

Abstract
Statement of Problem:
Change in color and loss of marginal adaptation of tooth colored restorative materials is not acceptable. Bleaching is commonly used for treating discolored teeth. However, the literature is scanty regarding its effect on color and marginal adaptation of direct and indirect composite laminate veneers (CLVs) under in vivo conditions.
Purpose:
Purpose of the study was to determine the effect of bleaching on color change and marginal adaptation of direct and indirect CLVs over a period of time when exposed to the oral environment.
Materials and Methods:
For this purpose, a total of 14 subjects irrespective of age and sex indicated for CLV restorations on maxillary anterior teeth were selected following the inclusion and exclusion criteria. For each subject, indirect CLVs were fabricated and looted in the first quadrant (Group 1) and direct CLV's (Group 2), were given in the second quadrant. Color change was assessed clinically using intra-oral digital spectrophotometer and marginal adaptation was assessed on epoxy resin replica of the tooth-restoration interface under scanning electron microscope. After 6 months, the subjects underwent a home bleaching regimen for 14 days using 10% carbamide peroxide. The assessment of color change and marginal adaptation was done at 6 months after veneering (0–180 days), immediately after the bleaching regimen (0–194 days) and 3 months after the bleaching regimen (0–284 days).
Results:
The difference in median color change (ΔE) between the groups was tested using Wilcoxon rank sum test while the median color change with time within the groups was tested using Wilcoxon signed rank test. The difference in the rates of marginal adaptation was tested between the groups using Chi-square/Fisher's exact test.
Bleaching led to statistically significant color change at cervical (CE), middle and incisal (IE) regions when direct and indirect composites were compared (P < 0.05). During intra-group comparison, direct CLV's showed significant color change at CE and IE regions when ΔE was compared at 180 days and 284 days (CE 10 vs. CE 30, P = 0.008, IE 10 vs. IE 30, P = 0.003). No significant differences were found when within group comparison was made for indirect laminates. Intergroup comparison between the groups showed significant difference in marginal adaptation at CE margin at all.time points (at baseline, P = 0.005; at 180 days, P = 0.007; 194 days, P = 0.025; at 284 days, P = 0.067).
Conclusion:
After bleaching, indirect CLVs performed better in terms of color stability whereas direct CLVs performed better in terms of marginal adaptation.
Clinical Significance:
Indirect composites should be preferred to direct composites as veneering materials as they have better color stability. Special attention should be given to their marginal adaptation especially in the CE region. Bleaching should be avoided in patients with composite restorations in the mouth.
Key Words: CIELAB color system, color change, composites, discoloration, spectrophotometer, veneers
INTRODUCTION
Discolored anterior teeth can be managed in a number of ways.[1] Mild and superficial discolorations in structurally intact teeth can be managed with bleaching using carbamide peroxide or hydrogen peroxide gel and/or micro abrasion or macro abrasion. Moderate to severe deep discolorations is best managed with laminate veneers. Modern day laminate veneers are made from porcelain or composite resins, where the latter can be fabricated by direct and indirect techniques. Traditional feldspathic porcelain veneers as well as newer pressable ceramics (though provide life like esthetics when compared to composite laminate veneers [CLVs]) are expensive, brittle and difficult to repair.[2,3,4]
Although composite resins have excellent esthetic properties, a major disadvantage is their susceptibility to discoloration after prolonged exposure to the oral environment.[5] Unacceptable color change especially marginal discoloration is a primary reason for their replacement.
Color stability and marginal adaptation are crucial for the success of any veneering material. With the current interest in esthetic dentistry, vital bleaching is a viable option to consider when treating intrinsically stained or discolored teeth whose form and integrity are deemed acceptable.[6] Literature reports are conflicting with regards to the effect of bleaching on tooth colored restorative materials.[7,8,9,10,11,12] Increased, decreased, or no alteration in surface characteristics of composite resins were found due to differences in study methodology, bleaching the agent and it's concentration, time of application and the composite tested.
