

Highlights
-
•
This nail impalement injury to the brain was self-inflicted by a mentally challenged person who presented in a non-neurosurgical centre.
-
•
After clinical assessment and limited investigations, a burr hole adjoining the nail was made by the orthopaedic team to loosen the nail and to carry out a successful extraction.
-
•
The patient’s headache resolved swiftly and his limb weakness recovered fully by four months.
Keywords: Nail impalement, Injury, Brain, Non-neurosurgical centre
Abstract
A nail impalement injury to the brain usually results from accidents like falls or nail gun miss-fires or suicide attempts or from barbaric punishment for certain crimes which are rarely practiced in some remote areas. We present an unusual, intentional, self-impalement of a 4 in. nail into the brain in a mentally challenged young man. This case report describes the challenges encountered in the management of a patient with impaled nail in the brain in a non-neurosurgical centre.
1. Introduction
Nail impalement injury to the brain is a rare neurosurgical emergency. It commonly results from accidental fall into shrapnel. More commonly, miss-firing of a nail gun during construction works can impale a nail into the brain [1], [2]. Very rarely some suicide attempts have been carried out by firing nail guns into the brain. An intentional impalement of nail to the brain for attempted suicide has been reported in the literature in a mentally challenged person [3]. Bomb blasts can also drive a nail piece from improvised explosive devices into the brain causing varying damages. Except for the bomb blast, the prognosis for the majority of patients with nail impalement injuries to the brain is good, because they are mainly low velocity injuries. Surgical extraction can be done successfully, especially when the nail head is secured but blind removal is largely unacceptable because of the risk of secondary brain injury [4]. This case report illustrates the challenges encountered in the management of nail impalement injury to the brain in a non-neurosurgical centre and it shows that in a poor resource setting, an impaled nail in the brain can be removed successfully especially when the nail head is secured.
2. Case report
A 23 year old mentally challenged male presented in the A&E on 21st October, 2013 with a 10 day history of having hammered a 4 in. nail into his brain. It was difficult for his mother to convince him to come to the hospital. The patient complained of headache and weakness of the right upper limb. He had engaged in an episode of self-harm in the past by burning his wrist in a candle flame. He was not violent and he was not considered to be mad by his mother or by their neighbours, rather mother said he had learning disability from childhood. He had poor speech and short attention span. He did not see any clinician routinely and he was not on any drugs.
On examination, he was not pale and not febrile. His intellectual capacity was quite low and he can be categorized as a person with learning disabilities. Glasgow Coma Score was 15/15. A nail head was visualized on his scalp (Fig. 1) with sero-purulent discharge around it. There was no focal neurological deficit involving the facial nerve because the mouth was not deviated and there was no ptosis. Also eye movements were normal. There was no change in speech. Thus, the cortical signs were largely negative. However, he would not obey the command of out-stretching his upper limbs with the palms facing upward so that we could demonstrate pronator drift, which is seen in subtle neurological deficit. The power in the right upper limb was largely 3/5 using the Medical Research Council grading, with poor hand grip in comparison to the left. Basic investigations included full blood count which showed normal haemoglobin, normal platelet and elevated total white cell count. Wound swab was taken for microscopy, culture and sensitivity but unknown to the team, the laboratory abandoned the swab stick when payment was not made for the test. Skull X-ray showed a vertically oriented radio-opaque nail with the head slightly above the skull (Fig. 2, Fig. 3). Facilities for angiography, though available in our centre, was not affordable. Computerized tomography scan was not available in our centre, and the affordability was also a problem. The plan was to extract the nail surgically. An informed consent was obtained and under sedation and local anaesthetic infiltration, a 6 cm curved incision was made across the nail head to raise a scalp flap. A small burr hole was created adjoining the nail to widen the interphase between it and the skull. When this was done, the nail became loose and with a forceps, the nail head was held and pulled out very slowly and gently. The field was dry and the only bleeding was from the scalp wound. The nail was rusted already except for the head (Fig. 4). The edge of the skull at the point of penetration was curetted and the track was irrigated copiously but gently with normal saline from a 10 ml syringe. The opening in the skull was covered by advancing the pericranium over it, while the wound was debrided and partially closed. Postoperative care was administered. Broad spectrum antibiotics was administered for 10 days. He was also given prophylaxis for seizures. The patient recovered uneventfully, and he was discharged on the fifth postoperative day. He was sent to the out-patient department for dressing. The wound healed by the third week and the limb weakness recovered completely by the end of the fourth month. The patient was referred to a special school for people with learning disabilities. He was also seen by the psychiatrist during one of the check-visits who concluded he had learning disability.
