

Abstract
Statement of Problem:
Surface of porcelain restoration is a matter of clinical concern because of its abrasive action on the opposing enamel.
Purpose:
This study comparatively evaluated wear of enamel when opposed by three different surface finishes of ceramic.
Materials and Methods:
A total of 60 metal-ceramic discs (10 mm × 2 mm) with different surface finishes were fabricated. They were divided into four groups of autoglazed ceramic surface, over glazed ceramic surface, ceramic surface polished with Shofu polishing kit and ceramic surface polished with DFS polishing wheels and paste. Each group comprised of 15 discs. Sixty human teeth samples were prepared from freshly extracted, unrestored, caries free, nonattrited maxillary first premolars. Each tooth sample was weighed before wear testing using AT200 Mettler Toledo electronic analytical balance of 0.0001 g accuracy. Occlusal surfaces of these teeth were then abraded against the substrates in a wear machine for a total of 10,000 cycles. Each tooth sample was weighed after 5000 cycles and after the total of 10,000 cycles, respectively, using the same balance. Differences in weight of tooth samples before and after wear testing were evaluated statistically using one-way analysis of variance and Bonferroni's correction for multiple group comparisons.
Results:
The values obtained for percentage weight loss after 10,000 cycles for over glazed ceramic surface were marginally higher than values obtained for autoglazed surface. It was observed that values obtained for percentage weight loss by polished ceramic after 10,000 cycles were statistically less as compared to the values obtained with autoglazed and over glazed ceramic surface (P < 0.001). There was no statistically significant difference between the values obtained by polished ceramic surfaces of two different groups.
Conclusion:
Enamel wear produced by polished porcelain is substantially less than autoglazed and over glazed porcelain. No significant difference was found in enamel wear when opposed by ceramic surfaces polished by two different methods. This study indicates the potential damage porcelain can inflict upon enamel and suggests that porcelain should be polished instead of over glazed.
Keywords: Abrasiveness, enamel wear, glazed ceramic, polished ceramic, surface finish
Clinical Implication: Porcelain has been used in dentistry for many years, and in many forms, as it is the most esthetic restorative material. Its greatest shortcoming is its abrasiveness. One of the reasons for its abrasiveness is its surface finish. According to this study, if the porcelain is well-polished, it is less abrasive as compared to the glazed finish.
INTRODUCTION
Restoration of missing, decayed or mutilated dentition has been one of the foremost responsibilities of dentists the world over. Materials selected for the restoration of teeth should fulfill the basic criteria of strength, biocompatibility and esthetics. In the past, metals were employed widely due to their unsurpassed strength, but their esthetic limitations led to the advent of porcelain. Recent years have shown a paradigm shift, with greater emphasis being laid on superior esthetics with ceramic becoming the current panacea.[1]
Brittleness of ceramics with the advent of newer metal free ceramics was overcome, but the increased strength itself remained an area of concern as it led to wearing down of opposing natural dentition. In spite of the constant evolution of restorative materials, their abrasive action on the opposing natural dentition has never been completely overcome and has remained a matter of clinical concern. Ideally a restorative material which either replaces enamel or opposes enamel should have functional characteristics similar to enamel.[2] “Wear” is defined as the loss of a substance due to continual use. Wear in dentistry occurs when two articulating surfaces undergo slipping and sliding movements against one another when a load is applied. The Institute of Mechanical Engineers of UK defined wear as “the progressive loss of substance from a body brought about by mechanical action”.[3] Seghi[4] stated that the wear rate of a restorative material should be equal to that of enamel. Lambrechts[5] reported that the wear of enamel opposing enamel is 20–40 μm/year and an ideal restorative material should mimic that. Excessive wear of teeth, restoration or the entire dentition may be associated with supra eruption of opposing teeth, periodontal breakdown, traumatic occlusion, loss of vertical dimension and even temporomandibular joint dysfunction.[6] Evaluation of wear leads us to its clinical significance which may have both systemic and biologic consequences.[7] The severity of this problem was best illustrated by Wiley[8] who stated that “group function in porcelain can elicit group destruction.” Hence the choice of the restorative material and its surface finish is of paramount importance.
