

Abstract
This study, using secondary data analysis, examined a mediation model of acculturation and ethnic pride as predictors of physical and mental health outcomes in a sample of 561 Mexican American women. Factors postulated as mediators were family support and religiosity. Systematic across-group comparison analyses were conducted to examine sources of differences in the mediation model between immigrant and non-immigrant women. The results partially supported the hypothesized mediation model, indicating that family support, but not religiosity, was a significant mediator in the relationship between ethnic pride and mental health problems. In addition, as differences between immigrant and non-immigrant women were observed only in the variables means, but not in the factor loadings or regression paths, the model tested may capture a common psychosocial process that affects these women and their health outcomes. Overall, this study offers important implications for future research and the design of intervention programs for Mexican American women.
Keywords: Mexican American women, Acculturation, Ethnic pride, Health outcomes, Health disparities, Mediation processes
Introduction
The physical and psychological well-being of ethnic minorities is a major public health concern in the United States (DHHS 2004). Recent DHHS (2004) reports have documented pervasive health disparities for ethnic minority groups and the presence of large gaps in information regarding these groups. Among them are Hispanics or Latina/os1 who constitute the largest ethnic minority population in the United States, and within this population, Latina/os of Mexican heritage represent the largest subgroup (US Census Bureau 2003). Mexicans and Mexican Americans,2 particularly immigrants, have received considerable attention from social scientists in recent years, but more specific information is needed to understand their adjustment experiences, especially those of Mexican American women in non-clinical settings, a much understudied sub-population. The present study consists of a secondary data analysis that examined a mediation model of the relationships of acculturation and ethnic pride to physical and mental health outcomes among immigrant and non-immigrant Mexican American women. More research on the acculturative and adjustment experiences of Mexican American women would contribute to our overall understanding of their life experiences and more generally of the life experiences of ethnic minority women. Furthermore, such research would help identify potential within-group differences among Mexican American women, which would provide important information regarding the unique experiences of immigrant and non-immigrant women.
Mexican American Population
The most recent US census report (2005a, b) showed that about two in three Latina/os living within the United States are of Mexican heritage, constituting 9% of the total American population. Among Mexican Americans, two in five are foreign-born, and women comprise 47% of the Mexican American population (US Census Bureau 2000). It is important to recognize the diversity that exists among Mexican Americans, especially with regard to gender and immigrant status. Moreover, health disparities not only occur between different ethnic groups but also within each group, and these disparities particularly affect women and immigrants (Zambrana and Dill 2006). This is especially true for Mexican American women, both of immigrant and non-immigrant backgrounds (DHHS 2004).
Theories and Measurement of Acculturation
Attention to cultural factors is essential in research with ethnic minority populations, especially for those of immigrant background (Castro and Hernandez-Alarcon 2002). One prominent factor in such research is acculturation. Acculturation is a process of change that occurs when groups and individuals from different cultures come into continuous contact with one another (Marin and Gamboa 2003; Redfield et al. 1936). Such acculturative changes may be reflected in behavior, language, values, and identity and may vary according to certain demographic variables, such as age, educational level, and generational status (Lara et al. 2005).
Changes associated with the acculturative experience often involve stress, which can lead to distress (Cervantes et al. 1991). Stress plays a prominent role in the acculturation process as immigrants/ethnic minorities confront new or dominant cultural demands and attempt to cope with significant life changes (Berry 2003). Acculturative stress may be intensified for undocumented immigrants who also have to worry about their “illegal” status and the ramifications of “criminal” arrest and deportation. For all immigrants, the stress experienced during the acculturation process can impact psychological and social dimensions of adaptation. Consistent with the notion that stress operates as a major component of the acculturation process, the stress-process model (Pearlin et al. 1981) provides a framework for investigating acculturation and other cultural variables. The stress-process model suggests that primary stressors can lead to secondary stressors, and that both can have direct and indirect (i.e., mediating processes) effects on psychological and/or physiological outcomes. The stress-process model also recognizes the effects of certain demographic variables, such as age and education, in influencing the type and degree of stress experienced by various individuals. According to the stress-process model, the acculturation experience can be conceptualized as a primary social stressor, which can lead to secondary stressors (e.g., intrapersonal and interpersonal conflicts), and that both primary and secondary stressors can directly and/or indirectly impact physical and mental health outcomes.
In previous research, the assessment of acculturation has been based on either the unidimensional model or the bidimensional model (Marin and Gamboa 1996; Rogler et al. 1991). Although the latter is considered in recent years a more advanced approach in acculturation research (Abe-Kim et al. 2001), most previous studies have used the former model. The main criticism of the unidimensional model of acculturation is that it only attends to the degree of immersion in or assimilation to the host or dominant culture (the term “acculturation level”3 is commonly used to describe this linear progression), whereas the bidimensional model attends to the degree of immersion in the host culture (acculturation) as well as the degree of immersion in the culture-of-origin (enculturation), allowing for an assessment of biculturalism and acculturation strategies or modes—assimilation, integration, separation, and marginalization (Berry 2003). The bidimensional model is an improvement from the unidimensional model, but not without criticisms (Rudmin 2003).
Regardless of the type of assessment that was used, acculturation has been shown to be an important variable in the study of physical and mental health outcomes among immigrants and ethnic minorities (Chun et al. 2003). However, in previous research with Latina/o samples as well as with other ethnic minority groups, findings for acculturation have been generally mixed (Hunt et al. 2004). For instance, in a review of the literature on the relationship between acculturation (unidimensional/proxy assessment; e.g., immigrant or generational status) and mental health outcomes across 30 studies with Latina/o samples (17 of these 30 studies focused on Mexican Americans) published between 1967 and 1989, Rogler and colleagues (1991) discovered that the number of studies that supported a positive relationship (12) was about the same as those that supported a negative relationship (13). They concluded that the mixed findings were mostly due to differences in research methodologies, particularly differences in the conceptualization and assessment of acculturation. The mixed findings may also be due to differences in the demographic characteristics of the study samples across the 30 studies, which included participants selected from inpatient or outpatient settings as well as participants recruited from non-clinical populations who varied in Latina/o ethnicity, socioeconomic status, age, gender, and so on. While the true impact of acculturation on health-related outcomes remains unclear, subsequent research with Latina/o samples is showing a somewhat more consistent pattern which suggests a positive relationship between acculturation (unidimensional measure) and mental health problems (mood and anxiety disorders, substance abuse and dependence), and this appears to be the case for Mexican Americans as well (Castro et al. 1999b; Shrout et al. 1992; Vega et al. 1998). A similar pattern of findings has emerged for physical health outcomes in research with ethnic minority populations (Flack et al. 1995). For example, previous studies have shown a positive relationship between acculturation (as defined by immigrant status) and poor health, such as diabetes and dementia, among ethnic minority adults (Graves et al. 1996; Huang et al. 1996).
Importance of Ethnic Pride
Ethnic pride is another important cultural factor that should be considered in research with ethnic minority populations. Ethnic pride reflects positive feelings of connectedness and belongingness with regard to an individual’s ethnic/cultural background, identity, and/or group. Ethnic pride is similar to or synonymous with the construct of “collective self-esteem” (Alvarez and Helms 2001), which has been defined as how one feels about being a member of one’s racial or ethnic group. These positive emotions and attitudes towards one’s ethnic background can facilitate a positive self-concept and optimism towards the future (Tugade and Frederickson 2004), which can influence an individual’s sense of well-being (Izard 2002).
