

Abstract
AIM: To evaluate the use of photogrammetry and identify the mathematical procedures applied when evaluating spinal posture.
METHODS: A systematic search using keywords was conducted in the PubMed, EMBASE, Scopus, Science and Medicine® databases. The following inclusion criteria adopted were: (1) the use of photogrammetry as a method to evaluate spinal posture; (2) evaluations of spinal curvature in the sagittal and/or frontal plane; (3) studies published within the last three decades; and (4) written entirely in English. The exclusion criteria were: (1) studies which objective involved the verification of some aspect of validation of instruments; (2) studies published as abstracts and those published in scientific events; and (3) studies using evaluation of the anteriorization of the head to determine the angular positioning of the cervical spine. The articles in this review were included and evaluated for their methodological quality, based on the Downs and Black scale, by two independent reviewers.
RESULTS: Initially, 1758 articles were found, 76 of which were included upon reading the full texts and 29 were included in accordance with the predetermined criteria. In addition, after analyzing the references in those articles, a further six articles were selected, so that 35 articles were included in this review. This systematic review revealed that the photogrammetry has been using in observational studies. Furthermore, it was also found that, although the data collection methodologies are similar across the studies, in relation to aspects of data analysis, the methodologies are very different, especially regarding the mathematical routines employed to support different postural evaluation software.
CONCLUSION: With photogrammetry, the aim of the assessment, whether it is for clinical, research or collective health purposes, must be considered when choosing which protocol to use to evaluate spinal posture.
Keywords: Lordosis, Kyphosis, Spine, Photogrammetry, Scoliosis, Posture
Core tip: With photogrammetry, various spinal posture assessment protocols can be adopted. However, the literature lacks evidence to support the use of photogrammetry in accompanying postural treatment, whether for clinical or research purposes. When using photogrammetry in scientific research, a protocol or software that provides detailed postural analysis should be the first choice. In the clinical environment, the choice of protocol will depend on the objectives established for the patient by the physiotherapist. When dealing with a collective health situation, such as groups of schoolchildren, it is necessary to prioritize simpler protocols.
INTRODUCTION
Photogrammetry is a widely used non-invasive technique for postural evaluation. It is a viable option for healthcare professionals and researchers in the field of posture[1], possibly because it allows a succinct and accurate quantitative evaluation by recording subtle changes in posture in general[2,3]. From the point of view of spinal evaluation, it is capable of providing information in the frontal and sagittal planes[4,5]. Furthermore, the use of photogrammetry undoubtedly contributes to reducing exposure to radiation and thus enables the monitoring of postural treatment. However, the application of this technique in postural evaluation is directly dependent on both the collection procedures and the mathematical methods used to provide measurements and postural diagnoses, and which should provide all the necessary aspects of validation[6,7].
Specifically regarding the application of photogrammetry in spinal evaluation, many studies have performed procedures to validate the technique[4,6,8-11]. Furthermore, in clinical practice, photogrammetry can be useful for evaluating and monitoring changes in spinal treatments by comparing quantitative data on posture[6,12]. Moreover, in scientific studies, its use may be helpful in both transverse and longitudinal observations and in intervention studies.
Although, according to the literature, the use of photogrammetry in spinal evaluation is widespread, its real applicability may be questioned, as it remains unclear how this technique is being used to monitor postural treatment or to map attitudes among populations in observational studies. Furthermore, many studies that have adopted the use of photogrammetry do not explain the methods used to generate the results obtained, thus constituting veritable “black boxes”, which makes it difficult for users both in clinical practice and in scientific research to apply this evaluation method. Hence, the objective of this systematic review was to evaluate the use of photogrammetry and to identify the mathematical procedures involved when it is applied to assess spinal posture.
MATERIALS AND METHODS
This study was a systematic review, in which the eligibility criteria were observational studies and randomized and nonrandomized clinical trials that have used photogrammetry as a tool to evaluate the spine in an attempt to understand its importance in the assessment of posture. The systematic review follows methods recommended by the Cochrane Collaboration[13].
A systematic literature search was performed in the PubMed, Embase, Scopus, Science and MEDICINE® databases in the months of December 2013 and January 2014. The keywords used were found in the Health Sciences Descriptors (DeCS, Descritores em Ciências da Saúde), Medical Subject Headings or Emtree: (“Photogrammetry” OR “Digital Analysis” OR “Digital Photographs” OR “Digital photography”) AND (“Spinal postural evaluation” OR “Spine” OR “Vertebral Column” OR “Column, Vertebral” OR “Columns, Vertebral” OR “Vertebral Columns” OR “Spinal Column” OR “Column, Spinal” OR “Columns, Spinal” OR “Spinal Columns” OR “Vertebra” OR “Vertebrae” OR “Lordosis” OR “Kyphosis” OR “Kyphoses” OR “Scoliosis” OR “Scolioses” OR “Posture” OR “Postures” OR “Spine Curvatures” OR “lumbar curvatures” OR “thoracic curvatures” OR “thoracic curve” OR “lordosis curve” OR “thoracic kyphosis” OR “lumbar lordosis”). The search was limited to articles written entirely in English, because it is the international language.
To constitute this systematic review, the articles identified by the initial search strategy had to meet the following inclusion criteria: (1) use photogrammetry as a method of postural evaluation; (2) evaluate the curvatures of the spine in the sagittal or frontal plane; (3) been published within the last three decades; and (4) been written entirely in English. The exclusion criteria were: (1) studies in which the objective involved verifying some aspect of instrument validation; (2) studies published as abstracts and published in scientific events; and (3) studies that used the evaluation of anteriorization of the head to determine the angular positioning of the cervical spine. These variables are believed to analyze different aspects of body posture and cannot be analyzed together.
All the search procedures, selection, quality assessment, data extraction and the reading of the articles were performed independently and individually by two reviewers. In case of any difference of opinion between the reviewers, a third reviewer was asked to appraise the article.
Initially, the studies were selected by reading the titles and abstracts, and those considered to have the potential to be included in the search were read and analyzed in full. In those cases where the title and the abstract were inconclusive, the full article was obtained and read in order not to risk of leaving out important studies in this review. Complementing this process, the references of each included article were also checked in order to identify items not found in the electronic search.
The studies that met the inclusion criteria were evaluated for their methodological quality using the Downs and Black scale, which consists of a checklist of 26 criteria that are answered “yes”, “no” or “impossible to determine”[14]. This scale was chosen because it is used to evaluate both observational studies and randomized clinical trials (RCTs), while some criteria are designed to assess RCTs exclusively, which were unnecessary in this systematic review. According to the guidelines for the use of the scale[14], the assessment criteria can be chosen based on the study objective, thus in the present study those criteria referring solely to the assessment of RCTs were excluded, and only 12 criteria from the Downs and Black scale were used when assessing methodological aspects.
The Downs and Black scale does not define a minimum score when determining the quality of studies[14]. Therefore, studies were not excluded based on their quality rating and only the total number of criteria rated as “yes” for each article was used. The higher the score for the criteria of article, the better methodological quality[14].
RESULTS
Initially, 1758 articles were found from the keywords used. Of these, 601 were excluded because they were duplicates and 1081 did not meet the inclusion criteria. Thus, 76 studies were initially included in this systematic review. After reading the articles in full, 29 studies were found to meet all the inclusion criteria. Subsequently, their reference lists were analyzed and, based on this analysis, a further that 6 articles were found to meet the inclusion criteria, thus 35 articles were selected for inclusion in this systematic review (Figure 1).
Figure 1.
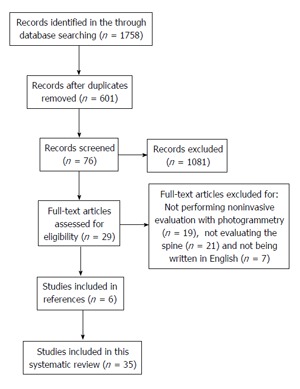
Flowchart of article selection.