Studies have shown that the wear rate of enamel depends on the texture and surface finish of the opposing restorative material. Ceramics can either be polished or glazed to achieve a good finish. Many studies were performed to identify finishing and polishing techniques that would create surfaces as smooth as or smoother than glazed porcelain. But the results were inconsistent. Differences in surface finish of ceramic may be responsible for variations in the amount of enamel wear.
Hence this study was undertaken to comparatively evaluate the wear of enamel surface when opposed by autoglazed, over glazed and polished ceramic so that the right choice could be made while deciding the surface finish for ceramic restoration and De Van's principle of preserving what is remaining rather than meticulous restoration of what is missing could be successfully employed.
MATERIALS AND METHODS
Total of 60 metal-ceramic discs were fabricated. Each finished disc was of the dimensions 10 mm × 2 mm (diameter × thickness). Total thickness of the disc was measured with metal and ceramic together. Initially, a custom milled steel template with 24 standardized circular moulds was fabricated [Figure 1]. Each inner mould was of the diameter 10mm and depth 0.5mm. This template was fabricated only for the metal disc fabrication as the desired thickness of each metal disc was 0.5mm. Sixty such metal discs of standard dimensions were fabricated. The metal used for casting was “4 all” which is a nickel-chromium alloy meant for metal-ceramics. Another custom milled steel template with 24 individual standardized moulds was fabricated. Each inner mould of this second template was of diameter 10mm and depth 2mm. Second template was used for ceramic built up. Steel template was duplicated in reversible hydrocolloid material that is, agar. It was then poured in phosphate bonded investment material. Three such refractory casts were obtained [Figure 2]. The finished metal discs were sandblasted. All the discs were then secured in refractory casts within each mould [Figure 3]. Vita Vacumat, 40 Furnace was used for ceramic built up. Degassing was carried out for all the discs. Two layers of opaque porcelain were applied, and discs were fired. Discs were then layered with feldspathic leucite ceramic layering material by Ivovlar Vivadent, IPS d.Sign. Condensing of dentin and enamel porcelain was done using the standard protocol for all the discs to achieve the thickness of 1.5 mm. Thickness of the dentin porcelain was 1 mm, and enamel porcelain was 0.5 mm. It was measured using a micrometer (±1 μ), Draper, Japan. All the discs were then autoglazed by progressively increasing the furnace temperature to 975°C. After cooling, discs were retrieved from the refractory casts [Figure 4]. Fifteen discs were randomly selected and kept aside as a control group (Group I – control/autoglazed ceramic surface). Remaining 45 metal-ceramic discs were mounted on plaster blocks and stabilized on the milling machine, Amann Girrbach af 350 [Figure 5]. Ceramic surface of the discs was roughened with Shofu adjustment bur to simulate chair side adjustment of the ceramic restorations. Straight hand piece at the speed of 10,000 rpm was used at constant pressure. All the discs were then finished using Shofu finishing cone (yellow ring). One finishing cone was used only for three samples. Samples were then randomly divided into three groups of 15 each. Group II comprised of over glazed ceramic samples. Glaze liquid was applied evenly to 15 discs of this group with sable brush [Figure 6]. Discs were then fired at the temperature of 915°C for glaze firing (Group II – over glazed ceramic surface). Polishing was done by two different methods for the samples of Group III and IV. Fifteen samples of Group III were polished using Shofu polishing kit [Figure 7]. Polishing cones with white ring for ultra-fine surface were used for polishing at the speed of 10,000rpm using gentle and even pressure for all the samples. Only one operator polished all the samples. One polishing cone was used only for three samples. Samples were then cleaned in an ultrasonic cleaner for 10 min (Group III – ceramic surface polished with Shofu polishing kit). Fifteen samples of Group IV were polished using DFS polishing wheel and polishing paste by Ivoclar Vivadent [Figure 8]. Straight handpiece at the speed of 10,000 rpm was used with even and gentle pressure for this purpose. One wheel was used for three samples. Samples were then cleaned in an ultrasonic cleaner for 10 min (Group IV – ceramic surface polished with DFS polishing wheel and polishing paste). All the ceramo metal discs of different groups were mounted in self-cure acrylic resin [Figure 9].
Figure 1.

