

Abstract
Background
Even if daptomycin does not have approval for the treatment of bone and joint infections (BJI), the Infectious Diseases Society of America guidelines propose this antibiotic as alternative therapy for prosthetic joint infection. The recommended dose is 6 mg/kg/d, whereas recent data support the use of higher doses in these patients.
Methods
We performed a cohort study including consecutive patients that have received daptomycin >6 mg/kg/d for complex BJI between 2011 and 2013 in a French regional reference center. Factors associated with treatment failure were determined on univariate Cox analysis and Kaplan-Meier curves.
Results
Forty-three patients (age, 61 ± 17 years) received a mean dose of 8 ± 0.9 mg/kg/d daptomycin, for a mean 81 ± 59 days (range, 6–303 days). Most had chronic (n = 37, 86 %) implant-associated (n = 37, 86 %) BJI caused by coagulase-negative staphylococci (n = 32, 74 %). A severe adverse event (SAE) occurred in 6 patients (14 %), including 2 cases of eosinophilic pneumonia, concomitant with daptomycin Cmin >24 mg/L. Outcome was favorable in 30 (77 %) of the 39 clinically assessable patients. Predictors for treatment failure were age, non-optimal surgery and daptomycin withdrawal for SAE.
Conclusions
Prolonged high-dose daptomycin therapy was effective in patients with complex BJI. However, optimal surgery remains the cornerstone of medico-surgical strategy; and a higher incidence of eosinophilic pneumonia than expected was recorded.
Keywords: Daptomycin, Bone and joint infection, Eosinophilic pneumonia
Background
Bone and joint infections (BJI) include very heterogeneous clinical entities, with different therapeutic strategies and prognoses. Some, such as uncomplicated childhood osteomyelitis, are easy to treat, as short-course antimicrobial therapy without surgery is classically associated with excellent prognosis. In contrast, in some situations such as chronic implant-associated BJI, the pathogen is difficult to eradicate, leading to high rates of relapse and morbidity despite aggressive surgical strategy and prolonged intravenous antibiotic therapy. In such cases, team-work in tertiary care centers is required to determine optimal surgical management so as to limit treatment failure, motor disability and risk of amputation. The choice of antimicrobial therapy is also challenging, requiring consideration of: (i) the problem of bone diffusion [1]; (ii) the necessity of using antimicrobials active against bacterial biofilms [2]; (iii) the growing incidence of antibiotic resistance; and (iv) the high risk of severe adverse events (SAE) in response to first-line antimicrobials in these patients [3]. Consequently, off-label use of recently developed antimicrobials, such as daptomycin, is frequently required as salvage therapy in complex BJI.
Daptomycin is a cyclic lipopeptide with rapid bactericidal action against Gram-positive bacteria, and is approved for complicated skin and skin-structure infection (4 mg/kg/day intravenously) and Staphylococcus aureus bacteraemia and/or right-side endocarditis (6 mg/kg/d). Beyond these FDA and European-approved indications, daptomycin is increasingly used in BJI, as: (i) Gram-positive cocci are the most frequent pathogens in BJI; (ii) staphylococci exhibit growing resistance to beta-lactams and glycopeptides; (iii) a randomized controlled trial supported the use of daptomycin in these patients [4]. Consequently, daptomycin has been proposed as an alternative therapeutic option in patients with staphylococcus or enterococcus prosthetic joint infection in the recent Infectious Diseases Society of America (IDSA) guidelines (6 mg/kg/d) [5]. As bone penetration of daptomycin is limited, some authors proposed higher doses in BJI: i.e., 8 mg/kg/d [6]. This attitude is supported by the retrospective post-marketing Eu-CORE® study, but prospective data are lacking, especially in patients at high risk of relapse receiving prolonged daptomycin therapy [7].
In this context, the present cohort study aimed to assess the safety and efficacy of prolonged high-dose (>6 mg/kg/d) daptomycin salvage therapy in patients with complex BJI, focusing on daptomycin-related SAEs such as rhabdomyolysis or eosinophilic pneumonia, and to determine risk-factors for treatment failure.
Methods
We performed a cohort study including consecutive patients that have received daptomycin >6 mg/kg/d as alternative therapy for complex BJI from January 2011 to July 2013 in a French regional reference center. Patients with creatinine clearance <30 mL/min were excluded. Diagnosis of BJI was based upon clinical and/or imaging evidence, and culture of microorganisms from synovial fluid or periprosthetic tissue (more than two specimens for bacteria from skin flora: e.g., coagulase-negative staphylococci, Corynebacterium spp, Propionibacterium acnes). Infection was classified as “chronic” when there was a delay of one month between the bone contamination (previous surgery) and diagnosis. In line with the definition given by the Health-care Supply Office (Direction Générale de l’Offre de Soins, DGOS) of the French Health Ministry (Ministère des Affaires Sociales et de la Santé), BJI was considered complex in the following circumstances: (i) relapsing BJI; and/or (ii) intolerance to first-line antimicrobial therapy; and/or (iii) requirement of large bone resection and/or reconstruction; and/or (iv) multi-drug resistant pathogen limiting therapeutic opportunities, such as a glycopeptide-resistant Gram-positive isolate.
