

Abstract
Epidemiological studies have linked daily concentrations of urban air pollution to mortality, but few have investigated specific traffic sources that can inform abatement policies. We assembled a database of >100 daily, measured and modelled pollutant concentrations characterizing air pollution in London between 2011 and 2012. Based on the analyses of temporal patterns and correlations between the metrics, knowledge of local emission sources and reference to the existing literature, we selected, a priori, markers of traffic pollution: oxides of nitrogen (general traffic); elemental and black carbon (EC/BC) (diesel exhaust); carbon monoxide (petrol exhaust); copper (tyre), zinc (brake) and aluminium (mineral dust). Poisson regression accounting for seasonality and meteorology was used to estimate the percentage change in risk of death associated with an interquartile increment of each pollutant. Associations were generally small with confidence intervals that spanned 0% and tended to be negative for cardiovascular mortality and positive for respiratory mortality. The strongest positive associations were for EC and BC adjusted for particle mass and respiratory mortality, 2.66% (95% confidence interval: 0.11, 5.28) and 2.72% (0.09, 5.42) per 0.8 and 1.0 μg/m3, respectively. These associations were robust to adjustment for other traffic metrics and regional pollutants, suggesting a degree of specificity with respiratory mortality and diesel exhaust containing EC/BC.
Keywords: mortality, short-term associations, time-series analysis, traffic-related pollution
INTRODUCTION
Epidemiological studies have provided a substantial body of evidence linking daily concentrations of outdoor air pollution to adverse effects on a range of health outcomes. This literature comprising evidence from cohort, time-series, toxicological and mechanistic studies, has been subject to thorough review.1, 2, 3, 4, 5 Studies have tended to focus on the mass concentrations of particles and selected gaseous pollutants, but more insight is required regarding the most harmful sources and components of the air pollution mixture to inform focused policies to protect public health. Hence, a growing number of studies have attempted to assess which components of the particle mixture are responsible for the observed associations.6, 7, 8, 9, 10, 11, 12, 13, 14
Time-series studies investigating associations between traffic-related pollution and mortality have used source-apportioned exposures to traffic15, 16, 17, 18, 19 or routinely measured pollutants such as PM2.5 or nitrogen dioxide (NO2)5 or elemental (EC) or black carbon (BC).13 There is suggestive evidence for the biological mechanism of these effects from controlled toxicological exposure studies,20 with increases in markers of oxidative stress21 and evidence of DNA methylation changes also identified.22 Because some traffic-related pollutants have other sources and spatial distributions, the challenge is to identify the degree to which the various components are specific for traffic, both in the near-roadside and urban background context. To meet this challenge, extensive data monitoring networks and measurement campaigns providing complete daily data over a sufficiently long period of time are required. Consequently, few epidemiological studies have been able to fully assess health effects associated with specific sources.
To investigate associations between short-term exposure to air pollutants arising from traffic sources and daily mortality in London, we assembled a database comprising daily counts of deaths from all causes and from cardiovascular and respiratory diseases and a large number of pollutants, measured daily, obtained from routine and campaign-based monitoring further enhanced by modelling. Based on the published literature on urban air pollution sources, analyses of temporal and seasonal patterns and the correlations between the assembled pollution metrics, we selected, a priori, indicators of diesel and petrol exhaust, tyre, brake and road wear for inclusion in a time-series analyses of daily mortality.
MATERIALS AND METHODS
Data
Individual death registration records for the period 1 January 2011 to 31 December 2012 were obtained from the Office for National Statistics. From these records, we constructed daily counts of deaths in London, United Kingdom based on the underlying cause of death for all disease-related causes and from cardiovascular (International Classification of Diseases, 10th revision—ICD10: I00-I99) and respiratory (ICD10: J00-J99) diseases.
Daily pollution concentrations were obtained from: (1) the London Air Quality Network (www.londonair.org.uk); (2) the UK Particle Concentrations and Numbers Network (http://uk-air.defra.gov.uk/networks/network-info?view=particle); (3) the ClearfLo23 project that measured pollutant concentrations at seven locations across London and the South East of England; and (4) by a receptor modelling exercise to isolate the urban increment from regional background concentrations. Data on over 100 pollutant metrics were assembled. From these data we selected, a priori, the most appropriate metrics to act as markers of a range of traffic sources in our main analyses. This selection was based on the analyses of temporal patterns and correlations between the metrics, knowledge of local emission sources and reference to the existing literature. Supplementary Table S1 online provides details regarding the rationale for the selection of these metrics and of their measurement methods. In brief, (1) oxides of nitrogen (NOX) was selected as a general indicator of traffic pollution as road transport represented ~47% of NOX emissions in 2010 compared with 16% for space heating;24 (2) carbon monoxide (CO) was selected as an indicator of petrol engine exhaust as in London it is derived predominately from incomplete petrol combustion;25 (3) EC in PM10 (mass of particles with aerodynamic diameter <10 μm) and BC in PM2.5 (mass of particles with aerodynamic diameter <2.5 μm) were selected as markers of emissions from diesel vehicles;26 (4) copper (Cu) was selected as an indicator of brake wear as it is generally the most abundant element in brake linings and in brake dust;27 (5) zinc (Zn) was selected as an indicator of tyre wear as it is the only element in tyres with concentrations above those found in crustal material;27 and (6) aluminium (Al) was selected as the indicator species for mineral dust including road wear.28 All of the above pollutants were measured at the central London background monitoring site at North Kensington. All measurements were 24-h averages except for CO, which were 8-h averages. We assessed the specificity of each traffic indicator from other sources by calculating a mean kerbside enrichment factor. This was defined as: kerbside enrichment factor=((roadside)−(background)/(background) using the London Marylebone Road monitoring site to indicate roadside concentrations and the North Kensington site to indicate background concentrations.
As a supplementary analysis, we estimated the concentrations of NOX, CO, BC and EC, designated NOX urban, CO urban, BC urban and EC urban, which were attributed to London sources rather than more distant sources. London has relatively little heavy industry and the calculation of an urban increment allowed us to focus more specifically on emissions from traffic sources. Using the method of Lenschow et al.,29 daily urban increments of NOX, BC and EC above the regional concentrations were calculated by subtracting from concentrations measured in North Kensington those measured at a rural site either to the west (Harwell, Oxfordshire, UK) or east (Detling, Kent, UK) of London dependent on the wind direction on each day. A similar approach was applied for CO using additional measurements made at Royal Holloway (University of London, Surrey, UK).
