

Abstract
Background
Computerized tomography (CT) is the gold standard technique for tibial torsion assessment. This study compared two methods of tibial torsion assessment and proposed a new method, which could be of value in cases of abnormal fibular changes.
Methods
The CT-scanograms of 60 participants were assessed by using two different techniques, differed in determination of the distal tibial axis.
Results
The interobserver reliability was 0.861 and 0.863 in the first and second methods, respectively. The intraobserver reliability in both measurement methods was 0.868.
Conclusions
We proposed a reliable method, independent of the fibular midpoint, in assessment of tibial torsion by CT.
Keywords: Tibia, Torsion, Computerized tomography
1. Introduction
Tibial torsion is defined as the twist of proximal versus distal articular axes of tibia around its longitudinal axis.1, 2 Deformities related to tibial torsion are usually presented with minimal clinical symptoms. Most common complaints of patients suffering from abnormal tibial torsion are cosmetic issues. However, in case of severe abnormal tibial torsion resulting in functional disorders, surgical intervention could be taken into consideration. Moreover, tibial torsion could contribute to abnormal posture of lower extremity.3, 4, 5, 6
Numerous attempts since early 20th century have been made to establish a precise assessment method for tibial torsion including clinical,7 anthropometric, and cadaveric skeletal measurement8, 9 and imaging techniques including computerized tomography (CT),10, 11, 12, 13, 14 fluoroscopy,1 magnetic resonance imaging (MRI),15 and ultrasonography.16
The method commonly used for assessment of tibial torsion is to measure the angle formed by proximal and distal articular axes of tibia in the transverse computerized tomograms which is considered as an accurate and reliable method and “golden standard” for tibial torsion assessment.10, 17, 18, 19, 20, 21 Assessment of tibial torsion using CT scan was performed for the first time in 1980 by Jakob et al.17 In 1981, Jend et al. proposed a similar method using CT scan for tibial torsion assessment.10
The current method (traditional method) of tibial torsion assessment requires both fibular and tibial axial CT-scanograms. But it must be taken into consideration that in a group of patients with abnormal or displaced distal fibula, validity of measurement using middle point of fibula, in the transverse cut of CT-scanograms for drawing distal axis of tibia is uncertain. The following conditions might result in an inaccurate measurement of tibial torsion by the traditional method: fracture of distal fibula, deformity of distal fibula, tumors, disruption of normal alignment of fibula and tibia like rupture of syndesmosis.
In this study, we compared two methods of tibial torsion assessment, and proposed a new method, which excludes the role of fibula and could be of value in cases of abnormal fibular changes.
2. Methods
2.1. Human subjects and entry criteria
This study has been approved by the appropriate ethics committee and has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants gave their informed consent prior to their inclusion in the study. In this study, 60 participants, 30 males and 30 females, with an average age of 32.7 ± 8.3 years were included. All participants needed to be assessed for tibial torsion regarding their orthopedic complaints. Those with history of trauma or previous fracture were excluded. All subjects signed an informed written consent to participate in this study. The ethics committee of Shahid Beheshti University of Medical Sciences approved this study.
2.2. Tibia torsion assessment
This was a diagnostic study, investigating the reliability of two methods to measure tibial torsion values using CT-scanograms. CT scan imaging of all subjects were performed at the same radiologic center. Tibial torsion in both lower extremities of the participants was assessed by low dose lower extremity spiral CT-scan. All patients had supine position during imaging and extremities were immobilized by a band in order to achieve maximal accuracy. For each participant, 2-mm CT-scan cuts from proximal and distal of tibia were obtained. Proximal cuts distal to the knee joint and proximal to the fibula (exactly just before appearance of the head of fibula) were selected and distal cuts were exactly proximal to tibiotalar joint (Fig. 1).
Fig. 1.