Susceptibility to glycopeptides and daptomycin was assessed in methicillin-resistant staphylococci based on the criteria of the European Committee on Antimicrobial Susceptibility Testing (EUCAST: Breakpoint tables for interpretation of minimum inhibitory concentrations [MICs] and zone diameters, version 4.0), if the strain was available at the time of daptomycin prescription. Notably, daptomycin MICs were determined by the E-test® method. In patients with implant-related infection, surgical treatment was considered optimal if based on French and IDSA guidelines: i.e., debridement-lavage and implant retention followed by antimicrobial therapy in acute infection, and implant removal (with or without reimplantation) followed by antimicrobial therapy in chronic infection. In patients with non-implant-related BJI, surgery was considered optimal when large debridement including bone resection was performed when required. Daptomycin was administered intravenously once daily by 30-min infusion.
All patients were scheduled for inclusion in the “safety analysis”. Only patients for whom at least two cultures were positive for Gram-positive micro-organisms from deep surgical specimens or joint-aspiration fluid were to be included in the “efficacy analysis”. The use of high doses of daptomycin entailed particular focus on daptomycin-related adverse events (AE), which were systematically collected and assessed on the Common Terminology Criteria for Adverse Events (CTCAE: version 3.0, published 9 August 2006). AEs were classified as mild (CTCAE stage 1), moderate (stage 2) or SAE (stages 3, 4 and 5). Standard biological testing, including blood creatine kinase (CK), was performed at least once a week. After October 2012, daptomycin trough plasma concentration (Cmin) was determined monthly for all patients, and additionally in case of AEs directly implicating daptomycin (i.e., at onset of elevated blood CK or of eosinophilic pneumonia), to detect any patients with daptomycin trough levels (Cmin) over 24 mg/L. Cmin was determined 24 h after daptomycin injection (just before reinjection, if performed) using a validated HPLC process developed in the laboratory and a diode array UV detector. Cmin > 24 mg/L was considered an overdose, as the risk of high CPK levels (with or without symptoms of myopathy) is greater above this threshold [8].
Treatment failure was defined as worsening or new clinical signs related to persistent and/or new infection at the BJI site. Treatment failure implicating daptomycin included relapse with the same Gram-positive strain, and super-infection due to another Gram-positive strain. Super-infection due to Gram-negative strains or fungi was not considered as treatment failure implicating daptomycin. Determinants of treatment failure were explored by univariate log-rank test and unadjusted Cox analysis. Statistical analysis used SPSS 17.0 software (SPSS Inc, Chicago, IL, USA). The research was conducted in accordance with the Declaration of Helsinki and national and institutional standards. The study received the approval of the French South-East II and III ethics committee with the reference number CAL2011-021 and n°QH 20/2014. In accordance with French legislation, written informed consent was not required for any part of the study, as (i) daptomycin was used as salvage therapy in the usual care of patients addressed to our regional reference center for complex BJI; (ii) patients were informed orally and by letter that data were being collected using a national database established by the DGOS (in line with ruling n°2012–220 of the French national data protection commission: Commission Nationale de l’Informatique et des Liberté). The study was registered to ISRCTN (number ISRCTN14244698).
Results
Baseline patient characteristics
During the study period, 43 complex BJIs were treated by daptomycin (>6 mg/kg/d) as salvage therapy in 42 patients. In 40 cases (93 %), osteomyelitis was diagnosed based on clinical signs: fistula (n = 26, 60 %), pain (n = 21, 49 %), inflammatory aspect (n = 17, 40 %), fever (n = 9, 21 %), abscess (n = 5, 12 %), osteoarthritis (n = 2, 5 %), or sepsis (n = 1, 2 %). Three patients (7 %) were asymptomatic: in 2 cases, daptomycin was prescribed for a super-infection documented on an explanted orthopaedic device; in the third, osteomyelitis was diagnosed from radiologic abnormalities.
Criteria for complexity were: (i) relapsing BJI in 27 patients (62 %); (ii) intolerance to first-line antimicrobial therapy in 42 (98 %); (iii) requirement of large bone resection and/or reconstruction in 37 (86 %); and (iv) infection with a glycopeptide-resistant Gram-positive strain in 22 (51 %). Glycopeptides were the most common prior treatment (n = 37, 86 %). The most common reason for discontinuing prior antibiotic therapy was the occurrence of a side-effect (n = 23, 53 %), including allergic reaction (n = 17, 40 %) and/or renal failure related to vancomycin overdose (n = 7, 16 %). Baseline characteristics are summarized in Table 1.
Table 1.