Although research on the relationship of ethnic pride to physical and mental health outcomes is limited, especially for Latina samples, existing studies with other ethnic minority or youth populations suggest the beneficial effects of ethnic pride on certain psychosocial and behavioral outcomes. For example, in an epidemiological study of 2,109 Filipino American adults, a strong sense of ethnic pride and intra-cultural group commitment were associated with fewer depressive symptoms (Mossakowski 2003). For African American children, ethnic pride was positively associated with academic achievement, as measured by grades and standardized test scores (Smith et al. 2003). In another study that involved ethnically diverse adolescents, including Mexican Americans, greater ethnic pride was negatively associated with drug use and exposure (Marsiglia et al. 2001). Austin (2004) also examined ethnic pride in a sample of Native Hawaiian adults and found that those with stronger ethnic pride were less likely to be perpetrators or victims of violence. Although little is known about the effects of ethnic pride in the lives of Mexican American women, findings from previous research, across different ethnic groups and outcomes, suggest the importance of this factor, which should be considered in conjunction with acculturative variables when examining health-related outcomes. Therefore, the present study also includes an assessment of ethnic pride in addition to acculturation.
Importance of Interpersonal and Intrapersonal Mediators
As suggested by Rogler and colleagues (1991), as well as other social scientists (e.g., Zane and Mak 2003), the mixed findings in research on acculturation may be partly a result of differences in methodology and study samples. Most previous research has tended to only examine the direct relationship of acculturation or other culturally related factors to specific outcomes, without considering other potentially important variables, including those that can operate as mediators (Castro and Hernandez-Alarcon 2002). Given that acculturation is a dynamic phenomenon that can impact both social and personal dimensions, certain interpersonal and intrapersonal variables may play important mediating roles in the prediction of physical and/ or mental health outcomes. The inclusion of mediators in the investigation of acculturation and ethnic pride as predictors of health outcomes would provide a more complex and more complete understanding of the collective impact of these factors in the lives of Mexican American women.
One potentially significant interpersonal mediator that may be related to health-outcomes is family support. The family is the centerpiece in the lives of most individuals, across all ethnic groups. However, for many individuals of immigrant background, especially those having limited social networks, the family may take on greater importance. Furthermore, stressors associated with acculturative experiences can exert a negative impact on the family and can undermine existing familial support (Dinh and Nguyen 2006; Prilleltensky 1993). For instance, acculturative stress as experienced by individual family members has been associated with a lower level of family cohesion in Latina/o families (Gil and Vega 1996). The impact of acculturation on immigrant families may, in turn, have a negative effect on coping capacity and adjustment. For instance, previous research showed that poor family emotional support was associated with symptoms of depression among Mexican immigrant women (Vega et al. 1991). Family factors (e.g., disrupted family systems, health practices of family members) also have been associated with poor physical health (Bagley et al. 1995), as well as health risk behaviors, such as alcohol, cigarette, and illicit drug use (Myers et al. 1995; Yee et al. 1995). Overall, these findings suggest that family factors, including family support, may play a significant mediating role in the relationship of acculturation or other cultural factors to health outcomes.
One potentially significant intrapersonal mediator is religiosity, which encompasses religious activities or practices and faith in a supreme being. Religion is an important aspect in the lives of many individuals, especially among Latina/os, of which 93% self-identify as Christian (Murray 2006). Nonetheless, the degree of religiosity can be influenced by the acculturation experience, as indicated by a previous study that showed a negative relationship between acculturation (as measured by preferred language use—Spanish or English) and personal religiosity among Latinas living in the United States (Pena and Frehill 1998). Previous research also has shown some positive effects of religiosity on specific dimensions of well-being, such as a lower level of suicidality (O’Donnell et al. 2004), a higher level of academic achievement (Jeynes 2003), and better physical health (Meadows et al. 2001). These findings raise a question about the process of acculturative change among Latinas—if religiosity confers Latinas with beneficial effects, but is then attenuated by increasing degree of immersion in host/dominant culture, does this imply a reduction in well-being among Latinas with increasing levels of acculturation? Therefore, religiosity may operate as another important mediator in the relationship of acculturation and ethnic pride to physical and mental health outcomes.
Attention to Demographic Characteristics
While more and more research is being conducted with Latina/o populations, much remains unknown regarding the effects of acculturation and other cultural factors on physical and mental health outcomes among Mexican American women, and whether these effects differ between immigrant and non-immigrant women. Immigrant status is a key demographic characteristic that may moderate the effects of acculturation on specific outcomes (Zambrana et al. 1997). Other demographic characteristics, such as age and education, also should be considered as they can provide additional contextual understanding of the life experiences of Mexican American women (Castro et al. 1999a).
Purpose of the Present Study
The primary purpose of this study was to examine a multivariate mediation model of the relationships of acculturation and ethnic pride to physical and mental health problems among immigrant and non-immigrant Mexican American women. The mediators were family support and religiosity. In addition, demographic variables of age and education were considered in the mediation model. Using structural equation modeling (SEM), the hypothesized mediation model was tested overall with both immigrant and non-immigrant women. In addition, systematic across-group comparison analyses of factor loadings, variable means, and regression paths were conducted to ascertain differences between immigrant and non-immigrant women. It was hypothesized that acculturation (based on the unidimensional model) and ethnic pride would have significant direct and indirect (mediating) effects on physical and mental health status. Specifically, acculturation would be positively associated with physical and mental health problems, whereas ethnic pride would be negatively associated with these same outcomes. Acculturation was hypothesized to be negatively associated with family support and religiosity, indicating that greater acculturation erodes the traditional cultural expressions of family support and religiosity for Mexican American women. By contrast, ethnic pride was hypothesized to be positively associated with these mediators, indicating that greater ethnic pride may be associated with, or otherwise contribute to stronger expressions of family support and religiosity. Family support and religiosity, in turn, were expected to be negatively associated with physical and mental health problems. That is, family support and religiosity may operate as cultural protective factors that enhance well-being. Finally, also using SEM, it was hypothesized that the variable means and regression paths within the mediation model would be significantly different between immigrant and non-immigrant women, suggesting that these two subpopulations of Latinas undergo different acculturative experiences based on their US-born/foreign-born status.
Method
Participants
Participants in this secondary data analysis study were part of a larger study of Latinas from a large metropolitan area in the Southwest region of the United States. From the original sample (N = 671), 561 women (286 immigrants; 275 non-immigrants) of Mexican descent who had complete data for all variables in this study were included in the analysis. These women were part of a random selection of membership rosters from each of the 14 churches that agreed to participate in the Compañeros en la Salud health promotion program. During the first year of this program, a total of 14 local churches were recruited as program sites. In a randomization procedure that involved stratification by church size, 7 churches were randomized into the Cancer Prevention Intervention and 7 churches were randomized into the Family Mental Health Comparison Group. Further detail on these churches and recruitment strategies is available in the research report by Castro et al. (1995). The data examined in the present study is from the baseline telephone survey, which was conducted prior to the respective interventions.
The mean age within the study sample of 561 Mexican American women was 43 (SD = 14.50), ranging from 18 to 84. The distribution for educational levels included 4.6% no education, 6.8% completed 3rd grade, 15% completed 6th grade, 8.7% completed 7th or 8th grade, 9.3% completed 9th or 10th grade, 33.5% completed 11th or 12th grade, 14.8% completed 2 years of community college, 6% completed 4 year college, 0.9% completed master’s program, and 0.4% completed doctorate program. Level of education was measured as the highest level of education attained, based on educational attainment in the native country (mostly applicable to immigrant women) and also in the United States. Among the women, 70.6% reported being currently married, 10% separated/divorced, 7.1% widowed, 6.8% never married, and 5.5% other.
Procedure
The telephone survey, using a structured interview format, was conducted by trained interviewers. The principal investigator and project director of the Compañeros en la Salud health promotion program (Castro et al. 1995) provided training to a cohort of bilingual/bicultural university undergraduate and graduate student research assistants in the conduct of telephone survey methodology, which included a series of role playing sessions to help interviewers gain skills in establishing rapport and adhering to interviewing and research protocols. Interviewers also gained skills in conducting the initial screening for eligibility as well as learning the details in scheduling interviews and follow-up calls and in data collection and data entry.