There are numerous in vitro studies evaluating the color stability and marginal adaptation of direct and indirect composite resins.[3,13,14,15,16,17,18] However, in vivo studies are limited to their use as posterior filling materials and as Class V restoratives.[19,20,21] This study was planned to evaluate the effect of bleaching on color change and marginal adaptation of direct and indirect CLVs on anterior teeth. We hypothesized that there is a significant effect of bleaching on color change and marginal adaptation of direct and indirect CLV's. The null hypothesis tested was that the difference in medians/proportions of color change/marginal adaptation between the groups was zero.
MATERIALS AND METHODS
A total of 14 subjects with indications for laminate veneers on the anterior teeth [Figure 1a] were included in the study after considering the inclusion and exclusion criteria.[1] Subjects with discolorations in anterior teeth that could not be removed by bleaching or microabrasion; with large labial erosions or extensive cervical (CE) restorations and; having healthy periodontium were included in the study while those with high caries activity, gross malocclusion, or indicated for full crowns were excluded. This study was approved by the Ethics Committee of the All India Institute of Medical Sciences (Ref. No: IESC/T-153/2010).
Figure 1.

(a) Pretreatment picture showing discolored teeth (b) Posttreatment picture showing composite laminates
To the best of our knowledge, no similar study using same materials and study design could be found. Hence, a pilot study was conducted to calculate the sample size and check the feasibility of the study. Based on the pilot study, with 80% power and 5% α error, the required sample was calculated to be 35 considering 10% dropouts. 38 veneers were fabricated for each group, and results were calculated accordingly as there was no loss to follow-up. Confidence interval was set at 95%.
For each subject, indirect CLVs were fabricated for discolored anterior teeth and looted in the first quadrant (Group 1) and direct CLV's (Group 2), were given in second quadrant [Figure 1b]. The indirect composite used was SR Adoro (Ivoclar Vivadent, Leichenstein), a micro filled composite with a high content (65 wt%) of inorganic fillers in nanoscale range. The direct composite used was Filtek Z350 (3M ESPE, India), a nanocomposite for universal application with nanofillers (78.5 wt%) with a cluster particle in micron scale range.
Diagnostic impression for custom tray fabrication was made and shade of the individual tooth was selected during the first diagnostic appointment using Vita shade guide (Lumin-Vaccum, Vitapan, Vita Zahnfabrik, Germany) using the uninvolved portion of teeth or adjacent or opposing teeth as references. Window-type preparation for laminate veneers was done at a depth of 0.3–0.5 mm guided by the depth cut marks.[22] Final impression was made in a custom tray, using heavy body and light body addition silicone impression material (Reprosil and Aquasil, Dentsply Caulk, USA), by two-step technique. The working cast was fabricated in type IV Gypsum product (Kalrock, Kalabhai, India). Indirect composite material was applied incrementally and cured (20 s per increment) using the hand held visible light curing unit (Bee Cool, Germany; wavelength of 430–490 nm; maximum intensity of 7.5 W). Proper contours of the restoration were achieved and the final curing was done under heat and light in a special curing chamber (Lumamat 100, Ivoclar Vivadent, Liechtenstein) for 25 min at 104°C. The indirect CLVs were removed from the working cast, finished and polished for clinical try in. The prepared teeth surfaces in the first quadrant were etched for 15 s using 36% phosphoric acid gel (DeTrey Conditioner 36, Dentsply DeTrey, Germany), followed by rinsing, air drying and application of bonding agent both on the tooth surface and on the indirect CLV's inner surface. Dual cured resin cement (Calibra, Dentsply Caulk, USA) was used for luting the indirect CLVs.
Prepared surface of teeth in the second quadrant were etched with 37% phosphoric acid gel (Scotchbond Etchant Gel, 3M ESPE, India) for 15 s, followed by rinsing, air drying and application of bonding agent (Adper Single bond Plus, 3M ESPE, India). Direct CLV restorations were done by incremental build up, and each increment was light-cured for 20 s. The restorations were finished and polished under adequate coolant spray. The shade of the restoration was recorded using the Intra oral digital spectrophotometer (Vita Easy Shade, Vita Zahnfabrik, Germany), where readings for each tooth at CE, middle (ME) and incisal (IE) regions were recorded and values were converted to numerical values of CIELAB system using a conversion chart for statistical analysis. The shades of all the CLVs were measured at three subsequent follow-ups (6 months after restoration, at the end of bleaching regimen and 3 months later) using the same methodology.