Demographic characteristics of 43 patients who received daptomycin-based antimicrobial therapy
| Characteristic | (n, %) |
|---|---|
| Gender | |
| Female | 18 (42) |
| Male | 25 (58) |
| Mean age, years (range) | 61 (18–88) |
| Age groups | |
| < 65 years | 25 (58) |
| ≥ 65–< 75 years | 8 (19) |
| ≥ 75 years | 10 (23) |
| Mean body weight, kg (range) | 75 (32–110) |
| Mean body mass index (range) | 27 (14–43) |
| BMI ≥ 25, < 30 | 9 (21) |
| BMI ≥ 30 | 14 (33) |
| Ethnicity (caucasian) | 42 (98) |
| Active smoking | 10 (23) |
| Underlying diseases | |
| Hypertension | 17 (40) |
| Diabetes mellitus | 5 (12) |
| Cardiovascular disease | 13 (30) |
| Cancer | 6 (14) |
| Creatinine clearance (MDRD) 30–60 mL/min | 3 (7) |
| Immunosuppression | 4 (9) |
| Mean ASA score (range) | 2.2 (1–4) |
| Past episode of BJI on the same site | 27 (63) |
| Anatomical site of infection | |
| Knee | 12 (28) |
| Hip | 9 (21) |
| Lower limb | 9 (21) |
| Rachis | 8 (19) |
| Upper limb | 2 (5) |
| Other | 1 (2) |
| Chronic osteomyelitis | 37 (86) |
| Physiopathology of osteomyelitis | |
| Post-operative | 41 (95) |
| Hematogenous infection | 2 (5) |
| Pressure ulcer | 2 (5) |
| Orthopedic device | |
| Prosthesis | 23 (53) |
| Osteosynthesis device | 14 (33) |
| None | 6 (14) |
| Previous exposition to antimicrobials for the index BJI before daptomycin prescription | |
| Glycopeptides | 37 (86) |
| Fluoroquinolones | 27 (63) |
| Rifampin | 25 (58) |
| Clindamycin, pristinamycin | 18 (42) |
| Piperacillin tazobactam | 15 (35) |
| Cephalosporins | 13 (30) |
| Fosfomycin | 13 (30) |
| Oxacillin, cloxacillin | 12 (28) |
| Aminoglycosids | 9 (21) |
| Fucidic acid | 7 (16) |
| Linezolid | 5 (12) |
| Others | 18 (42) |
Data are n (%) unless otherwise indicated
ASA American Society of Anesthesiologists, BJI Bone and joint infection, BMI Body mass index, MDRD Modification of the diet in renal disease
Microbiology and daptomycin prescription patterns
Culture results from deep samples included 33 bone samples (77 %), 5 joint aspirate samples (12 %), and 2 other deep samples (5 %). Coagulase-negative staphylococcus was implicated in 32 patients (74 %), S. aureus in 11 (26 %), P. acnes in 8 (19 %), Corynebacterium spp. in 4 (9 %) and Enterococcus in 3 (7 %). Five of these patients (12 %) were co-infected with Gram-negative bacilli, and 3 with fungi (8 %). Infection was polymicrobial in 23 cases (59 %). Twenty-seven of the 32 coagulase-negative staphylococci isolates (84 %) were methicillin-resistant; vancomycin MIC was >2 mg/L and equal to 2 mg/L in 10 (31 %) and 12 (39 %) isolates, respectively; and 18/32 (56 %) isolates were resistant to teicoplanin. Daptomycin E-test® results were available in 25 isolates among the methicillin-resistant strains (93 %): all were susceptible to daptomycin, with MIC values ranging from 0.064 to 1 mg/L (mean, 0.33 ± 0.27 mg/L).
In S. aureus, methicillin resistance was detected in 1 patient (9 %), with conserved susceptibility to glycopeptides, and daptomycin MIC of 0.125 mg/L.
Daptomycin was administered at doses ranging from 6.5–10 mg/kg/d (mean, 8 ± 0.9 mg/kg/d). Thirteen patients (30 %) received >8 mg/kg/d. Daptomycin was included in anti-Gram-positive combination therapy in 37 patients (86 %), most commonly associated with fosfomycin (n = 15, 35 %), rifampin (n = 9, 21 %) or clindamycin (n = 5, 12 %). Fourteen patients (33 %) received daptomycin treatment as outpatient parenteral antibiotic therapy.
Safety analysis
The primary reason for stopping daptomycin was completion of therapy (37 patients, 86 %). Mean treatment duration was 81 ± 59 days (range 6–303 days). During daptomycin-based antimicrobial therapy, 17 patients (40 %) experienced 26 AEs (Table 2). Eight patients (16 %) experienced mild AEs, 2 (5 %) moderate AEs and 6 (14 %) SAEs, none of which were life-threatening. AEs occurred after a mean 56 ± 48 days’ daptomycin therapy (range, 6–180 days). All 6 SAEs (Table 3) led to daptomycin withdrawal (Fig. 1). Three patients (7 %) experienced mild transient asymptomatic increase in CK; none were receiving statins. Three patients developed pneumonia, including two cases of certain eosinophilic pneumonia directly implicating daptomycin. These two patients had pulmonary infiltrates and bronchoalveolar fluid with eosinophils (35 % and 11 %, respectively; Fig. 2); of note, both were receiving more than 8 mg/kg/d daptomycin (8.4 and 8.7 mg/kg/d, respectively), and daptomycin Cmin > 24 mg/L was associated (Table 3). Cox univariate analysis and Kaplan Meier curves showing the cumulative probability of SAEs during daptomycin-based therapy showed no significant differences between patients receiving 6–8 mg/kg/d vs. > 8 mg/kg/d (Fig. 3, panel A). Daptomycin Cmin was assessed 52 times in 20 patients (47 %) after October 2012; 1 case showed daptomycin Cmin > 24 mg/L, with asymptomatic elevation of blood CK. Of note, asymptomatic transient daptomycin Cmin > 24 mg/L was detected in 3 other patients, without elevation of blood CK. Cmin was not significantly predictive of occurrence of SAE (6 events; HR, 1.092; 95 % CI, 0.950–1.254), whereas it was predictive of occurrence of mild to severe AEs (8 events; HR, 1.037; 95 % CI, 1.002–1.073).