Fig. 1.
A picture of the mentally challenged young man showing a visible nail head on his head.
Fig. 2.
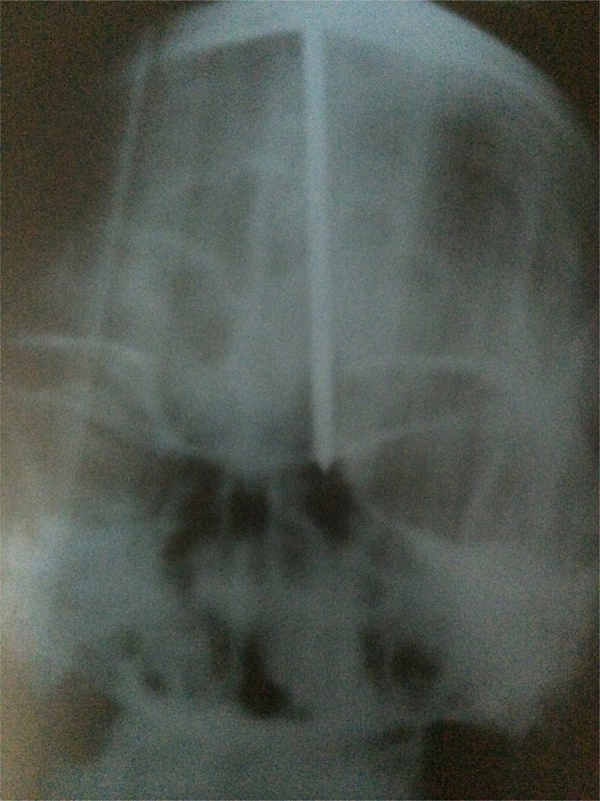
Antero-posterior plain radiograph of the skull showing impaled nail in the brain.
Fig. 3.
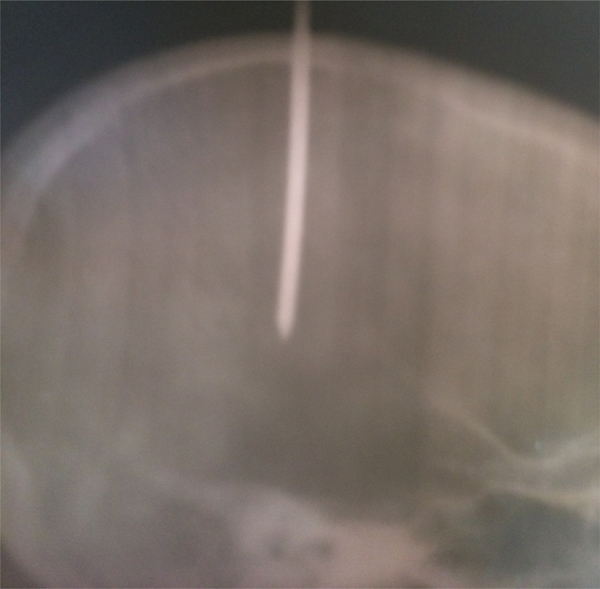
Lateral view of plain skull radiograph showing the impaled nail in the brain.
Fig. 4.

Showing a picture of the 4 in. impaled nail after extraction.
3. Discussion
Nail impalement injury to the brain is a rare neurosurgical emergency. It may occur as a result of construction site accidents and accidental falls into shrapnel or as a result of bomb blasts. Construction workers that use nail guns can sustain impalement injuries when the gun misfires, driving nails into the body [1], [2]. There are reports of intentional use of nail gun for attempted suicide [3]. This case is probably the first self-inflicted nail impalement injury to the brain by a mentally challenged person, reported in this environment. Following impalement injury to the brain, pre-hospital care involving the stabilization and the ‘securing of the object and preventing its movement to avoid further damage, is necessary. If the patient comes in as an emergency, resuscitation and proper assessment of any neurological deficit are important before any attempt to remove the impaled object [5]. In addition to nails, different types of objects like knives, crowbar, screw driver, scissors and spear have been reported impaled in the brain [4], [5].