Finally, we assessed associations with regulated pollutants including PM10, PM2.5, NO2, sulphur dioxide (SO2) and ozone (O3) measured at background monitoring stations at North Kensington and as daily averages of concentrations measured at all available background monitoring stations across London (see Supplementary Table S1 online for details of measurement methods and summaries of daily pollutant concentrations and intercorrelations between monitoring stations).
Mean daily temperature (°C) and relative humidity (%) were also collected for the period 2011–2012 from a meteorological station close to the North Kensington monitoring site.
Statistical Methods
We used generalized additive models to investigate associations between daily concentrations of each pollutant and daily mortality counts assuming a Poisson distribution with adjustment for overdispersion. The model was of the form:
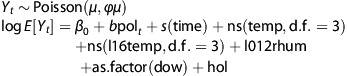 |
where Yt is the number of deaths on day t, with expectation μ, ϕ is the overdispersion parameter, “pol” is the pollutant concentration and “time” is a continuous variable indicating each day of the study period (1–722). Based on a previous work in London,30 we selected a priori, previous day pollution concentrations (lag 1) for total and CVD mortality and the previous 2 days concentration (lag 2) for respiratory mortality. As a sensitivity analysis for the lag choice, we also investigated the cumulative effect over weekly exposure (lags 0–6) using unconstrained distributed lag models.31 The time variable was introduced into the model using penalized regression splines (s) with natural spline basis, to capture the association between omitted time-varying covariates and daily mortality. The degrees of freedom (d.f.) for time adjustment were chosen based on the minimization of the absolute value of the sum of the partial autocorrelation function of the residuals (lags 1–30), with a minimum of 3 d.f. per year.32 Weather-related confounding effects on mortality were controlled using mean daily temperature and relative humidity. Two temperature terms were introduced in the model using natural cubic splines with 3 d.f.: same-day temperature (temp) to capture the heat effect and the average of the previous 6 days temperature (l16(temp)) to capture the prolonged cold effect. A linear term of the average of the same and the two previous days' relative humidity (l012rhum) was used. Dummy variables for week day (dow) and public holidays (hol) were also included in the model. Associations between EC/BC, Cu, Zn and Al and mortality were assessed using two-pollutant models incorporating particle (PM10/PM2.5) mass concentrations.
We also assessed associations stratified by season—warm season was defined as the period from April to September and cool season from October to March. The model used in the seasonal analysis was similar to the annual one, except for seasonality and long-term trends control, for which we used indicator variables per month per year of the study.
Two-pollutant models were applied for pollutant pairs with a correlation coefficient below 0.7 and representing different sources (e.g. NOX or CO controlling for non-traffic-related gases such as SO2 and O3). For multipollutant models involving EC/BC or metals where adjustment for PM mass was also required, we used the constituent residual method of Mostofsky et al.33
Results are presented as percent change in mortality for an interquartile (IQR) increase in pollutant concentration to facilitate comparison of relative risks (RRs) between pollutants. Analyses were performed using R v.3.0.3 software (R development Core Team (2011), ISBN 3-900051-07-0; URL: http://www.R-project.org).
RESULTS
Brief descriptive statistics for daily mortality counts, pollutants, temperature and humidity are presented in Table 1. Mortality data were available for 722 days during the 2-year study period. The median daily numbers of deaths from all causes, and cardiovascular and respiratory diseases were 117, 35 and 17, respectively. All pollutant concentrations were available for at least 86% of the days during the study period. Daily median PM2.5, NOX and CO concentrations were 9.0, 41.8 and 0.3 mg/m3, respectively. Urban NOX concentrations comprised ~75% of total NOX measured in Central London, whereas only 33% of CO concentrations were attributed to the urban increment. EC/BC concentrations in PM2.5 were also driven by local sources (median urban concentrations of EC and BC were 0.6 and 0.7 μg/m3, respectively, compared with total EC and BC concentrations of 0.8 and 1.2 μg/m3, respectively). Median concentrations of all pollutants except O3 were lower during the warm period compared with the cool period of the year (Supplementary Table S2). Roadside enrichment factors for NOX, BC, EC and Cu were 4.6, 5.6, 5.4 and 4.7, respectively, indicating a high degree of specificity for traffic sources, but lower for CO (1.4), Zn (1.3) and Al (1.3). Enrichment factors in the cool period for NOX, BC, EC and Cu were 3.5, 4.5, 4.2 and 3.8, respectively, increasing to 6.8, 7.2, 7.3 and 5.9 during the warm period of the year.
Table 1. Descriptive statistics for study variables.a.