Custom milled steel template with standardized moulds
Figure 2.

Refractory casts
Figure 3.

Metal discs secured in refractory casts
Figure 4.
Standardized metal-ceramic discs
Figure 5.
Discs stabilized on the milling machine to simulate chair side adjustments
Figure 6.

Samples of Group II (glazed ceramic surface)
Figure 7.
Samples of Group III polished with shofu kit
Figure 8.

Samples of Group IV polished with DFS wheels
Figure 9.
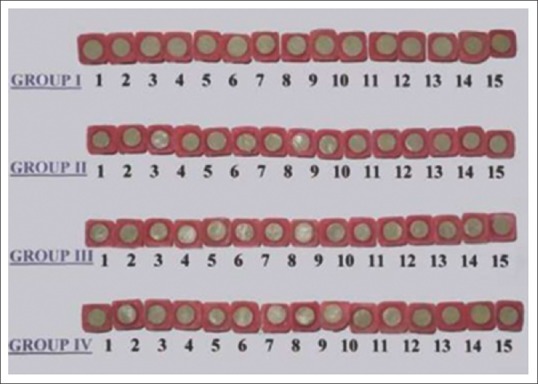
Samples of ceramo-metal discs mounted on acrylic blocks
Total 60 freshly extracted human unrestored, caries free, nonattrited maxillary first premolars of young adolescent patients undergoing orthodontic extractions were collected. They were disinfected in formalin and preserved in saline. Occlusal anatomy of all the teeth was observed under a stereomicroscope, Zoom (MV-NSZ-405). Only those teeth having sharp cusps and proper anatomy were selected. Teeth were sectioned transversely at the cemento-enamel junction to separate crowns from the roots. All the crowns of premolars were mounted in self-cured acrylic resin. Sixty mounted extracted premolars were then randomly divided into four groups of 15 each [Figure 10].
Figure 10.
Extracted premolars mounted on acrylic blocks
Each mounted tooth sample was weighed before testing, using AT200 Mettler Toledo electronic analytical balance of 0.0001 g accuracy [Figure 11]. As this electronic machine had a fully automated calibration technology and a micro weighing scale, values of all the mounted premolars were accurately measured. Each mounted specimen was cleaned and dried with absorbent paper before weighing. To ensure accuracy, the balance was kept on a free-standing table at all times, away from vibrations, and weighed the specimens with the glass doors of the balance closed to avoid the effect of air currents.
Figure 11.

Electronic analytical balance of 0.0001g accuracy
The mounted discs and extracted human premolars were placed onto holders on a two-body wear machine, 5130 Taber Abraser, which provided contact between the specimens. Tooth sample was attached to the lower member (rotating wheel), and the disc was attached to the upper member. The test samples were positioned in holders and additionally secured to the machine with the sticking tape. The cusp tips and ceramic discs were positioned under a constant load of 1.5 kg and sprayed with artificial saliva (Biomed, MP Sai, Mumbai, India) for the entire duration of the experiment [Figure 12]. The specimens were made to rub against one another in a sliding motion to simulate the oral wear cycle. The test was run for a total of 10,000 cycles on the wear machine, for each pair of samples. Each tooth sample was also weighed after first 5000 cycles. This was done in order to determine if wear rate varied with duration of testing.
Figure 12.

Samples mounted against each other on a wear machine during testing
All the mounted premolars were weighed after 10,000 cycles. The same protocol used for measuring baseline weight was repeated. The readings, baseline, intermediate and final that is, before testing, after 5000 cycles and after 10,000 cycles of wear for each tooth sample, were statistically analyzed to obtain the tooth substance loss at each interval.
RESULTS
The data on percentage weight change is shown as median with minimum and maximum for each group. For this study, median was used as it does not get affected by the wide variations in values. Relative percentage change in weight was calculated using the following formula:

The statistical comparison of average levels of percentage change in weight between various groups was done using one-way analysis of variance technique with Bonferroni's correction for multiple group comparisons as appropriate with necessary transformations to satisfy underlying normality assumption. Within the group, comparison was done by Paired analysis using Wilcoxon's signed rank test, a nonparametric test procedure.
After analyzing statistically according to the formula mentioned above, following results were obtained:
The median percentage weight loss of tooth samples with autoglazed ceramic samples was 0.08 after first 5000 cycles, 0.08 after second 5000 cycles and 0.16 after 10000 cycles. The values ranged from 0.06 to 0.11, 0.07 to 0.10 and 0.13 to 0.20, respectively [Table 1]. No statistically significant difference was found in the weight loss after first and second 5000 cycles [P > 0.05, Table 2]. This means wear of enamel increased consistently with an increase in number of cycles.
Table 1.
Comparison of groups for percentage change in weight