Table 1 presents the assessment of the methodological quality based on Downs and Black scale of the studies selected for review. All 35 items had checklist scores higher or equal to 6. In addition, 9 studies had scores between 7 and 8; 19 studies had scores between 9 and 10; and 6 studies had scores between 11 and 12 (Table 1).
Table 1.
Results of the quality assessment of studies by downs and black scale
| Ref. |
Criteria checklist downs and black |
Total | |||||||||||
| 1 | 2 | 3 | 6 | 7 | 9 | 10 | 11 | 12 | 16 | 18 | 20 | (No. of √) | |
| Almeida et al[15] | √ | X | √ | X | √ | √ | √ | ? | ? | √ | √ | √ | 8 |
| Cheng et al[16] | √ | √ | √ | √ | √ | √ | √ | ? | ? | √ | √ | √ | 10 |
| Fortin et al[17] | √ | √ | √ | √ | √ | √ | √ | ? | ? | √ | √ | √ | 10 |
| Annetts et al[18] | √ | √ | √ | √ | √ | √ | √ | X | X | √ | √ | √ | 10 |
| Weber et al[19] | √ | √ | √ | √ | X | ? | √ | X | X | √ | √ | √ | 8 |
| Edmondston et al[20] | √ | √ | √ | √ | √ | √ | √ | X | X | √ | √ | √ | 10 |
| Milanesi et al[21] | √ | √ | √ | √ | √ | √ | √ | ? | ? | √ | √ | √ | 10 |
| de Oliveira Pezzan et al[22] | √ | √ | √ | √ | √ | √ | √ | ? | ? | √ | √ | √ | 10 |
| Yang et al[23] | √ | √ | √ | √ | ? | √ | √ | ? | ? | √ | √ | √ | 9 |
| Silveira et al[24] | √ | √ | √ | √ | √ | √ | √ | ? | ? | √ | √ | √ | 10 |
| Iunes et al[25] | √ | √ | √ | √ | X | √ | √ | ? | ? | √ | √ | √ | 9 |
| Belli et al[26] | √ | √ | √ | √ | √ | √ | X | √ | √ | √ | √ | √ | 11 |
| Chase et al[27] | √ | √ | √ | √ | √ | ? | √ | √ | √ | √ | √ | ? | 10 |
| Iunes et al[12] | √ | √ | √ | √ | √ | √ | √ | X | X | √ | √ | √ | 10 |
| Iunes et al[28] | √ | √ | √ | √ | √ | √ | √ | ? | ? | √ | √ | √ | 10 |
| Penha et al[29] | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 12 |
| Rodrigues et al[30] | √ | √ | √ | √ | √ | √ | √ | X | X | √ | √ | √ | 10 |
| Straker et al[31] | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 12 |
| Iunes et all[32] | √ | √ | √ | √ | X | √ | √ | X | X | √ | √ | √ | 9 |
| Smith et al[3] | √ | √ | X | √ | √ | √ | √ | ? | ? | √ | √ | √ | 9 |
| Yi et al[33] | √ | √ | √ | √ | √ | √ | √ | ? | ? | √ | √ | √ | 10 |
| Min et al[34] | X | √ | √ | √ | √ | √ | ? | ? | ? | √ | ? | √ | 7 |
| Straker et al[35] | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ? | 11 |
| Szopa et al[36] | √ | √ | √ | √ | √ | X | √ | ? | ? | √ | ? | √ | 8 |
| Amsters et al[37] | √ | √ | √ | √ | √ | √ | X | ? | ? | √ | ? | X | 7 |
| O’Sullivan et al[38] | √ | √ | √ | √ | √ | √ | √ | ? | ? | √ | √ | √ | 10 |
| Milosavljevic et al[39] | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 12 |
| Munhoz et al[40] | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | 12 |
| Lima et al[41] | √ | √ | √ | √ | X | ? | √ | ? | ? | √ | √ | ? | 7 |
| Raine et al[42] | √ | √ | √ | X | √ | X | √ | X | X | √ | √ | √ | 8 |
| Christie et al[43] | √ | √ | √ | √ | √ | √ | √ | ? | ? | √ | √ | √ | 10 |
| Watson et al[44] | √ | ? | √ | X | √ | √ | X | ? | ? | √ | √ | √ | 7 |
| Raine et al[45] | √ | √ | √ | √ | √ | √ | √ | X | X | √ | √ | √ | 10 |
| Mitchell et al[46] | X | √ | √ | √ | √ | √ | ? | ? | ? | √ | ? | X | 6 |
| Dieck et al[47] | √ | √ | √ | √ | X | ? | √ | ? | ? | √ | √ | √ | 8 |
Downs and black criteria: (1) Is the hypothesis/objective clearly described? (2) Are the main results to be measured clearly described in the Introduction or Materials and Methods? (3) Were the characteristics of the patients included clearly described? (6) Are the main findings of the study clearly described? (7) Does the study estimate the random variability in the data of the main results? (9) Were the characteristics of the lost patients described in the study? (10) Were the true probability values reported for the main results? (11) Are the subjects asked to participate in the study representative of the entire population where they were recruited? (12) Are the subjects recruited to participate in the study representative of the entire population where they were recruited? (16) If any of the results of the study were based on “data dredging”, was it clear? (18) Were statistical tests used to assess the main results appropriate? (20) Were the main results evaluated accurate (valid and reliable)? Responses to the criteria: √: Yes; X: No; ?: Unable to determine.
The 35 studies included in this review that use photogrammetry as a tool to evaluate the spine in the sagittal and frontal planes are presented and described (Table 2). The aspects related to the objective, the type of study, the methodology and the results of the studies are also shown.
Table 2.
Synthesis of the 35 studies included in this systematic review
| Ref. | Objective | Type of study | Methodology | Results |
| Almeida et al[15] | To assess the correlation between pulmonary function and posture; to investigate the correlation between body composition and body posture | Observational | n = 34 adult patients with asthma. Measurements: Bioelectrical impedance, spirometry, whole-body plethysmography, measurement of diffusing capacity for carbon monoxide and assessment of respiratory muscle strength. The lumbar lordosis was assessed by the pelvic anteversion (PAS) | The patients exhibit lumbar hyperlordosis. These postural abnormalities correlate with patients' pulmonary function and body composition |
| Cheng et al[16] | To investigate the influence of lower body stabilization and pencil design on body biomechanics (postural alterations) in children with CP | Observational | n = 14 children with CP. In the posterior view was measured the trunk lateral inclination angle and posterior superior iliac spine-C7/L4 angle; and in the lateral view was measured the trunk forward inclination angle (AutoCAD software) | A chair which provides proper positioning was effective in improving trunk posture in children with CP during handwriting activity. A pencil with assigned grip height or with a biaxial design, when compared with a regular one, could improve trunk alignment |
| Fortin et al[17] | To explore differences in standing and sitting postures and to compare differences between thoracic and thoraco-lumbar or lumbar scoliosis | Observational | n = 50 (29 thoracic scoliosis, 14 thoraco-lumbar scoliosis and 7 lumbar scoliosis). The cervical lordosis (sagittal plane) and scoliosis (frontal plane) was assessed by angles in standing and sitting positions (software program developed by their multidisciplinary team) | The cervical lordosis was not different in the two postures and scoliosis angle was significantly lower in the standing position. No significant difference was found for the index scoliosis angle in groups of scoliosis |
| Annetts et al[18] | To investigate the difference in lumbar angle and neck angle when comparing four seating designs; and consider the postures adopted on the four chairs in relation to an "ideal" posture | Observational | n = 14. The lumbar and neck angle was assessed in sit posture in the four seating designs (Matlab programme) | All chairs also resulted in a negative value for the lumbar region indicating a lordotic posture was adopted. All chairs resulted in a positive value for neck angle demonstrating the extent of the forward head position. No chair seemed to consistently produce an ideal posture across all regions |
| Weber et al[19] | To evaluate the relationship between cervical lordosis, and forward head posture and head position | Observational | n = 80 women. The cervical curvature was measured by the horizontal distance from a vertical line tangent (postural assessment software - SAPO®). Three angles measured the position of the head: Head flexion/extension (between C7, tragus and palpebral commissure), forward head posture A1 (between line of the tragus-C7 with the horizontal), and forward head posture A2 (between the external acoustic meatus, chin and sternal notch) | There were negative moderate and significant correlation between cervical lordosis and forward head posture A1. There were moderate and significant correlation between cervical lordosis and head flexion/extension |
| Edmondston et al[20] | To examine the extension mobility of the thoracic spine; and to evaluate the influence of the thoracic kyphosis on the thoracic extension range of motion, and the end range extension position | Observational | n = 40. The thoracic mobility was measured by kyphosis angle between T1, T6 e T12, in standing, sitting, 4-point kneeling, and prone lying (ImageJ Software) | The total sagittal range of motion in standing was 20.2° ± 6.6°, consisting of 8.7° ± 5.8° of extension and 11.5° ± 3.7° of flexion. The mean amount of thoracic angle was 21.6° ± 5.6°. The magnitude of the thoracic kyphosis was associated with the end range extension position but not with the range of motion toward extension |