Marginal adaptation of all the laminate veneers in each group was evaluated qualitatively on epoxy resin dies (obtained from post-restorative impressions) at baseline and at each follow-up under scanning electron microscope (SEM).[23] All epoxy resin dies were gold sputtered [Figure 2] to form a uniform layer of thickness of about 30–40 nm over the specimens to make them conductive of electricity and help in scanning by high energy electron beam. All the four margins of the laminates (Cervical, Incisal, Mesial, and Distal) were evaluated at the midpoint of the respective margin under × 200 magnification. Margins were assessed as Score 0: No marginal gap [Figure 3a] and Score 1: Visible gap [Figure 3b].
Figure 2.

Gold sputtered epoxy resin dies
Figure 3.
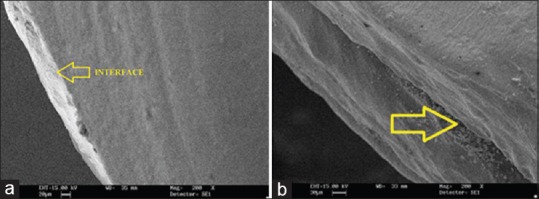
(a) Scanning electron microscope picture of a sample showing no marginal gap (b) Scanning electron microscope picture of a sample showing marginal gap
At the end of 6 months post-restoration, the bleaching tray was fabricated on the working cast using a thermoplastic sheet of 2 mm thickness by pressure molding technique. The area for reservoir of bleaching gel was outlined on the tooth, 0.5–1 mm short from the margins. A heat resistant silicone block out material (Silkit, Sheu Dental, Germany) was applied on the outlined area for about 0.5 mm thickness. The bleaching tray was delivered to the patient and 10% carbamide peroxide gel (Opalescence, Ultradent Products, USA) was dispensed. The patient was instructed about the method of gel delivery onto the bleaching tray. The patients were instructed to use the bleaching agent with the tray for 14 consecutive days for 8 h/day.[24,25] The second follow-up was done after the end of the night guard bleaching regimen. The final follow-up was done at 3 months after the second follow-up.
The data obtained were analyzed using Stata 11.0 (College station, Texas, USA). The data were presented as n (%) or median (minimum–maximum) as appropriate. Since the data were not following the normal distribution, the difference in median color change (ΔE) between the groups was tested using Wilcoxon rank sum test. While the median color change with time within the groups was tested using Wilcoxon signed rank test. The difference in the rates of marginal adaptation was tested between the groups using Chi-square/Fisher's exact test. Statistical significance for all tests was set at P < 0.05.
RESULTS
Color stability
For each sample, three color difference values (ΔE), one each for CE, ME and IE regions were calculated from intra oral dental spectrophotometer values at following intervals:
At 0–180 days: After 6 months of veneering
At 0–194 days: After completion of bleaching regimen of 14 days
At 194–284 days: 3 months after bleaching
At 0–284 days: From baseline to 3 months postbleaching.
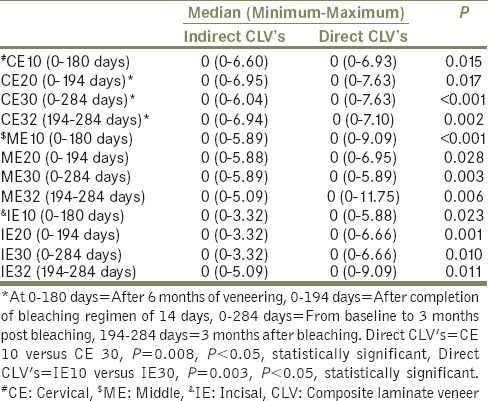
Bleaching led to statistically significant color change at CE, ME and IE regions when direct and indirect composites were compared (P < 0.05) [Table 1], [Graphs 1–3]. During intragroup comparison, direct CLV's showed significant color change at CE and IE regions when ΔE was compared at 180 days and 284 days (CE 10 vs. CE 30, P = 0.008, IE 10 vs. IE 30, P = 0.003). Statistically nonsignificant differences were found when within group comparison was made for indirect laminates (P > 0.05).
