

Abstract
Background:
Cancelation of surgery is a constant agonizing dilemma for nearly all healthcare services that has been intensively investigated to find out its roots, consequences, and possible solutions. The rates of cancelation of surgery vary between centers and more so among surgical specialties with numerous reasons standing behind this phenomenon.
Patients and Methods:
In the current study, analysis of monthly cancelation rates from January 2009 to December 2012, and assessment of establishing new operating rooms (ORs) using statistical process control charts was conducted. A detailed review of a total of 1813 cases canceled on the day of surgery from January to December 2012, to examine the various reasons of cancelation among surgical specialties.
Results:
The average cancelation rate was 11.1%, which dropped to 9.0% after launching of new theaters. Four reasons explained about 80% of cancelations; Patients “no show” was the leading cause of cancelation (27%). One-fourth of cancelations (24.3%) were due to the need for further optimization, and the third most prominent cause of cancelation was a lack of OR time (19.5%). Unavailability of staff/equipment/implants accounted for only 0.7% of cancelations. The no show was the most common cause of cancelation among all surgical specialties ranging from 21% for plastic surgery to 32% in ophthalmic surgeries.
Conclusion:
It was confirmed that there is a unique profile of cancelation of surgery problem for every institute, an extension of infrastructure may not be the only solution. Control charts helped to enhance the general picture and are functional in monitoring and evaluating changes in the cancelation of surgery.
Keywords: Cancelation of surgery, Saudi Arabia, Statistical process control
Introduction
Cancelation of surgery is a constant agonizing dilemma for nearly all healthcare services in terms of wastage of resources and inconvenience caused to both patients and families.[1,2] The rates of cancelation of surgery were extensively studied as there was no uniformity in the recorded rates. Different institutions reported rates of cancelation ranging from as low as 3.9%[3] to extremely high as 40%.[4] More so, various surgical specialties suffered differentially from the cancelation of surgery.[5]
Reasons behind cancelation are commonly demarcated as patient related such as being unfit for surgery or patient declining the surgical operation, facility related causes including lack of elective or Intensive Care Unit (ICU) beds or operating room (OR) time, in addition to process related such as wrong booking.[6] Some of these reasons could be considered as avertable while others cannot be avoided.[7]
Studying reasons of cancelations in various health facilities and specialties yielded nearly a unique profile of cancelation in each institution. Many centers reported the leading reasons as patient “no shows,” lack of OR time and patients not adequately prepared for the surgery.[8,9] As rectifying reasons, and roots of the problem will positively clarify the way to solve it, Cancelation of surgery should not be inferred as a “system failure” as hospitals, in which the OR time is reallocated and cases effectively rescheduled are more able to focus on assessing the performance rather than reducing the cancelation rate.[10,11]
Many studies even tried to postulate solutions and evaluated the effect of certain intervention on the rate of cancelation.[12,13,14] The National Health Service in the United Kingdom has established operations diagnostic tool to trace and record cancelations in a trial to plan effective programs for avoiding cancelations and their drawbacks.[15]
Cancelation of surgery was intensively studied using a wide range of statistical methodologies ranging from merely reporting the rates to more advanced approaches, which are considered as important additions contributing to the depth and understanding of cancelation of surgery.[16,17,18] A relatively recent statistical approach of assessing the variations encountered in the medical field is to use statistical process control (SPC) analysis. Using SPC to assess the variation of cancelation rates can help not only to clarify the baseline situation, but it can concurrently be used to track improvement of rates over time when intervention is applied.[19,20]
The objective of the current study was to investigate the cancelation of surgery in terms of their rates, and reasons while simultaneously assessing the effect of new OR rooms on the cancelation rate using SPC.
Patients and Methods
This study was conducted in a Tertiary Hospital, which is considered as one of the largest medical centers in the country. It has 1346 beds (as March 2014) and provides both emergency and elective healthcare in addition to highly specialized services such as cardiac surgeries and liver transplant. The ORs in the main hospital are serving all specialties including general surgery, urology, ear, nose, and throat, ophthalmology, plastic surgery, gynecology, orthopedic, and neurosurgery. A new surgical building was established and was fully operational by June 2011. The building has inpatient surgical wards, surgical ICU, and four operating theaters.