Once screened for eligibility, each woman was read a paragraph providing informed consent information that participation would be voluntary, that the respondent could terminate the interview at any time, and that participant’s information would be confidential and not be shared with any governmental agency or other organization. The participants were advised that a supervisor would be checking for completeness of interview, and that incomplete interviews would require a brief return call. The telephone interview had a mean duration time of 47 min, with most interviews ranging from 35 to 55 min long. A few interviews were conducted in two, or up to three sessions, as some women needed to end the interview temporarily to attend to household or child care duties.
The telephone survey included questions that asked about general physical health status, nutrition, general and specific cancer issues, religiosity, depression, family issues, acculturation, and demographic information. Respondents had the option to choose either the English language or Spanish language version of the interview. The original survey was developed in English, translated into Spanish, and back-translated into English by separate translators. Members of the Compañeros research team reviewed drafts of both versions concurrently for sources of non-equivalence. In addition, the wording was modified as needed with attention to the low literacy levels of many Latinas in the local community. Attention also was given to local forms of usage in Spanish. As a step towards local adaptation, a semi-final version of the interview was given to each of the 30 lay health workers (Promotoras), who were members of the Compañeros project, for their feedback with regard to readability, content, and clarity. All this feedback was used to generate the final version, which was pilot-tested with 6 women who were not part of the study, to test for length of administration time and other potential sources of difficulty. In this study, 55.6% of the women chose to respond to the telephone survey in Spanish whereas 44.4% chose to respond in English.
Instruments
Acculturation
Three items were used as measures of acculturation in this study. These items were drawn from the General Acculturation Index (Balcazar et al. 1995; Castro et al. 1999b), and variants of these items are typically included in lengthier acculturation scales and are highly correlated with these scales (e.g., Cuellar et al. 1995a, 5b; Norris et al. 1996). Of the three items, one assessed for language proficiency: “I speak:” followed by a 5-point response scale, ranging from “Only Spanish,” to “Only English.” The second item assessed for country of residence while growing up: “My childhood from infancy to 21 years was spent:” followed by a 5-point response scale ranging from “only in Mexico/Latin America” to “only in the United States.” The third item assessed for ethnic peer/friendship affiliation: “Currently my circle of friends are:” followed by a 5-point response scale ranging from “almost exclusively Mexicans/Hispanics” to “almost exclusively Anglo-Americans.” Because the items were based on the unidimensional model of acculturation, higher scores represented higher degrees of acculturation (i.e., higher levels of immersion in or assimilation to host/dominant culture). These three items were used as indicators of the latent construct of acculturation in the hypothesized mediation model and have a Cronbach’s alpha of .90.
Ethnic Pride
One item was used as a measure of ethnic pride, which included the statement, “In relation to my Mexican/Hispanic background, I feel: (1) no pride, (2) little pride, (3) somewhat proud, (4) proud, or (5) very proud.” This item represented an observed variable in the hypothesized mediation model.
Family Support
Four items were used as a measure of family support concerning health care. These items assessed for the frequency of caring support as provided by a spouse or other family members, and these would typically be regarded as helpful and likely stress-reducing actions, rather than as sources of stress and conflict. Examples included, “my spouse/family is there to help me whenever I’m concerned about my health” and “a member of my family spends time caring for me when I’m ill,” followed by a 5-point response scale ranging from “never” to “always.” While these items specifically asked about family support with regard to health care they also may have reflected the general level of family support as experienced by the participants. Thus, the four items were used as indicators of the latent construct of family support in the hypothesized mediation model, with a Cronbach’s alpha of .86.
Religiosity
Two items were used as measures of participants’ religiosity, which included their frequency in church/mass attendance and involvement in church activities, such as prayer group and Bible study. A religiosity index score was created based on the z-scores of these two items and was included as an observed variable in the hypothesized mediation model. A higher score indicated a higher level of religiosity.
Mental Health Status
In this study, measures of depression and life dissatisfaction were used as indicators of the latent factor for mental health status in the hypothesized mediation model. One of two available measures of depression was the Beck Depression Inventory-Short Form (BDI-SF) (Beck et al. 1988), which is based on the original 21-item BDI (Beck et al. 1961). The original BDI has demonstrated good convergent and discriminant validity in diverse samples, including Spanish-speaking participants (Bonicatto et al. 1998). The BDI-SF is a 13-item measure that taps into symptoms of depression, such as feelings of hopelessness and sadness, and loss of interest in normal activities. The BDI-SF is highly correlated with the original BDI (correlations ranged from .89 to .97) and has demonstrated sufficient internal consistency, ranging from .73 to .92. In this study, the Cronbach’s alpha for the BDI-SF was .83.
The other available measure of depression was the Center for Epidemiological Studies-Depression (CES-D) scale (Radloff 1977). It is a 20-item measure, utilizing a 4-point response scale, ranging from (1) “rarely or none of the time” to (4) “most or all of the time.” Sample items include: “I felt fearful,” “I enjoyed life,” and “I had crying spells.” The CES-D scale has been shown to exhibit good internal consistency (α = .86) across diverse populations and relatively good short-term test–retest reliability (Orme et al. 1986). In this study, the Cronbach’s alpha for the CES-D was .88.
In addition to the depression measures, an assessment of life satisfaction was included in this study as another indicator of mental health status. A 10-item scale was developed for the original survey to assess the degree of satisfaction in areas of self perception and interpersonal/social relations. Examples of items include “How satisfied are you with your sense of self,” “How satisfied are you with your ability to handle stressful situations,” and “How satisfied are you with your social poise, confidence with others.” A 5-point response scale accompanied each item, ranging from (1) “very dissatisfied” to (5) “very satisfied.” This 10-item scale showed good internal consistency with a coefficient alpha of .84 for this study sample. To align this life satisfaction scale with the two depression scales used in this study and as required in SEM statistical methodology, we reversed the polarity of this scale to produce a score for life dissatisfaction.
Physical Health Status
Two items were used as measures of participants’ general physical health status, which included “Would you say your health, in general, is poor, fair, good, or excellent?” and “Do you have a chronic health problem or condition that restricts your ability to do ordinary daily activities, such as bathing, shopping, or working?” A physical health status index score was created based on the z-scores of these two items and was included as an observed variable in the hypothesized mediation model. A higher score indicated poorer physical health.
Statistical Analysis
Prior to the main analyses, outlier analysis was used to ascertain whether serious outliers existed in the data that might bias the relationships among the study’s variables (Stevens 1984). Results based on the Mahalanobis’ distance and Cook’s distance showed no serious outliers among the study’s variables. Correlational analysis was conducted to examine the relationships among all study’s variables, including variables as indicators of latent factors. Structural equation modeling was used to test the hypothesized mediation model of the relationships between cultural predictors and health outcomes. SEM also was used to test whether or not the factor structures, variable means, and regression paths within the mediation model significantly differed between immigrant and non-immigrant women.
Results
Relationships among Study’s Variables
Table 1 shows the intercorrelations among all study’s variables. There were a number of statistically significant associations among predictor, mediator, and outcome variables. The degrees of correlation varied across the 15 study variables, ranging from small to large. With regard to the cultural variables, acculturation and ethnic pride variables were significantly and negatively correlated with physical and mental health outcomes. Higher levels of acculturation and ethnic pride were associated with better physical and mental health. In examining the associations among the indicators for each of the latent factors of acculturation, family support, and mental health problems, they were all statistically significant. For example, the four indicators representing the family support latent factor were positively associated with each other (at least p < .05). Both age and educational level appeared to be important demographic variables. For example, educational level was positively associated with the acculturation variables, but negatively associated with physical and mental health problems, while age was negatively associated with mental health problems but positively associated with physical health problems. These two demographic variables were included in the hypothesized mediation model as covariates.
Table 1.