| Number of days |
Percentiles |
|||||
|---|---|---|---|---|---|---|
| 10th | 25th | 50th | 75th | 90th | ||
| Mortality (n per day) | ||||||
| Total | 722 | 99 | 107 | 117 | 128 | 139 |
| Cardiovascular | 722 | 27 | 31 | 35 | 40 | 45 |
| Respiratory | 722 | 11 | 13 | 17 | 21 | 25 |
| Pollutants (μg/m3) | ||||||
| Traffic markers | ||||||
| NOX | 697 | 21.8 | 27.5 | 41.8 | 69.1 | 106.7 |
| NOX urban increment | 694 | 14.9 | 19.7 | 31.3 | 53.4 | 84.8 |
| CO (mg/m3) | 720 | 0.2 | 0.2 | 0.3 | 0.4 | 0.5 |
| CO urban increment (mg/m3) | 715 | 0 | 0 | 0.1 | 0.1 | 0.2 |
| EC (in PM10) | 674 | 0.4 | 0.5 | 0.8 | 1.3 | 1.9 |
| EC urban (in PM10) | 582 | 0.3 | 0.4 | 0.6 | 0.9 | 1.4 |
| BC (in PM2.5) | 693 | 0.6 | 0.8 | 1.2 | 1.8 | 2.8 |
| BC urban (in PM2.5) | 621 | 0.3 | 0.5 | 0.7 | 1.1 | 1.8 |
| Cu (in PM10) | 668 | 0.003 | 0.004 | 0.007 | 0.012 | 0.018 |
| Zn (in PM10) | 668 | 0.004 | 0.005 | 0.009 | 0.014 | 0.025 |
| Al (in PM10) | 668 | 0.023 | 0.033 | 0.056 | 0.095 | 0.154 |
| Regulated pollutants | ||||||
| PM10 | 720 | 9 | 11 | 15 | 21 | 32.6 |
| PM2.5 | 721 | 5 | 6 | 9 | 14 | 25 |
| NO2 | 697 | 18.6 | 23.3 | 33.6 | 47 | 58.1 |
| SO2 | 708 | 0 | 0.4 | 1.8 | 2.6 | 3.6 |
| O3 | 707 | 21.6 | 39 | 54.4 | 69.7 | 86 |
| Meteorology | ||||||
| Mean temperature (°C) | 722 | 5 | 8.1 | 11.8 | 15.5 | 18.1 |
| Relative humidity (%) | 722 | 61.6 | 69.6 | 77.9 | 84.1 | 88.5 |
Abbreviations: Al, Aluminium; BC, black carbon; CO, carbon monoxide; Cu, Copper; EC, elemental carbon; NO2, nitrogen dioxide; NOX, oxides of nitrogen; O3, ozone; PM, particulate matter; PM2.5, mass of particles with diameter <2.5 microns; PM10, mass of particles with diameter <10 microns; SO2, sulphur dioxide; Zn, Zinc.
Traffic-related and regulated pollutants and meteorological variables in London, United Kingdom, for 1 January 2011–22 December 2012.
Pearson's correlation coefficients for pollutant pairs for the study period, and by warm and cool periods are given in Supplementary Table S3 online. Across the study period, NOX concentrations were closely correlated with CO concentrations (Pearson's correlation coefficient r=0.83), with both EC and BC (r=0.91 and 0.90, respectively), but less so with markers of brake and tyre wear (Cu, r=0.77; Zn, r=0.68) and only weakly correlated with road wear (Al, r=0.36). Urban increments of NOX, EC and BC were strongly correlated with total concentrations (r=0.98, 0.92 and 0.92, respectively), whereas urban increments of CO were generally less strongly correlated with daily total CO concentrations (r=0.6). When stratified by warm and cool periods of the year, the pattern of correlations was broadly similar, other than for O3, where associations with all traffic markers were generally positive during the warm period and negative during the cool period.
Table 2 shows the percent change in mortality (and 95% confidence intervals (CIs)) associated with an IQR increase in traffic-related pollutants, lagged 1 day for total and cardiovascular mortality and for 2 days for respiratory mortality. Associations for cumulative concentrations (average of lags 0–6) are given in Supplementary Table S4 online. For total and cardiovascular mortality, there was little evidence for associations with any traffic marker: associations for interquartile range increments in the pollutants were generally below 1% with CIs that spanned 0%. Associations with respiratory mortality tended to be positive and the largest associations observed were for EC adjusted for particle mass (2.66% (95% CI: 0.11, 5.28) and BC adjusted for particle mass (2.72% (95% CI: 0.09, 5.42) per IQR. Associations with the urban increment estimates followed those of the measured concentrations (Supplementary Table S5 online). Associations with the regulated pollutants, PM10, PM2.5, NO2, SO2 and O3, measured at North Kensington were negative except for O3 (Supplementary Table S6 online). A similar pattern of associations was observed when daily, London-wide average concentrations derived from all available background monitors were used (data not shown).
Table 2. Percent change in mortality (and 95% CIs) associated with an IQR increase.a.
| Pollutant | IQR | Total% (95% CI) | Cardiovascular% (95% CI) | Respiratory% (95% CI) |
|---|---|---|---|---|
| NOX | 41.6 | −0.43 (−1.24, 0.40) | −1.29 (−2.72, 0.17) | −0.04 (−1.96, 1.91) |
| CO | 0.2 | −0.79 (−1.63, 0.04) | −1.47 (−2.94, 0.01) | 0.41 (−1.62, 2.48) |
| EC (PM10) | 0.8 | 0.45 (−0.58, 1.49) | −0.47 (−2.30, 1.40) | 2.66 (0.11, 5.28) |
| BC (PM2.5) | 1.0 | 0.47 (−0.63, 1.58) | −0.83 (−2.75, 1.13) | 2.72 (0.09, 5.42) |
| Cu (PM10) | 0.008 | −0.05 (−1.14, 1.05) | −0.94 (−2.85, 1.00) | 1.53 (−1.14, 4.27) |
| Zn (PM10) | 0.009 | −0.12 (−1.06, 0.83) | −1.58 (−3.25, 0.12) | −0.34 (−2.83, 1.84) |
| Al (PM10) | 0.062 | 0.58 (−0.62, 1.80) | 0.38 (−1.70, 2.50) | 1.77 (−1.18, 4.81) |
Abbreviations: Al, Aluminium; BC, black carbon; CI, confidence interval; CO, carbon monoxide; Cu, Copper; EC, elemental carbon; IQR, interquartile range; NOX, oxides of nitrogen; PM, particulate matter; PM2.5, mass of particles with diameter <2.5 microns; PM10, mass of particles with diameter <10 microns; Zn, Zinc.
Results for EC/BC and elemental components are adjusted for PM mass.
In traffic-related pollutants (lag 1 for total and cardiovascular and lag 2 for respiratory mortality) in London, United Kingdom, for 1 January 2011–22 December 2012.
Figure 1 gives the percent change in total (A), cardiovascular (B) and respiratory (C) mortality (and 95% CIs) associated with a period-specific IQR increase in traffic-related pollutants (lag 1 for total and cardiovascular and lag 2 for respiratory mortality). Point estimates and confidence intervals are also tabulated in the Supplementary Table S7 online. Associations between all pollutants and total and cause-specific mortality in the warm period of the year were generally positive and larger than cool period associations, although the seasonal differences did not achieve statistical significance.
Figure 1.

