation of all variables. Before comparisons were made, the distributions of the dependent variables were tested for normality using the Shapiro-Wilk test. The difference between men and women was tested for significance using the unpaired Student’s t-test, and when variables were not normally distributed, the Mann-Whitney U test was used. Pearson product correlations were performed to determine the relationships between toe flexor muscle strength and intrinsic toe flexor muscle size as measured by ultrasound and between the morphological and functional variables of toe flexor muscle and physical performance. Significance was accepted for values of p<0.05.
RESULTS
Age was similar between genders. Men were taller and heavier than women. Compared with women, men had higher anatomical CSA in the FDB and AbH, as well as muscle volume and physiological CSA of the FDB. Maximum TFS-5-toes and TFS-4-toes were higher in men than in women; however, the specific strength (TFS-4-toes per unit physiological CSA) of the FDB, walking speed and functional reach were similar for both men and women (Table 1).
Table 1. Maximum toe flexor muscle strength, physical performance and ultrasound measurements of intrinsic foot muscle sizes of young men and women.
| Men | Women | Overall | |
|---|---|---|---|
| (n=17) | (n=17) | (n=34) | |
| Age (yrs) | 24 (4) | 24 (4) | 24 (4) |
| Height (m) | 1.71 (0.05)* | 1.60 (0.05) | 1.66 (0.07) |
| Body mass (kg) | 72.9 (11.4)* | 52.1 (5.1) | 62.5 (13.6) |
| Body mass index (kg/m2) | 24.8 (3.1)* | 20.4 (2.0) | 22.6 (3.4) |
| Foot length (cm) | 25.2 (1.2)* | 22.6 (0.7) | 23.9 (1.6) |
| Flexor digitorum brevis | |||
| ACSA max (cm2) | 2.61 (0.38)* | 1.65 (0.33) | 2.13 (0.60) |
| MV (cm3) | 11.95 (2.93)* | 6.66 (2.10) | 9.31 (3.67) |
| PCSA (cm2) | 6.38 (1.04)* | 3.95 (0.97) | 5.17 (1.58) |
| Abductor hallucis | |||
| ACSA (cm2) | 2.89 (0.69)* | 2.02 (0.59) | 2.46 (0.77) |
| TFS-5 toes (kg) | 29.1 (5.3)* | 21.2 (4.7) | 25.1 (6.4) |
| TFS-4 toes (kg) | 10.4 (3.2)* | 6.4 (2.6) | 8.4 (3.5) |
| TFS-4 toes/PCSA (kg/cm2) | 1.63 (0.40) | 1.62 (0.56) | 1.63 (0.48) |
| Walking speed (m/s) | 3.19 (0.65) | 3.14 (0.66) | 3.17 (0.64) |
| Functional reach (cm) | 38.1 (6.3) | 39.1 (4.0) | 38.6 (5.2) |
Maximum toe flexor muscle strength with (TFS-5 toes) and without (TFS-4 toes) the contribution of the great toe; ACSA, anatomical cross-sectional area; MV, muscle volume; PCSA, physiological cross-sectional area. *Significant difference from women, p<0.001
There was a significant correlation between TFS-5-toes and TFS-4-toes of men (r = 0.739, p < 0.001) and women (r = 0.731, p < 0.001). Both TFS-5-toes and TFS-4-toes correlated positively with the maximum walking speed of men (r = 0.584, p = 0.014 and r = 0.553, p = 0.021, respectively), women (r = 0.748, p < 0.001 and r = 0.533, p = 0.028, respectively) and the whole sample (r = 0.535, p = 0.001 and r = 0.459, p = 0.006, respectively). However, the correlations between TFS-5-toes and functional reach of both men (r = −0.399) and women (r = 0.166) were not significant (p>0.05).
Anatomical CSA of the AbH did not significantly correlate with TFS-5-toes of either men (r = 0.034, p = 0.896) or women (r = 0.387, p = 0.125); however, the correlation of the whole sample was significant (r = 0.454, p = 0.006). For women, there were significant positive correlations between TFS-5-toes and anatomical CSA max (r = 0.713, p = 0.001), muscle volume (r = 0.604, p = 0.010), and physiological CSA (r = 0.687, p = 0.002) of the FDB. For men, however, the observed anatomical CSA max (r = 0.143, p = 0.584), muscle volume (r = 0.332, p = 0.192), and physiological CSA (r = 0.333, p = 0.191) of the FDB did not correlate significantly with TFS-5-toes. Physiological CSA of the FDB correlated positively with TFS-4-toes of men (r = 0.541, p = 0.025), women (r = 0.573, p = 0.016) and the whole sample (r = 0.720, p < 0.001) (Fig. 2).