Intercorrelations among study variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | – | −.16 | .01 | .16 | .12 | −.01 | .10 | .12 | .04 | −.01 | .15 | −.02 | −.17 | −.18 | .26 |
| 2. Education | – | .56 | .43 | .35 | .14 | .02 | .02 | −.04 | .11 | −.01 | −.10 | −.12 | −.15 | −.29 | |
| 3. Acc1—language | – | .80 | .52 | .03 | .05 | .04 | −.05 | .08 | −.07 | −.15 | −.16 | −.14 | −.24 | ||
| 4. Acc2—country of residence | – | .51 | .02 | .05 | .02 | −.08 | .05 | −.07 | −.11 | −.14 | −.12 | −.12 | |||
| 5. Acc3—ethnic peer affiliation | – | .12 | .08 | .07 | .00 | .07 | −.03 | −.12 | −.17 | −.16 | −.19 | ||||
| 6. Ethnic Pride | – | .09 | .13 | .09 | .01 | .04 | −.09 | −.08 | −.17 | −.14 | |||||
| 7. Family1—concerned about health | – | .47 | .38 | .35 | .02 | −.33 | −.25 | −.31 | −.03 | ||||||
| 8. Family2—stay healthy | – | .46 | .36 | .06 | −.22 | −.22 | −.20 | −.02 | |||||||
| 9. Family3—caring when ill | – | .34 | .07 | −.21 | −.19 | −.17 | .04 | ||||||||
| 10. Family4—healthy activities | – | .02 | −.23 | −.19 | −.25 | −.14 | |||||||||
| 11. Religiosity | – | −.09 | −.08 | −.14 | .03 | ||||||||||
| 12. BDI-SF (depression) | – | .67 | .57 | .26 | |||||||||||
| 13. CES-D (depression) | – | .50 | .16 | ||||||||||||
| 14. Life Dissatisfaction | – | .17 | |||||||||||||
| 15. Physical Health Problems | – | ||||||||||||||
| Mean | 42.52 | 5.09 | 2.50 | 3.27 | 2.35 | 4.37 | 4.34 | 4.12 | 3.97 | 3.13 | .00 | 1.23 | 1.48 | 2.10 | .00 |
| SD | 14.50 | 1.93 | 1.14 | 1.77 | .92 | .81 | 1.17 | 1.32 | 1.44 | 1.67 | .84 | .30 | .46 | .54 | .83 |
Note: N = 561. Acc1, acculturation item 1—language used to speak; Acc2, acculturation item 2—country of residence from infancy to age 21; Acc3, acculturation item 3—ethnic peer affiliation; Family1, family support item 1—spouse or family is there to help when concerned about health; Family2, family support item 2—family encourages me to stay healthy; Family3, family support item 3—family spends time caring for me when I’m ill; Family4, family support item 4—spouse or family participate in healthy activities with me; Religiosity, index score based on z-scores of 2 items (attend mass or church and involvement in church activities); BDI-SF, Beck’s Depression Inventory—Short Form; CES-D, Center for Epidemiologic Studies Depression Scale; Physical Health Problems, index score based on z-scores of two items for physical health (perceived physical health status and chronic health problem status)
Coefficients ≥ .09 were statistically significant, p <.05
Mediation Model of the Relationship between Cultural Predictors and Health Outcomes
Figure 1 shows the results from the SEM testing of the hypothesized mediation model of the relationships between cultural predictors (acculturation and ethnic pride), mediators (family support and religiosity) and physical and mental health outcomes. The relationships of age and education also were considered in this model (for simplicity in presentation, the paths from age and education to other variables and factors are not shown in Fig. 1). As shown in Fig. 1, the model fit the data adequately, using the maximum likelihood estimation, χ2(64, N = 561) = 151.50, Comparative Fit Index (CFI) = .96, and the Root Mean Square Error of Approximation (RMSEA) = .05. With the consideration of age and education in the model, acculturation was directly and negatively associated with physical (p < .01) and mental health (p < .05) problems, while ethnic pride was directly and negatively associated with only physical health problems (p < .05), thus indicating that higher levels of acculturation and ethnic pride were associated with lower levels of health problems.
Fig. 1.
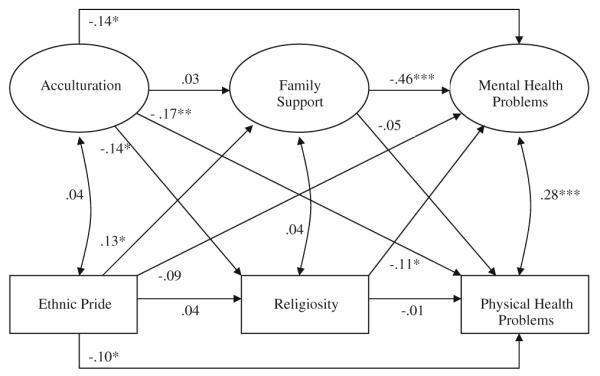
Mediation model of the relationships of acculturation and ethnic pride to physical and mental health outcomes. Note Although the regression paths are not shown in this figure, the effects of age and education were considered in the model. *p < .05, **p < .01, ***p < .001
In examining the paths between cultural predictors and mediators, acculturation was negatively associated with religiosity (p < .05), whereas ethnic pride was positively associated with family support (p < .05). In examining the paths between mediators and health outcomes, family support (p < .001) and religiosity (p < .05) were negatively associated with mental health problems. According to Baron and Kenny’s (1986) requirements for mediation effects, the results indicated that family support mediated the relationship between ethnic pride and mental health problems, while religiosity mediated the relationship between acculturation and mental health problems. However, to determine the statistical significance of these mediation effects, they were tested using the multivariate delta method (MacKinnon 1994; Sobel 1986). This method calculates the standard error of a product of two random variables, which is then used to test the significance of the mediation effect. The results revealed that family support operated as a significant mediator (z = 2.54, p < .05), whereas religiosity did not (z = 1.77, ns). Mexican American women with higher levels of ethnic pride reported higher levels of family support, which in turn predicted lower levels of mental health problems.
Figure 1 also shows that mental health problems were positively associated with physical health problems (p < .001). Although not shown in Fig. 1, age and education were significantly associated with several of the other variables/latent factors in the model. Age was positively associated with religiosity (β = .19, p < .001) and physical health problems (β = .27, p < .001). Education was positively associated with acculturation (r = .57, p < .001) and ethnic pride (r = .14, p < .05), but negatively associated with physical health problems (β = −.14, p < .05).
Across-Group Comparison of the Mediation Model Based on Immigrant Status
Using SEM, invariance analyses were conducted through sequential steps (Joreskog and Sorbom 1985; Widaman and Reise 1997) to test whether the mediation model, including factor loadings, variable means, and regression paths, were significantly different between immigrant and non-immigrant Mexican American women. Table 2 shows the results from these invariance analyses. First, a baseline model was established in which no constraints were specified in the model, meaning the factor loadings, variable means, and regression paths were not constrained to be equal between the two groups. The second step involved the testing of a full constraint model, in which the factor loadings, variable means, and regression paths were constrained to be equal between the two groups. This full constraint model was then compared to the baseline model to evaluate invariance in the mediation model between the two groups. The results indicated that the two models were significantly different (Δχ2(35) = 269.22, p < .001), indicating the presence of potential differences between immigrant and non-immigrant women. Subsequently, three models with varying patterns of constraint were tested to examine whether the sources of across-group differences involved the factor loadings, variable means, and/or regression paths. As shown in Table 2, the testing of model 3 (constraint of factor loadings), in comparison with the baseline model, showed that differences in the factor loadings were non-significant between immigrant and non-immigrant women. In model 4, in addition to constraining the factor loadings, variable means were constrained as equal in this model, which was then compared to model 3. The results of this comparison indicated that the variable means were significantly different between the two groups (Δχ2(15) = 244.02, p < .001). Finally, in model 5, in addition to constraining the factor loadings, the regression paths were constrained as equal for the two groups, and this model was then compared to model 3, indicating that differences in the regression paths were non-significant between the two groups. According to Knight and Hill (1998), the results showed that the factor loadings and regression paths were equivalent between immigrant and non-immigrant women, and that the across-group differences were present only in the variable means, namely age, education, acculturation, depression, and life dissatisfaction (Table 3—for brevity only significant mean differences are shown). Immigrant women exhibited lower levels of acculturation, but slightly higher levels of depression and life dissatisfaction, when compared with non-immigrant women. In addition, immigrant women, on average, were younger in age and less educated than their non-immigrant counterparts.