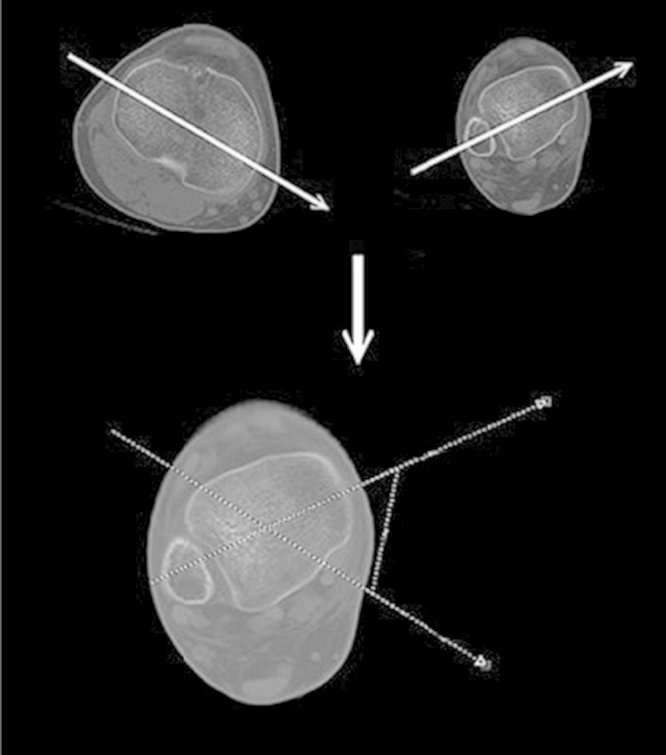
Traditional method for measurement of tibial torsion.
In this study, main distal and proximal axes of tibia were drawn in CT scan cuts and the angle between main axis of distal and proximal tibia was measured as the value of tibial torsion. In order to determine the main axis of proximal tibia in CT scanograms, the tibial plateau line was drawn which crossed tangentially posterior to both proximal condyles (Fig. 2).
Fig. 2.
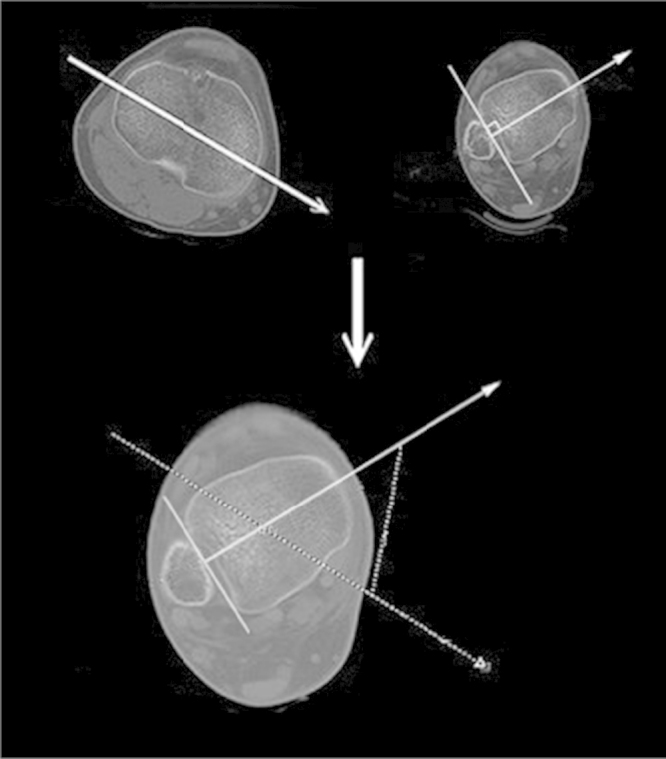
New method for measurement of tibial torsion.
In the traditional method, the middle of tibia and fibula was used as reference points; in the new technique, first introduced by this article, the perpendicular axis to the line connecting the distal fibular notches of the tibia on CT scanograms was drawn and considered to be the distal axis of tibia. In order to assess the reliability of these methods, CT-scanograms of the participants were copied on paper and four trained physicians were asked to draw the distal axis of tibia by the two aforementioned methods. To reduce the measurement error, each physician measured the corresponding angles and finally an orthopedic surgeon re-measured the reported values using a goniometer. No statistics attributed to measures of this person. A month later, these lines were redrawn by the same physicians who had no access to the lines drawn 1 month ago. Then, intraobserver and interobserver agreements were analyzed.
2.3. Statistical analysis
In all cases, the tibial torsion values measured by each physician were compared to the measurements of the other physicians to assess the interobserver agreement. Also, the values of tibial torsion measured by one physician in two separate measurements, a month apart were compared to assess the intraobserver agreement. Analysis of variance and ICC were used to determine the reliability of the measurements using SPSS software. To determine the agreement, interclass correlation coefficients (ICC) with 95% confidence intervals were used. P-values <0.05 were considered statistically significant.
3. Results
Mean values of tibial torsion measured by four trained physicians using the traditional method were 30.4 ± 8.6° (range 9–62.5°) and 30 ± 8.7° (range 9.5–59°) at first and second measurements 1 month apart, respectively (Table 1).
Table 1.