Fig. 2.

Relationships between physiological cross-sectional area (CSA) in the flexor digitorum brevis (FDB) and toe flexor muscle strength (TFS-4 toes) of young men and women. TFS-4 toes: toe flexor muscle strength without the contribution of the great toe. Open circles are men and filled circles are women
DISCUSSION
The main findings of the present study were that physiological CSA of the FDB was significantly correlated with TFS-4-toes of both men and women; physiological CSA of the FDB was significantly correlated with TFS-5-toes of women, but not that of men; there was a significant correlation between toe flexor muscle strength and maximum walking speed in both genders.
In the present study, the FDB was selected as representative of the intrinsic toe flexor muscles, because a more accurate estimation of muscle volume by ultrasound and calculation of physiological CSA of the muscle can be achieved than of the other intrinsic toe flexor muscles. The FDB muscle volume reliability results (ICC of 0.971 and SEM of 0.57 cm3) indicate that the ultrasound method of the present study is a good repeatable technique for measuring muscle volume. The FDB is located in the sole of the foot and separates into four tendons that insert onto the middle phalanges of the four lateral toes10) (without the great toe). Therefore, our results demonstrate that the physiological CSA of the FDB is associated with TFS-4 toes of both men and women, even though the correlation was only moderate. Toe flexor muscle strength is generated from a combination of the intrinsic and extrinsic foot muscles. In the hand, the grip strength decreases by approximately 50% after median and ulnar nerve (intrinsic muscles) blocks compared with the pre-block measurement13). Accordingly, the contribution of extrinsic toe flexor muscles may reflect the moderate correlations between TFS-4 toes and physiological CSA of the FDB. In addition, individual differences in the moment arm (located between the center of curvature of the metatarsal head and the center of the flexor tendon) and/or differences in the dominant/non-dominant sides may also be unknown factors14).
Our findings show that the anatomical and physiological CSA of the FDB of women were significantly correlated with TFS-5 toes. For men, however, the correlation coefficients were not statistically significant. Only one study6) has examined the relationships between toe flexor muscle strength and intrinsic and extrinsic foot muscle sizes in young sedentary adults (14 men and 12 women) and a pooled sample was used for data analysis. That study reported significant correlations between TFS-5 toes and MRI-measured anatomical CSA of the medial parts (r=0.775, p<0.01) and lateral parts (r=0.739, p<0.01) of the foot intrinsic muscles, although only one MRI image was used in that investigation. In the present study, the reason for the lack of a significant correlation between TFS-5 toes and the FDB muscle size observed in men is unknown. The participants in the previous study6) were sedentary adults. Approximately half of our young women were sedentary and the other half performed mainly jogging/running or canoeing. Therefore, our women participants may have had relatively homogeneous morphological and functional properties of the toe flexor muscles, which might partially explain the significant correlations. On the other hand, most of our young men were physically active and performed different sports including judo, resistance exercise and/or soccer. A likely explanation is that physical activity in different sports may elicit non-homogeneous features among toe flexor muscles, especially between the great toe and the four other toes. Together, the results of the present and previous studies suggest that differences in sports experience may be a factor underlying the poor correlation of TFS-5-toes and FDB muscle size in young men. Additional research into these issues is needed.
In the present study, both TFS-4-toes and TFS-5-toes are positively associated with maximum walking speed in young men and women. This finding is consistent with the results of previous studies5, 15) which found significant correlations between 10-m walking performance and TFS-5-toes (r=−0.459, p<0.01)5) and improved 50-m dash time following 8 weeks of toe flexor strength training15). Thus, the results of the present and previous studies demonstrate that toe flexor muscle strength is an important factor determining maximum walking speed. On the other hand, no significant correlation of TFS-5-toes and functional reach of either young men or women was found. Although a pooled sample with a wide age range (20 to 84 yrs) was used, one study reported a significant positive correlation (r=0.620, p<0.01) between TFS-5-toes and functional reach5). The discrepancy in the results of the present and that previous study is not known, but the difference in subject age ranges between the two studies may have played a role.