During the pre-operative work up of the patient, a combined orthopaedic units’ review was carried out and some were of the opinion that the patient might bleed during the extraction that would need an experienced operator to navigate, and so the patient needs to be referred to a neurosurgical centre. This is based on the fact that penetrating objects could cause tamponade effect on the vessels, which prevents bleeding at the time of impalement but may bleed during the extraction. Though bleeding during the extraction was a possibility, some believe that it could still be handled by a careful extraction along the nail track. Also the nail was not entirely intracranial, and the visible nail head could be secured easily for a successful extraction. Some authors had also advised using this tamponade effect to advantage by delaying the extraction of impaled object so that stable clots will form around it, provided there is no active bleeding [6]. Our patient presented 10 days after the impalement and we took this into consideration as we planned the removal. As part of the preparation, a senior resident neurosurgeon in the only regional neurosurgical centre was contacted, and he wanted the patient referred. Also, he could not give any opinion on the patient without a physical clinical assessment. The patient could not be convinced yet again to go to another hospital and the mother also made it clear that they cannot afford to travel out of the state. Many reports allude to the fact that majority of impaled nail injuries to the brain result in minor neurological deficits [3], [7]. A nail was discovered to be lodged in the brain of a patient who had attempted suicide 12 years previously during an investigation for headache [3]. Impalements, whether self-inflicted or from nail gun miss-fires, are usually low velocity projectile injuries. They are not associated with cavitation, shock waves or diffuse axonal dysfunction. The injuries are limited locally along the nail track [8] and a major risk though rare, is the formation of pseudo-aneurysm [9], [10].
We decided to undertake the surgical extraction considering the challenges inherent in impalement injuries and peculiar challenges in the patient. During the operation, efforts were made to remain within the nail track and to avoid additional injury to the brain. Other immediate concern were infection and seizures. The only tight interphase was between the nail and the skull and once the space was widened by a small burr hole, the nail became loose and it was extracted easily without any resistance. The duration of impalement could have accounted for the minimal bleeding as clots would have sealed off any injured vessels. The delay on the other hand caused rusting of the nail and mild wound infection. The track was copiously irrigated with normal saline, the wound necessarily debrided and partially left open for dressing. It is recommended that antibiotics be administered for at least 1–2 weeks [4]. Our patient was given broad spectrum antibiotics for 10 days during which the purulent discharge stopped. There was no major complication like cerebral abscess, meningitis, cavernous sinus thrombosis or persistent cerebrospinal fluid leakage. Even when there are no symptoms, it is recommended that any impaled nail should be removed surgically after thorough radiological and clinical assessment [3]. Blind extraction by pulling on the impaled object is not recommended because of secondary brain injuries that may result [4]. Some works have advised on the use of computerized tomography scan to determine the extent of associated brain injury though efforts should be made to reduce excessive metal artefact shadows by using dual energy scan [10], [11]. Some centres also consider the use of combined arterial and venous phase angiography as it obviates the metal artefact shadows that is inherent in CT scan [4] and also, it defines the relationship between the impaled object and the critical anatomy further. The usefulness of angiography and computerized tomography scan cannot be over-emphasized. Angiography will locate any major vessels in the vicinity of the nail and more importantly can also define any pseudo-aneurysm [4], which may cause catastrophic bleeding, if it ruptures during the extraction. Some small post traumatic false aneurysm may resolve while some may enlarge further and can rupture on the long term after treatment for penetrating brain injury. There is the need for monitoring where possible, with follow up CT scans especially without the metal artefact or with angiography [4], [9], [10]. Their unaffordability and unavailability made reliance on clinical assessment and radiography the only diagnostic workup and postoperative follow-up of our patient. In a poor resource setting like ours, the challenges in managing this patient were enormous and the solutions may not have been by just referring the patient to a faraway neurosurgical centre but in ensuring that the patient got to the referral centre. In this patient as in many other cases, this was not possible and so we were committed to managing our resources well enough to provide this specialized care for the patient. The traditional Hudson brace and burr drill bits were the only armamentaria available to us.