Table 1.
Color change (ΔE) between various follow-up combinations measured for Indirect CLV'S at cervical, middle and incisal regions (n=38)
Graph 1.
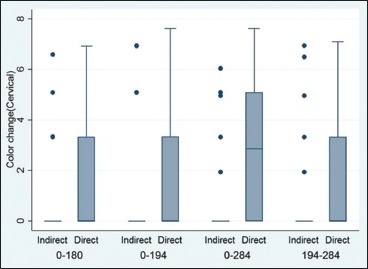
Intergroup comparison of color change at the cervical region
Graph 2.
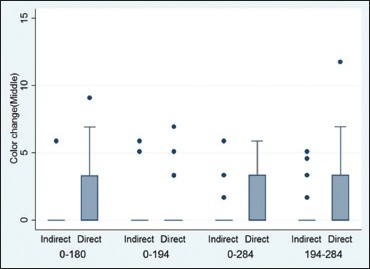
Intergroup comparison of color change at the middle region
Graph 3.
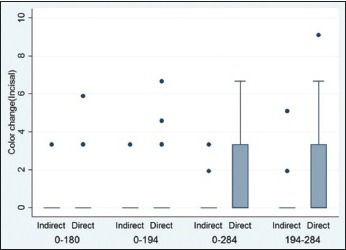
Intergroup comparison of color change at incisal region
Marginal adaptation
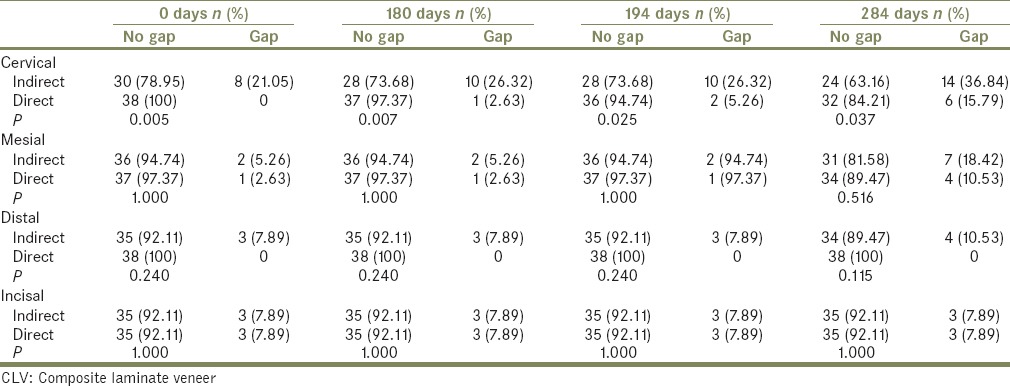
Marginal gap was scored as “0” for no gap and “1” for visible gap under SEM. Intergroup comparison between the groups showed significant difference in marginal adaptation at CE margin at various time points (at baseline, P = 0.005; at 180 days, P = 0.007; 194 days, P = 0.025; at 284 days, P = 0.037). This difference was statistically nonsignificant for mesial, distal and IE margins. Intragroup comparison revealed that no. of samples showing gap at CE margin increased with time in both the groups though the percentage increase was more in indirect CLV's [Table 2].
Table 2.
Intergroup comparison of marginal adaptation at various assessment times between indirect and direct CLV's (n=38)
DISCUSSION
The literature reports significant lightening of the teeth after bleaching. Since at least 40% of patients requiring bleaching have some tooth colored restorative material on their teeth, it is important to know the effects of bleaching on tooth colored restorative materials.[26]
Effect of bleaching was studied on color and marginal adaptation of direct and indirect CLV's. As results of the study showed that that the differences in medians/proportions of color change/marginal adaptation between the groups were not zero, hence the null hypothesis was rejected.