Percent change in total (a), cardiovascular (b) and respiratory (c) mortality (and 95% confidence intervals (CIs)) associated with a period-specific interquartile range (IQR) increase in traffic-related pollutants (lag 1 for total and cardiovascular and lag 2 for respiratory mortality). Al, Aluminium; BC, black carbon; CO, carbon monoxide; Cu, Copper; EC, elemental carbon; NOX, oxides of nitrogen; Zn, Zinc.
Results from selected two-pollutant models are shown in Table 3. In general, associations for NOX and CO increased in magnitude after adjustment for O3 and SO2. The table shows the impact on the EC/BC mortality associations after adjustment for particle mass — associations increased in magnitude, particularly for respiratory mortality. Adjustment for CO, O3 and SO2 increased the magnitude of the EC/BC associations further still. Similar patterns of changes in the magnitude of the associations were observed for Cu and Al, but not Zn when adjusted for PM mass, CO, O3 and SO2.
Table 3. Results from two-pollutant models.a.
| Pollutant (IQR, μg/m3) | Adjustment |
Mortality% (95% CI) |
||
|---|---|---|---|---|
| Total | Cardiovascular | Respiratory | ||
| NOX (41.6) | None | −0.43 (−1.24, 0.40) | −1.29 (−2.72, 0.17) | −0.04 (−1.96, 1.91) |
| O3 | −0.09 (−1.03, 0.86) | −0.47 (−2.11, 1.20) | 0.54 (−1.64, 2.76) | |
| SO2 | 0.05 (−0.94, 1.06) | −0.75 (−2.50, 1.03) | 1.01 (−1.40, 3.48) | |
| PM2.5 | 0.05 (−0.99, 1.10) | −0.82 (−2.67, 1.07) | 0.42 (−2.02, 2.92) | |
| CO (0.2 mg/m3) | None | −0.79 (−1.63, 0.04) | −1.47 (−2.94, 0.01) | 0.41 (−1.62, 2.48) |
| EC (PM10)b | −0.75 (−1.59, 0.09) | −1.42 (−2.91, 0.09) | 0.43 (−1.62, 2.53) | |
| O3 | −0.60 (−1.50, 0.30) | −0.87 (−2.44, 0.72) | 0.90 (−1.29, 3.15) | |
| SO2 | −0.52 (−1.47, 0.43) | −0.96 (−2.63, 0.73) | 0.95 (−1.39, 3.35) | |
| EC (0.8) | None | 0.03 (−0.84, 0.90) | −0.90 (−2.43, 0.66) | 1.52 (−0.59, 3.68) |
| PM10 | 0.45 (−0.58, 1.49) | −0.47 (−2.30, 1.40) | 2.66 (0.11, 5.28) | |
| PM10+CO | 1.57 (0.18, 2.98) | 0.64 (−1.82, 3.16) | 3.20 (−0.25, 6.77) | |
| PM10+O3 | 0.67 (−0.40, 1.75) | 0.11 (−1.79, 2.04) | 3.06 (0.42, 5.76) | |
| PM10+SO2 | 0.73 (−0.36, 1.84) | −0.19 (−2.13, 1.78) | 3.17 (0.43, 5.98) | |
| BC (1.0) | None | −0.28 (−1.09, 0.55) | −1.30 (−2.72, 0.14) | 1.28 (−0.67, 3.27) |
| PM2.5 | 0.47 (−0.63, 1.58) | −0.83 (−2.75, 1.13) | 2.72 (0.09, 5.42) | |
| PM2.5+CO | 1.76 (0.17, 3.36) | −0.10 (−2.81, 2.69) | 3.98 (0.15, 7.95) | |
| PM2.5+O3 | 0.63 (−0.50, 1.78) | −0.32 (−2.29, 1.70) | 3.20 (0.49, 5.99) | |
| PM2.5+SO2 | 0.55 (−0.61, 1.73) | −0.71 (−2.74, 1.35) | 3.70 (0.86, 6.62) | |
| Cu (0.008) | None | −0.35 (−1.25, 0.56) | −1.24 (−2.81, 0.35) | 0.73 (−1.44, 2.95) |
| PM10 | −0.05 (−1.14, 1.05) | −0.94 (−2.85, 1.00) | 1.53 (−1.14, 4.27) | |
| PM10+CO | 0.43 (−0.84, 1.71) | −0.19 (−2.39, 2.06) | 1.11 (−1.96, 4.27) | |
| PM10+O3 | 0.16 (−0.96, 1.30) | −0.46 (−2.40, 1.53) | 1.81 (−0.92, 4.61) | |
| PM10+SO2 | 0.17 (−0.96, 1.31) | −0.79 (−2.76, 1.22) | 1.76 (−1.02, 4.62) | |
| Zn (0.009) | None | −0.36 (−1.05, 0.34) | −1.39 (−2.60, −0.17) | −0.44 (−2.13, 1.28) |
| PM10 | −0.12 (−1.06, 0.83) | −1.58 (−3.25, 0.12) | −0.34 (−2.83, 1.84) | |
| PM10+CO | 0.08 (−0.91, 1.08) | −1.25 (−3.00, 0.52) | −0.74 (−3.18, 1.77) | |
| PM10+O3 | 0.02 (−0.94, 0.98) | −1.34 (−3.02, 0.37) | −0.21 (−2.57, 2.22) | |
| PM10+SO2 | 0.02 (−0.95, 1.01) | −1.38 (−3.10, 0.37) | −0.31 (−2.74, 2.17) | |
| Al (0.062) | None | −0.04 (−0.94, 0.87) | −0.50 (−2.02, 1.04) | 0.62 (−1.54, 2.82) |
| PM10 | 0.58 (−0.62, 1.80) | 0.38 (−1.70, 2.50) | 1.77 (−1.18, 4.81) | |
| PM10+CO | 0.65 (−0.58, 1.89) | 0.40 (−1.67, 2.52) | 1.75 (−1.21, 4.80) | |
| PM10+O3 | 0.48 (−0.73, 1.70) | −0.02 (−2.11, 2.12) | 1.84 (−1.17, 4.94) | |
| PM10+SO2 | 0.71 (−0.52, 1.95) | 0.34 (−1.77, 2.50) | 1.87 (−1.18, 5.01) | |
Abbreviations: Al, Aluminium; BC, black carbon; CI, confidence interval; CO, carbon monoxide; Cu, copper, EC, elemental carbon; IQR, interquartile range; NOX, oxides of nitrogen; O3, ozone; PM, particulate matter; PM2.5, mass of particles with diameter <2.5 microns; PM10, mass of particles with diameter <10 microns; SO2, sulphur dioxide; Zn, zinc.