Table 2.
Adverse events potentially related to the daptomycin-based antimicrobial therapy (n = 43) that occurred in 17 of the 43 included patients. Daptomycin dose is expressed in mg/kg/d. AEs onsets are notified in days
| Adverse events | n (%) | Daptomycin dose (mean, range) | AE onset (mean, range) | Daptomycin withdrawal | Companion drug withdrawal |
|---|---|---|---|---|---|
| Hematologic disorders | 12 (28) | 7,8 (7–9) | 44 (7–92) | 4/12 | 3/12 |
| Hypereosinophilia | 6 (14) | 7,8 (7–9) | 43 (10–92) | 3/6 | 1/6 |
| Neutropenia | 4 (9) | 7,8 (7–9) | 73 (49–88) | 1/4 | 2/4 |
| Increased blood CPK | 4 (9) | 7,5 (7–8) | 49 (9–92) | 2/4 | 2/4 |
| PICC thrombosis | 3 (7) | 8,3 (7–9) | 39 (12–79) | 1/3 | 0/3 |
| Hepatic disorders | 3 (7) | 8,2 (7,5–9) | 71 (13–112) | 0/3 | 1/3 |
| Eosinophilic pneumonia | 2 (5) | 8,5 (8–9) | 17 (6–23) | 2/2 | 1/1 |
| Increased blood creatinine | 1 (2) | 8 | 8 | 1 | 1 |
| Pancreatitis | 1 (2) | 8 | 180 | 0 | 1 |
AE, Adverse event, CK, Creatine kinase, PICC, Peripherally inserted central catheter
Table 3.
Serious adverse events (SAE) occurring in 6 patients under daptomycin-based antimicrobial therapy
| Patient | Dose (mg/kg/d) | Additional antibiotic | SAE | SAE onset (days) | Cmin at SAE onset (mg/L) | Daptomycin withdrawal | Companion drug withdrawal |
|---|---|---|---|---|---|---|---|
| 1 | 8,8 | Rifampicin* | Neutropenia | 73 | NA | Yes | Yes |
| 2 | 7,1 | Rifampicin | Hypereosinophilia | 92 | NA | Yes | No |
| 3 | 8,4 | Rifampicin | Eosinophilic pneumonia, rhabdomyolysis | 10 | 134 | Yes | Yes |
| 4 | 8,7 | Pristinamycin | PICC thrombosis | 12 | NA | Yes | No |
| 5 | 8,7 | None | Eosinophilic pneumonia | 23 | 38 | Yes | NA |
| 6 | 7,8 | Linezolid | Acute renal failure | 8 | NA | Yes | Yes |
In bold: SAE directly attributed to daptomycin
NA Not available, PICC Peripherally inserted central catheter, SAE Serious adverse event
*Rifampicin can induce both neutropenia and eosinophilia
Fig. 1.
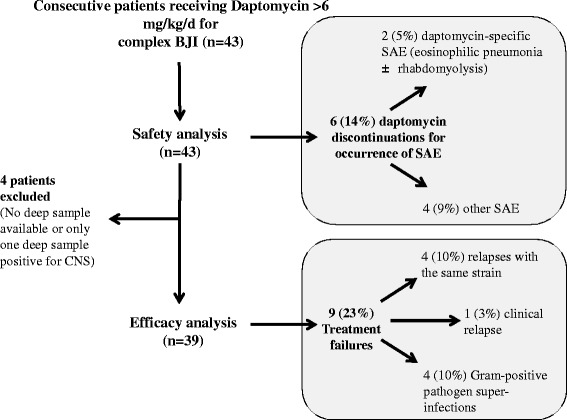
Flow chart of the cohort study. CNS, Coagulase negative staphylococci; SAE, Serious adverse event
Fig. 2.
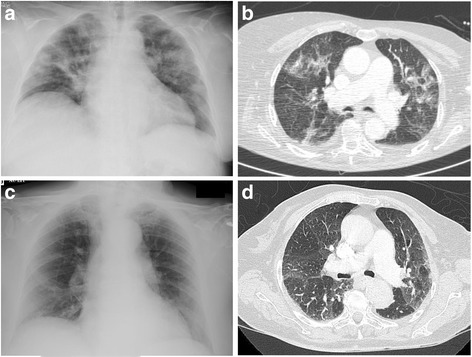
Chest X-ray (a, c) and computed tomography (b, d) for the two patients with eosinophilic pneumonia
Fig. 3.