The numbers of scheduled and canceled surgeries were obtained from the OR registries from January 2009 to December 2012, inclusive to construct SPC charts for rates of cancelation. We defined the canceled cases as the booked case (already documented on the OR list), which is canceled on the same day of surgery. A detailed review of a total of 1813 cases canceled on the day of surgery from January 2012 to December 31, 2012 was conducted to examine the various reasons of cancelation and surgical specialty of canceled cases. All patient records/information were anonymized and de-identified prior to analysis.
Causes of cancelation were divided into three categories
Patient related factors which included patient “no show,” patient's refusal to sign consent form and death prior to the date of the operation.
Preoperative preparation causes such as the need for further optimization, further investigation, abnormal tests, or change in the treatment plan.
Facility related factors including lack of OR time, no elective or ICU beds, unavailability of equipment, implants, or staff administrative errors such as incorrect booking, surgery done as an emergency, or conducted elsewhere.
SPC charts are a dynamic line graph that plots data over time. Time is represented on the horizontal (X) axis and the rates of cancelation are plotted on the vertical (Y) axis. A centerline (CL) represents the average rate of cancelation. Control charts also display lines for an upper control limit (UCL) and a lower control limit (LCL), which are calculated from the intrinsic variation of the data and represents the limits of random variability. Variations on graphs reflect common variations or may indicate significant special cause variation, which can be on the favorable direction (low cancelation rate) or on the unfavorable direction (high cancelation rate). Special cause variations need to be studied carefully either to encourage or discourage these causes according to its effect on the studied process.[19,21,22,23]
In the current study, from January 2009 to May 2011 inclusive was considered as the preinterventional phase, and the period from July 2011 to December 2012 was considered as the postinterventional phase. We excluded, June 2011, from this analysis as it was the 1st month of opening and operation of the new operating theaters. We employed the t-test, to compare Freeman-Tukey transformed values of cancelation rates[24] before and after intervention, as well as the original values to detect, if there was any improvement of cancelation rates after establishment of the new surgical building.
The statistical analysis was conducted using SPSS version 16 (SPSS Inc., Chicago, IL, USA). SPSS can directly generate a wide range of SPC. Online tutorial for constructing SPC can help clinicians to build their own graphs.[25]
Results
Over the study period, from January 2009 to December 2012, 54, 419 surgeries were scheduled, of which 6048 cases were canceled displaying a cancelation rate of 11.11%. The highest reported cancelation rate was observed in August 2010 (14.7%) and the lowest in September 2011 (5.1%).
Figure 1 is plotting monthly cancelation rate during the preintervention phase. The rate of cancelation of surgery seemed to be “controlled” with obvious month to month variations. The UCL was 15.0%, the LCL did not exceed 7.18%; and the average cancelation rate was 10.0%.
Figure 1.
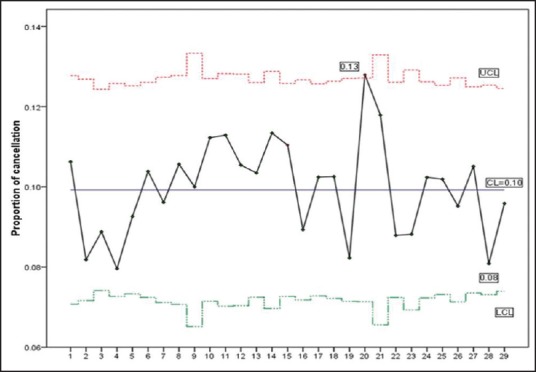
Control Chart: Preinterventional phase (January 2009 to May 2011)
Figure 2 shows the cancelation rates, from July 2011 to December 2012. The cancelation rates appeared more controlled with four points violating control rules on the favorable direction (lower cancelation rate). September 2011 pointed below the level of three sigmas. Moreover, May to July 2012, signified 6 consecutive points trending down. The UCL declined to 12.0%, LCL dropped to 5.5%, and the average cancelation rate was 9.0%.
Figure 2.