Percent change in mortality (and 95% CIs) associated with an IQR increase in traffic-related (lag 1 for total and cardiovascular and lag 2 for respiratory mortality) in London, United Kingdom, for 1 January 2011–22 December 2012.
Adjusted for PM mass.
DISCUSSION
Overview
We investigated associations between daily concentrations of specific traffic-related pollutants and daily total and cause-specific mortality in London between 2011 and 2012. Pollutants selected a priori were NOX (general traffic pollution); EC/BC and CO (markers of diesel and petrol exhaust, respectively); Cu (tyre wear); Zn (brake wear) and Al for mineral dust. Associations between all pollutants and mortality were generally below 1% per IQR, with confidence intervals that spanned 0%. Associations with respiratory mortality were generally positive, stronger in the warmer months of the year and most convincing for EC and BC adjusted for PM mass.
Selection of Traffic Indicators
Our approach of selecting source-specific pollutant metrics contrasts with the usual approach adopted in time-series studies of focusing on routinely monitored, regulated pollutants. The assembly of an analytic database containing a large number of pollutant metrics facilitated a thorough assessment of the seasonal patterns of a range of pollutants, the correlations between them and the calculation of urban increments and roadside enrichment factors. These analyses underpinned our strategy of selecting traffic-specific metrics for our analyses. Our selected indicators of traffic pollution were, in general, moderately correlated, except for our marker of general traffic pollution (NOX), which was highly correlated with both diesel and petrol exhaust indicators and therefore was not expected to provide additional information.
The use of indicator species to identify emissions from air pollution sources is well established in receptor analysis and source apportionment.34 The correct interpretation of the results from our epidemiological analyses does, however, rely on source specificity of the selected metrics. Roadside enrichment factors were over 4 for NOX, BC, EC and Cu, indicating a high degree of specificity for traffic sources but lower for CO, Zn and Al. However, we acknowledge that the metrics selected are not exclusive indicators of the relevant traffic sources —a point made by the HEI in their review of traffic pollution.20 Nonetheless, our approach goes some way towards providing policy makers with the information needed to formulate policy and regulation to protect public health. The development of more specific markers for traffic pollutants would improve future studies. Although the increasing measurement of organic aerosol using aerosol mass spectrometry is opening insights into these types of particles, the complexity of organic aerosol and the aging and oxidation processes that it is subject to makes establishing a tracer difficult.35 The application of primary matrix factorization on the PM metrics measured at North Kensington was not able to separate different types of traffic emission sources.36
Our selective approach is also particularly relevant when a large number of pollutant metrics are available for analysis, as it enables a hypothesis testing strategy. This approach minimizes the problem of multiple testing common in air pollution epidemiology, where many outcomes and pollutants lead to large numbers of model results and consequently difficulties in interpreting the findings and a greater potential for publication bias. Alternative approaches to this problem include assessing associations with mixtures rather than individual pollutants37 and source apportionment techniques to identify factors indicating specific pollution sources.15, 19 These data-driven techniques characterize complex local pollution mixtures and inform policy thinking but are limited when health impact assessment exercises are required to formulate policy options and in monitoring the effects of policy measures implemented to reduce pollution. Another approach using the time-series design incorporated dispersion models to differentiate residential locations exposed to traffic and non-traffic sources or to focus on peak periods of pollution dominated by traffic sources.38 Both of these approaches require substantial data and analytical effort to focus on traffic sources, but supplement studies of regulated pollutants by providing more specific policy relevant information.
Is Short-Term Exposure to Traffic Pollution Associated with Mortality?
We found no evidence for associations between our chosen indicator of general traffic pollution, NOX, and total or cause-specific mortality. Relatively few time-series studies have assessed associations with NOX, focusing instead upon NO2 as a regulated pollutant. We did not find evidence for an association between NO2 and mortality. NOX interacts with O3 interchanging NO and NO239 and is negatively correlated with O3, although the correlations between the pollutants also vary by season. Adjustment for O3 increased the size of the NOX associations (Table 3), but our conclusion regarding NOX remained unaltered. The recent review by the World Health Organization on the health effects associated with air pollution specifically addressed the question of traffic pollution and health and focused on PM components and NO2 rather than NOX.5 An earlier review by the Health Effects Institute focusing on the health effects associated with traffic pollution20 identified only four studies that utilized a variety of traffic indicators and concluded that the findings “were somewhat unclear with respect to associations between short-term exposure to pollutants derived from traffic emissions and all-cause mortality”.
Can We Differentiate Between Different Components of Traffic Pollution?
Our analysis of total and cause-specific mortality in relation to the components of traffic pollution revealed some degree of specificity, with positive associations observed between daily concentrations of EC and BC (each adjusted for PM mass and lagged 2 days) and respiratory mortality that were robust to adjustment for other traffic source indicators. There was, however, some inconsistency between the single-day and cumulative lag results. Although we have no clear explanation for these apparent inconsistencies, it is possible that the cumulative measures are capturing some harvesting.40, 41
Associations between EC/BC and respiratory mortality have been reported in a recently published study from the MED-PARTICLES project42 and are consistent with the conclusions from an assessment of BC particles.13 A more recent systematic review of time-series studies focusing on particle components concluded that the evidence per unit mass was strongest for EC/BC and respiratory mortality.10 Although the lack of evidence for associations between EC/BC and cardiovascular mortality reported in this study is inconsistent with the positive associations also highlighted in these reviews,10, 13 we note that the present study, together with our earlier time-series study in London,30 also failed to find evidence of adverse associations between PM2.5 and cardiovascular mortality, findings contrary to evidence presented in systematic reviews.43 The results for cardiovascular mortality in Athens and Barcelona,42 whereas positive and statistically significant for 1 of the 4 lags investigated, were substantially smaller than those observed for respiratory mortality.