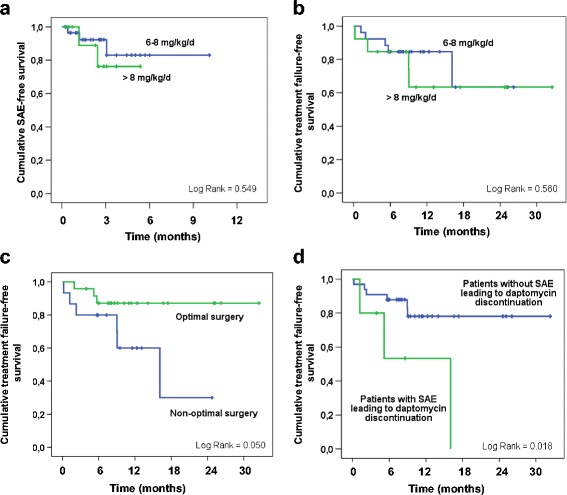
Risk factors for failure and for severe adverse event
Efficacy analysis
Four cases of osteitis were excluded from the efficacy analysis (Fig. 1). Two of the 39 patients included (5 %) underwent no surgery, because of severe underlying disease. Surgery was considered optimal in 24 patients (62 %). During follow-up (387 ± 243 days), treatment failure was recorded for 9 patients (23 %) (Fig. 1), all concerning implant-associated BJI. None of the strains involved developed daptomycin MIC elevation during the study period. All patients in whom daptomycin was discontinued experienced relapse. Univariate Cox analysis and Kaplan-Meier curves showed that dose exceeding 8 mg/kg/day was not associated with better outcome (Table 4; Fig. 3, panel B). Three factors were significantly associated with treatment failure: age (hazard ratio [HR], 1.89; 95 % confidence interval (CI), 1.03–3.47), non-optimal surgery (HR, 3.63, 95 % CI, 0.91–14.73) and SAE leading to daptomycin discontinuation (HR, 4.84; 95 % CI, 1.17–20.05) (Table 4; Fig. 3, panel C and D).
Table 4.
Cox univariate analysis showing variables associated with treatment failure during daptomycin-based antimicrobial therapy
| Variable | n (%) | unadjusted HR (95 % CI) | p-value |
|---|---|---|---|
| Age (per 10 years) | NA | 1.89 (1.03–3.47) | 0.041 |
| Male sex | 23 (59) | 1.48 (0.25–1.48) | 0.245 |
| Obesity | 12 (31) | 1.06 (0.93–1.06) | 0.932 |
| ASA score | NA | 1.11 (0.79–1.11) | 0.787 |
| Smoking | 13 (33) | 0.91 (0.23–3.65) | 0.896 |
| Implant associated BJI | 33 (85) | 27.8 (0.02–40422.69) | 0.371 |
| Chronic BJI | 5 (13) | 1.15 (0.14–9.22) | 0.894 |
| Fistula | 14 (36) | 2.94 (0.60–14.43) | 0.185 |
| Relapsing BJI | 15 (63) | 5.50 (0.69–44.02) | 0.108 |
| S. aureus | 11 (28) | 0.59 (0.12–2.89) | 0.517 |
| No or non-optimal surgery | 15 (38) | 3.63 (0.91–14.73) | 0.068 |
| Previous treatment with glycopeptides | 34 (87) | 25.47 (0.01–142518.48) | 0.462 |
| Glycopeptide-resistant isolate | 20 (51) | 2.965 (0.70–12.58) | 0.141 |
| Daptomycin ≤ 8 mg/kg/d | 26 (67) | 0.676 (0.18–2.55) | 0.563 |
| Daptomycin discontinuation for SAE | 6 (15) | 4.844 (1.17–20.05) | 0.029 |
ASA American Society of Anesthesiologists, BJI bone and joint infection, HR, hazard ratio, NA not applicable (continuous variable), SAE serious adverse events
Discussion
Despite its non-comparative, non-randomized, single-center design, this cohort study provides important data concerning off-label use of prolonged high-dose daptomycin therapy in complex BJI, reflecting the real-life use of daptomycin in a BJI referral center. Daptomycin therapy in patients with complex BJI shows a high rate of treatment success (77 %), despite the patient population being at high risk of relapse. Age, non-optimal surgery and daptomycin discontinuation for serious adverse events were the three determinants of treatment failure. Daptomycin was safe, but a higher incidence of eosinophilic pneumonia than expected was recorded, in contexts of daptomycin Cmin > 24 mg/L.
Daptomycin does not have approval for the treatment of BJI by the US and European authorities. However, based on retrospective data and one randomized controlled trial, it was proposed as an alternative option in patients with staphylococcus or enterococcus prosthetic joint infection in the recent IDSA guidelines, at the standard dose of 6 mg/kg/d [4, 5, 7]. Recent reports of poor daptomycin bone penetration encourage the use of higher doses [6]. In addition to these pharmacological studies, doses up to 8 mg/kg are supported by in vitro [9, 10] and in vivo studies [11–13] High doses have been described in retrospective studies [14–16], but prospective studies including patients receiving high doses of daptomycin are crucial to determine efficacy and safety in BJI.
