

Abstract
Snapping hip syndrome is a relatively common problem that can be easily managed with conservative treatment. This syndrome can be divided into external, internal and intra-articular types. Internal snapping hip syndrome is the rarest amongst these and its etiology is not well understood. We report a unique case of osteochondroma arising from the anterior inferior iliac spine (AIIS), which caused the internal snapping hip syndrome with hip pain and restriction of activity. This rare case of snapping hip syndrome from the AIIS was treated surgically and the symptoms completely disappeared after excision of the tumor.
Keywords: Osteochondromas, Ilium, Hip Joint/physiopathology, Tendons/physiopathology
Osteochondromas are the most common of benign bone tumors that are characterized by a cartilage-capped bony mass that arises mostly from the metaphysis or diaphysis of a long bone. They account for approximately 40% of all benign bone tumors. The distal metaphysis of the femur and the proximal metaphysis of the tibia and humerus are the most commonly affected bones. Osteochondroma is rarely found in the pelvic bone and reports of solitary pelvic osteochondroma are also rare.1,2) Usually, these conditions are asymptomatic but may require conservative treatment if they become symptomatic. In certain cases, excision of the tumors may be performed if clinical findings include mechanical signs of increased volume, intractable pain, cosmetic problem, symptoms from compression of neurovascular structures, and/or possible malignant degeneration.3,4,5)
Snapping hip syndrome is characterized by a snapping sound or clicking and accompanying hip pain.3,4,6,7,8,9) It can be attributed to both the iliotibial band and the iliopsoas tendon,3,4,6,7,8) which are easily distinguishable distinct entities. The iliotibial band is involved in external snapping hip, and the iliopsoas tendon is related to the internal type. Both types can usually be managed conservatively but occasionally require surgical treatment.
Currently, there are very few reports on snapping hip related to osteochondromas.4,6) Two reports described osteochondroma of the proximal femur associated with snapping hip syndrome.4,6) We reported an extremely rare case of osteochondroma that arose from anterior inferior iliac spine (AIIS) causing internal snapping hip.
CASE REPORT
A 32-year-old woman presented to Kyung Hee University Hospital at Gangdong with a history of chronic right groin pain along with limited hip joint mobility. There was no history of trauma. Her symptoms were aggravated at the time of the hospital visit. The patient indicated that shortly after squatting, she had difficulty extending her hip and had subsequent difficulty walking. Thereafter, she occasionally noticed a snapping phenomenon in her right hip.
A mass with hard consistency was palpable in the right groin area, but there was no tenderness. The motion of the right hip was fully preserved. There was obviously a snapping phenomenon with mild pain when her right hip was forced into a squatting position.
Pelvic plain films were taken initially (Fig. 1). It was difficult to determine a bony abnormality in the anteroposterior view of the pelvis; however, the internal oblique view demonstrated an irregularly calcified, pedunculated lesion that arose from the right ilium. This lesion presented as a peripheral outgrowth with its cortex in continuity with the ilium (Fig. 1); however, neither a periosteal reaction nor bony destruction was seen. Three-dimensional computed tomography (Fig. 2) and magnetic resonance imaging (Fig. 3) showed an approximately 3.3 cm × 2.8 cm × 2.0 cm sized round mass surrounding a cartilaginous cap with < 5 mm in thickness. Due to persistent pain, restriction of daily activity and the potential for malignant degeneration, the patient elected to undergo surgical excision of the tumor. During the operation, the patient was placed in supine position, and a curved incision was made while palpating the mass around the AIIS. The pedunculated mass was exposed after splitting the muscles. An osteotomy was performed to transect the base of the mass from the AIIS after the femoral nerve was identified and exposed.
Fig. 1. The anteroposterior view of pelvis (A) shows abnormal bony contour around the right acetabular roof and the internal oblique view (B) demonstrates an irregularly calcified, pedunculated lesion arising from the right ilium. It presents as a peripheral outgrowth with its cortex in continuity with the ilium (arrow).

Fig. 2. Three-dimensional computed tomography scans show a pedunculated exostotic mass about 3.3 cm × 2.8 cm × 2.0 cm in size.
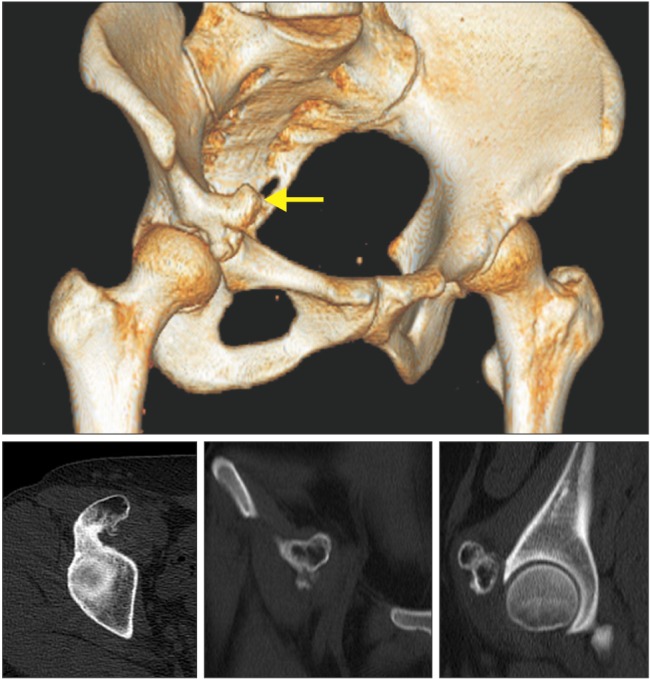
Fig. 3. Low signal on T1- and T2-weighted images and T2 fat suppression sagittal images show the thin cartilaginous cap over exostosis as band of high signal intensity (arrowheads). The displaced and compressed iliopsoas musculotendinous junction is seen on the T1-weighted image (arrow).