Mean degree ± SD of the tibial torsion measured using two methods by four different observers.
| Observers | Traditional method |
New method |
||
|---|---|---|---|---|
| 1st measurement | 2nd measurement | 1st measurement | 2nd measurement | |
| 1st observer | 30.3 ± 8.4 | 28.8 ± 8.5 | 36.4 ± 8.1 | 36.1 ± 8.9 |
| 2nd observer | 29.8 ± 8.9 | 31.3 ± 8.6 | 35.5 ± 9.0 | 34.4 ± 9.8 |
| 3rd observer | 30.9 ± 8.3 | 31.2 ± 8.8 | 35.1 ± 8.4 | 35.1 ± 8.4 |
| 4th observer | 30.7 ± 30.7 | 28.6 ± 8.6 | 36.5 ± 9.0 | 35.3 ± 9.2 |
| Mean | 30.4 ± 8.6 | 30.0 ± 8.7 | 35.8 ± 8.6 | 35.2 ± 9.1 |
In the measurements using the new method, tibial torsion values at first measurement made by four trained physicians were 35 ± 8.6° (range 16–70°), and for the next month measurements it was 35.2 ± 9.1° (range 6–71.5°) (Table 1).
Analysis of variance between all measurement sessions with the two techniques of measurement did not show any significant difference, so it can be assumed that the measurement of torsion by both techniques has the same outcome and the results can be interchangeably used. Reliability of the measured values in two different measurement sessions using both techniques was assessed by ICC. The ICC was 0.861 in the traditional method. In the new method, ICC was 0.863. In our study, the intraobserver reliability in both measurement techniques was high.
4. Discussion
Previous studies have suggested CT-scan as an accurate imaging modality in assessment of tibial torsion.17 Despite the lack of a certain definition regarding the determination of midpoints of tibia and fibula, our study indicated that the traditional method used to measure tibial torsion values is reliable. We proposed an alternative method independent of the fibular midpoint, which was shown to have high reliability and could be of value in assessment of tibial torsion even in the case of fibular deformity.
Lower extremities form during the fourth to fifth week of intrauterine life.22, 23 Subsequently during the seventh week, internal rotation of the tibia occurs and hallux moves to the midline. Gradually, the lower extremities rotate externally until puberty. Disorders in the growth process, due to the replacement of foot medially, can lead to the development of movement disorders or abnormal gait. However, various other etiologies could be taken into consideration. With respect to the best diagnostic method in assessment of tibial torsion, controversy exists in the literature and various studies have proposed different techniques.3, 6, 7, 11, 24, 25
In our study, the CT-scan images of the participants were assessed by 4 physicians, by two different methods, in two separate occasions. Values of tibial torsion using the traditional method in two separate measurements with 1-month interval were 30.4 ± 8.6° (range 9–62.5°) and 30 ± 8.7° (range 9.5–59°) respectively. Using the new method, the corresponding values were 35.8 ± 8.6° (range 16–70°) and 35.2 ± 9.1° (range 6–71.5°) respectively. The interclass correlation coefficient more than 0.8 shows that in case of using these two different methods by different physicians, the results taken would be similar. ICC measurements by the traditional method in 2 occasions were 0.911 and 0.828; the values for the new method were 0.884 and 0.854. Considering these values, our study indicated the reliability of both methods.
Previously, Jend et al. determined normal tibial torsion values in 69 limbs as 40 ± 9°, and using CT scan, error of repeated measurements in this study was reported as 1.1° and 1.5° at the proximal and distal tibia respectively.10 In another study, Schneider et al. studied tibial torsion in 98 healthy adults with average age of 42 using Jend's method; the mean value was 41.7 ± 8.9°. The difference of repeated measurements in the same study was reported as 3.0 ± 2.7°.26 Also in 2009, Guven et al. reported tibial torsion values in 25 participants, as 10.05 ± 3.06°, using thigh-transmalleolar angle (TMA).7
In the current method of measurement which is the traditional method used in our study, the middle of tibia and fibula was used as reference points to draw the distal axis. However, considering the irregular shape of both of these bones in the axial cut, determination of midpoint for both tibia and fibula by different physicians could lead to unsatisfactory reliability. The uncertainty regarding the wide variation of measurements has been previously addressed.1, 27 In our method, the perpendicular axis to the line connecting the distal fibular notches on CT scanograms was drawn and considered to be the distal axis of tibia. Despite the uncertainties regarding the reliability of the traditional method that was mentioned earlier, we observed a high ICC for both methods, indicating that similar reference fibular and tibial midpoints were determined by the different physicians. In the method presented by this study, an extra line is to be drawn in comparison with the traditional method, which could lead to higher measurement error regarding the complexity added. However, in case of computerized drawing of the perpendicular line, the precision and simplicity of measurement for both methods would not differ significantly. Although in the new method fibula's role is excluded from measurement, the edges of tibia must have been formed by fibula to be measured by the method. Therefore, this method in cases which lack this feature is useless.