In conclusion, although toe flexor muscle strength correlated positively with walking speed in both genders, its correlation with functional reach was not statistically significant. Physiological CSA of the FDB of women was correlated with toe flexor strength. For men, physiological CSA of the FDB correlated positively with only TFS-4-toes. The lack of a significant relationship between TFS-5-toes and physiological CSA of the FDB in men may be related to different experiences in sports.
Acknowledgments
The authors would like to thank the individuals who participated in this study. This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The authors have no conflicts of interest to declare.
REFERENCES
- 1.Abe T, Loenneke JP, Thiebaud RS, et al. : Morphological and functional relationships with ultrasound measured muscle thickenss of the upper extremeities and trunk. Ultrasound, 2014, 22: 229–235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Barber L, Barrett R, Lichtwark G: Validation of a freehand 3D ultrasound system for morphological measures of the medial gastrocnemius muscle. J Biomech, 2009, 42: 1313–1319. [DOI] [PubMed] [Google Scholar]
- 3.Horlings CG, van Engelen BG, Allum JH, et al. : A weak balance: the contribution of muscle weakness to postural instability and falls. Nat Clin Pract Neurol, 2008, 4: 504–515. [DOI] [PubMed] [Google Scholar]
- 4.Kobayashi R, Hosoda M, Minematsu A, et al. : Effects of toe grasp training for the aged on spontaneous postural sway. J Phys Ther Sci, 1999, 11: 31–34. [Google Scholar]
- 5.Handa S, Horiuchi K, Aoki K: A stueedy on the measurement of toes grasping strength and effect of standing posture control. Jpn J Ergon, 2004, 40: 139–147(in Japanese). [Google Scholar]
- 6.Kurihara T, Yamauchi J, Otsuka M, et al. : Maximum toe flexor muscle strength and quantitative analysis of human plantar intrinsic and extrinsic muscles by a magnetic resonance imaging technique. J Foot Ankle Res, 2014, 7: 26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abe T, Thiebaud RS, Loenneke JP, et al. : Association between toe grasping strength and accelerometer-determined physical activity in middle-aged and older women. J Phys Ther Sci, 2015, 27: 1893–1897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Crofts G, Angin S, Mickle KJ, et al. : Reliability of ultrasound for measurement of selected foot structures. Gait Posture, 2014, 39: 35–39. [DOI] [PubMed] [Google Scholar]
- 9.Chapman JP, Chapman LJ, Allen JJ: The measurement of foot preference. Neuropsychologia, 1987, 25: 579–584. [DOI] [PubMed] [Google Scholar]
- 10.Kura H, Luo ZP, Kitaoka HB, et al. : Quantitative analysis of the intrinsic muscles of the foot. Anat Rec, 1997, 249: 143–151. [DOI] [PubMed] [Google Scholar]
- 11.Abe T, Ogawa M, Thiebaud RS, et al. : Is muscle strength ratio a criterion for diagnosis of site-specific muscle loss? Geriatr Gerontol Int, 2014, 14: 837–844. [DOI] [PubMed] [Google Scholar]
- 12.Soma M, Murata S, Kai Y, et al. : An examination of limb position for measuring toe-grip strength. J Phys Ther Sci, 2014, 26: 1955–1957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kozin SH, Porter S, Clark P, et al. : The contribution of the intrinsic muscles to grip and pinch strength. J Hand Surg Am, 1999, 24: 64–72. [DOI] [PubMed] [Google Scholar]
- 14.Green SM, Briggs PJ: Flexion strength of the toes in the normal foot. An evaluation using magnetic resonance imaging. Foot, 2013, 23: 115–119. [DOI] [PubMed] [Google Scholar]
- 15.Hashimoto T, Sakuraba K: Strength training for the intrinsic flexor muscles of the foot: effects on muscle strength, the foot arch, and dynamic parameters before and after the training. J Phys Ther Sci, 2014, 26: 373–376. [DOI] [PMC free article] [PubMed] [Google Scholar]