The excised mass had a gross appearance typical of osteochondroma (Fig. 4). Histological findings demonstrated cartilaginous cap at the margin of the exostosis, a reflected layer of the periosteum over the exostosis and irregularity of the chondrocytes within the cartilaginous cap. Endochondral ossification was apparent at the base of the cap (Fig. 4). Finally, the patient has not experienced the snapping phenomenon since the surgery.
Fig. 4. (A) Gross appearance of the specimen after removal is typical with an osteochondroma. (B) Photomicrograph of the cartilage cap at the margin of the exostosis demonstrates the reflected layer of the periosteum over the exostosis and irregularity of the chondrocytes within the cartilage cap. Endochondral ossification is apparent at the base of the cap (H&E, × 40).

DISCUSSION
Osteochondroma usually occurs in long bones but may occasionally be seen in flat bones such as the scapula or the pelvic bone.1,2,10) Although osteochondroma is potentially difficult to diagnose owing to its asymptomatic nature, it can be recognized as a palpable mass that may cause pain due to overlying bursal inflammation, a fracture through a pedunculated stalk, or impingement of an overlying neurovascular structure.3,4,5) The diagnosis could have been missed in this case due to the rare presence of osteochondroma in the pelvic bone.1,2)
Snapping hip syndrome also referred to as coxa saltans is a syndrome with an audible snapping that is associated with hip pain.3,4,6,7,8,9) The snapping is usually evoked by flexion and extension of the hip. This syndrome can have several causes and is generally classified into 3 types: external, internal, and intra-articular. The external type is the most common and is related to the iliotibial band sliding over the greater trochanter.3,4,6,7,8,9) The internal type is thought to be caused by the iliopsoas tendon slipping over the iliopectineal eminence, the iliopsoas bursa, the anterior capsule of the hip or the femoral head.3,7,8) But the etiology of the internal type is somewhat poorly understood in comparison to the external type.3,4,9) The intra-articular type is caused by an intra-articular pathology such as a loose body, labral tear or femoroacetabular impingement.3) In the present case, the snapping phenomenon of iliopsoas tendon occurred when it was caught by the osteochondroma from AIIS; hence, it was classified as an internal type.
This case was unique because of the unique location of the osteochondroma on the AIIS, which was accompanied by the snapping phenomenon. However, the association between an osteochondroma and snapping hip has been described only in 2 previous reports.4,6) The first described two cases of osteochondroma on the lesser trochanter that were classified as internal snapping hip.6) The second reported one case of osteochondroma on the posterior side of the proximal femur that caused the snapping of the iliotibial band and was an external type of snapping hip.4) To the best of our knowledge, an osteochondroma arising from the AIIS resulting in the snapping of the iliopsoas tendon has not been reported previously.
ACKNOWLEDGEMENTS
The authors would like to thank Young Ha You (Plymouth University, Peninsula College of Medicine & Dentistry, Plymouth, UK) for his assistance and English editing.
Footnotes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Ghormley RK, Meyerding HW, Mussey RD, Jr, Luckey CA. Osteochondromata of the pelvic bones. J Bone Joint Surg Am. 1946;28(1):40–48. [PubMed] [Google Scholar]
- 2.Kim WJ, Kim KJ, Lee SK, Choy WS. Solitary pelvic osteochondroma causing L5 nerve root compression. Orthopedics. 2009;32(12):922. doi: 10.3928/01477447-20091020-25. [DOI] [PubMed] [Google Scholar]
- 3.Allen WC, Cope R. Coxa saltans: the snapping hip revisited. J Am Acad Orthop Surg. 1995;3(5):303–308. doi: 10.5435/00124635-199509000-00006. [DOI] [PubMed] [Google Scholar]
- 4.Inoue S, Noguchi Y, Mae T, Rikimaru S, Hotokezaka S. An external snapping hip caused by osteochondroma of the proximal femur. Mod Rheumatol. 2005;15(6):432–434. doi: 10.1007/s10165-005-0433-7. [DOI] [PubMed] [Google Scholar]
- 5.Staals EL, Bacchini P, Mercuri M, Bertoni F. Dedifferentiated chondrosarcomas arising in preexisting osteochondromas. J Bone Joint Surg Am. 2007;89(5):987–993. doi: 10.2106/JBJS.F.00288. [DOI] [PubMed] [Google Scholar]
- 6.Schaberg JE, Harper MC, Allen WC. The snapping hip syndrome. Am J Sports Med. 1984;12(5):361–365. doi: 10.1177/036354658401200504. [DOI] [PubMed] [Google Scholar]
- 7.Lyons JC, Peterson LF. The snapping iliopsoas tendon. Mayo Clin Proc. 1984;59(5):327–329. doi: 10.1016/s0025-6196(12)61428-1. [DOI] [PubMed] [Google Scholar]
- 8.Jacobson T, Allen WC. Surgical correction of the snapping iliopsoas tendon. Am J Sports Med. 1990;18(5):470–474. doi: 10.1177/036354659001800504. [DOI] [PubMed] [Google Scholar]
- 9.Gruen GS, Scioscia TN, Lowenstein JE. The surgical treatment of internal snapping hip. Am J Sports Med. 2002;30(4):607–613. doi: 10.1177/03635465020300042201. [DOI] [PubMed] [Google Scholar]
- 10.Cooley LH, Torg JS. "Pseudowinging" of the scapula secondary to subscapular osteochondroma. Clin Orthop Relat Res. 1982;(162):119–124. [PubMed] [Google Scholar]