| Milanesi et al[21] | To verify the impact of the mouth breathing occurred in the childhood on the body posture in the adult age | Observational | n = 24 study group (subjects with history of mouth breathing during childhood) and 20 control group. The cervical and lumbar lordosis were assessed by angles and distances; and the thoracic kyphosis was assessed by angle (postural evaluation software-SAPO v 0.68®) | The cervical lordosis angle and the cervical distance measures were larger in the study group. The lumbar lordosis angle was smaller in the study group, meaning greater lumbar lordosis in these subjects. No significant difference was observed between the groups for thoracic kyphosis and lumbar distance |
| de Oliveira Pezzan et al[22] | To analyze the influences of wearing wedge high-heeled shoes on lumbar lordosis angle among adolescents who were users and nonusers of high-heeled shoes and to correlate these angles with ages and the time of high-heel use | Observational | n = 50 UG and n = 50 NUG of high-heeled shoes. The photographs were taken in a barefoot condition and with high-heeled shoes. Lumbar lordosis was assessed by angle (Postural Analysis Software) | The UG had lower lordosis angles compared with the NUG. In the barefoot condition, the lumbar lordosis angle in the NUG decreases, whereas the UG increases. In the high-heeled condition, the lumbar lordosis angles in the UG increased and in the NUG decreases |
| Yang et al[23] | To analyze the correlation between cost density and cosmetic outcomes in the surgical treatment of AIS | Observational | n = 58 cases of IAS. Measurements: Photographic preoperative and follow-up and determination of cost. The scoliosis was assessed by angles (trunk shift and rib hump) and distances (waist line asymmetry) (Adobe Photoshop CS4) | On all post-operative photographic variables measured there was no statistically significant correlation between increasing cost density and change in cosmetic variables from pre-op to follow-up |
| Silveira et al[24] | To assess postural changes based on age and their association with the respiratory function in mouth breathing children | Observational | = 17 nasal breathing and 17 mouth breathing children. The pulmonary function was assessed by forced spirometer. It was assessed the neck lordosis and lumbar lordosis angle (Fisiometer®3.0 Software) | Mouth-breathing children have neck hyperlordosis which increase with age, besides reduction in spirometry values. There was no difference in the lumbar lordosis between the groups |
| Iunes et al[25] | To analyze the efficacy of the Klapp method for treating scoliosis | Randomized clinical trial | n = 16 patients with scoliosis. The cervical lordosis, thoracic kyphosis and lumbar lordosis were assessed by angles (ALCimagem® - 2000 software) before and after of treatment with 20 sessions of the Klapp method | Only the lumbar lordosis angle suffered modification post-intervention with Klapp method, with a trend to its decrease |
| Belli et al[26] | To assess the body posture of children with asthma compared to a non-asthmatic control group matched for gender, age, weight and height | Observational | n = 30 asthmatic children and 30 control group. The cervical lordosis, thoracic kyphosis and lumbar lordosis was assessed by angles (ALCimagem®-2000 software) | A significantly lower thoracic kyphosis angle value was observed in the asthmatic children. However, no significant differences were found between groups for the other angles |
| Chase et al[27] | To determine whether a sample of children and adolescents with STC had trunk musculoskeletal characteristics different from age- and sex-matched control subjects | Observational | n = 40 subjects with STC and 40 control subjects. The passive angle of the trunk flexion-extension was measured in the in prone-lying and trunk forward flexion and sagittal plane sitting posture was assessed by measurement of thoracolumbar flexion-extension angle (ImageJ Software) | There was no difference in spinal mobility between the two subject groups. The thoracolumbar flexion angle during sitting was statistically higher in the STC group than control group |
| Iunes et al[12] | To compare the agreement between the visual postural assessment carried out and the postural assessment carried out through computerized photogrammetry | Observational | n = 21. Evaluations: Visual postural assessment and computerized photogrammetry. In the photogrammetry, the cervical lordosis, thoracic kyphosis and lumbar lordosis were assessed by angles (ALCimagem®-2000 software) | For the cervical lordosis, thoracic kyphosis and lumbar lordosis it was not possible to compare the visual analysis with that from photogrammetry because there are not reports in the literature about normality values of the vertebral curvatures |
| Iunes et al[28] | To compare cervical spine alignment among individuals, with and without TMD | Observational | n = 90 (30 control group, 30 muscle signs and symptoms of TMD and 30 muscle signs and symptoms of TMD such as established diagnoses of dislocation and joint disorders). The cervical lordosis was assessed by angle (ALCimagem®-2000 software) | There were no differences among the three groups regarding cervical lordosis. The presence of TMD did not influence cervical posture, independent of TMD type or lack |
| Penha et al[29] | To quantitatively characterize spinal posture to verify any differences in the postural aspects analyzed and their possible correlation to sex or age in 7- and 8-year-old public school students in the city of Amparo, São Paulo, Brazil | Observational | n = 230 (115 in 7-year-old and 115 in 8-year-old). The thoracic kyphosis, lumbar lordosis and lateral spinal deviation were assessed by angles (CorelDraw v.11.0 software) | Only the group of 7-year-old boys showed lower angles in the lumbar lordosis from the other groups. In the thoracic kyphosis, there was a difference between the age groups, the 8-year-old children were more kyphotic than the 7-year-old. Eighty eight point seven percent of the children showed lateral spinal deviation. The most common side was to the left, the most frequent location was thoracic, and the proportion of the deviation was greater for boys (63%) than for girls (45%) |
| Rodrigues et al[30] | To measure the degree of thoracic kyphosis in older adult women with and without spinal osteoporosis and to verify the difference between the obtained values | Observational | n = 12 (6 women with a spinal osteoporosis and 6 women with a spinal osteopenia). The thoracic kyphosis was measured by angles (Autocad-2006) | The degree of thoracic kyphosis of the women with osteoporosis (66.8°) were higher when compared with the values of the women with osteopenia (53.0°) |
| Straker et al[31] | To evaluate the relationships between cervical, thoracic and lumbar sagittal sitting postures and adolescent prolonged NSP, with consideration of gender | Observational | n = 1593 adolescents. NSP was assessed by a questionnaire. It was assessed the cervicothoracic, lumbar and trunk angles in three static sitting postures: Looking straight ahead, looking down at their lap, and sitting slumped (Peak Motus motion analysis system v.8) | There were significant differences between gender in cervicothoracic, lumbar and trunk angles. Females showed more erect and lordotic postures when looking straight ahead. Adolescents with prolonged NSP sat with a more flexed cervicothoracic angle, a lower extended trunk angle, and a lower lordotic lumbar angle |
| Iunes et al[32] | To assess whether the frequency of high heel use has any influence on postural changes, and whether the type of high heel interferes in the posture | Observational | n = 40 (20 women that wore high-heeled shoes every day and 20 women that wore high heels occasionally to social functions). The subjects were photographed wore a two-piece swimsuit and no shoes. The cervical lordosis, thoracic kyphosis and lumbar lordosis were assessed by angles (ALCimagem® - 2000 software) | The frequency of use and type of high heel did not modify static posture in women |
| Smith et al[3] | (1) To determine whether photographic assessment could result in similar subgroups to previous, radiographically determined subgroups and clinically used subgroups of sagittal standing posture; (2) To explore the profiles of the clusters on gender, height and weight, and to explore the relationship of various spinal pain variables with identified clusters | Observational | n = 766 adolescents. Back pain experience was assessed by a questionnaire contained 130 questions. It was assessed the lumbar and trunk angle (Peak Motus motion analysis system) | Using 2-dimensional photographic images, the standing, sagittal thoraco-lumbo-pelvic alignment of adolescents can be classified into 4 groups: Neutral, sway, hyperlordotic, and flat. Adolescents classified as having non- neutral postures when compared with those classified as having a neutral posture demonstrated significantly higher odds for back pain ever |