Given the close correlation between NOX and EC/BC (r=0.91 & 0.9), the inconsistency in associations with respiratory mortality between NOX and EC/BC was surprising. This inconsistency was partially explained by the fact that risk estimates for EC/BC were adjusted for particle mass, whereas NOX was not, and after adjustment for PM2.5, the NOX association increased from −0.04 to 0.42 per IQR (Table 3).
Both measured and modelled urban increment concentrations of CO were associated with respiratory mortality, especially during the warmer months of the year. However, adjustment for carbon, particularly EC, attenuated the CO–respiratory mortality associations, suggesting some confounding. Compared with other source indicators, the association between ambient outdoor CO and mortality has received relatively little attention.44 A systematic review of the time-series evidence published in 2007 identified positive associations with increased mortality.45 At that time, the evidence regarding the independence of CO associations from other pollutants was very limited and inconclusive.
We did not find evidence for associations between markers of brake and tyre wear and mortality. As these metallic components are highly enriched at the roadside27 and have established chemical toxicity,46, 47 the lack of an association either suggests that population exposures away from the roadside are insufficient to overwhelm endogenous airway defences or that their toxic action requires longer-term accumulation within the body, and are therefore unlikely to be apparent when interrogating short-term health effects.48 Al, which was used as a marker of mineral dust, did yield smaller positive associations with total mortality, but only during the winter months.
Overall, the pattern of associations observed suggests that traffic pollution in London, particularly that arising from the exhaust of diesel vehicles (based on the associations observed with EC and BC controlled for PM mass), has short-term impacts on respiratory mortality.
Are Associations with Traffic Markers Confounded by Other Sources of Pollution?
Our analyses using multipollutant models suggest that our findings for NOX are not confounded (positively or negatively) by regional pollutants such as SO2 or O3. Our selected metrics for EC/BC were adjusted for PM10/PM2.5 mass and are also, therefore, unlikely to be confounded by other particle components including secondary aerosols. Previous analyses of particle metric data in London reported associations between PM mass metrics and respiratory mortality driven by the non-primary particulate component.30, 49 Our finding from the present study for EC/BC adjusted for particle mass suggests that these earlier associations with secondary particles may have been confounded by EC/BC — a hypothesis that we were unable to test in the earlier study.
Seasonal Results
We observed a tendency for associations between traffic metrics and respiratory mortality to be stronger in the warmer period of the year, although we note that seasonal differences were not generally statistically significant and the period-specific associations were not precisely estimated. Nonetheless, we hypothesized that concentrations of NOX and CO during the warmer period of the year would be more indicative of traffic emissions than during winter months when space heating contributes more to NOX emissions.24 The higher roadside enrichment factors in the warm vs cool periods support this suggestion. Another possible explanation for the larger associations in the warm vs cool period is differential exposure misclassification arising from different patterns of human behaviour in the two periods of the year, in particular time spent out doors and indoor/outdoor air exchange rates.50
Strengths and Limitations
Our study benefits from the availability of complete recording of death registrations in a large city. In time-series studies, statistical power is determined by the number of observations (days), as well as the mean numbers of events per day. Our study was limited with regard to the number of days (722 days), although this was compensated for to some degree by the large study population. However, analyses with more years of data would improve the precision of our model estimates and aid interpretation.
A further limitation of our study, one inherent in many time-series studies, was the potential misclassification of exposure due to the use of pollution data from a single background monitoring station in central London. Zeger et al.51 have shown that what matters is how well the exposure series matches the mean daily exposures over the city as a whole. In London, PM2,5 measured at monitoring stations in different geographical locations are strongly correlated,52 and, to some extent, for particle number concentrations also.53 In our data, daily concentrations of PM2.5 and NO2 measured at background monitoring stations across London were well correlated, median (IQR) correlations 0.9 (0.16) and 0.77 (0.19), respectively (Supplementary Table S1 online). Results of analyses using daily averages derived from all available data from background monitoring stations across London produced comparable results to those using only data from North Kensington (data not shown). EC/BC and metals were only measured at North Kensington and we were therefore unable to assess the spatial distribution and temporal correlations across London.
Measurement errors for particle constituents are generally larger than for PM mass and, as classical error in an explanatory variable can lead to attenuation in the estimation of the RR, it is possible that the RRs for each metric may be influenced by their measurement error. However, in time-series studies exposure error comprises a combination of classical and Berskon54 error, the latter derived from the use of average exposures as a surrogate for individual exposures. How these errors impact upon the estimation of the RR can vary depending on whether the errors are additive or multiplicative.55 Without further, more extensive monitoring campaigns, it is impossible to assess these issues fully and we acknowledge that, as in other similar time-series studies, the RRs obtained in this study may be influenced by these factors. Therefore, caution should be exercised in interpreting these risk estimates.
Our analysis of the components of traffic pollution and adverse effects on daily mortality suggests a degree of specificity for respiratory mortality and diesel exhaust containing EC/BC rather than petrol exhaust or mechanical sources such as brake and tyre wear. Further studies are needed to confirm this specificity in other locations and to determine the precise nature of the toxic components of the exhaust mixture. The suggestion that these associations are more evident during the warmer months of the year warrants replication in other urban environments as it has implications for policies to protect public health.
Acknowledgments
Research described in this article was conducted under the Grant Agreement No. NE/I0078571 from National Environment Research Council, United Kingdom.
The authors declare no conflict of interest.