Attin et al. concluded that 10% carbamide peroxide bleaching agent was able to remove extrinsic stains from composite restorative materials.[9] SEM and profilometric studies have shown that 10–16% carbamide peroxide bleaching gels may lead to a slight but statistically significant increase in roughness and the amount of porosities in micro-filled and hybrid composite resins and thus polishing of restorations after bleaching is advised. Monaghan et al. put forward three hypothesis for the bleaching effect of composites: (1) Oxidation of readily accessible surface pigments leading to less intense color species, (2) oxidation of amine compounds which may have been implicated as responsible for color instability over time and (3) the degree of conversion of the resin matrix to polymer may allow some resins to be attacked by the bleaching solutions and not others.[8]
In this in vivo study, the direct CLVs showed greater change in color than indirect CLVs before and after bleaching [Table 1, Graphs 1–3]. This can be attributed to the fact that the direct CLVs have a lower degree of polymerization leading to more intermolecular spaces and thus more water sorption leading to hydrolysis of matrix and penetration of extrinsic stains.[17] Furthermore, the direct composite material evaluated in this study had a greater percentage of fillers (78.9 wt%) when compared to the indirect composite material (65 wt%). According to a study on composite polymer networks by Ferracane, greater the volume of filler particles in the composite formulation, lower will be the degree of conversion resulting in larger number of double bonds and lower quality of bonds formed.[27] Therefore, the resulting composition will be more predisposed to the action of the solvent due to greater free volume for solvent action, leading to plasticization action and a decrease in surface hardness and greater color alteration.
According to Cullen et al., micro filled composites are affected by bleaching more when compared to nanocomposites.[28] This contradicts with the findings of Anagnostou et al. that nano-hybrid composite produces greater color change than hybrid or micro filled composites after bleaching.[29] Studies indicating the effects of bleaching agents on the microhardness of restorative materials have reported conflicting results.[12] The discrepancies between the studies may be explained by differences in experimental methodologies, bleaching agents applied and restorative materials used. Rattacaso et al. has also concluded that the surface microhardness reduction after bleaching gel application is significantly higher for nanocomposite when compared to micro filled composite.[30] Literature review of El-Murr et al.[26] and in vitro study of Pruthi et al.[31] also concluded that significant changes occur in color of nanocomposites after bleaching with 10–15% carbamide peroxide.
Intergroup comparison between the groups showed a significant difference in marginal adaptation at CE margin at various time points. No. of samples with marginal gap were higher for indirect CLV's as compared to direct CLV's. As shown in Table 2, the indirect CLVs demonstrated higher percentage of marginal discrepancy at the baseline (especially at CE margin; 21%) when compared to direct CLVs (0%). This can be attributed to the use of luting agent with comparatively inferior mechanical properties in case of indirect CLVs. This view is also supported by Scheibenbogen-Fuchsbrunner et al.[20] According to them, for indirect composites, loss of marginal integrity at baseline can be caused by polymerization shrinkage or removal of cement flashes with blunt instruments, while for direct composites, this can be explained by the fact that the larger the volume of composite to be polymerized, larger the residual internal stresses in the polymerized composite even if placed incrementally. Celik and Gemaalmaz concluded that indirect CLVs do not have perfect marginal integrity due to polymerization shrinkage and viscosity of the material.[18] This is concordance with the results of the present study. van Dijken and Horstedt concluded that micro filled composites have greater polymerization shrinkage when compared to nano filled and hybrid composites.[32] This is comparable to the results of the current study, where a micro filled indirect composite resin had inferior marginal integrity as compared to a direct nano filled composite resin.
Furthermore, among both the groups, the CE region showed the greatest percentage of samples with loss of marginal integrity. This finding is consistent with that of previous studies.[33,34,35,36] According to these researchers, the marginal leakage at CE margin is greater than at other margins because of the deviation in orientation of enamel prisms and also thin enamel in this part of the tooth. The enamel prisms alter from vertical to oblique toward the CE region. Atsu et al. summarized the findings of Nattress et al. and Ferrari et al. that a preparation depth of 0.5 mm for laminate veneer may expose the dentin cervically and the failure rates are higher when the veneers are bonded to dentin.[37] According to Sadowsky, marginal gap is more in CE region due to frequent dentin exposure in this area, due to thin enamel and the bond strength of composite to dentin is less than that of enamel.[3]
The effects of bleaching on marginal adaptation of composite resins have always been a subject of controversy. Crime reported that bleaching agents did not impair the marginal seal of class V composite restorations placed at cementoenamel junction.[38] Ulukapi et al. showed that bleaching significantly increased the micro-leakage of labial restorations with enamel margins only.[39] Similar results were reported by Turkun and Turkun in case of composite resins used as access cavity fillings.[40] In the present study, bleaching caused a significant increase in the percentage of samples with marginal gap in case of indirect CLVs. Although this change was not observed immediately after bleaching, it was observed 3 months postbleaching. This may be because of the chemical softening of the luting resin by the bleaching agent making it more susceptible to wear. This statement is in concordance with the results obtained by Canay and Cehreli that bleaching agents deteriorates the surface of resins and weakens the covalent bonds making it more susceptible to wear from action of dietary particles and the abrasive action of toothpaste and dentifrices.[24] The limitations of the study were the small sample size and limited follow-ups. Further studies are needed with longer follow-up to confirm the findings. Profilometric analyses to assess the effect of bleaching on surface roughness of different types of restorative materials can be done to draw more meaningful conclusions for clinical applications.