Concerning safety, patients with BJI are particularly exposed to serious adverse events, as most antimicrobials are used in combination, at high doses and for several weeks or months [3]. In the present study, 40 % of patients experienced at least one AE during treatment, which is notably higher than in previous reports [7]. This difference can probably be explained by longer treatment duration (81 days, versus 28 days in the EU-CORESM database), as AEs occurred after a mean 56 days. Despite this high AE rate, only 6 patients experienced an SAE that led to daptomycin discontinuation, which is consistent with the 10 % rate of toxicity-related daptomycin withdrawal observed in a recent retrospective series of 20 patients [16]. Of note, 2 of the 6 presented confirmed eosinophilic pneumonia (5 % of patients), which is more than expected, as eosinophilic pneumonia is considered to be an infrequent daptomycin-related SAE: 0.5 % of patients receiving daptomycin in the retrospective post-marketing Eu-CORE® study experienced eosinophilic pneumonia, and a recent review of the literature reported only 24 published cases [17]. The pathophysiology of daptomycin-associated eosinophilic pneumonia is unclear, and it is unknown whether high doses of daptomycin might contribute to the occurrence of eosinophilic pneumonia. In vitro investigations suggest that hydrophilic proteins contained in the pulmonary surfactant (particularly surfactant protein C) bind to daptomycin, inhibit its antibacterial activity and facilitate the formation of surfactant aggregates [18]. The relation between eosinophilic pneumonia and daptomycin Cmin > 24 mg/L has to be explored, especially as there was daptomycin Cmin > 24 mg/L in both patients with eosinophilic pneumonia. Daptomycin Cmin > 24 mg/L in plasma may lead to drug accumulation in the alveolar spaces and induce formation of surfactant aggregates, followed by eosinophil recruitment in lung parenchyma.
Moreover, 6 patients are presented in Table 3 with serious adverse events: 4 of them with dose higher than 8 mg/kg and 2 of them with dose higher than 7 mg/kg. Variables associated with treatment failure did not include daptomycin dose lower than 8 mg/kg: regarding these data, we do not recommend to use doses higher than 8 mg/kg/d.
Concerning efficacy, there was a high success rate (77 %) in a population at high risk of failure, especially as most of our patients presented chronic relapsing implant-associated BJI. This rate is consistent with the 75 % clinical cure rate reported by Seaton et al. [7]. Of note, in the present study: (i) daptomycin was used as second-line antimicrobial therapy in patients often previously exposed to vancomycin; and (ii) half of the patients (22 patients, 51 %) were infected with Gram-positive pathogens with decreased susceptibility to glycopeptides (mostly teicoplanin-resistant coagulase-negative staphylococci, and 10 patients with vancomycin-resistant strains). These two conditions have been reported to facilitate acquisition of daptomycin-resistance during treatment in patients with persistent bacteraemia or endocarditis [19–21]. Of note, in the present series, patients experiencing treatment failure did not show acquired daptomycin-resistance.
In the present study, as in others, age emerged as a risk factor for treatment failure [22]. Interestingly, patients for whom daptomycin was withdrawn for SAE were also at higher risk of treatment failure. This is easily explained, inasmuch as daptomycin was mostly used as salvage therapy, and very few other treatment options were available for our patients. Finally, non-optimal surgery was also a risk factor for relapse, highlighting surgical management as the cornerstone of the treatment of complex BJI. For instance, in patients with chronic orthopaedic implant-associated infection, total removal of the implant is required to limit bacterial persistence [23]. Likewise, it is of the utmost importance to remove the cement in patients with cemented prosthesis joint infection. As removing the cement without inducing bone fracture is usually challenging, particular improved techniques, such as ultrasonic cement removal, are used in reference centers, limiting the need for osteotomy and preserving the bone stock that is essential for reconstruction and reimplantation [24].
Consequently, in case of difficult-to-treat BJI, in which relapse is associated with severe disabilities, the complex choice of aggressive surgical strategies and the difficult monitoring of off-label use of alternate therapies such as daptomycin fully justify management in a regional reference center. The French care network created in 2008 by the French Health Ministry (i.e., management of patients with complex BJI in one of the 9 approved regional reference centers, in collaboration with primary public or private-sector hospitals) may improve prognosis in one of the most difficult-to-treat bacterial infections.
Conclusion
In conclusion, prolonged high-dose daptomycin was associated with a high success rate in our cohort of patients with complex BJI, partly because antimicrobial therapy was associated with optimal surgery in a regional reference cente, which is essential for the prognosis of complex BJI. Daptomycin was safe, although there was a higher incidence of eosinophilic pneumonia than expected, surprisingly in patients with daptomycin Cmin > 24 mg/L. Based on our results, 8 mg/kg/d (and no more) seems to be the adequate dose of daptomycin for the treatment of BJI. Monitoring daptomycin levels seems important in patients receiving high-doses of daptomycin, to limit occurrence of adverse events.