The new method has other limitations that deserve comment; validating the new method presented by this study is clearly an area for further research. In addition, CT as an accepted method of imaging has certain limitations of availability, high expense, and simplicity.7
Previous studies have suggested CT-scan as an accurate imaging modality in assessment of tibial torsion. Despite lack of a certain definition regarding the determination of midpoints of tibia and fibula, our study indicated that the traditional method used to measure tibial torsion values is reliable. We proposed an alternative method independent of the fibular midpoint, which was shown to have high reliability and could be of value in assessment of tibial torsion even in the case of fibular deformity and future studies need to be considered to evaluate the possibility of using this method in other imaging techniques such as MRI.
Conflicts of interest
The authors have none to declare.
Acknowledgement
The authors would like to express their sincere appreciation to Mr. Sam Z. Mehrizi, for his valuable effort and admirable assistance in progress of the study. Dr. Hamed Yazdanshenas is a scholar supported by the Clinical Research Education and Career Development (CRECD), Phase II grant # CRECD 5MD007610, NIH-NIMHD. Additionally, Dr. Yazdanshenas was supported by the AXIS NIH-NIMHD grant 2U54MD007598-07.
References
- 1.Clementz B.G. Assessment of tibial torsion and rotational deformity with a new fluoroscopic technique. Clin Orthop Relat Res. 1989:199–209. [Epub 1989/08/01] [PubMed] [Google Scholar]
- 2.Fabry G., Cheng L.X., Molenaers G. Normal and abnormal torsional development in children. Clin Orthop Relat Res. 1994:22–26. [Epub 1994/05/01] [PubMed] [Google Scholar]
- 3.Staheli L.T., Corbett M., Wyss C., King H. Lower-extremity rotational problems in children. Normal values to guide management. J Bone Joint Surg Am. 1985;67:39–47. [Epub 1985/01/01] [PubMed] [Google Scholar]
- 4.Staheli L.T. Rotational problems in children. Instr Course Lect. 1994;43:199–209. [Epub 1994/01/01] [PubMed] [Google Scholar]
- 5.Staheli L.T. In-toeing and out-toeing in children. J Fam Pract. 1983;16:1005–1011. [Epub 1983/05/01] [PubMed] [Google Scholar]
- 6.Kling T.F., Jr., Hensinger R.N. Angular and torsional deformities of the lower limbs in children. Clin Orthop Relat Res. 1983:136–147. [Epub 1983/06/01] [PubMed] [Google Scholar]
- 7.Guven M., Akman B., Unay K., Ozturan E.K., Cakici H., Eren A. A new radiographic measurement method for evaluation of tibial torsion: a pilot study in adults. Clin Orthop Relat Res. 2009;467:1807–1812. doi: 10.1007/s11999-008-0655-z. [Epub 2008/12/05] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hutter C.G., Jr., Scott W. Tibial torsion. J Bone Joint Surg Am. 1949;31A:511–518. [Epub 1949/07/01] [PubMed] [Google Scholar]
- 9.Yoshioka Y., Siu D.W., Scudamore R.A., Cooke T.D. Tibial anatomy and functional axes. J Orthop Res. 1989;7:132–137. doi: 10.1002/jor.1100070118. [Epub 1989/01/01] [DOI] [PubMed] [Google Scholar]
- 10.Jend H.H., Heller M., Dallek M., Schoettle H. Measurement of tibial torsion by computer tomography. Acta Radiol Diagn (Stockh) 1981;22:271–276. doi: 10.1177/028418518102203a10. [Epub 1981/01/01] [DOI] [PubMed] [Google Scholar]
- 11.Staheli L.T., Engel G.M. Tibial torsion: a method of assessment and a survey of normal children. Clin Orthop Relat Res. 1972;86:183–186. [Epub 1972/07/01] [PubMed] [Google Scholar]
- 12.Eckhoff D.G., Johnson K.K. Three-dimensional computed tomography reconstruction of tibial torsion. Clin Orthop Relat Res. 1994:42–46. [Epub 1994/05/01] [PubMed] [Google Scholar]