CLINICAL SIGNIFICANCE
Indirect composites should be preferred to direct composites as veneering materials as they have better color stability. Special attention should be given to their marginal adaptation especially in the CE region. Bleaching should be avoided in patients with composite restorations in the mouth.
CONCLUSIONS
Two commonly used composites were evaluated for color stability and marginal adaptation under in vivo conditions. These parameters are crucial for long-term success of any restorative material. Effect of bleaching was also evaluated, which is commonly used to treat discolored natural teeth.
Direct CLVs showed more color change than indirect CLVs in the oral cavity. Bleaching led to statistically significant color change in CE and IE thirds of direct CLVs. Changes in the matrix of the composites due to bleaching might have led to this color change.
Visible marginal gap was greater for indirect CLV's as compared to direct veneers for all the margins, but the difference was statistically significant for CE margins only. Bleaching led to increase in marginal gap in both the groups, but it was significantly greater in the indirect group.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Thosre D, Mulay S. Smile enhancement the conservative way: Tooth whitening procedures. Journal of Conservative Dentistry. 2009;12:164–8. doi: 10.4103/0972-0707.58342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lim CC. Case selection for porcelain veneers. Quintessence Int. 1995;26:311–5. [PubMed] [Google Scholar]
- 3.Sadowsky SJ. An overview of treatment considerations for esthetic restorations: A review of the literature. J Prosthet Dent. 2006;96:433–42. doi: 10.1016/j.prosdent.2006.09.018. [DOI] [PubMed] [Google Scholar]
- 4.Layton DM, Clarke M. A systematic review and meta-analysis of the survival of non-feldspathic porcelain veneers over 5 and 10 years. Int J Prosthodont. 2013;26:111–24. doi: 10.11607/ijp.3202. [DOI] [PubMed] [Google Scholar]
- 5.Ronk SL. Dental lamination: Clinical problems and solutions. J Am Dent Assoc. 1982;104:844–6. doi: 10.14219/jada.archive.1982.0315. [DOI] [PubMed] [Google Scholar]
- 6.Heymann HO. Indirect composite resin veneers: Clinical technique and two-year observations. Quintessence Int. 1987;18:111–8. [PubMed] [Google Scholar]
- 7.Fay RM, Servos T, Powers JM. Color of restorative materials after staining and bleaching. Oper Dent. 1999;24:292–6. [PubMed] [Google Scholar]
- 8.Monaghan P, Lim E, Lautenschlager E. Effects of home bleaching preparations on composite resin color. J Prosthet Dent. 1992;68:575–8. doi: 10.1016/0022-3913(92)90368-k. [DOI] [PubMed] [Google Scholar]
- 9.Attin T, Hannig C, Wiegand A, Attin R. Effect of bleaching on restorative materials and restorations – A systematic review. Dent Mater. 2004;20:852–61. doi: 10.1016/j.dental.2004.04.002. [DOI] [PubMed] [Google Scholar]
- 10.Schemehorn B, González-Cabezas C, Joiner A. A SEM evaluation of a 6% hydrogen peroxide tooth whitening gel on dental materials in vitro . J Dent. 2004;32(Suppl 1):35–9. doi: 10.1016/j.jdent.2003.10.012. [DOI] [PubMed] [Google Scholar]
- 11.Costa SX, Becker AB, Rastelli AN, Loffredo LC, Andrade MF, Bagnato VS. Effect of four bleaching regimens on color changes and microhardness of dental nanoflled composite. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:e59–64. [Google Scholar]