| Yi et al[33] | To investigate the relationship between diaphragm excursion and spinal curvatures in mouth breathing children | Observational | n = 52 children (22 nose breathing group - control and 20 mouth breathing group). Images of diaphragm excursion were recorded using anteroposterior X-ray. The cervical lordosis, thoracic kyphosis and lumbar lordosis were assessed by angles (postural evaluation software-SAPO) | There is no relationship between spinal curvatures and diaphragm excursion in the groups studied |
| Min et al[34] | To describe the WBKA measured on preoperative clinical photographs and its significance in operative planning | Observational (retrospectively) | n = 11 patients who underwent lumbar spine osteotomy. The WBKA were measured in preoperative and at the last follow-up (mean 4 yr) | The average WBKA was 41 degrees (20 to 70 degrees) preoperatively and was 10.5 degrees (8 to 14 degrees) at the last follow up |
| Straker et al[35] | To test the hypothesis that the duration of computer use is associated with habitual postures in male and female adolescents | Observational | n = 884 adolescents. The computer use was assessed by questionnaire. The angles of thoracic flexion (line of C7 to T12 with respect to vertical), cervico-thoracic angle (angle between line of tragus to C7 and line of C7 to T12), trunk (angle between line of C7 to T12 and line of T12 to greater trochanter) and lumbar (angle between line of T12 to ASIS and line of ASIS to greater trochanter) were assessed in three sitting postures: Looking down, looking straight ahead and slumped position (Peak Motus motion analysis system) | Males - sitting looking straight ahead: no significant associations were observed between levels of computer use and variable postures. Males - sitting looking down: Significant but weak linear trend was observed, with thoracic flexion increasing with computer use. Females - sitting looking straight ahead: Increasing levels of computer use associated with increased lumbar lordosis. Females - sitting looking down: increasing levels of computer use associated with decreasing lumbar angle. Males and females - sitting slumped: Increasing of computer use associated with decreasing lumbar angle, only in females |
| Szopa et al[36] | To identify and define some compensatory postural patterns in children with CP in vertical positions | Observational | n = 18 children with CP. The angle of mechanical spinal axis deviation from the anatomical axis, the relation of the plumb line to the gluteal slitin was measured in these positions: Standing with both feet, and one (right and left) foot, two-knee kneeling, one-knee (right and left) kneeling and sitting (software manufactured by INFOMED) | Two main compensational postural patterns were distinguished on this basis in hemiparetic children, called antigravitational and progravitational posturing. The lateral curve of the spine in both types was directed towards the healthy body side, but in the antigravitational type the healthy side was the overloaded one, whereas in the progravitational type it was the unweighted one |
| Amsters et al[37] | To compare the posture of people with tetraplegia of short duration and long duration, in a static but functional position in a manual wheelchair | Observational | n = 30 people with tetraplegia; n = 30 control group. The thoracic kyphosis was assessed in sit posture in the wheelchair by chest angle | Significantly greater of the kyphosis thoracic were demonstrated for the tetraplegic group compared with able-bodied groups |
| O’Sullivan et al[38] | To examine whether a relationship exists between spinal posture and LBP in a specific sub-group of industrial workers who reported flexion-provoked pain | Observational | n = 21 control subjects and 24 LBP subjects. The low back pain was assessed by questionnaire. The lumbar lordosis was measured as the angle between the intersection of the tangents drawn through the T10/L2 markers and the L4/S2 markers. Positions: Natural sitting and maximal slumped sitting postures, natural standing and maximal sway standing postures, and lifting and maximal standing lumbar flexion postures (Scion Image analysis software) | No difference was observed between the two groups when comparing their "usual" sitting, standing and lifting lumbar flexion angles. When comparing the lumbar angle difference between "usual" sitting and maximal slumped sitting, the LBP group sat significantly closer to their end of range lumbar flexion in their "usual" sitting posture |
| Milosavljevic et al[39] | To determine whether adaptive postural and movement characteristics were evident in the thoracic and lumbar spine as well as the hips of shearers, and to determine whether any observed adaptive changes were associated with either current or previous LBP | Observational | n = 64 shearers and 64 non-shearers. Lumbar sagittal lordotic posture was determined by cord angular change between T12, L3 and the PSIS and it was expressed in radians per metre (rad/m). Mid-upper and mid-lower sagittal thoracic curves were also calculated and expressed in rad/m about the T1, T4, T8, and T4, T8, T12 respectively. Three positions were analyzed: Flexion, normal stance, extension (CAD program) | The mean value for lumbar extension for shearers (9.88) was significantly less than for non-shearers (14.08). Lumbar flexion demonstrated similar mean scores for both groups and no significant differences were noted. Lower thoracic curvature for shearers (2.14 rad/m) was significantly "flatter". than for nonshearers (2.48 rad/m). Comparisons of both lumbar lordosis as well as upper thoracic kyphosis did not demonstrate any significant differences between the two groups. In the non-shearing group, participants with previous LBP had significantly reduced ranges of lumbar extension and lumbar flexion. Shearers with previous LBP did not demonstrate any significant reduction of either of these ranges of lumbar motion. The mean lumbar extension in the non-shearing subgroup with previous LBP was still greater than that of the shearer group |
| Munhoz et al[40] | To investigate the relationship between internal derangements of the TMJ and body posture deviations | Observational | n = 50 (30 individuals with TMJ internal derangement and 20 control group). The cervical lordosis, thoracic kyphosis and lumbar lordosis were assessed by distances of the most prominent region until of the plumb line (CorelDraw v.9.0 software) | No statistically significant body postural differences between the groups were observed |
| Lima et al[41] | To determine and compare the posture of children with OMB and FMB in relation to NB children | Observational | n = 62 children (17 OMB group, 26 FMB group and 19 NB group). The cervical lordosis, thoracic kyphosis, lumbar lordosis and lateral deviation of the spine were assessed by angles (ALCimagem®-2000 software) | Significant alterations were observed in cervical straightening in the OMB group. Significant changes were observed in the thoracic kyphosis, indicating convexity in the OMB group. For the lumbar lordosis and lateral deviation of the spine, no significant alterations were observed in any of the groups |
| Raine et al[42] | To quantitatively describe the curvature of the thoracic spine in the sagittal plane | Observational | n = 160 asymptomatic men and women. The upper and lower thoracic kyphosis was assessed by the tangent angles in radians/mm between C7-T6 and T6-T12, respectively | Results of thoracic kyphosis were not shown |
| Christie et al[43] | To evaluate any static standing or sitting postural aberrations in chronic and acute low back pain patients in comparison with healthy individuals, in search of potential risk factors or associations for LBP | Observational | n = 59 (39 participants with LBP and 20 control group). Pain intensity was recorded using a VAS. The subjects were divided in acute and chronic pain. The lumbar lordosis and thoracic kyphosis was assessed by angles between C7-T12 and T12-L5, respectively, in standing and sitting positions | Standing positions: The chronic pain group had a significantly increased lordosis compared with the control group. The acute group had an increased kyphosis than the control group. Lumbar lordosis is the parameter most important in prediction of LBP group. Sitting positions: individuals with acute pain had an increased thoracic kyphosis. Thoracic kyphosis, indicated contribution to the prediction of study group |
| Watson[44] | To investigate possible relationships between the incidence of sports injury and the existence of body posture defects in football players | Observational | n = 52 football players (soccer, rugby, Gaelic football). The injuries were divided in four categories: Back injuries, knee injuries, ankle injuries and muscle strains. The assessment of the scoliosis, thoracic kyphosis and lumbar lordosis were not clear | Back injuries were associated with thoracic kyphosis, lumbar lordosis and scoliosis. Subjects who suffered from two, three or all four types of injuries had significantly lower scores for lordosis than subjects who sustained less than two types of injuries |