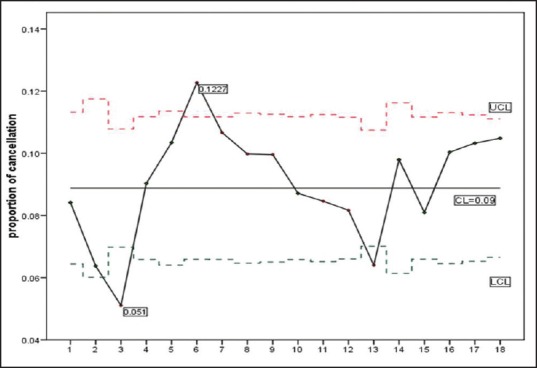
Control Chart: Postinterventional phase (July 2011 to December 2012)
Comparing Freeman-Tukey transformation values before and after the new surgical building through Student's t-test showed significant reduction in the sample means (standard deviations) from 0.32 (0.02) to 0.30 (0.3), P = 0.03. The comparison of the original values of cancelation rates revealed comparable results; reduction of rates from 11.1 (1.5) to 9.9 (2.1) was significant with P = 0.04.
We studied a total of 1813 cancelations over the year 2012, to define various reasons and specialties of canceled surgeries. Table 1 shows different reasons behind cancelations classified into three categories: Patient, preoperative preparation, and facility related. Patients “no show” was the leading cause of cancelation (27%). One-fourth of cancelations (24.3%) were due to the need for further optimization, and the third most prominent cause of cancelation was a lack of OR time (350 cases canceled, 19.5%). Unavailability of staff/equipment/implants accounted for only 0.7% of cancelations.
Table 1.
Reasons behind cancelation of surgeries, January to December 2012
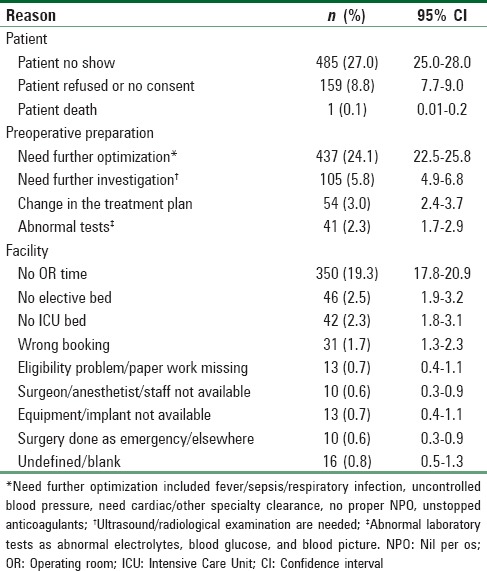
Figure 3 shows Pareto charting of the different causes of cancelations. Pareto chart defined “no show,” “need further optimization,” “no OR time” together with patient refusal as main four causes accounting for approximately 80% of all cancelations of surgeries.
Figure 3.
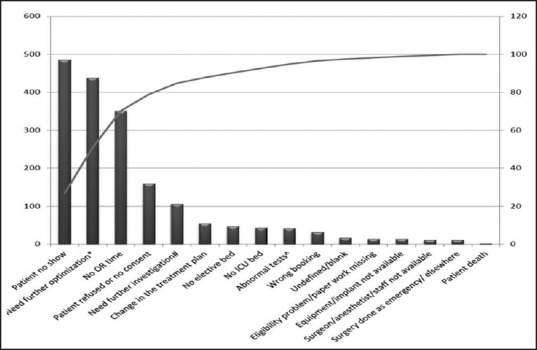
Pareto chart of causes of cancelations, January to December 2012
Figure 4 displays the main reasons of cancelation, according to different specialties. “No show” was consistently the most common cause of cancelation among all surgical specialties, ranging from 21% for plastic and neurosurgery to 32% in ophthalmic surgeries. Figure 5 shows the main causes of cancelation for each month of the studied period. The patients “no show” was highest in August, where it explained about 40% of cancelations. The need for further optimization, which included chest infections/fever and sepsis, reached its maximum values in January (30.2%), February (29.5%), and March (33.0%).