- 12.Mujdeci A, Gokay O. Effect of bleaching agents on the microhardness of tooth-colored restorative materials. J Prosthet Dent. 2006;95:286–9. doi: 10.1016/j.prosdent.2006.01.010. [DOI] [PubMed] [Google Scholar]
- 13.Gross MD, Moser JB. A colorimetric study of coffee and tea staining of four composite resins. J Oral Rehabil. 1977;4:311–22. doi: 10.1111/j.1365-2842.1977.tb00997.x. [DOI] [PubMed] [Google Scholar]
- 14.Powers JM, Fan PL, Raptis CN. Color stability of new composite restorative materials under accelerated aging. J Dent Res. 1980;59:2071–4. doi: 10.1177/00220345800590120801. [DOI] [PubMed] [Google Scholar]
- 15.Douglas RD. Color stability of new-generation indirect resins for prosthodontic application. J Prosthet Dent. 2000;83:166–70. doi: 10.1016/s0022-3913(00)80008-6. [DOI] [PubMed] [Google Scholar]
- 16.Tanoue N, Soeno K, Kawasaki K, Atsuta M. Influence of acidulated phosphate fluoride solution on the color stability of indirect composites. J Prosthet Dent. 2004;92:343–7. doi: 10.1016/j.prosdent.2004.07.008. [DOI] [PubMed] [Google Scholar]
- 17.Bausch JR, de Lange K, Davidson CL, Peters A, de Gee AJ. Clinical significance of polymerization shrinkage of composite resins. J Prosthet Dent. 1982;48:59–67. doi: 10.1016/0022-3913(82)90048-8. [DOI] [PubMed] [Google Scholar]
- 18.Celik C, Gemalmaz D. Comparison of marginal integrity of ceramic and composite veneer restorations luted with two different resin agents: An in vitro study. Int J Prosthodont. 2002;15:59–64. [PubMed] [Google Scholar]
- 19.Wassell RW, Walls AW, McCabe JF. Direct composite inlays versus conventional composite restorations: Three-year clinical results. Br Dent J. 1995;179:343–9. doi: 10.1038/sj.bdj.4808919. [DOI] [PubMed] [Google Scholar]
- 20.Scheibenbogen-Fuchsbrunner A, Manhart J, Kremers L, Kunzelmann KH, Hickel R. Two-year clinical evaluation of direct and indirect composite restorations in posterior teeth. J Prosthet Dent. 1999;82:391–7. doi: 10.1016/s0022-3913(99)70025-9. [DOI] [PubMed] [Google Scholar]
- 21.Wakiaga J, Brunton P, Silikas N, Glenny AM. Direct versus indirect veneer restorations for intrinsic dental stains. Cochrane Database Syst Rev. 2004;1:CD004347. doi: 10.1002/14651858.CD004347.pub2. [DOI] [PubMed] [Google Scholar]
- 22.Heymann HO, Swift EJ, Jr, Ritter AV. Additional conservative esthetic procedures. In: Roberson TM, editor. Sturdvent's Art and Science of Dentistry. 5th ed. St Louis, Missouri: Mosby; 2006. pp. 625–82. [Google Scholar]
- 23.Jha R, Jain V, Das TK, Shah N, Pruthi G. Comparison of marginal fidelity and surface roughness of porcelain veneers fabricated by refractory die and pressing techniques. J Prosthodont. 2013;22:439–44. doi: 10.1111/jopr.12032. [DOI] [PubMed] [Google Scholar]
- 24.Canay S, Cehreli MC. The effect of current bleaching agents on the color of light-polymerized composites in vitro . J Prosthet Dent. 2003;89:474–8. doi: 10.1016/S0022391303001689. [DOI] [PubMed] [Google Scholar]
- 25.Villalta P, Lu H, Okte Z, Garcia-Godoy F, Powers JM. Effects of staining and bleaching on color change of dental composite resins. J Prosthet Dent. 2006;95:137–42. doi: 10.1016/j.prosdent.2005.11.019. [DOI] [PubMed] [Google Scholar]