| Raine et al[45] | To identify gender differences in the thoracic kyphosis and to correlate thoracic kyphosis with head and shoulder position | Observational | n = 39. The upper (C7-T6) and lower (T6-T12) thoracic curvature were measured from the surface contour of the thoracic spine by the tangent angles in radians/cm (GTCO digitizer) | No significant difference between females and males for the measurement of upper thoracic, however the lower thoracic was significant higher in males. The sagittal plane head alignment was negatively correlated with upper thoracic curvature; there was increased curvature of the upper thoracic spine when the head was placed more anteriorly |
| Mitchell et al[46] | To report a new method of measuring the angle of curvature of the lumbar spine in pregnant women | Observational | n = 13 pregnant women. The lumbar lordosis was assessed by angle between T12-L1 and L5-S1 | The degree of lumbar spine curvature in pregnant women was 33.9° (± 3.6°) |
| Dieck et al[47] | To examine the relationship between postural asymmetry and the subsequent development of back and neck pain | Observational | n = 903 women. Back and neck pain and risk factors were obtained by questionnaire. Deviation of the spine from de midline of the body to scoliosis measurement was assessed by angle | There was no evidence of a relationship between increasing midline deviation and subsequent low back pain |
PAS: Postural Assessment Software; CP: Cerebral palsy; AIS: Adolescents idiophatic scoliosis; STC: Slow transit constipation; TMD: Temporomandibular disorder; UG: Users group; NUG: Nonuser group; NSP: Neck/shoulder pain; WBKA: Whole body kyphosis angle; LBP: Low back pain; TMJ: Temporomandibular Joint; OMB: Obstructive mouth breathing; FMB: Functional mouth breathing; NB: Nasal breathing; VAS: Visual analogue scale.
Of the studies in which photogrammetry is used as a postural assessment tool, only one involves a randomized clinical trial, while the others are observational studies. Regarding study populations, most studies involved adults, followed by children and adolescents, while a few studies involved populations with specific diseases that may affect some aspect of posture was evaluated (Table 2).
The vast majority of studies included in this systematic review are concerned with evaluating the sagittal curvature of the spine, while scoliosis is evaluated in only eight studies. To achieve their objectives, several mathematical routines are used in the postural evaluation software programs to measure the alterations in the spine. Most, whether for the frontal or sagittal plane, used angular and/or linear values to measure the magnitude of the spinal alterations (Table 2).
DISCUSSION
This systematic review aimed to verify the applicability of photogrammetry and to identify the mathematical procedures involved in the use of this technique to evaluate the posture of the spine. Among the 35 articles included in this study, there is considerable similarity regarding the applicability of photogrammetry within scientific circles. However, there are important differences in the mathematical procedures used to evaluate the spine. Next, the articles included in this review were analyzed by groups, regarding the methodology used to collect and analyze data with photogrammetry: (1) type of study; (2) evaluated population; (3) region of the spine and type of alteration evaluated; and (4) types of mathematical procedures.
Comparing the studies in which photogrammetry is used as a postural evaluation tool, only one study is a randomized clinical trial[25], all the others being observational studies. The reason for not using this tool in “trial” studies of type “trials” is unclear, since photogrammetry is recognized as a valid and reproducible instrument for monitoring treatment progression, both in clinical practice and research[5,6,25,48]. Among the possible explanations for these findings are the lack of free access software for evaluating the spine and/or recent use of digital photographs and analysis software for the use in large intervention studies[1].
Furthermore, the difficulty involved in treating conditions related to spinal posture may also go some way to explain these results, since this body segment is highly influenced by mechanical, social, political and psychological factors[49].
As nearly all the studies presented in this systematic review were cross-sectional, their objectives varied according to the population assessed, making it possible to evaluate some specific characteristics of spinal posture in the groups involved. Moreover, photogrammetry is particularly useful for that purpose because it is capable of recording subtle transformations and so is able to quantify the morphological variables related to posture[2,3]. Some specific populations were evaluated using photogrammetry, such as adults[12,19,20,42,45,47], children and teenagers[3,29,31,35], pregnant women[46] and athletes[44]. In some studies, where the samples consisted of adults, some utensils (e.g., chairs and high-heeled shoes) are used in order to verify any change in the posture of the spine during their use[18,22,32].
Similarly, some studies include patients with various diseases, where the authors believe they have a relationship with spinal posture. There are articles in which the samples comprise patients with asthma[15,26], tetraplegia[37], cerebral palsy[16,36] temporomandibular joint dysfunction[28,40], osteoporosis and osteopenia[30], low back pain[38,43], slow transit constipation[27] and children with mouth breathing[21,24,33,41].
With regard to the region of the spine evaluated, greater difficulty has been documented in evaluating the sagittal plane compared to the frontal plane. This may be explained by the fact that, in the frontal plane, symmetry between the right and left sides and straightness of the spine can be expected[6,12]. By contrast, in the sagittal plane, the spine presents physiological curvatures and changes characterized by an increase or decrease in the magnitude of the curvatures[50], which hinders visual and subjective evaluation. In an attempt to quantify the magnitude of the curvatures, various mathematical procedures have been proposed for evaluating the sagittal curvature of the spine. Possibly for this reason, about 80% of the studies found in this systematic review attempted to evaluate cervical lordosis, thoracic kyphosis and lumbar lordosis, while only eight articles evaluated the existence of scoliosis[16,17,23,29,36,41,44,47].
Nevertheless, in the literature, there is still a need for postural evaluation software that can be used to do more than quantify joint angles and the distances between the segments, which, in addition can, be used to provide a diagnostic classification of changes in the magnitudes of the spine in individuals. To achieve this, normality values of body segments need to be established in the literature. However, regarding the spine, there is some controversy in relation to the reference values for the angles of curvature in the sagittal plane in the ideal alignment[12].
The data collection protocols in the studies using photogrammetry as an evaluation tool tend to be very similar, differing minimally according to the purpose of each evaluation. All the methods are based on basic procedures such as: (1) preliminary preparation of the collection location with standardized location of the camera and the subject; (2) palpation and marking of anatomical reference points; and (3) photographic records of individuals in certain positions[2,8,9,45].
However, concerning the data analysis procedures, various software and digital routines are used for scanning anatomical landmarks. Similarly, the mathematical procedures adopted in software or digital routines are very different[51]. Nevertheless, in most cases, the studies do not provide information on the mathematical procedures adopted in the software or in digital routines that support the evaluation results. Allied to this, in some cases the software is not freely available, which makes it difficult to reproduce the evaluation method in other studies.
Therefore, we emphasize the wide divergence of software and mathematical procedures found in this review. Among the known and validated software packages used repeatedly in the selected articles are ALCimagem®-2000[12,25,26,28,32,41], Postural Assessment Software (PAS)[15,19,21,22,33], Peak Motus Motion Analysis System[3,31,35], CorelDraw[29,40], AutoCad[16,30] and Image J Software[8,27].
As regards the various mathematical routines embedded in these systems, angular and linear values have been the most widely used to measure alterations of the spine in the frontal and sagittal planes, i.e., to determine the magnitudes of scoliosis and anteroposterior curvatures, respectively. Figure 2 illustrates some of the techniques used to measure the spinal alterations.
Figure 2.