Table 2.
Across-group comparison analyses of mediation model by immigrant status
| Model | χ 2 | df | Model comparison | Δ χ 2 | Δ df | p value |
|---|---|---|---|---|---|---|
| 1. No constraint | 200.95 | 125 | ||||
| 2. Full constraint | 469.72 | 160 | 2 vs. 1 | 269.22 | 35 | <.001 |
| 3. Constraint of factor loadings | 208.92 | 132 | 3 vs. 1 | 7.97 | 7 | NS |
| 4. Constraint of factor loadings and variable means | 452.94 | 147 | 4 vs. 3 | 244.02 | 15 | <.001 |
| 5. Constraint of factor loadings and regression paths | 223.15 | 145 | 5 vs. 3 | 14.24 | 13 | NS |
Note: These analyses involved sequential tests of the equality of the baseline model, the equality of the factor loadings, the equality of the variable means, and the equality of the regression paths in the mediation model between immigrant and non-immigrant Mexican American women
Table 3.
Significant mean differences between immigrant and non-immigrant Mexican American women
| Variable | Mean (SD) |
F | p value | |
|---|---|---|---|---|
| Immigrant | Non-immigrant | |||
| Age | 39.35 (13.29) | 45.81 (14.98) | 29.32 | <.001 |
| Education | 4.34 (2.00) | 5.87 (1.51) | 103.30 | <.001 |
| Acc1—language | 1.65 (0.72) | 3.38 (0.78) | 753.18 | <.001 |
| Acc2—country of residence | 1.78 (1.10) | 4.82 (0.62) | 1613.87 | <.001 |
| Acc3—ethnic peer affiliation | 1.92 (0.85) | 2.81 (0.76) | 169.69 | <.001 |
| BDI-SF (depression) | 1.26 (0.32) | 1.20 (0.27) | 4.88 | <.05 |
| CES-D (depression) | 1.55 (0.48) | 1.40 (0.43) | 15.07 | <.001 |
| Life Dissatisfaction | 2.18 (0.51) | 2.01 (0.56) | 13.34 | <.001 |
Note: Acc1, acculturation item 1—language used to speak; Acc2, acculturation item 2—country of residence from infancy to age 21; Acc3, acculturation item 3—ethnic peer affiliation; BDI-SF, Beck’s Depression Inventory-Short Form; CES-D, Center for Epidemiologic Studies-Depression Scale
Discussion
The main purpose of this study was to examine a mediation model of the relationships of acculturation and ethnic pride to physical and mental health problems among Mexican American women. It was hypothesized that family support and religiosity would be significant mediators. It also was hypothesized that this mediation model would be significantly different between immigrant and non-immigrant women, as indicated by differences in variable means and regression paths. The main results partially supported the hypothesized mediation model. In addition, differences between immigrant and non-immigrant women were observed in the variable means, but not in the regression paths.
In the analysis of the hypothesized mediation model, acculturation and ethnic pride were directly associated with physical and/or mental health problems. These results further underscore the importance of considering acculturation and other culturally-related variables in research with immigrant and ethnic minority populations. Contrary to what was hypothesized, greater acculturation (i.e., higher level of immersion in or assimilation to host culture) was associated with better physical and mental health. High acculturated Mexican American women reported less depression and life dissatisfaction, and fewer physical health problems. Thus, contrary to some prior research that suggests detrimental effects of increasing acculturation on well-being, the present results suggest a beneficial effect of greater levels of acculturation on psychological and physical well-being. Given that one of the indicators of acculturation was English language proficiency, this component of acculturation may play a particularly important role in health outcomes. For many recent immigrants, learning a new language constitutes a major stressor that can compromise access to adequate employment and housing, social services, and health care (Weiss et al.2006). Of course, this is not to say that immigrants should abandon their native language and culture, as a bicultural mode of acculturation has been suggested to be most advantageous (Berry 2001; La Fromboise et al. 1993). This does recognize, however, that limited language proficiency in any new culture can operate as a barrier to better health care, and also can contribute to a lower sense of well-being and quality of life. Another explanation for these findings involves the higher level of education observed among the more acculturated women. Indeed, higher educational level has been shown to be associated with higher socioeconomic status and with other positive outcomes (e.g., Jackson 2003), suggesting the presence of fewer uncontrollable stressors in the lives of these women, and consequently better health outcomes. Overall, these findings are consistent with the theoretical underpinnings of the stress-process model (Pearlin et al. 1981).
Acculturation and ethnic pride also can impact interpersonal and intrapersonal factors as indicated by the negative relationship between acculturation and religiosity and the positive relationship between ethnic pride and family support. Consistent with previous research (Pena and Frehill 1998), more acculturated women reported a lower level of religiosity, showing a decrease in the frequency of church attendance and involvement in church-related activities. However, this does not necessarily indicate a lower level of spirituality or religious beliefs in a supreme being; instead this may reflect less of a need to be involved in day-to-day church activities. For many individuals, involvement in church activities can facilitate a network of social support that can exert an important helping role in people’s lives (Carothers et al. 2005). The need for this type of social support may be less important among US-born or higher acculturated women who have greater access to social capital and to other forms of social support, including a more extensive network of family members and friends, as compared to the resources available to recently immigrated women. As expected, a sense of pride and connectedness with one’s ethnic background was associated with a higher level of family support. For Mexican American women and other women of color, ethnic pride is an integral part of their family background and history. Therefore, among ethnic minority persons, having positive feelings about their ethnic heritage can contribute to positive relationships and support among family members. As the present study is cross-sectional in design, it is also plausible that having greater family support may engender higher levels of ethnic pride. Both interpretations are consistent with previous research on the positive association between ethnic pride and family factors (Hughes 2003).
Family support, but not religiosity, was a significant mediator, particularly in the relationship between ethnic pride and mental health problems, further underscoring the importance of family in the lives of Mexican American women. Consistent with previous research, family support operated as a protective factor against mental distress and disorder (Vega et al. 1991). However, contrary to the main hypotheses, neither family support nor religiosity operated as significant mediators in the relationships between acculturation/ethnic pride and physical health problems. While both acculturation and ethnic pride exhibited direct effects on physical health problems, their mediating or indirect effects may be nonexistent or may involve different variables from the ones included in this study. In addition, the sociocultural process and its pattern of mediating effects on physical health problems may differ significantly from the process that influences mental health problems. Nonetheless, it is also important to note that in this study, mental health problems were positively associated with physical health problems, suggesting a close connection between these two areas of well-being.
The relevance of demographic variables, such as age and education, was indicated by the results of this study. These findings are consistent with the literature (Castro et al. 1999b), suggesting the importance of including these variables in research with Mexican American women as they comprise a diverse population. Thus, in our attempt to understand the underlying factors that contribute to health disparities it is necessary to examine within-group differences in addition to the typical investigations of between-ethnic group differences. In the present study, both age and education were significant correlates of physical health problems, indicating the need to consider these variables when addressing issues of health disparities among Mexican American women.
As expected, immigrant status was another important demographic characteristic but differences between immigrant and non-immigrant women in the hypothesized mediation model were observed only among some of the variable means. These results suggest that the measurement constructs and the pattern of relationships between the variables and latent factors in the mediation model were generally similar for immigrant and non-immigrant women. Consistent with the theoretical work of Berry (2003), immigrant women experience more distress than their non-immigrant counterparts, pointing to the stress involved in their adjustment to a new cultural environment. In thinking about issues of health disparities among Mexican American women, immigrant status is another important factor that must be considered in future research. However, results of the present study suggest the occurrence of a common process of acculturative effects for both immigrant and non-immigrant women. Perhaps as these women share a common status as minorities and women of color, this commonality may introduce common life experiences that surpass any influences introduced by immigrant-native status. Additional research that clearly distinguishes between ethnicity and minority status (Meyerowitz et al. 1998) may clarify the nature of these potential effects.