4. Conclusion
Careful planning and preparation for a selected case like this yield good results. In situations where neurosurgeons are not readily available, and the nearest regional neurosurgical centre is still faraway, orthopaedic surgeons in my institution are officially rostered to double as specialist surgeons to manage some neurosurgical emergencies. It is our recommendation that younger residents be encouraged to pursue capacity building in neurosurgery. This will enhance manpower development, provide better expert services and increase the hope to achieve our millennium development goals in health care delivery.
Conflict of interest
There is no conflict of interest amongst the authors.
Funding
The work is self-sponsored by the first author who conceptualized and designed and wrote the manuscript. The second author assisted in the surgery provided some literature review and made necessary correction which lead to the final manuscript.
Ethical approval
The ethical committee of Imo State University Teaching Hospital Orlu where the authors carried out the procedure approved the work. Ref no. IMSUTH/24/9/2015.
Consent
The patient and his mother gave an informed consent for this publication. They understand that part of his images will be published and also understand that due to the rarity of the case, that it is worthwhile publishing it for education and for health care delivery. The consent was unconditional.
Author contribution
The first author carried out the procedure, designed and wrote the manuscript. The second author assisted during the surgery, provided immediate care, provided some literature review and made necessary correction which lead to the final manuscript.
Guarantor
Agu Thaddeus Chika.
References
- 1.Dollahite H., Collinge C. Removal of a nail from bone after nail gun injury: a case report and utility of a classic technique. J. Orthop. Trauma. 2012;26(August (8)):129–131. doi: 10.1097/BOT.0b013e31823a8517. [DOI] [PubMed] [Google Scholar]
- 2.Wei L., Hai L., Shuyu H., Ying Z., Jingsheng L., Baiyun L. Penetrating brain injury caused by nail guns: two case reports and a review of the literature. Brain Inj. 2012;26(13):1756–1762. doi: 10.3109/02699052.2012.700085. [DOI] [PubMed] [Google Scholar]
- 3.Schwarzschild M. Nail in the brain. N. Engl. J. Med. 1993;328:620. [Google Scholar]
- 4.Justin M.S., Jonathan J.L., Saleen I.A. Management of non-missile penetrating brain injuries: a description of three cases and review of the literature. Skull Base Rep. 2011;1(May (1)):39–46. doi: 10.1055/s-0031-1275257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jacobs L.M., Berrizbeitia L.D., Ordia J. Crowbar impalement of the brain. J. Trauma. 1985;25(April (4)):359–361. doi: 10.1097/00005373-198504000-00016. [DOI] [PubMed] [Google Scholar]
- 6.Williams J.R., Aghion D.M., Doberstein C.E., Cosgrove G.R., Asaad W.F. Penetrating brain injury after suicide attempt with speargun: case study and review of literature. Front. Neurol. 2014;5:133. doi: 10.3389/fneur.2014.00113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jacob J.T., Cohen-Gadol A.A., Maher C.O., Meyer F.B. Trans-orbital penetrating brainstem injury in a child: a case report. J. Neurosurg. 2005;102(April (3)):350–352. doi: 10.3171/ped.2005.102.3.0350. [DOI] [PubMed] [Google Scholar]
- 8.Hussain M., Muhammad E.B. Suicide bomb attack causing penetrating craniocerebral injury. Chin. J. Traumatol. 2013;16(1):51–53. [PubMed] [Google Scholar]
- 9.Darwin J.F., Ludwig G.K. False aneurysm secondary to penetration of the brain through orbito-facial wounds: report of two cases. J. Neurosurg. 1972;36(April (4)):503–506. doi: 10.3171/jns.1972.36.4.0503. [DOI] [PubMed] [Google Scholar]
- 10.Litvack Z.N., Hunt M.A., Weinstein J.S., West G.A. Self-inflicted nail gun injury with 12 cranial penetration and associated cerebral trauma: case report and review of the literature. J. Neurosurg. 2006;104(May (5)):828–834. doi: 10.3171/jns.2006.104.5.828. [DOI] [PubMed] [Google Scholar]
- 11.Nakayama Y., Tanaka A., Arista T. Penetrating head injury caused by weed: a case report. No To Shinkei. 1995;47(12):1192–1194. [PubMed] [Google Scholar]