Figure 4.
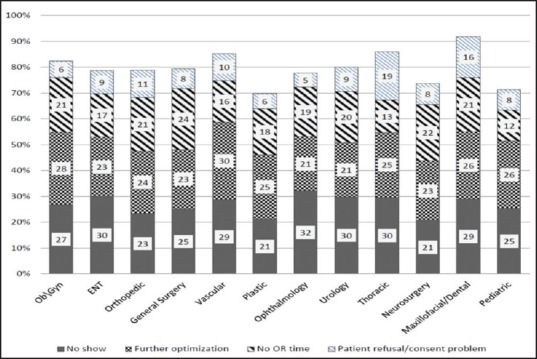
Distribution of main causes of cancelations among surgical specialties
Figure 5.
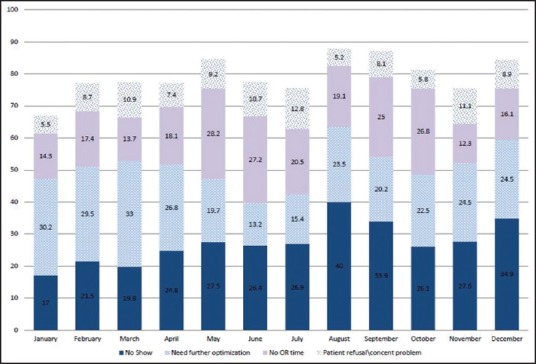
Monthly distribution of main causes of cancelations, January to December 2012
Discussion
The average rate of cancelation of surgery in the current study was approximately 11% before establishing new operating theaters. This rate is comparable with many other institutes, which reported cancelation rates ranging between 11% and 16%;[2,6,26,27] and is even lower than some institutions who reported rates around 20%.[28,29] Nevertheless, this rate is considerably higher than what has been recorded by many other studies (5-8%)[30,31,32,33] leaving significant room for improvement.
In reporting reasons of cancelation, a patient “no show” was reported as the most common reason among different specialties and all through the studied period. Monthly reported reasons emphasized the “no show” as a reason for cancelation, especially during vacation seasons. This finding is in accordance with other studies whereby failure of patients to attend falls in the preeminent causes of cancelation.[12,34] However, the percentage of “no show” in our study is imminently higher than that observed in other studies, which have reported “no show” as low as 5-7%[31,33] or even no cases of “no show” at all.[1] Reasons behind “no show” were not assessed in the current study, but they were investigated by other authors, and recommendations were made to decrease the “no show” by calling or mailing patients prior to their appointments in attempt to remind them.[35] Moreover, we reported that about 9% of cancelation was due to patient refusal or consent problems that might reflect the need for additional consultation and comprehensible discussion between the patient and his physician. This will clarify all the possible worries of patients and provide better involvement of patients in the decision-making and thus better compliance with the scheduled surgery.[36]
A high proportion of surgeries was canceled (24%) due to the need of further optimization, which included respiratory infections and febrile illnesses. However, a noticeable drop in cancelation rates was observed over the months of May, June, and July of 2012. It was concluded that relatively fewer cases of respiratory infections were reported during this period, which is expected over the summer season in comparison to the winter season.[34]
The third most common cause for cancelation of surgery in the current study was the lack of OR time (19%). This cause is commonly reported in studies of cancelation of surgery though with variable percentages.[6,37] In the current study, we were fortunate enough to investigate the cancelation rates due to the opening of new operating theaters. In June 2011, provision of a new surgical building had an immediate effect in reducing the cancelation rate over the months of August and September 2011. This improvement in the cancelation rate was confirmed by a statistical significant difference in rates before and after operation of the new ORs and was affirmed by the SPC charts. It is understandable; however, that this expansion of infrastructure is not feasible for all institutions due to physical, financial, or special reasons.
In the current study, using SPC allowed us to specifically define some uncontrolled time points whereby cancelation rates were of unusual variation. For instance, before the commencement of the new ORs, SPC showed that March 2010 was violating the control rules because it marked 6 consecutive points above the central line. In March 2010, is marking the end of the winter season of 2009, when Saudi Arabia was declared to be affected by the pandemic of influenza A.[38] Unfortunately, the retrospective nature of the current study encumbered confirmation of this coincidence with higher cancelation rate as a cause-result relationship.