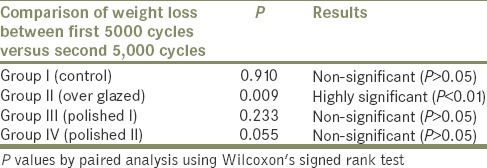
Table 2.
Comparison within each group for a percentage change in weight after first 5000 and second 5000 cycles
The median percentage weight loss of tooth samples with over glazed ceramic samples was 0.11 after first 5000 cycles, 0.07 after second 5000 cycles and 0.18 after 10000 cycles. The values ranged from 0.02 to 0.30, 0.0 to 0.16 and 0.14 to 0.31, respectively [Table 1]. It was observed that values obtained after first 5000 cycles were significantly high than those obtained after second 5000 cycles. This means wear of enamel increased with increase in number of cycles but was more during first 5000 cycles than second 5000 cycles [P < 0.001, Table 2]. The values obtained for percentage weight loss after 10000 cycles for over glazed ceramic surface were marginally higher than values obtained for autoglazed surface. However, the difference was not statistically significant with P value of 0.153 [P > 0.05 Table 3].
Table 3.
Comparison between the groups for percentage change in weight after 10,000 cycles
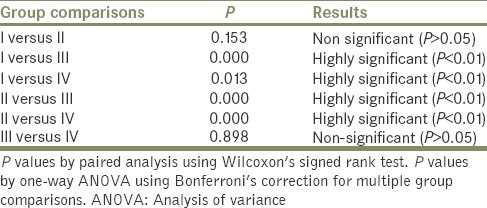
The median percentage weight loss of tooth samples with polished ceramic samples (Group III, polishing done with Shofu polishing kit) was 0.06 after first 5000 cycles, 0.06 after second 5000 cycles and 0.11 after 10000 cycles. The values ranged from 0.03 to 0.08, 0.04 to 0.08 and 0.07 to 0.16, respectively [Table 1]. No statistically significant difference was found in the weight loss after first and second 5000 cycles [P > 0.05, Table 2]. This means wear of enamel increased consistently with increase in number of cycles. It was observed that values obtained for percentage weight loss by polished ceramic after 10000 cycles were statistically less as compared to the values obtained with autoglazed and over glazed ceramic surface [P < 0.001, Table 3].
The median percentage weight loss of tooth samples with polished ceramic samples (Group III, polishing done with polishing wheels and paste) was 0.06 after first 5000 cycles, 0.06 after second 5000 cycles and 0.11 after 10000 cycles. The values ranged from 0.03 to 0.10, 0.04 to 0.10 and 0.07 to 0.20, respectively [Table 1]. No statistically significant difference was found in the weight loss after first and second 5000 cycles [P > 0.05, Table 2]. This means wear of enamel increased consistently with an increase in number of cycles. It was observed that values obtained for percentage weight loss by polished ceramic after 10000 cycles were statistically less as compared to the values obtained by autoglazed and over glazed ceramic surface [P < 0.001, Table 3]. There was no statistically significant difference between the values obtained by polished ceramic surfaces of two different groups (Group III and IV) [P > 0.05, Table 3]. This means two different techniques of polishing ceramic used in this study give similar surface finish which caused the least enamel wear.
DISCUSSION
The surface wear of natural tooth structure and antagonistic restorative material occurs at an ultrastructural level. Structure of restorative material, crystal size and surface hardness all play a role in controlling antagonistic enamel wear. Won et al.[9] studied microstructural factors affecting enamel and ceramic wear; these factors were hardness, frictional resistance, fracture toughness, porosity, crystals, chemical degradation and surface finish. Ceramics can either be polished or glazed to achieve a good finish, which can affect wear of antagonist enamel. This study investigated the wear of enamel when opposed by autoglazed, over glazed and polished ceramic of ceramo-metal restorative material (IPS d.Sign) using a wear machine that was modified in an attempt to simulate the wear process that occurs in the mouth. IPS d.Sign is fluoroapatite leucite based glass ceramic with excellent esthetic properties. It was selected to check its wear compatibility to enamel. The wear machine used provided a combined action of the impact, followed by sliding that matches the inherent action of closure during mastication of the mandibular teeth onto the maxillary teeth. The regime for wear testing was based on previous reports from the literature.[10,11,12] In this study, cusp tips of maxillary premolars were positioned against the restorative surface under the constant load of 13.5 N. For each sample, abrasive test was run for a total of 10000 cycles on the wear machine.[12] Artificial saliva, Biomed, was used in this study to simulate oral environment. The wet oral environment imparts positive surface charge on ceramics leading to loss of sodium ions and thereby reducing surface hardness.[9]
In the present study, occlusal enamel surface was tested to evaluate wear. Phillips[13] stated that enamel varies in its properties depending on the position of the enamel on the tooth and its histological structure. Hence in this study, freshly extracted nonattrited maxillary first premolars of young adolescent patients undergoing orthodontic extractions were used. Ahmad et al.[14] studied the effect of handpiece speed on the flexural strength of ceramic and concluded that simulated clinical polishing at 10,000 rpm did not appear to substantially strengthen or weaken the ceramic specimens. Polishing at 20,000 rpm reduced flexural strength of the ceramic bars. In this study, all the metal-ceramic samples were finished and polished at 10,000 rpm speed with constant pressure.