Limitations of the Present Study
There are a few limitations to the present study, which may affect the generalizability of its findings. First, acculturation, using only three items, was based on the linear or unidimensional model of acculturation, which constitutes just one mode of acculturation and provides a limited understanding of the effects of acculturation on mediators and health-related outcomes. Increasing acculturation towards the host culture does not necessarily always involve abandoning connections with one’s culture-of-origin (Rogler et al. 1991), and this may be the case for both immigrant and non-immigrant Mexican American women. Second, our measurement of the complex construct of ethnic pride was based on a single item, which limits a more complete assessment of this variable. In other words, what exactly are the underlying dimensions of ethnic pride that can influence family relationships and health outcomes? Third, because the results were based on cross-sectional data, the model presented in the present study is one of several similar models that can be postulated such that variants in the directionality of the observed effects are possible. As noted earlier, greater ethnic-pride could promote greater family support, although conversely, greater family support could engender greater ethnic pride. Other similar configurations in the temporal relations between the various model variables can be postulated. Finally, the women in this study were of Mexican descent living in the Southwest region of the United States, so the results may not apply to other Latina groups, such as Cuban or Puerto Rican women.
Implications for Future Research and Interventions
Despite these limitations, the findings from this study offer important implications for research and the design of prevention and treatment interventions aimed at reducing health disparities among Latinas of Mexican heritage. The main implication is that future research with Mexican and Mexican American women or with other ethnic minority women cannot ignore the potential impact of acculturation-related factors on the quality of life for these women. Notwithstanding the criticisms that some investigators have raised regarding current approaches to acculturation research (Hunt et al. 2004), the process of acculturative adaptation is a daily reality for many immigrants (both documented and undocumented), as well as for US-born ethnic minority people, who migrate from rural to urban communities in search of a better life. While research on the effects of acculturative variables has proliferated in recent years, we still know very little about their true effects, especially for ethnic minority women. Certainly, more complex assessments and multivariate models for investigating the health impacts of the acculturative processes are needed to understand the complex dynamics involved in ubiquitous sociocultural phenomena such as the process of acculturation. The same issues apply to the complex construct of ethnic pride, which has received little attention as a factor that can influence health outcomes, and thus our knowledge of its effects in health and health disparities is even more limited than that for acculturation. Needless to say, more longitudinal research is needed if we are to ascertain the temporal effects, both risk-inducing and protective, of acculturation and other cultural variables on health-related outcomes.
Another implication is that future research and intervention programs with Mexican American women must consider the role of family in mental health and well-being. Although this knowledge is not unique to this study’s sample, further in-depth study regarding the potential protective effects of family is warranted, especially among recent immigrants who have limited social networks, educational attainment, and resources. While there is unanimous agreement among social scientists regarding the importance of family factors, little is still known about the specific aspects of family support and relationships as these may contribute to Mexican American women’s physical and mental well-being. Given that previous research with other ethnic minority samples has demonstrated the importance of specific dyadic relationships in adjustment outcomes (e.g., Dinh et al. 1994; Dinh and Nguyen 2006), future research with Mexican American women should explore in greater depth specific family relationships and the roles of specific family members in the maintenance of health or illness. Such research would provide a better understanding of the determinants of salubrious health status among Mexican American women as well as contributing crucial information for the design of more effective prevention intervention programs.
Conclusion
The present study, utilizing secondary data analysis, examined a multivariate mediation model of the relationships of acculturation and ethnic pride to physical and mental health outcomes. Given that Mexican American women constitute a large and diverse segment of the Latina/o population in the United States, yet remain a relatively understudied sub-population, the present study contributes to the limited knowledge about the effects of specific cultural factors on their health status. In this study, only family support and religiosity were modeled as mediators, although certainly other interpersonal and intrapersonal mediators, such as peer support/network and personal coping capacity, as well as key contextual variables (e.g., access to health care, neighborhood factors, etc.) should be considered in future research to examine the determinants of various health outcomes. Indeed, more complex investigations guided by specific cultural models of acculturation, such as the one presented in this study, may provide more in depth information to further our understanding of the life experiences of Mexican American women and other Latinas. Ultimately new knowledge generated from such studies may aid in designing culturally-relevant health promotion intervention programs that can address barriers to health, reduce or eliminate health disparities, while also enhancing existing strengths and resources for all Latinas.
Footnotes
In this article we use the terms “Latina/os” and “Hispanics” interchangeably, based on the dual usage that occurs within the contemporary literature. The terms “Hispanic” and “Latina/o” are generic labels that refer to people living in the United States, primarily Mexican Americans, Puerto Ricans (both from the Island of Puerto Rico and from the US mainland), Cubans, as well as other Hispanics/Latina/os, including Colombians, Guatemalans, Nicaraguans, and other immigrants and naturalized persons from Central America and South America.
Here we recognize that among persons of Mexican heritage, immigrants typically are recognized or self-identify as “Mexicans,” and US-born (native-born) persons of Mexican heritage typically are recognized or self-identify as “Mexican Americans.” For brevity and ease of presentation as well as differentiation from Mexican women living in Mexico, we refer generally to immigrant and non-immigrant women in our study as “Mexican American women” or as “Latinas of Mexican heritage.”
An important note to mention here involves the myriad of terminologies used in acculturation research that often can be confusing. The term “acculturation” in many instances is an umbrella term that encompasses the study of adaptation and changes among immigrants and minorities in their continuous contact with the host/dominant culture, and encompasses the various theories and models that attempt to explicate the process of change and adaptation. In many other instances, the term “acculturation” is also used by researchers to connote “assimilation” or a linear progression of immersion in the host culture, and commonly the term “acculturation level” is also used in these instances. Individuals who are able to adopt aspects of the new culture while maintaining aspects of their culture-of-origin are defined as “bicultural” or “integrated.”
Contributor Information
Khanh T. Dinh, Department of Psychology, University of Massachusetts Lowell, 870 Broadway, Lowell, MA 01854, USA
Felipe González Castro, Arizona State University, Tempe, AZ, USA.
Jenn-Yun Tein, Arizona State University, Tempe, AZ, USA.
Su Yeong Kim, University of Texas at Austin, Austin, TX, USA.