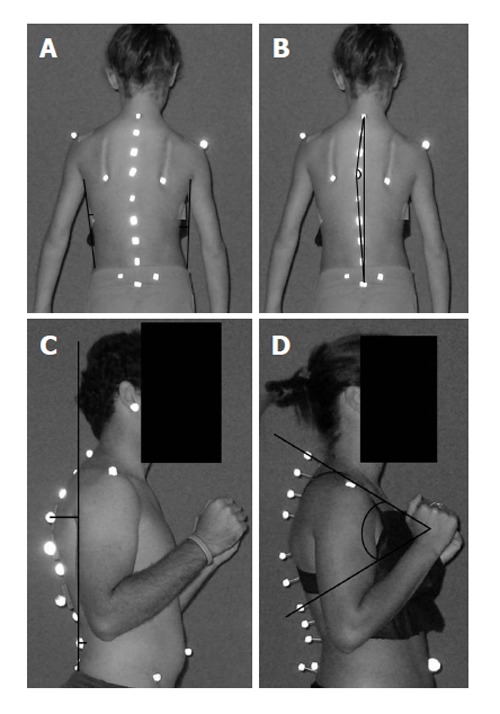
Examples of the techniques used to measure spinal curvature found in the articles composing the present systematic review. A: Linear values for scoliosis evaluation[23]; B: Angular values for scoliosis evaluation[17]; C: Linear values for thoracic and lumbar curvatures[21]; D: Angular values for thoracic curvature[30]. The images used are illustrations prepared for the present study.
The angular values are often used, since the gold standard of postural assessment uses an angular calculation to measure the degree of scoliosis and the magnitude of the sagittal curvature of the spine. In other words, in the X-ray examination of the spine it is possible to calculate the so-called Cobb angle, which is widely used for diagnosis of spinal posture[52].
Some of the selected studies evaluate the angles of scoliosis using photogrammetry in a similar way to the Cobb angle[17,23]. However, while the Cobb angle uses the vertebral bodies for evaluation, photogrammetry calculates the magnitude of the curve through the spinal processes of the vertebrae of interest. For this evaluation, two lines are drawn joining the spinous processes and the angle between these lines gives the angle of curvature[17,23].
The linear values in the frontal plane are established according to the statement that the spine should be a straight line[6]. Hence, methodologies calculate postural alteration by the degree to which marked points, referring to the spinous processes, deviate from the vertical line[23,29,36,47].
In the sagittal plane, angular values are more often used than linear values for evaluating the anteroposterior curvatures of the spine.
Similar to the Cobb angle, photogrammetry is recommended for use in evaluating the spinal curvature based on the calculation of the angle between two points on the spine[30,43,46]. However, it uses the spinous processes as a reference, while radiography uses the vertebral bodies.
Nevertheless, it should be noted that the spinous processes have an angle of inclination in relation to the vertebral body[53] and that this angle may interfere with obtaining the angle of curvature by photogrammetry. Thus, caution is recommended when using a similar method to the gold standard in the mathematical procedures of postural evaluation software, since palpated anatomical landmark and used with reference is totally different.
When the photogrammetric evaluation software resembles the way of measuring the magnitude of the curves, they diverge in relation to vertebral levels used or anatomical landmarks. When distinct marked points are used, the calculation of curvatures will be modified, making it difficult to compare studies. In the studies included in this systematic review, some vertebral levels reported for thoracic kyphosis were between: C7-T12[43], T1-T4-T8[39], T4-T8-T12[39] and T1-T6-T12[20]. For lumbar lordosis they were between T12-L5[43], T12-Anterior superior iliac spine - femur greater trochanter[3,31,35].
Besides the similarity with the calculation of Cobb angle, some recurring angular values were calculated angles for the three curvatures: (1) cervical lordosis: the union of three lines passing through occipital, C4 and C7 until a later vertical line; (2) thoracic kyphosis: The union of three lines passing through C7, T7 and T12 until a posterior-vertical line; and (3) lumbar lordosis: Union of three lines passing through T12, L3 and L5 posterior to a vertical line[12,22,25,26,28]. Among these possibilities for measuring sagittal curvature, routines based on other types of calculations were also found, such as the curvatures of the contour tangent[38,42,45], torso angle[3,16,31,35], and chest angle[37].
According to the theories that use linear values to evaluate the spine in the sagittal plane, alterations in the curvature can be quantified by measuring the distance from the spinous process to a vertical reference line. In rectified curvatures, the distances decrease, while in increased curvatures the distances increase[6].
Despite the wide range of mathematical procedures that can be used to quantitatively evaluate the spine, inserted in photogrammetry, in clinical practice and research, health professionals and students are often faced with a scarcity of tools that allow them to classify an individual’s posture. In other words, the angular or linear results provided by software often lack clinical significance because they are not equivalent to the gold standard. Thus, the benefits, limitations, target audience, and use characteristics of photogrammetry need to be carefully considered when selecting the software and/or mathematical procedure in order to facilitate the correct choice of evaluation methodology for different situations, both in clinical and in scientific research.
The present systematic review shows that photogrammetry can be widely used in the scientific research environment, because it facilitates the collection and analysis of detailed data, thus permitting assessment not only of the spine but also of other body segments in both the sagittal and frontal planes. On the other hand, in the school environment, data collection should prioritize simplified protocols, thus facilitating the assessment of large populations. Moreover, the software and mathematical procedures for the postural analysis should be easily available, as are PAS and ALCimagem®-2000. In the clinical environment, the choice of photogrammetric data collection and of the assessment protocol will depend on the purpose of the postural evaluation, as well as the health professional’s investigative focus, so that a simplified or more complete assessment protocol can be used.
A wide range of studies was found to use photogrammetry as a tool for non-invasive evaluation of the spine, both for measurement of anteroposterior and lateral alterations. However, most of the selected articles were observational studies, only one being a randomized clinical trial.
Yet, it was also observed that, although the data collection methodologies used are similar across the studies, they are very different concerning aspects of data analysis, especially with regard to the mathematical routines that support the different software packages for postural evaluation. Finally, even though photogrammetry is a viable, valid and reproducible option for the evaluation of the spine, there is still a lack of studies in the literature showing software whose results provide both the magnitude of the curvatures and the diagnostic classification of the posture of the spine, certified with clinical significance.
COMMENTS
Background
Photogrammetry is a widely used non-invasive technique for measuring aspects of the spine for the purpose of postural evaluation. Its use undoubtedly contributes to reducing exposure to radiation and thus enables the monitoring of postural treatment. However, the application of this technique in postural evaluation is directly dependent on both the collection procedures and the mathematical methods used to provide measurements and postural diagnoses. Although the use of photogrammetry in spinal evaluation is widespread, its applicability may be questioned, as it remains unclear how this technique is being used to monitor postural treatment or to map attitudes among populations in observational studies.
Research frontiers
Essentially, the problem is two different researchers can look at the same image and arrive at different conclusions regarding diagnosis because they use distinct mathematical methods. Hence, there is a need to identify the best method of using photogrammetry to accurately measure spinal curvatures.
Innovations and breakthroughs
To be best of the authors’ knowledge there is no systematic review which brings together the protocols and mathematical methods involved when it is applied in the assessment of spinal posture. Hence, the aim of this study is to present, in a concise way, the articles dealing with the application of photogrammetry in postural evaluation, so researchers can more easily discuss the suitability of the procedures currently being applied.
Applications
With photogrammetry, the aim of the assessment, whether it is for clinical, research or collective health purposes, must be considered when choosing which protocol to use to evaluate spinal posture. When using photogrammetry in scientific research, a protocol or software that provides detailed postural analysis should be the first choice. In the clinical environment, the choice of protocol will depend on the objectives established for the patient by the physiotherapist. When dealing with a collective health situation, such as groups of schoolchildren, it is necessary to prioritize simpler protocols.