Footnotes
Supplementary Information accompanies the paper on the Journal of Exposure Science and Environmental Epidemiology website (http://www.nature.com/jes)
Supplementary Material
References
- 1EPA. Integrated science assessment for particulate matter. National Center for Environmental Assessment-RTP Division, Office of Research and Development. US Environmental Protection Agency Research: : Triangle Park, NC, USA. 2009. Report no. EPA/600/R-08/139F. [Google Scholar]
- 2EPA. Integrated science assessment for ozone and related photochemical oxidants. National Center for Environmental Assessment-RTP Division Office of Research and Development. US Environmental Protection Agency Research: : Triangle Park, NC, USA. 2013. Report no. EPA 600/R-10/076F. [Google Scholar]
- 3EPA. Integrated science assessment for oxides of nitrogen — health criteria. National Center for Environmental Assessment-RTP Division Office of Research and Development. US Environmental Protection Agency Research: : Triangle Park, NC, USA. 2018. Report no. EPA/600/R-08/07. [Google Scholar]
- 4EPA. Integrated science assessment for carbon monoxide. National Center for Environmental Assessment-RTP Division Office of Research and Development. US Environmental Protection Agency Research: : Triangle Park, NC, USA. 2010. Report no. EPA/600/R-09/019F. [Google Scholar]
- 5World Health Organisation. Review of Evidence on Health Aspects of Air Pollution — REVIHAAP Project: Final Technical Report. WHO: Geneva, Switzerland. 2013. [Google Scholar]
- 6Ruckerl R, Schneider A, Breitner S, Cyrys J, Peters A. Health effects of particulate air pollution: a review of epidemiological evidence. Inhal Toxicol 2011; 23: 555–592. [DOI] [PubMed] [Google Scholar]
- 7Cassee FR, Heroux ME, Gerlofs-Nijland ME, Kelly FJ. Particulate matter beyond mass: recent health evidence on the role of fractions, chemical constituents and sources of emission. Inhal Toxicol 2013; 25: 802–812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8EPA. Policy assessment for the review of the particulate matter national ambient air quality standards. US Environmental Protection Agency Office of Air Quality Planning and Standards Health and Environmental Impacts Division: : Triangle Park, NC, USA. 2011. Report no. EPA 452/R-11-003. [Google Scholar]
- 9Levy JI, Diez D, Dou Y, Barr CD, Dominici F. A meta-analysis and multisite time-series analysis of the differential toxicity of major fine particulate matter constituents. Am J Epidemiol 2012; 175: 1091–1099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10Atkinson RW, Mills IC, Walton HA, Anderson HR. Fine particle components and health-a systematic review and meta-analysis of epidemiological time series studies of daily mortality and hospital admissions. J Expo Sci Environ Epidemiol 2014; 25: 208–214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11Bell M. Assessment of the health impacts of particulate matter characteristics. Health Effects Institute: : Boston, MA, USA. 2011. Report no. 16. [PubMed] [Google Scholar]
- 12Ostro B, Hu J, Goldberg D, Reynolds P, Hertz A, Bernstein L et al. Associations of mortality with long-term exposures to fine and ultrafine particles, species and sources: Results from the california teachers study cohort. Environ Health Perspect 2015; 123: 549–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13Janssen NA, Hoek G, Simic-Lawson M, Fischer P, van BL, ten BH et al. Black carbon as an additional indicator of the adverse health effects of airborne particles compared with PM10 and PM2.5. Environ Health Perspect 2011; 119: 1691–1699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14Smith KR, Jerrett M, Anderson HR, Burnett RT, Stone V, Derwent R et al. Public health benefits of strategies to reduce greenhouse-gas emissions: health implications of short-lived greenhouse pollutants. Lancet 2009; 374: 2091–2103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15Laden F, Neas LM, Dockery DW, Schwartz J. Association of fine particulate matter from different sources with daily mortality in six U.S. cities. Environ Health Perspect 2000; 108: 941–947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16Mar TF, Ito K, Koenig JQ, Larson TV, Eatough DJ, Henry RC et al. PM source apportionment and health effects. 3. Investigation of inter-method variations in associations between estimated source contributions of PM2.5 and daily mortality in Phoenix, AZ. J Expo Sci Environ Epidemiol 2006; 16: 311–320. [DOI] [PubMed] [Google Scholar]
- 17Mar TF, Norris GA, Koenig JQ, Larson TV. Associations between air pollution and mortality in Phoenix, 1995-1997. Environ Health Perspect 2000; 108: 347–353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18Maynard D, Coull BA, Gryparis A, Schwartz J. Mortality risk associated with short-term exposure to traffic particles and sulfates. Environ Health Perspect 2007; 115: 751–755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19Ito K, Christensen WF, Eatough DJ, Henry RC, Kim E, Laden F et al. PM source apportionment and health effects: 2. An investigation of intermethod variability in associations between source-apportioned fine particle mass and daily mortality in Washington, DC. J Expos Sci Environ Epidemiol 2005; 16: 300–310. [DOI] [PubMed] [Google Scholar]
- 20HEI Panel on the Health Effects of Traffic-Related Air Pollution. Traffic-related air pollution: A critical review of the literature on emissions, exposure, and health effects. Health Effects Institute: : Boston, MA, USA. 2010. Special Report no. 17. [Google Scholar]
- 21Laumbach RJ, Kipen HM, Ko S, Kelly-McNeil K, Cepeda C, Pettit A et al. A controlled trial of acute effects of human exposure to traffic particles on pulmonary oxidative stress and heart rate variability. Part Fibre Toxicol 2014; 11: 45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22Baccarelli A, Wright RO, Bollati V, Tarantini L, Litonjua AA, Suh HH et al. Rapid DNA methylation changes after exposure to traffic particles. Am J Respir Crit Care Med 2009; 179: 572–578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23Bohnenstengel SI, Belcher SE, Aiken A, Allan JD, Allen G, Bacak A et al. Meteorology, air quality, and health in London: the ClearfLo project. Bull Am Meteor Soc 2014; 96: 719–804. [Google Scholar]
- 24Greater London Authority. The London Atmospheric Emissions Inventory, London, UK, 2012.