- 13.Reikeras O., Hoiseth A. Torsion of the leg determined by computed tomography. Acta Orthop Scand. 1989;60:330–333. doi: 10.3109/17453678909149288. [Epub 1989/06/01] [DOI] [PubMed] [Google Scholar]
- 14.Stuberg W., Temme J., Kaplan P., Clarke A., Fuchs R. Measurement of tibial torsion and thigh-foot angle using goniometry and computed tomography. Clin Orthop Relat Res. 1991:208–212. [Epub 1991/11/01] [PubMed] [Google Scholar]
- 15.Schneider B., Laubenberger J., Jemlich S., Groene K., Weber H.M., Langer M. Measurement of femoral antetorsion and tibial torsion by magnetic resonance imaging. Br J Radiol. 1997;70:575–579. doi: 10.1259/bjr.70.834.9227249. [Epub 1997/06/01] [DOI] [PubMed] [Google Scholar]
- 16.Hudson D., Royer T., Richards J. Ultrasound measurements of torsions in the tibia and femur. J Bone Joint Surg Am. 2006;88:138–143. doi: 10.2106/JBJS.D.02924. [Epub 2006/01/05] [DOI] [PubMed] [Google Scholar]
- 17.Jakob R.P., Haertel M., Stussi E. Tibial torsion calculated by computerised tomography and compared to other methods of measurement. J Bone Joint Surg Br. 1980;62B:238–242. doi: 10.1302/0301-620X.62B2.7364840. [Epub 1980/05/01] [DOI] [PubMed] [Google Scholar]
- 18.Madadi F., Yazdanshenas H., Madadi F., Bazargan-Hejazi S. Double acetabular wall – a misleading point for hip arthroplasty: an anatomical, radiological, clinical study. Int Orthop. 2013;37:1007–1011. doi: 10.1007/s00264-013-1780-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Murphy S.B., Simon S.R., Kijewski P.K., Wilkinson R.H., Griscom N.T. Femoral anteversion. J Bone Joint Surg Am. 1987;69:1169–1176. [Epub 1987/10/01] [PubMed] [Google Scholar]
- 20.Pfeifer T., Mahlo R., Franzreb M. Computed tomography in the determination of leg geometry. In Vivo. 1995;9:257–261. [Epub 1995/05/01] [PubMed] [Google Scholar]
- 21.Strecker W., Keppler P., Gebhard F., Kinzl L. Length and torsion of the lower limb. J Bone Joint Surg Br. 1997;79:1019–1023. doi: 10.1302/0301-620x.79b6.7701. [Epub 1997/12/11] [DOI] [PubMed] [Google Scholar]
- 22.Staheli L.T. Torsional deformity. Pediatr Clin North Am. 1977;24:799–811. doi: 10.1016/s0031-3955(16)33499-x. [Epub 1977/11/01] [DOI] [PubMed] [Google Scholar]
- 23.Guidera K.J., Ganey T.M., Keneally C.R., Ogden J.A. The embryology of lower-extremity torsion. Clin Orthop Relat Res. 1994:17–21. [Epub 1994/05/01] [PubMed] [Google Scholar]
- 24.Yazdanshenas H., Madadi F., Madadi F., Washington Iii E.R., Jones K., Shamie A.N. Patellar tendon donor-site healing during six and twelve months after Anterior Cruciate Ligament Reconstruction. J Orthop. 2015 doi: 10.1016/j.jor.2015.05.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chabok S., Yazdanshenas H., Naeeni A. The impact of body mass index on treatment outcomes among traumatic brain injury patients in intensive care units. Eur J Trauma Emerg Surg. 2014;40:51–55. doi: 10.1007/s00068-013-0314-2. [DOI] [PubMed] [Google Scholar]
- 26.Schneider B., Laubenberger J., Wildner M., Exne V., Langer M. [NMR tomographic measurement of femoral ante-torsion and tibial torsion] Rofo. 1995;162:229–231. doi: 10.1055/s-2007-1015870. [Epub 1995/03/01. Kernspintomographisches Messungsverfahren von Femurantetorsion und Tibiatorsion] [DOI] [PubMed] [Google Scholar]
- 27.Laasonen E.M., Jokio P., Lindholm T.S. Tibial torsion measured by computed tomography. Acta Radiol Diagn (Stockh) 1984;25:325–329. doi: 10.1177/028418518402500413. [Epub 1984/01/01] [DOI] [PubMed] [Google Scholar]