

Abstract
Adrenal cysts are rare and should be considered in the differential diagnosis of retroperitoneal cysts. We present a case of a huge adrenal cyst displacing the right kidney anteriorly toward the left side in a young female.
Key words: Benign adrenal cyst, giant adrenal cyst, retroperitoneal cysts
INTRODUCTION
Cystic lesions of the adrenal gland are rare. They may be true cyst, infectious cyst, malignancy with cystic degeneration or pseudocyst.[1] It can be correctly diagnosed by pathological examination. We present an interesting case of symptomatic giant adrenal cyst in a young female.
CASE REPORT
A 26-year-old female was admitted with a history of mass in the right upper abdomen associated with abdominal discomfort for 3 months. The patient's physical examination revealed a huge non-tender lump in the right upper quadrant of the abdomen. The ultrasound of the abdomen showed a huge cyst in the right upper quadrant. Contrast-enhanced computerized tomography [Figures 1 and 2] revealed a biloculated hypodense cystic lesion of 23 cm × 13 cm size in the right renal bed with moderately enhancing thick septa and indicated no evidence of a solid component. The lesion displaced the right kidney across the midline toward the left side, probably because of its large size. As the origin of the lesion was uncertain, the patient underwent an exploratory laparotomy which revealed a large cyst arising from the right adrenal gland. During the dissection, the cyst ruptured, revealing several liters of clear fluid. A complete cyst excision with right adrenalectomy was performed. The post-operative period was uneventful. Histologically, the cyst wall had an endothelial lining and multiple nodular areas, showing adrenal cortical tissue, which suggested a diagnosis of benign adrenal cyst. The patient was followed-up for the past 6 months and showed no other symptoms.
Figure 1.
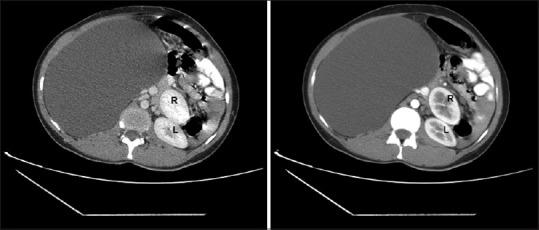
Computerized tomography showing a large retroperitoneal cyst displacing the right kidney anteriorly toward the left side
Figure 2.

Computerized tomography with coronal reconstruction showing a large retroperitoneal cyst displacing the right kidney
DISCUSSION
Retroperitoneal cystic masses are difficult to diagnose and treat. Pre-operative workup should include careful history taking, laboratory investigations and radiography, not least computerized tomography.[1] Even with the use of multiple diagnostic modalities, the organ of origin of many cystic lesions cannot be diagnosed pre-operatively. The differential diagnosis of retroperitoneal cysts would include a large variety of neoplastic lesions (cystic lymphangioma, mucinous cystadenoma, cystic teratoma, cystic mesothelioma, Müllerian cyst, epidermoid cyst, bronchogenic cyst, cystic change in solid neoplasms, pseudomyxoma retroperitonei) and non-neoplastic lesions (pancreatic pseudocyst, non-pancreatic pseudocyst, lymphocele, urinoma, hematoma).[2]
The adrenal cyst is a rare disease that represents approximately 5% of incidentally discovered adrenal lesions. Most commonly, these cysts present in the fourth/fifth decades of life. Adrenal cysts should be included in the differential diagnosis of cystic abdominal lesions and, when suspected, the functional status may need to be verified by screening for urinary catecholamines and/or metanephrines.[3] In the current case, functional studies were not performed as the patient was asymptomatic. But, one cannot rely on the symptoms alone for ruling out hormonally active adrenal enlargement.[4]
Enucleation with preservation of the adrenal gland is the procedure of choice for benign adrenal cysts. En bloc adrenalectomy with cyst resection is the appropriate procedure in cases of malignancy;[1] however, due to diagnostic uncertainty, cyst excision with right adrenalectomy was performed in this case.
Histopathological examination is required to establish the definitive diagnosis. Pre-operative diagnosis of malignant lesions is essential as malignancy occurs in 7% of all adrenal cystic lesions.[5] In conclusion, adrenal cysts should be considered in the differential diagnosis of retroperitoneal cysts and computerized tomography is the imaging modality of choice for the primary evaluation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Davenport M, Pollard K, Smith SE, MacMahon MJ. Adrenal cysts-report, review and classification. Postgrad Med J. 1988;64:71–3. doi: 10.1136/pgmj.64.747.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yang DM, Jung DH, Kim H, Kang JH, Kim SH, Kim JH, et al. Retroperitoneal cystic masses: CT, clinical and pathological findings and literature review. Radiographics. 2004;24:1353–65. doi: 10.1148/rg.245045017. [DOI] [PubMed] [Google Scholar]
- 3.Sioka E, Symeonidis D, Chatzinikolaou I, Koukoulis G, Pavlakis D, Zacharoulis D. A giant adrenal cyst difficult to diagnose except by surgery. Int J Surg Case Rep. 2011;2:232–4. doi: 10.1016/j.ijscr.2011.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bittner JG, 4th, Brunt LM. Evaluation and management of adrenal incidentaloma. J Surg Oncol. 2012;106:557–64. doi: 10.1002/jso.23161. [DOI] [PubMed] [Google Scholar]
- 5.Kini JR, Gautam K, Augustine A. Adrenal gland cyst: A diagnostic conundrum: Report of a case with review of literature. J Med Soc. 2014;28:123–4. Available from: http://www.jmedsoc.org/textasp?2014/28/2/123/141107 . [Google Scholar]