Acknowledgements
This work was supported by the Lyon hospitals board (Hospices Civils de Lyon). Lyon Bone and Joint Infection Study Group (collaborators): Physicians – Tristan Ferry, Thomas Perpoint, André Boibieux, François Biron, Florence Ader, Julien Saison, Florent Valour, Fatiha Daoud, Johanna Lippman, Evelyne Braun, Marie-Paule Vallat, Patrick Miailhes, Christian Chidiac, Dominique Peyramond; Surgeons – Sébastien Lustig, Philippe Neyret, Olivier Reynaud, Caroline Debette, Anthony Viste, Jean-Baptiste Bérard, Frédéric Dalat, Olivier Cantin, Romain Desmarchelier, Michel-Henry Fessy, Cédric Barrey, Francesco Signorelli, Emmanuel Jouanneau, Timothée Jacquesson, Pierre Breton, Ali Mojallal, Fabien Boucher, Hristo Shipkov, Joseph Chateau; Microbiologists – Frederic Laurent, François Vandenesch, Jean-Philippe Rasigade, Céline Dupieux, Sophie Trouillet-Assant; Nuclear Medicine – Isabelle Morelec, Marc Janier, Francesco Giammarile; PK/PD specialists – Michel Tod, Marie-Claude Gagnieu, Sylvain Goutelle; Clinical Research Assistant – Eugénie Mabrut.
Abbreviations
- AE
adverse event
- BJI
bone and joint infection
- CK
creatine kinase
- Cmin
trough plasma concentration
- CTCAE
common terminology criteria for adverse events
- DGOS
Direction Générale de l’Offre de Soins
- EUCAST
European Committee on Antimicrobial Susceptibility Testing
- FDA
Food and Drug Administration
- HPLC
high performance liquid chromatography
- IDSA
Infectious Diseases Society of America
- MIC
minimum inhibitory concentration
- SAE
severe adverse event
Footnotes
Competing interests
SR, FV, JK, MCG, TP, SL, FA, BM, FL, CC have nothing to declare
TF participated to the Eucore study, and received travel grant by Novartis
Authors’ contributions
SR wrote the primary version of the manuscript and participated to the study design with TF; SR, FV, JK, TP, SL, FA, BM, CC and TF participate to the patient’s care and to the multidisciplinary meetings; MCG performed the dosage of daptomycin; FL participated to the multidisciplinary meeting and performed the bacteriological diagnosis of infection; All authors participated to the revision of the manuscript and approved the final version of the manuscript.
References
- 1.Landersdorfer CB, Bulitta JB, Kinzig M, Holzgrabe U, Sörgel F. Penetration of antibacterials into bone: pharmacokinetic, pharmacodynamic and bioanalytical considerations. Clin Pharmacokinet. 2009;48(2):89–124. doi: 10.2165/00003088-200948020-00002. [DOI] [PubMed] [Google Scholar]
- 2.Jacqueline C, Caillon J. Impact of bacterial biofilm on the treatment of prosthetic joint infections. J Antimicrob Chemother. 2014;69(Suppl 1):i37–40. doi: 10.1093/jac/dku254. [DOI] [PubMed] [Google Scholar]
- 3.Valour F, Karsenty J, Bouaziz A, Ader F, Tod M, Lustig S, et al. Antimicrobial-related severe adverse events during treatment of bone and joint infection due to methicillin-susceptible Staphylococcus aureus. Antimicrob Agents Chemother. 2014;58(2):746–55. doi: 10.1128/AAC.02032-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Byren I, Rege S, Campanaro E, Yankelev S, Anastasiou D, Kuropatkin G, et al. Randomized controlled trial of the safety and efficacy of Daptomycin versus standard-of-care therapy for management of patients with osteomyelitis associated with prosthetic devices undergoing two-stage revision arthroplasty. Antimicrob Agents Chemother. 2012;56(11):5626–32. doi: 10.1128/AAC.00038-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Osmon DR, Berbari EF, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis Off Publ Infect Dis Soc Am. 2013;56(1):e1–25. doi: 10.1093/cid/cis803. [DOI] [PubMed] [Google Scholar]
- 6.Montange D, Berthier F, Leclerc G, Serre A, Jeunet L, Berard M, et al. Penetration of daptomycin into bone and synovial fluid in joint replacement. Antimicrob Agents Chemother. 2014;58(7):3991–6. doi: 10.1128/AAC.02344-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Seaton RA, Malizos KN, Viale P, Gargalianos-Kakolyris P, Santantonio T, Petrelli E, et al. Daptomycin use in patients with osteomyelitis: a preliminary report from the EU-CORE(SM) database. J Antimicrob Chemother. 2013;68(7):1642–9. doi: 10.1093/jac/dkt067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bhavnani SM, Rubino CM, Ambrose PG, Drusano GL. Daptomycin exposure and the probability of elevations in the creatine phosphokinase level: data from a randomized trial of patients with bacteremia and endocarditis. Clin Infect Dis Off Publ Infect Dis Soc Am. 2010;50(12):1568–74. doi: 10.1086/652767. [DOI] [PubMed] [Google Scholar]
- 9.Parra-Ruiz J, Bravo-Molina A, Peña-Monje A, Hernández-Quero J. Activity of linezolid and high-dose daptomycin, alone or in combination, in an in vitro model of Staphylococcus aureus biofilm. J Antimicrob Chemother. 2012;67(11):2682–5. doi: 10.1093/jac/dks272. [DOI] [PubMed] [Google Scholar]