Terminology
Photogrammetry: Is the technique of determining measurements based on photographs. The Cobb angle: Is used to measure the spinal curvatures, defined as the angle formed between a line drawn parallel to the superior endplate of one vertebra above the curvature and a line drawn parallel to the inferior endplate of the vertebra one level below the curvature.
Peer-review
This article demonstrates an in-depth review of the available literature on the application of photogrammetry in postural evaluation.
Footnotes
Conflict-of-interest statement: All the authors declare that they have no competing interests.
Data sharing statement: The dataset is available from the corresponding author at jefferson.loss@ufrgs.br.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: May 5, 2015
First decision: June 20, 2015
Article in press: December 4, 2015
P- Reviewer: Bicanic G, Robertson GA S- Editor: Qiu S L- Editor: A E- Editor: Liu SQ
References
- 1.Carman DL, Browne RH, Birch JG. Measurement of scoliosis and kyphosis radiographs. Intraobserver and interobserver variation. J Bone Joint Surg Am. 1990;72:328–333. [PubMed] [Google Scholar]
- 2.Dunk NM, Lalonde J, Callaghan JP. Implications for the use of postural analysis as a clinical diagnostic tool: reliability of quantifying upright standing spinal postures from photographic images. J Manipulative Physiol Ther. 2005;28:386–392. doi: 10.1016/j.jmpt.2005.06.006. [DOI] [PubMed] [Google Scholar]
- 3.Smith A, O’Sullivan P, Straker L. Classification of sagittal thoraco-lumbo-pelvic alignment of the adolescent spine in standing and its relationship to low back pain. Spine (Phila Pa 1976) 2008;33:2101–2107. doi: 10.1097/BRS.0b013e31817ec3b0. [DOI] [PubMed] [Google Scholar]
- 4.Fortin C, Feldman DE, Cheriet F, Gravel D, Gauthier F, Labelle H. Reliability of a quantitative clinical posture assessment tool among persons with idiopathic scoliosis. Physiotherapy. 2012;98:64–75. doi: 10.1016/j.physio.2010.12.006. [DOI] [PubMed] [Google Scholar]
- 5.D’osualdo F, Schierano S, Cisotti C. The evaluation of the spine through the surface: The role of surface measurements in the evaluation and treatment of spine diseases in young patients. Eura Medicophys. 2002:38; 147–152. [Google Scholar]
- 6.Furlanetto TS, Candotti CT, Comerlato T, Loss JF. Validating a postural evaluation method developed using a Digital Image-based Postural Assessment (DIPA) software. Comput Methods Programs Biomed. 2012;108:203–212. doi: 10.1016/j.cmpb.2012.03.012. [DOI] [PubMed] [Google Scholar]
- 7.Masso PD, Gorton GE. Quantifying changes in standing body segment alignment following spinal instrumentation and fusion in idiopathic scoliosis using an optoelectronic measurement system. Spine (Phila Pa 1976) 2000;25:457–462. doi: 10.1097/00007632-200002150-00011. [DOI] [PubMed] [Google Scholar]
- 8.Edmondston SJ, Christensen MM, Keller S, Steigen LB, Barclay L. Functional radiographic analysis of thoracic spine extension motion in asymptomatic men. J Manipulative Physiol Ther. 2012;35:203–208. doi: 10.1016/j.jmpt.2012.01.008. [DOI] [PubMed] [Google Scholar]
- 9.Letafatkar A, Amirsasan R, Abdolvahabi Z, Hadadnezhad M. Reliability and validity of the AutoCAD software method in lumbar lordosis measurement. J Chiropr Med. 2011;10:240–247. doi: 10.1016/j.jcm.2011.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 10.Leroux MA, Zabjek K, Simard G, Badeaux J, Coillard C, Rivard CH. A noninvasive anthropometric technique for measuring kyphosis and lordosis: an application for idiopathic scoliosis. Spine (Phila Pa 1976) 2000;25:1689–1694. doi: 10.1097/00007632-200007010-00012. [DOI] [PubMed] [Google Scholar]
- 11.van Niekerk SM, Louw Q, Vaughan C, Grimmer-Somers K, Schreve K. Photographic measurement of upper-body sitting posture of high school students: a reliability and validity study. BMC Musculoskelet Disord. 2008;9:113. doi: 10.1186/1471-2474-9-113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Iunes DH, Bevilaqua-Grossi D, Oliveira AS, Castro FA, Salgado HS. Comparative analysis between visual and computerized photogrammetry postural assessment. Braz J Phys Ther. 2009;13:308–315. [Google Scholar]
- 13.Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions. 2014. Available from: http//handbook.cochrane.org/v5.0.2/ [Google Scholar]
- 14.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377–384. doi: 10.1136/jech.52.6.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Almeida VP, Guimarães FS, Moço VJ, Menezes SL, Mafort TT, Lopes AJ. [Correlation between pulmonary function, posture, and body composition in patients with asthma] Rev Port Pneumol. 2013;19:204–210. doi: 10.1016/j.rppneu.2013.03.004. [DOI] [PubMed] [Google Scholar]
- 16.Cheng HY, Lien YJ, Yu YC, Ju YY, Pei YC, Cheng CH, Wu DB. The effect of lower body stabilization and different writing tools on writing biomechanics in children with cerebral palsy. Res Dev Disabil. 2013;34:1152–1159. doi: 10.1016/j.ridd.2012.12.019. [DOI] [PubMed] [Google Scholar]
- 17.Fortin C, Ehrmann Feldman D, Cheriet F, Labelle H. Differences in standing and sitting postures of youth with idiopathic scoliosis from quantitative analysis of digital photographs. Phys Occup Ther Pediatr. 2013;33:313–326. doi: 10.3109/01942638.2012.747582. [DOI] [PubMed] [Google Scholar]
- 18.Annetts S, Coales P, Colville R, Mistry D, Moles K, Thomas B, van Deursen R. A pilot investigation into the effects of different office chairs on spinal angles. Eur Spine J. 2012;21 Suppl 2:S165–S170. doi: 10.1007/s00586-012-2189-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Weber P, Corrêa ECR, Milanesi JM, Soares JC, Trevisa ME. Craniocervical posture: cephalometric and biophotogrammetric analysis. Braz J Oral Sci. 2012;11:416–421. [Google Scholar]
- 20.Edmondston SJ, Waller R, Vallin P, Holthe A, Noebauer A, King E. Thoracic spine extension mobility in young adults: influence of subject position and spinal curvature. J Orthop Sports Phys Ther. 2011;41:266–273. doi: 10.2519/jospt.2011.3456. [DOI] [PubMed] [Google Scholar]
- 21.Milanesi JM, Borin G, Corrêa EC, da Silva AM, Bortoluzzi DC, Souza JA. Impact of the mouth breathing occurred during childhood in the adult age: biophotogrammetric postural analysis. Int J Pediatr Otorhinolaryngol. 2011;75:999–1004. doi: 10.1016/j.ijporl.2011.04.018. [DOI] [PubMed] [Google Scholar]
- 22.de Oliveira Pezzan PA, João SM, Ribeiro AP, Manfio EF. Postural assessment of lumbar lordosis and pelvic alignment angles in adolescent users and nonusers of high-heeled shoes. J Manipulative Physiol Ther. 2011;34:614–621. doi: 10.1016/j.jmpt.2011.09.006. [DOI] [PubMed] [Google Scholar]