Moreover, from the SPC view, the improvement of cancelation rate after launching new ORs did not last for long, and the cancelation rate had risen above central line within few months. The process of cancelation gave the impression of being more controlled yet more progression can be achieved as the cancelation rate in the current study was attributed more to the “no show” of patients rather than deficiency in the OR time.
Different surgical services experience varying rates of cancelation. In the current study, general surgery along with orthopedic surgery displayed the highest rates of cancelation. This finding is in accordance with other studies.[5,6] Reasons behind cancelation showed nearly, similar distribution among different specialties as “no show” and “need further optimization” explained about 50% of cancelations. However, numerous studies have investigated cancelation of surgery in predefined surgical specialties and defined almost the same reasons for cancelation, but with various grades.[7,31,34,39]
Finally, we believe a limitation to our study is the retrospective nature of the investigation. We recommend that any future investigation on the cancelation of surgery should be conducted in prospective manner to validate categorization and definition of causes of cancelation in more depth.
Conclusion
In summary, it was confirmed that there is a unique profile of cancelation of surgery problem for every institute. The lower rate does not imply that we do not need any further investigation and the extension of infrastructure may not be the only solution. SPC use helped to enhance the general picture and initiated critical thinking to solve the problem. Using SPC is functional in monitoring and evaluating changes in the cancelation of surgery.
Financial support and sponsorship
This study was funded by King Abdullah International Medical Research Center, Riyadh, Saudi Arabia. Grant No RC/12/110/R.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We acknowledge the valuable help provided by Dr. Iram Ahmed in proof reading and editing the final manuscript.
References
- 1.Trentman T, Mueller J, Fassett S, Dormer C, Weinmeister K. Day of surgery cancellations in a tertiary care hospital: A one year review. J Anesth Clin Res. 2010;1:2. [Google Scholar]
- 2.Schofield WN, Rubin GL, Piza M, Lai YY, Sindhusake D, Fearnside MR, et al. Cancellation of operations on the day of intended surgery at a major Australian referral hospital. Med J Aust. 2005;182:612–5. doi: 10.5694/j.1326-5377.2005.tb06846.x. [DOI] [PubMed] [Google Scholar]
- 3.Jim’Enez A, Artigas C, Elia M, Casamayor C, Gracia J, Mart’Inez M. Cancellations in ambulatory day surgery: An observational study. Ambul Surg. 2006;12:119–23. [Google Scholar]
- 4.Chalya PL, Gilyoma JM, Mabula JB, Simbila S, Ngayomela IH, Chandika AB, et al. Incidence, causes and pattern of cancellation of elective surgical operations in a university teaching hospital in the Lake Zone, Tanzania. Afr Health Sci. 2011;11:438–43. [PMC free article] [PubMed] [Google Scholar]
- 5.Laisi J, Tohmo H, Keränen U. Surgery cancelation on the day of surgery in same-day admission in a Finnish hospital. Scand J Surg. 2013;102:204–8. doi: 10.1177/1457496913492626. [DOI] [PubMed] [Google Scholar]
- 6.Argo JL, Vick CC, Graham LA, Itani KM, Bishop MJ, Hawn MT. Elective surgical case cancellation in the Veterans Health Administration system: Identifying areas for improvement. Am J Surg. 2009;198:600–6. doi: 10.1016/j.amjsurg.2009.07.005. [DOI] [PubMed] [Google Scholar]
- 7.Leslie R, Beiko D, Van Vlymen J, Siemens D. Day of surgery cancellation rates in urology: Identification of modifiable factors. Can Urol Assoc J. 2013;7:167–73. doi: 10.5489/cuaj.12020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kumar R, Gandhi R. Reasons for cancellation of operation on the day of intended surgery in a multidisciplinary 500 bedded hospital. J Anaesthesiol Clin Pharmacol. 2012;28:66–9. doi: 10.4103/0970-9185.92442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Garg R, Bhalotra AR, Bhadoria P, Gupta N, Anand R. Reasons for cancellation of cases on the day of surgery - A prospective study. Indian J Anaesth. 2009;53:35–9. [PMC free article] [PubMed] [Google Scholar]