References
- Abe-Kim J, Okazaki S, Goto SG. Unidimensional versus multidimensional approaches to the assessment of acculturation for Asian American populations. Cultural Diversity and Ethnic Minority Psychology. 2001;7:232–246. doi: 10.1037/1099-9809.7.3.232. [DOI] [PubMed] [Google Scholar]
- Alvarez AN, Helms JE. Radical identity and reflected appraisals as influences on Asian Americans’ racial adjustment. Cultural Diversity and Ethnic Minority Psychology. 2001;7:217–231. doi: 10.1037/1099-9809.7.3.217. [DOI] [PubMed] [Google Scholar]
- Austin AA. Alcohol, tobacco, other drug use, and violent behavior among Native Hawaiians: Ethnic pride and resilience. Substance Use and Misuse. 2004;39(5):721–746. doi: 10.1081/ja-120034013. [DOI] [PubMed] [Google Scholar]
- Bagley SP, Angel R, Dilworth-Anderson P, Liu W, Schinke S. Panel V: Adaptive health behaviors among ethnic minorities. Health Psychology. 1995;14:632–640. doi: 10.1037//0278-6133.14.7.632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balcazar H, Castro FG, Krull JL. Cancer risk reduction in Mexican American women: The role of acculturation, education, and health risk factors. Health Education Quarterly. 1995;22:61–84. doi: 10.1177/109019819502200107. [DOI] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, Garbin MG. Short form of Depression Inventory: Cross-validation. Psychological Reports. 1988;34(3):1184–1186. [PubMed] [Google Scholar]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Archives of General Psychiatry. 1961;4:561–571. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- Berry JW. A psychology of immigration. Journal of Social Issues. 2001;57:615–631. [Google Scholar]
- Berry JW. Conceptual approaches to acculturation. In: Chun KM, Organista PB, Marin G, editors. Acculturation: Advances in theory, measurement, and applied research. American Psychological Association; Washington, DC: 2003. pp. 17–37. [Google Scholar]
- Bonicatto S, Dew AM, Soria JJ. Analysis of the psychometric properties of the Spanish version of the Beck Depression Inventory in Argentina. Psychiatric Research. 1998;79(3):277–285. doi: 10.1016/s0165-1781(98)00047-x. [DOI] [PubMed] [Google Scholar]
- Carothers SS, Borkowski JG, Lefever JB, Whitman TL. Religiosity and the socioemotional adjustment of adolescent mothers and their children. Journal of Family Psychology. 2005;19:263–275. doi: 10.1037/0893-3200.19.2.263. [DOI] [PubMed] [Google Scholar]
- Castro FG, Cota MK, Vega SC. Health promotion in Latino populations: A sociocultural model for program planning, development, and evaluation. In: Huff RM, Kline HV, editors. Promoting health in multicultural populations: A handbook for practitioners. Sage; Thousand Oaks, CA: 1999a. pp. 137–168. [Google Scholar]
- Castro FG, Elder J, Coe K, Tafoya-Barraza HM, Moratto S, Campbell N, et al. Mobilizing churches for heath promotion in Latino communities: Compañeros en la Salud. Journal of the National Cancer Institute Monographs. 1995;18:127–135. [PubMed] [Google Scholar]
- Castro FG, Hernandez-Alarcon E. Integrating cultural variables into drug abuse prevention and treatment with racial/ethnic minorities. Journal of Drug Issues. 2002;32:783–810. [Google Scholar]
- Castro FG, Proescholdbell RJ, Abeita L, Rodriguez D. Ethnic and cultural minority groups. In: McCrady BS, Epstein EE, editors. Addictions: A comprehensive guidebook. Oxford Press; New York: 1999b. pp. 499–526. [Google Scholar]
- Cervantes RC, Padilla AM, Salgado de Snyder N. The Hispanic Stress Inventory: A culturally relevant approach to psychosocial assessment. Psychological Assessment. 1991;3:438–447. [Google Scholar]
- Chun KM, Organista PB, Marin G. Acculturation: Advances in theory, measurement and applied research. American Psychological Association; Washington, DC: 2003. [Google Scholar]
- Cuellar I, Arnold B, Gonzalez G. Cognitive referents of acculturation: Assessment of cultural constructs in Mexican Americans. Journal of Community Psychology. 1995a;23:339–356. [Google Scholar]
- Cuellar I, Arnold B, Maldonado R. Acculturation Rating Scale for Mexican Americans-II: A revision of the original ARSMA Scale. Hispanic Journal of Behavioral Sciences. 1995b;17:275–304. [Google Scholar]
- Dinh KT, Nguyen HH. The effects of acculturative variables on Asian American parent–child relationships. Journal of Social and Personal Relationships. 2006;23(3):407–426. [Google Scholar]
- Dinh KT, Sarason BR, Sarason IG. Parent–child relationships in Vietnamese immigrant families. Journal of Family Psychology. 1994;8:471–488. [Google Scholar]
- Flack JM, Amaro H, Jenkins W, Kunitz S, Levy J, Mixon M, et al. Panel I: Epidemiology of minority health. Health Psychology. 1995;14:592–600. doi: 10.1037//0278-6133.14.7.592. [DOI] [PubMed] [Google Scholar]
- Gil AG, Vega WA. Two different worlds: Acculturation stress and adaptation among Cuban and Nicaraguan families. Journal of Social and Personal Relationships. 1996;13:435–456. [Google Scholar]
- Graves AB, Larson EB, Edland SD, Bowen JD, McCormick WC, McCurry SM, et al. Prevalence of dementia and its subtypes in the Japanese American population of King County, Washington State. American Journal of Epidemiology. 1996;144:760–771. doi: 10.1093/oxfordjournals.aje.a009000. [DOI] [PubMed] [Google Scholar]
- Huang B, Rodriguez BL, Burchfiel CM, Chyou P, Curb JD, Yano K. Acculturation and prevalence of diabetes among Japanese-American men in Hawaii. American Journal of Epidemiology. 1996;144:674–681. doi: 10.1093/oxfordjournals.aje.a008980. [DOI] [PubMed] [Google Scholar]
- Hughes D. Correlates of African American and Latino parents’ messages to children about ethnicity and race: A comparative study of racial socialization. American Journal of Community Psychology. 2003;31:15–33. doi: 10.1023/a:1023066418688. [DOI] [PubMed] [Google Scholar]
- Hunt LM, Schneider S, Comer B. Should “acculturation” be a variable in health research? A critical review of research on U.S. Hispanics. Social Science and Medicine. 2004;59:973–986. doi: 10.1016/j.socscimed.2003.12.009. [DOI] [PubMed] [Google Scholar]
- Izard CE. Translating emotion theory and research into preventive interventions. Psychological Bulletin. 2002;128:796–824. doi: 10.1037/0033-2909.128.5.796. [DOI] [PubMed] [Google Scholar]
- Jackson AP. The effects of family and neighborhood characteristics on the behavioral and cognitive development of poor Black children. American Journal of Community Psychology. 2003;32:175–186. doi: 10.1023/a:1025615427939. [DOI] [PubMed] [Google Scholar]
- Jeynes WH. The effects of the religious commitment of twelfth graders living in non-intact families on their academic achievement. Marriage & Family Review. 2003;35:77–97. [Google Scholar]
- Joreskog KG, Sorbom D. Simultaneous analysis of longitudinal data from several cohorts. In: Mason WM, Fienberg SE, editors. Cohort analysis in social research: Beyond the identification problem. Springer-Verlag; New York: 1985. [Google Scholar]
- Knight GP, Hill NE. Measurement equivalence in research involving minority adolescents. In: McLoyd V, Steinberg L, editors. Research on minority adolescents: Conceptual, methodological and theoretical issues. Lawrence Erlbaum; Mahwah, NJ: 1998. pp. 183–210. [Google Scholar]
- La Fromboise T, Coleman HLK, Gerton J. Psychological impact of biculturalism: Evidence and theory. Psychological Bulletin. 1993;114:395–412. doi: 10.1037/0033-2909.114.3.395. [DOI] [PubMed] [Google Scholar]
- Lara M, Gamboa C, Kahramanian MI, Morales L, Hayes-Bautista DE. Acculturation and Latino health in the United States: A review of the literature and its sociopolitical context. Annual Review of Public Health. 2005;26:367–397. doi: 10.1146/annurev.publhealth.26.021304.144615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP. Analysis of mediating variables in prevention and intervention research. National Institute of Drug Abuse Research Monograph Series. 1994;139:127–153. [PubMed] [Google Scholar]
- Marin G, Gamboa RJ. A new measurement of acculturation for Hispanics: The Bidimensional Acculturation Scale for Hispanics (BAS) Hispanic Journal of Behavioral Sciences. 1996;18:297–316. [Google Scholar]
- Marin G, Gamboa RJ. Acculturation and changes in cultural values. In: Chun KM, Organizta PB, Marin G, editors. Acculturation: Advances in theory, measurement, and applied research. American Psychological Association; Washington, DC: 2003. pp. 83–93. [Google Scholar]
- Marsiglia FF, Kulis S, Hecht M. Ethnic labels and ethnic identity as predictors of drug use among middle school students in the Southwest. Journal of Research on Adolescence. 2001;11:21–48. [Google Scholar]
- Meadows LM, Thurston WE, Melton C. Immigrant women’s health. Social Sciences & Medicine. 2001;52:1451–1458. doi: 10.1016/s0277-9536(00)00251-3. [DOI] [PubMed] [Google Scholar]
- Meyerowitz BE, Richardson JE, Hudson S, Leedham B. Ethnicity and cancer outcomes: Behavioral and psychosocial considerations. Psychological Bulletin. 1998;123:47–70. doi: 10.1037/0033-2909.123.1.47. [DOI] [PubMed] [Google Scholar]
- Mossakowski KN. Coping with perceived discrimination: Does ethnic identity protect mental health? Journal of Health and Social Behavior. 2003;44:318–331. [PubMed] [Google Scholar]
- Murray B. [Retrieved March 15, 2006];Latino religion in the U.S.: Demographic shifts and trends. Facsnet. 2006 Jan 5; From http://www.facsnet.org/issues/faith/espinosa.php.