- 10.Parra-Ruiz J, Vidaillac C, Rose WE, Rybak MJ. Activities of high-dose daptomycin, vancomycin, and moxifloxacin alone or in combination with clarithromycin or rifampin in a novel in vitro model of Staphylococcus aureus biofilm. Antimicrob Agents Chemother. 2010;54(10):4329–34. doi: 10.1128/AAC.00455-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.John A-K, Baldoni D, Haschke M, Rentsch K, Schaerli P, Zimmerli W, et al. Efficacy of daptomycin in implant-associated infection due to methicillin-resistant Staphylococcus aureus: importance of combination with rifampin. Antimicrob Agents Chemother. 2009;53(7):2719–24. doi: 10.1128/AAC.00047-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Garrigós C, Murillo O, Lora-Tamayo J, Verdaguer R, Tubau F, Cabellos C, et al. Fosfomycin-daptomycin and other fosfomycin combinations as alternative therapies in experimental foreign-body infection by methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother. 2013;57(1):606–10. doi: 10.1128/AAC.01570-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Murillo O, Garrigós C, Pachón ME, Euba G, Verdaguer R, Cabellos C, et al. Efficacy of high doses of daptomycin versus alternative therapies against experimental foreign-body infection by methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother. 2009;53(10):4252–7. doi: 10.1128/AAC.00208-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gallagher JC, Huntington JA, Culshaw D, McConnell SA, Yoon M, Berbari E. Daptomycin therapy for osteomyelitis: a retrospective study. BMC Infect Dis. 2012;12:133. doi: 10.1186/1471-2334-12-133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Avery LM, Steed ME, Woodruff AE, Hasan M, Rybak MJ. Daptomycin-nonsusceptible vancomycin-intermediate staphylococcus aureus vertebral osteomyelitis cases complicated by bacteremia treated with high-dose daptomycin and trimethoprim-sulfamethoxazole. Antimicrob Agents Chemother. 2012;56(11):5990–3. doi: 10.1128/AAC.01046-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lora-Tamayo J, Parra-Ruiz J, Rodríguez-Pardo D, Barberán J, Ribera A, Tornero E, et al. High doses of daptomycin (10 mg/kg/d) plus rifampin for the treatment of staphylococcal prosthetic joint infection managed with implant retention: a comparative study. Diagn Microbiol Infect Dis. 2014;80(1):66–71. [DOI] [PubMed]
- 17.Phillips J, Cardile AP, Patterson TF, Lewis JS., 2nd Daptomycin-induced acute eosinophilic pneumonia: analysis of the current data and illustrative case reports. Scand J Infect Dis. 2013;45(10):804–8. doi: 10.3109/00365548.2013.805427. [DOI] [PubMed] [Google Scholar]
- 18.Silverman JA, Mortin LI, Vanpraagh ADG, Li T, Alder J. Inhibition of daptomycin by pulmonary surfactant: in vitro modeling and clinical impact. J Infect Dis. 2005;191(12):2149–52. doi: 10.1086/430352. [DOI] [PubMed] [Google Scholar]
- 19.Gasch O, Camoez M, Domínguez MA, Padilla B, Pintado V, Almirante B, et al. Emergence of resistance to daptomycin in a cohort of patients with methicillin-resistant Staphylococcus aureus persistent bacteraemia treated with daptomycin. J Antimicrob Chemother. 2014;69(2):568–71. doi: 10.1093/jac/dkt396. [DOI] [PubMed] [Google Scholar]
- 20.Van Hal SJ, Paterson DL, Gosbell IB. Emergence of daptomycin resistance following vancomycin-unresponsive Staphylococcus aureus bacteraemia in a daptomycin-naïve patient--a review of the literature. Eur J Clin Microbiol Infect Dis Off Publ Eur Soc Clin Microbiol. 2011;30(5):603–10. doi: 10.1007/s10096-010-1128-3. [DOI] [PubMed] [Google Scholar]
- 21.Tenover FC, Sinner SW, Segal RE, Huang V, Alexandre SS, McGowan JE, Jr, et al. Characterisation of a Staphylococcus aureus strain with progressive loss of susceptibility to vancomycin and daptomycin during therapy. Int J Antimicrob Agents. 2009;33(6):564–8. doi: 10.1016/j.ijantimicag.2008.12.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mackintosh CL, White HA, Seaton RA. Outpatient parenteral antibiotic therapy (OPAT) for bone and joint infections: experience from a UK teaching hospital-based service. J Antimicrob Chemother. 2011;66(2):408–15. doi: 10.1093/jac/dkq445. [DOI] [PubMed] [Google Scholar]
- 23.Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. N Engl J Med. 2004;351(16):1645–54. doi: 10.1056/NEJMra040181. [DOI] [PubMed] [Google Scholar]
- 24.Fletcher M, Jennings GJ, Warren PJ. Ultrasonically driven instruments in the transfemoral approach--an aid to preservation of bone stock and reduction of implant length. Arch Orthop Trauma Surg. 2000;120(10):559–61. doi: 10.1007/s004020000176. [DOI] [PubMed] [Google Scholar]