- 23.Yang S, Jones-Quaidoo SM, Eager M, Griffin JW, Reddi V, Novicoff W, Shilt J, Bersusky E, Defino H, Ouellet J, et al. Right adolescent idiopathic thoracic curve (Lenke 1 A and B): does cost of instrumentation and implant density improve radiographic and cosmetic parameters? Eur Spine J. 2011;20:1039–1047. doi: 10.1007/s00586-011-1808-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Silveira Wd, Mello FC, Guimarães FS, Menezes SL. Postural alterations and pulmonary function of mouth-breathing children. Braz J Otorhinolaryngol. 2010;76:683–686. doi: 10.1590/S1808-86942010000600002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Iunes DH, Cecílio MB, Dozza MA, Almeida PR. Quantitative photogrammetric analysis of the Klapp method for treating idiopathic scoliosis. Rev Bras Fisioter. 2010;14:133–140. [PubMed] [Google Scholar]
- 26.Belli JF, Chaves TC, de Oliveira AS, Grossi DB. Analysis of body posture in children with mild to moderate asthma. Eur J Pediatr. 2009;168:1207–1216. doi: 10.1007/s00431-008-0911-y. [DOI] [PubMed] [Google Scholar]
- 27.Chase JW, Stillman BC, Gibb SM, Clarke MC, Robertson VJ, Catto-Smith AG, Hutson JM, Southwell BR. Trunk strength and mobility changes in children with slow transit constipation. J Gastroenterol Hepatol. 2009;24:1876–1884. doi: 10.1111/j.1440-1746.2009.05940.x. [DOI] [PubMed] [Google Scholar]
- 28.Iunes DH, Carvalho LCF, Oliveira AS, Bevilaqua-Grossi D. Craniocervical posture analysis in patients with temporomandibular disorder. Braz J Phys Ther. 2009;13:89–95. [Google Scholar]
- 29.Penha PJ, Baldini M, João SM. Spinal postural alignment variance according to sex and age in 7- and 8-year-old children. J Manipulative Physiol Ther. 2009;32:154–159. doi: 10.1016/j.jmpt.2008.12.009. [DOI] [PubMed] [Google Scholar]
- 30.Rodrigues ACC, Romeiro CAP, Patrizzi LJ. Evaluation of thoracic kyphosis in older adult women with osteoporosis by means of computerized biophotogrammetry. Braz J Phys Ther. 2009;13:205–209. [Google Scholar]
- 31.Straker LM, O’Sullivan PB, Smith AJ, Perry MC. Relationships between prolonged neck/shoulder pain and sitting spinal posture in male and female adolescents. Man Ther. 2009;14:321–329. doi: 10.1016/j.math.2008.04.004. [DOI] [PubMed] [Google Scholar]
- 32.Iunes DH, Monte-Raso VV, Santos CBA, Castro FA, Salgado HS. Postural influence of high heels among adult women: analysis by computerized photogrammetry. Braz J Phys Ther. 2008;12:454–459. [Google Scholar]
- 33.Yi LC, Jardim JR, Inoue DP, Pignatari SS. The relationship between excursion of the diaphragm and curvatures of the spinal column in mouth breathing children. J Pediatr (Rio J) 2008;84:171–177. doi: 10.2223/JPED.1771. [DOI] [PubMed] [Google Scholar]
- 34.Min K, Hahn F, Leonardi M. Lumbar spinal osteotomy for kyphosis in ankylosing spondylitis: the significance of the whole body kyphosis angle. J Spinal Disord Tech. 2007;20:149–153. doi: 10.1097/01.bsd.0000211252.67576.d9. [DOI] [PubMed] [Google Scholar]
- 35.Straker LM, O’Sullivan PB, Smith A, Perry M. Computer use and habitual spinal posture in Australian adolescents. Public Health Rep. 2007;122:634–643. doi: 10.1177/003335490712200511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Szopa A, Domagalska M, Czupryna K, Plaszewski M. Postural consequences of muscle tone disorders in children with cerebral palsy (hemiparesis) Fizioter. 2007;3:241–249. [Google Scholar]
- 37.Amsters D, Nitz J. The consequences of increasing age and duration of injury upon the wheelchair posture of men with tetraplegia. Int J Rehabil Res. 2006;29:347–349. doi: 10.1097/MRR.0b013e328010f540. [DOI] [PubMed] [Google Scholar]
- 38.O’Sullivan PB, Dankaerts W, Burnett AF, Garreth TF, Jefford E, Naylor CS, O’Sullivan KJ. Effect of different upright sitting postures on spinal- pelvic curvature and trunk muscle activation in a pain-free population. Spine. 2006;31:E707–E712. doi: 10.1097/01.brs.0000234735.98075.50. [DOI] [PubMed] [Google Scholar]
- 39.Milosavljevic S, Milburn PD, Knox BW. The influence of occupation on lumbar sagittal motion and posture. Ergonomics. 2005;48:657–667. doi: 10.1080/00140130500070848. [DOI] [PubMed] [Google Scholar]
- 40.Munhoz WC, Marques AP, de Siqueira JT. Evaluation of body posture in individuals with internal temporomandibular joint derangement. Cranio. 2005;23:269–277. doi: 10.1179/crn.2005.038. [DOI] [PubMed] [Google Scholar]
- 41.Lima LC, Baraúna MA, Sologurem MJ, Canto RS, Gastaldi AC. Postural alterations in children with mouth breathing assessed by computerized biophotogrammetry. J Appl Oral Sci. 2004;12:232–237. doi: 10.1590/s1678-77572004000300014. [DOI] [PubMed] [Google Scholar]
- 42.Raine S, Twomey LT. Head and shoulder posture variations in 160 asymptomatic women and men. Arch Phys Med Rehabil. 1997;78:1215–1223. doi: 10.1016/s0003-9993(97)90335-x. [DOI] [PubMed] [Google Scholar]
- 43.Christie HJ, Kumar S, Warren SA. Postural aberrations in low back pain. Arch Phys Med Rehabil. 1995;76:218–224. doi: 10.1016/s0003-9993(95)80604-0. [DOI] [PubMed] [Google Scholar]
- 44.Watson AW. Sports injuries in footballers related to defects of posture and body mechanics. J Sports Med Phys Fitness. 1995;35:289–294. [PubMed] [Google Scholar]
- 45.Raine S, Twomey L. Posture of the head, shoulders and thoracic spine in comfortable erect standing. Aust J Physiother. 1994;40:25–32. doi: 10.1016/S0004-9514(14)60451-7. [DOI] [PubMed] [Google Scholar]
- 46.Mitchell J, Ness D. A new method of measuring the degree of lumbar spine curvature in pregnant women. Physiotherapy. 1992;48:51–54. [Google Scholar]
- 47.Dieck GS, Kelsey JL, Goel VK, Panjabi MM, Stephen WD, Laprade MH. An epidemiologic study of the relationship between postural asymmetry in the teen years and subsequent back and neck pain. Spine. 1985;10:872–877. doi: 10.1097/00007632-198512000-00002. [DOI] [PubMed] [Google Scholar]
- 48.de Oliveira TS, Candotti CT, La Torre M, Pelinson PP, Furlanetto TS, Kutchak FM, Loss JF. Validity and reproducibility of the measurements obtained using the flexicurve instrument to evaluate the angles of thoracic and lumbar curvatures of the spine in the sagittal plane. Rehabil Res Pract. 2012;2012:186156. doi: 10.1155/2012/186156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hanna T. What is somatics? Somatics. Novato Institute for Somatic Research and Training. 1986;5:4–8. [Google Scholar]
- 50.Singh DK, Bailey M, Lee R. Biplanar measurement of thoracolumbar curvature in older adults using an electromagnetic tracking device. Arch Phys Med Rehabil. 2010;91:137–142. doi: 10.1016/j.apmr.2009.08.145. [DOI] [PubMed] [Google Scholar]
- 51.Fortin C, Feldman DE, Cheriet F, Labelle H. Validity of a quantitative clinical measurement tool of trunk posture in idiopathic scoliosis. Spine (Phila Pa 1976) 2010;35:E988–E994. doi: 10.1097/BRS.0b013e3181cd2cd2. [DOI] [PubMed] [Google Scholar]
- 52.Mac-Thiong JM, Pinel-Giroux FM, de Guise JA, Labelle H. Comparison between constrained and non-constrained Cobb techniques for the assessment of thoracic kyphosis and lumbar lordosis. Eur Spine J. 2007;16:1325–1331. doi: 10.1007/s00586-007-0314-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Gilad I, Nissan M. Sagittal evaluation of elemental geometrical dimensions of human vertebrae. J Anat. 1985;143:115–120. [PMC free article] [PubMed] [Google Scholar]