- 10.Dexter F, Shi P, Epstein RH. Descriptive study of case scheduling and cancellations within 1 week of the day of surgery. Anesth Analg. 2012;115:1188–95. doi: 10.1213/ANE.0b013e31826a5f9e. [DOI] [PubMed] [Google Scholar]
- 11.Epstein RH, Dexter F. Rescheduling of previously cancelled surgical cases does not increase variability in operating room workload when cases are scheduled based on maximizing efficiency of use of operating room time. Anesth Analg. 2013;117:995–1002. doi: 10.1213/ANE.0b013e3182a0d9f6. [DOI] [PubMed] [Google Scholar]
- 12.Hovlid E, Bukve O, Haug K, Aslaksen AB, von Plessen C. A new pathway for elective surgery to reduce cancellation rates. BMC Health Serv Res. 2012;12:154. doi: 10.1186/1472-6963-12-154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Strum DP, Vargas LG, May JH. Surgical subspecialty block utilization and capacity planning: A minimal cost analysis model. Anesthesiology. 1999;90:1176–85. doi: 10.1097/00000542-199904000-00034. [DOI] [PubMed] [Google Scholar]
- 14.Dix P, Howell S. Survey of cancellation rate of hypertensive patients undergoing Anesthesia and elective surgery. Br J Anaesth. 2001;86:789–93. doi: 10.1093/bja/86.6.789. [DOI] [PubMed] [Google Scholar]
- 15.London: NHS; 2002. National Health Service. Results from the theatre programme cancelled operations diagnostic tool. [Google Scholar]
- 16.Ehrenfeld J, Dexter F, Rothman B, Johnson A, Epstein R. Case cancellation rates measured by surgical service differ whether based on the number of cases or the number of minutes cancelled. Anesth Analg. 2013;117:711–6. doi: 10.1213/ANE.0b013e31829cc77a. [DOI] [PubMed] [Google Scholar]
- 17.Dexter F, Maxbauer T, Stout C, Archbold L, Epstein RH. Relative influence on total cancelled operating room time from patients who are inpatients or outpatients preoperatively. Anesth Analg. 2014;118:1072–80. doi: 10.1213/ANE.0000000000000118. [DOI] [PubMed] [Google Scholar]
- 18.Dexter F, Marcon E, Epstein RH, Ledolter J. Validation of statistical methods to compare cancellation rates on the day of surgery. Anesth Analg. 2005;101:465–73. doi: 10.1213/01.ANE.0000154536.34258.A8. [DOI] [PubMed] [Google Scholar]
- 19.Mestre G, Berbel C, Tortajada P, Alarcia M, Coca R, Gallemi G, et al. “The 3/3 strategy”: A successful multifaceted hospital wide hand hygiene intervention based on WHO and continuous quality improvement methodology. PLoS One. 2012;7:e47200. doi: 10.1371/journal.pone.0047200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Al-Hussein FA. Guideline implementation in clinical practice: Use of statistical process control charts as visual feedback devices. J Family Community Med. 2009;16:11–7. [PMC free article] [PubMed] [Google Scholar]
- 21.Sellick JA., Jr The use of statistical process control charts in hospital epidemiology. Infect Control Hosp Epidemiol. 1993;14:649–56. doi: 10.1086/646659. [DOI] [PubMed] [Google Scholar]
- 22.Benneyan JC. Statistical quality control methods in infection control and hospital epidemiology, part I: Introduction and basic theory. Infect Control Hosp Epidemiol. 1998;19:194–214. doi: 10.1086/647795. [DOI] [PubMed] [Google Scholar]
- 23.Mohammed MA. Using statistical process control to improve the quality of health care. Qual Saf Health Care. 2004;13:243–5. doi: 10.1136/qshc.2004.011650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Miller JJ. The inverse of the Freeman-Tukey double arcsine transformation. Am Stat. 1978;32:138. [Google Scholar]
- 25. [Last accessed 2014 June 20]. Available from: http://www.pic.dhe.ibm.com/infocenter/spssstat/v20r0m0/index.jsp?topic=%2Fcom.ibm.spss.statistics.cs%2Fspchart_table.htm .