- 26.El-Murr J, Ruel D, St-Georges AJ. Effects of external bleaching on restorative materials: A review. J Can Dent Assoc. 2011;77:b59. [PubMed] [Google Scholar]
- 27.Ferracane JL. Hygroscopic and hydrolytic effects in dental polymer networks. Dent Mater. 2006;22:211–22. doi: 10.1016/j.dental.2005.05.005. [DOI] [PubMed] [Google Scholar]
- 28.Cullen DR, Nelson JA, Sandrik JL. Peroxide bleaches: Effect on tensile strength of composite resins. J Prosthet Dent. 1993;69:247–9. doi: 10.1016/0022-3913(93)90100-3. [DOI] [PubMed] [Google Scholar]
- 29.Anagnostou M, Chelioti G, Chioti S, Kakaboura A. Effect of tooth-bleaching methods on gloss and color of resin composites. J Dent. 2010;38(Suppl 2):e129–36. doi: 10.1016/j.jdent.2010.06.006. [DOI] [PubMed] [Google Scholar]
- 30.Rattacaso RM, da Fonseca Roberti Garcia L, Aguilar FG, Consani S, de Carvalho Panzeri Pires-de-Souza F. Bleaching agent action on color stability, surface roughness and microhardness of composites submitted to accelerated artificial aging. Eur J Dent. 2011;5:143–9. [PMC free article] [PubMed] [Google Scholar]
- 31.Pruthi G, Jain V, Kandpal HC, Mathur VP, Shah N. Effect of bleaching on color change and surface topography of composite restorations. Int J Dent 2010. 2010 doi: 10.1155/2010/695748. 695748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.van Dijken JW, Hörstedt P. Marginal adaptation of composite resin restorations placed with or without intermediate low-viscous resin. An SEM investigation. Acta Odontol Scand. 1987;45:115–23. doi: 10.3109/00016358709098366. [DOI] [PubMed] [Google Scholar]
- 33.Zaimoglu A, Karaagaçlioglu L. Microleakage in porcelain laminate veneers. J Dent. 1991;19:369–72. doi: 10.1016/0300-5712(91)90060-c. [DOI] [PubMed] [Google Scholar]
- 34.Sim C, Neo J, Chua EK, Tan BY. The effect of dentin bonding agents on the microleakage of porcelain veneers. Dent Mater. 1994;10:278–81. doi: 10.1016/0109-5641(94)90075-2. [DOI] [PubMed] [Google Scholar]
- 35.Tjan AH, Dunn JR, Sanderson IR. Microleakage patterns of porcelain and castable ceramic laminate veneers. J Prosthet Dent. 1989;61:276–82. doi: 10.1016/0022-3913(89)90127-3. [DOI] [PubMed] [Google Scholar]
- 36.Boksman L, Jordan RE, Suzuki M, Galil KA, Burgoyne AR. Etched porcelain labial veneers. Ont Dent. 1985;62:11. 13, 15, 9. [PubMed] [Google Scholar]
- 37.Atsu SS, Aka PS, Kucukesmen HC, Kilicarslan MA, Atakan C. Age-related changes in tooth enamel as measured by electron microscopy: Implications for porcelain laminate veneers. J Prosthet Dent. 2005;94:336–41. doi: 10.1016/j.prosdent.2005.08.008. [DOI] [PubMed] [Google Scholar]
- 38.Crim GA. Prerestorative bleaching: Effect on microleakage of Class V cavities. Quintessence Int. 1992;23:823–5. [PubMed] [Google Scholar]
- 39.Ulukapi H, Benderli Y, Ulukapi I. Effect of pre- and postoperative bleaching on marginal leakage of amalgam and composite restorations. Quintessence Int. 2003;34:505–8. [PubMed] [Google Scholar]
- 40.Türkün LS, Türkün M. Effect of bleaching and repolishing procedures on coffee and tea stain removal from three anterior composite veneering materials. J Esthet Restor Dent. 2004;16:290–301. doi: 10.1111/j.1708-8240.2004.tb00056.x. [DOI] [PubMed] [Google Scholar]