- Myers HF, Kagawa-Singer M, Kumanyika SK, Lex BW, Markides KS. Panel III: Behavioral risk factors related to chronic diseases in ethnic minorities. Health Psychology. 1995;14:613–621. doi: 10.1037//0278-6133.14.7.613. [DOI] [PubMed] [Google Scholar]
- Norris AE, Ford K, Bova CA. Psychometrics of a brief acculturation scale for Hispanics in a probability sample of urban Hispanic adolescents and young adults. Hispanic Journal of Behavioral Sciences. 1996;18:29–38. [Google Scholar]
- O’Donnell L, O’Donnell C, Wardlaw DM, Stueve A. Risk and resiliency factors influencing suicidality among urban African American and Latino youth. American Journal of Community Psychology. 2004;33:37–49. doi: 10.1023/b:ajcp.0000014317.20704.0b. [DOI] [PubMed] [Google Scholar]
- Orme JG, Reis J, Herz EJ. Factorial and discriminant validity of the Center for Epidemiological Studies Depression (CES-D) Scale. Journal of Clinical Psychology. 1986;42(1):28–33. doi: 10.1002/1097-4679(198601)42:1<28::aid-jclp2270420104>3.0.co;2-t. [DOI] [PubMed] [Google Scholar]
- Pearlin LI, Lieberman MA, Menaghan EG, Mullan JT. The stress process. Journal of Health and Social Behaviors. 1981;19:337–356. [PubMed] [Google Scholar]
- Pena M, Frehill LM. Latina religious practice: Analyzing cultural dimensions in measures of religiosity. Journal for the Scientific Study of Religion. 1998;37:620–635. [Google Scholar]
- Prilleltensky I. The immigration experience of Latin American families: Research and action on perceived risk and protective factors. Canadian Journal of Community Mental Health. 1993;12:101–116. [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1(3):385–401. [Google Scholar]
- Redfield R, Linton R, Herskovits MJ. Memorandum for the study of acculturation. American Anthropologist. 1936;38:149–152. [Google Scholar]
- Rogler LH, Cortes DE, Malgady RG. Acculturation and mental health status among Hispanics: Convergence and new direction for research. American Psychologist. 1991;46:585–597. doi: 10.1037//0003-066x.46.6.585. [DOI] [PubMed] [Google Scholar]
- Rudmin FW. Critical history of the acculturation psychology of assimilation, separation, integration, and marginalization. Review of General Psychology. 2003;7:3–37. [Google Scholar]
- Shrout PE, Canino GJ, Bird HR, Rubio-Stipec M, Bravo M, Burnam MA. Mental health status among Puerto Ricans, Mexican Americans, and non-Hispanic whites. American Journal of Community Psychology. 1992;20:729–752. [PubMed] [Google Scholar]
- Smith EP, Atkins J, Connell CM. Family, school, and community factors and relationships to racial-ethnic attitudes and academic achievement. American Journal of Community Psychology. 2003;32:159–173. doi: 10.1023/a:1025663311100. [DOI] [PubMed] [Google Scholar]
- Sobel ME. Some new results on indirect effects and their standard errors in structure equation models. In: Tuma N, editor. Social Methodology. Jossey Bass; San Francisco: 1986. pp. 159–186. [Google Scholar]
- Stevens JP. Outliers and influential data points in regression analysis. Psychological Bulletin. 1984;95:334–344. [Google Scholar]
- Tugade MM, Frederickson BL. Resilient individuals use positive emotions to bounce back from negative emotional experiences. Journal of Personality and Social Psychology. 2004;86:320–333. doi: 10.1037/0022-3514.86.2.320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- US Census Bureau [Retrieved May 5, 2006];Fact sheet for selected population group: Mexican. 2000 From http://factfinder.census.gov.
- US Census Bureau . The Hispanic population in the United States: March 2002. U.S. Department of Commerce, Economics and Statistics Administration; Washington, DC: 2003. [Google Scholar]
- US Census Bureau [Retrieved June 25, 2005];Fact for features: Special edition (Cinco de Mayo) 2005 From http://www.census.gov/acs/www/index.html.
- US Census Bureau [Retrieved November 29, 2005];Race and Hispanic or Latino origin of the population of the United States: 2003 and 2004. 2005 From www.census.gov/Press-Release/www/releases/archives/natrecepop2004_tb1.pdf.
- US Department of Health and Human Services 2004 National healthcare disparities report. 2004. (AHRQ Publication No. 05-0014)
- Vega WA, Kolody B, Aguilar-Gaxiola S, Alderete E, Catalano R, Caraveo-Anduaga J. Lifetime prevalence of DSMIII-R psychiatric disorders among urban and rural Mexican Americans in California. Archives of General Psychiatry. 1998;55:771–782. doi: 10.1001/archpsyc.55.9.771. [DOI] [PubMed] [Google Scholar]
- Vega WA, Kolody B, Valle R, Weir J. Social networks, social support, and their relationship to depression among immigrant Mexican women. Human Organization. 1991;50:154–162. [Google Scholar]
- Weiss L, Bauer T, Hill C, Fuld J, Bergman J. [Retrieved July 14, 2006];Language as a barrier to health care for New York City children in immigrant families: Haitian, Russian and Latino perspectives. From the New York Academy of Medicine Web site. 2006 May; http://www.nyam.org/initiatives/sp-pub.shtml.
- Widaman KF, Reise SP. Exploring the measurement invariance of psychological instruments: Applications in the substance use domain. In: Bryant KJ, Windle M, West SG, editors. The science of prevention: Methodological advances from alcohol and substance abuse research. American Psychological Association; Washington, DC: 1997. pp. 281–324. [Google Scholar]
- Yee BWK, Castro FG, Hammond WR, John R, Wyatt GE, Yung BR. Panel IV: Risk-taking and abusive behaviors among ethnic minorities. Health Psychology. 1995;14:622–631. doi: 10.1037//0278-6133.14.7.622. [DOI] [PubMed] [Google Scholar]
- Zambrana R, Dill BT. Disparities in Latina health: An intersectional analysis. In: Shulz AJ, Mullings L, editors. Gender, race, class and health: Intersectional approaches. Jossey-Bass; San Francisco, CA: 2006. pp. 192–227. [Google Scholar]
- Zambrana RE, Scrimshaw SCM, Collins N, Dunkel-Schetter C. Prenatal health behaviors and psychosocial risk factors in pregnant women of Mexican origin: The role of acculturation. American Journal of Public Health. 1997;87:1022–1026. doi: 10.2105/ajph.87.6.1022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zane N, Mak W. Major approaches to the measurement of acculturation among ethnic minority populations: A content analysis and an alternative empirical strategy. In: Chun KM, Organista PB, Marin G, editors. Acculturation: Advances in theory, measurement, and applied research. American Psychological Association; Washington, DC: 2003. pp. 39–60. [Google Scholar]