- 26.Sanjay P, Dodds A, Miller E, Arumugam PJ, Woodward A. Cancelled elective operations: An observational study from a district general hospital. J Health Organ Manag. 2007;21:54–8. doi: 10.1108/14777260710732268. [DOI] [PubMed] [Google Scholar]
- 27.Seim AR, Fagerhaug T, Ryen SM, Curran P, Saether OD, Myhre HO, et al. Causes of cancellations on the day of surgery at two major university hospitals. Surg Innov. 2009;16:173–80. doi: 10.1177/1553350609335035. [DOI] [PubMed] [Google Scholar]
- 28.Lacqua MJ, Evans JT. Cancelled elective surgery: An evaluation. Am Surg. 1994;60:809–11. [PubMed] [Google Scholar]
- 29.Jonnalagadda R, Walrond ER, Hariharan S, Walrond M, Prasad C. Evaluation of the reasons for cancellations and delays of surgical procedures in a developing country. Int J Clin Pract. 2005;59:716–20. doi: 10.1111/j.1742-1241.2004.00354.x. [DOI] [PubMed] [Google Scholar]
- 30.Haana V, Sethuraman K, Stephens L, Rosen H, Meara JG. Case cancellations on the day of surgery: An investigation in an Australian paediatric hospital. ANZ J Surg. 2009;79:636–40. doi: 10.1111/j.1445-2197.2009.05019.x. [DOI] [PubMed] [Google Scholar]
- 31.Bathla S, Mohta A, Gupta A, Kamal G. Cancellation of elective cases in pediatric surgery: An audit. J Indian Assoc Pediatr Surg. 2010;15:90–2. doi: 10.4103/0971-9261.71748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.González-Arévalo A, Gómez-Arnau JI, delaCruz FJ, Marzal JM, Ramírez S, Corral EM, et al. Causes for cancellation of elective surgical procedures in a Spanish general hospital. Anesthesia. 2009;64:487–93. doi: 10.1111/j.1365-2044.2008.05852.x. [DOI] [PubMed] [Google Scholar]
- 33.Dimitriadis PA, Iyer S, Evgeniou E. The challenge of cancellations on the day of surgery. Int J Surg. 2013;11:1126–30. doi: 10.1016/j.ijsu.2013.09.002. [DOI] [PubMed] [Google Scholar]
- 34.Singh G, Agha R, Roberts D. Cancellations in day-case ENT surgery. Ambul Surg. 2005;12:57–60. [Google Scholar]
- 35.Grover S, Gagnon G, Flegel KM, Hoey JR. Improving appointment-keeping by patients new to a hospital medical clinic with telephone or mailed reminders. Can Med Assoc J. 1983;129:1101–3. [PMC free article] [PubMed] [Google Scholar]
- 36.Parhiscar A, Rosenfeld RM. Can patient satisfaction with decisions predict compliance with surgery? Otolaryngol Head Neck Surg. 2002;126:365–70. doi: 10.1067/mhn.2002.123445. [DOI] [PubMed] [Google Scholar]
- 37.Chiu CH, Lee A, Chui PT. Cancellation of elective operations on the day of intended surgery in a Hong Kong hospital: Point prevalence and reasons. Hong Kong Med J. 2012;18:5–10. [PubMed] [Google Scholar]
- 38.BinSaeed AA. Characteristics of pandemic influenza A (H1N1) infection in patients presenting to a university hospital in Riyadh, Saudi Arabia. Ann Saudi Med. 2010;30:59–62. doi: 10.4103/0256-4947.59377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Schuster M, Neumann C, Neumann K, Braun J, Geldner G, Martin J, et al. The effect of hospital size and surgical service on case cancellation in elective surgery: Results from a prospective multicenter study. Anesth Analg. 2011;113:578–85. doi: 10.1213/ANE.0b013e318222be4d. [DOI] [PubMed] [Google Scholar]