- 25Rhys-Tyler GA, Legassick W, Bell MC. The significance of vehicle emissions standards for levels of exhaust pollution from light vehicles in an urban area. Atmos Environ 2011; 45: 3286–3293. [Google Scholar]
- 26EEA. Status of black carbon monitoring in ambient air in Europe. European Environment Agency: : Luxemburg City, Luxemburg. 2013. Luxembourg: Publications Office of the European Union. ISBN 978-92-9213-415-0. ISSN 1725-2237. EEA technical report no. 18/2013. [Google Scholar]
- 27Thorpe A, Harrison RM. Sources and properties of non-exhaust particulate matter from road traffic: A review. Sci Total Environ 2008; 400: 270–282. [DOI] [PubMed] [Google Scholar]
- 28Viana M, Kuhlbusch TAJ, Querol X, Alastuey A, Harrison RM, Hopke PK et al. Source apportionment of particulate matter in Europe: a review of methods and results. J Aerosol Sci 2008; 39: 827–849. [Google Scholar]
- 29Lenschow P, Abraham HJ, Kutzner K, Lutz M, Preuss JD, Reichenbacher W. Some ideas about the sources of PM10. Atmos Environ 2001; 35 (Suppl. 1): S23–S33. [Google Scholar]
- 30Atkinson RW, Fuller GW, Anderson HR, Harrison RM, Armstrong B. Urban ambient particle metrics and health: a time-series analysis. Epidemiology 2010; 21: 501–511. [DOI] [PubMed] [Google Scholar]
- 31Zanobetti A, Schwartz J, Samoli E, Gryparis A, Touloumi G, Atkinson R et al. The temporal pattern of mortality responses to air pollution: a multicity assessment of mortality displacement. Epidemiology 2002; 13: 87–93. [DOI] [PubMed] [Google Scholar]
- 32Samoli E, Stafoggia M, Rodopoulou S, Ostro B, Declercq C, Alessandrini E et al. Associations between fine and coarse particles and mortality in Mediterranean cities: results from the MED-PARTICLES project. Environ Health Perspect 2013; 121: 932–938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33Mostofsky E, Schwartz J, Coull BA, Koutrakis P, Wellenius GA, Suh HH et al. Modeling the association between particle constituents of air pollution and health outcomes. Am J Epidemiol 2012; 176: 317–326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34Watson JG, Zhu T, Chow JC, Engelbrecht J, Fujita EM, Wilson WE. Receptor modeling application framework for particle source apportionment. Chemosphere 2002; 49: 1093–1136. [DOI] [PubMed] [Google Scholar]
- 35Donahue NM, Kroll JH, Pandis SN, Robinson AL. A two-dimensional volatility basis set-Part 2: diagnostics of organic-aerosol evolution. Atmos Chem Phys 2012; 12: 615–634. [Google Scholar]
- 36Beddows DCS, Harrison RM, Green DC, Fuller GW. Receptor modelling of both particle composition and size distribution from a background site in London, UK. Atmos Chem Phys 2015; 15: 10107–10125. [Google Scholar]
- 37Oakes M, Baxter L, Long TC. Evaluating the application of multipollutant exposure metrics in air pollution health studies. Environ Int 2014; 69: 90–99. [DOI] [PubMed] [Google Scholar]
- 38Madsen C, Rosland P, Hoff DA, Nystad W, Nafstad P, Naess OE. The short-term effect of 24-h average and peak air pollution on mortality in Oslo, Norway. Eur J Epidemiol 2012; 27: 717–727. [DOI] [PubMed] [Google Scholar]
- 39Seinfeld JH, Pandis SN. Atmospheric Chemistry and Physics — From Air Pollution to Climate Change. Wiley: New York, NY, USA. 2006. [Google Scholar]
- 40Zanobetti A, Schwartz J, Samoli E, Gryparis A, Touloumi G, Peacock J et al. The temporal pattern of respiratory and heart disease mortality in response to air pollution. Environ Health Perspect 2003; 111: 1188–1193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41Goodman PG, Dockery DW, Clancy L. Cause-specific mortality and the extended effects of particulate pollution and temperature exposure. Environ Health Perspect 2004; 112: 179–185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42Ostro B, Tobias A, Karanasiou A, Samoli E, Querol X, Rodopoulou S et al. The risks of acute exposure to black carbon in Southern Europe: results from the MED-PARTICLES project. Occup Environ Med 2015; 72: 123–129. [DOI] [PubMed] [Google Scholar]
- 43Atkinson RW, Kang S, Anderson HR, Mills IC, Walton HA. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: a systematic review and meta-analysis. Thorax 2014; 69: 660–665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44Samoli E, Touloumi G, Schwartz J, Anderson HR, Schindler C, Forsberg B et al. Short-term effects of carbon monoxide on mortality: an analysis within the APHEA project. Environ Health Perspect 2007; 115: 1578–1583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45Anderson HR, Atkinson RW, Bremner SA, Carrington J, Peacock J. Quantitative Systematic Review of Short Term Associations Between Ambient Air Pollution (Particulate Matter, Ozone, Nitrogen Dioxide, Sulphur Dioxide And Carbon Monoxide), and Mortality and Morbidity. Department of Health: : UK. 2007. [Google Scholar]
- 46Jomova K, Valko M. Advances in metal-induced oxidative stress and human disease. Toxicology 2011; 283: 65–87. [DOI] [PubMed] [Google Scholar]
- 47Wu W, Bromberg PA, Samet JM. Zinc ions as effectors of environmental oxidative lung injury. Free Radic Biol Med 2013; 65: 57–69. [DOI] [PubMed] [Google Scholar]
- 48Ghio AJ. Disruption of iron homeostasis and lung disease. Biochim Biophys Acta 2009; 1790: 731–739. [DOI] [PubMed] [Google Scholar]
- 49Pirani M, Best N, Blangiardo M, Liverani S, Atkinson RW, Fuller GW. Analysing the health effects of simultaneous exposure to physical and chemical properties of airborne particles. Environ Int 2015; 79: 56–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50Weschler CJ. Ozone in indoor environments: concentration and chemistry. Indoor Air 2000; 10: 269–288. [DOI] [PubMed] [Google Scholar]
- 51Zeger SL, Thomas D, Dominici F, Samet JM, Schwartz J, Dockery D et al. Exposure measurement error in time-series studies of air pollution: concepts and consequences. Environ Health Perspect 2000; 108: 419–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52Puustinen A, Hämeri K, Pekkanen J, Kulmala M, de Hartog J, Meliefste K et al. Spatial variation of particle number and mass over four European cities. Atmos Environ 2007; 41: 6622–6636. [Google Scholar]
- 53Cyrys J, Pitz M, Heinrich J, Wichmann HE, Peters A. Spatial and temporal variation of particle number concentration in Augsburg, Germany. Sci Total Environ 2008; 401: 168–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54Armstrong BG. Effect of measurement error on epidemiological studies of environmental and occupational exposures. Occup Environ Med 1998; 55: 651–656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55Butland BK, Armstrong B, Atkinson RW, Wilkinson P, Heal MR, Doherty RM et al. Measurement error in time-series analysis: a simulation study comparing modelled and monitored data. BMC Med Res Methodol 2013; 13: 136. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.