The results indicate that enamel loss was significantly different (P < 0.001) depending on the surface condition (polished and glazed, P < 0.001) as indicated in Tables 2 and 3. Significant enamel loss was shown by over glazed and autoglazed ceramic surfaces, followed by polished surfaces of ceramo-metal. Both the polished surfaces of ceramo-metal showed the least wear (Group III and IV). Over glazed surface of ceramic caused marginally high wear than autoglazed ceramic surface [Graph 1]. However, the difference was statistically insignificant.
Graph 1.
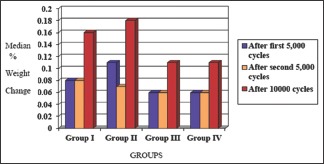
Comparison of groups for percentage change in weight. Values are median (minimum-maximum)
This study shows that over the glazed surface of ceramic causes significant enamel wear. This could be attributed to the fact that the hardness of the glazed surface is higher.
According to the results of this study autoglazed ceramic surface caused significantly higher wear than polished ceramic surface. This does not support the work of Monasky and Taylor,[15] Wiley,[8] and Jagger and Harrison.[10] They all reported that there is no statistically significant difference in the average surface roughness between the final polished surface and the initial autoglazed surface of ceramic. According to this study, polished surface of ceramic is the least detrimental to opposing dentition.
Significant correlation was also found between initial and subsequent wear of enamel at different intervals. The enamel wear produced by over the glazed surface was significantly greater initially (up to first 5000 cycles) while the percentage of wear receded during 2nd 5000 cycles. Multiple comparisons were done to evaluate the amount of enamel wear produced by the different ceramic surface finish groups at each measurement time (after 1st 5000 cycles, after 2nd 5000 cycles and after 10000 cycles). The difference in the amount of enamel wear produced by autoglazed and polished ceramics was not statistically significant after 1st 5000 cycles and after 2nd 5000 cycles. The comparisons showed that at both the intervals, the amount of enamel wear produced by autoglazed and polished ceramic was consistent [P > 0.005, Table 3]. This could be attributed to the fact that the glaze was removed after the short period of time intraorally.[10] Thus after the glaze is removed wear rate reduces comparatively. The results of this study indicate that polished ceramics produce less enamel wear than their glazed counterparts. Mahalick et al.[3] have stated that the amount of enamel wear depends on factors such as neuromuscular forces, lubricants, foreign bodies, patient habits and type of restorative material used. Of all these, the prosthodontist has the most control over the choice of restorative material selected and its surface finish. Hence, the use of glazed ceramic should be gradually phased out as it was found to cause maximum damage to the opposing dentition. The polished ceramic surface is the gateway to the future of ceramic restorations as it is kind to the opposing dentition. Further in vivo studies can be carried out to correlate the results achieved by this in vitro study.
CONCLUSIONS
Within the limitations of this in vitro study and after analyzing the data statistically the following conclusions were drawn:
Both the polished surfaces of ceramic polished with Shofu system and with DFS system with polishing paste showed the least enamel wear among the four groups
Over glazed surface of ceramic caused the maximum amount of wear
Autoglazed surface of ceramic caused marginally less wear than over the glazed surface but the difference was not statistically significant
No significant difference was found in enamel wear when opposed by ceramic surfaces polished by two different methods
Wear caused by over glazed surface of ceramic was more initially during the first 5000 cycles and the wear rate receded during the second 5000 cycles
Wear caused by autoglazed and polished ceramic increased consistently with an increase in number of cycles.
Thus, the conclusion of this in vitro study is that the enamel wear produced by polished porcelain is substantially less than autoglazed and over glazed porcelain. This study indicates the potential damage porcelain can inflict upon the enamel and suggests that porcelain should be polished instead of over glazed.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Kelly JR, Nishimura I, Campbell SD. Ceramics in dentistry: Historical roots and current perspectives. J Prosthet Dent. 1996;75:18–32. doi: 10.1016/s0022-3913(96)90413-8. [DOI] [PubMed] [Google Scholar]
- 2.Hudson JD, Goldstein GR, Georgescu M. Enamel wear caused by three different restorative materials. J Prosthet Dent. 1995;74:647–54. doi: 10.1016/s0022-3913(05)80319-1. [DOI] [PubMed] [Google Scholar]
- 3.Mahalick JA, Knap FJ, Weiter EJ. Occusal wear in prosthodontics. J Am Dent Assoc. 1971;82:154–9. doi: 10.14219/jada.archive.1971.0018. [DOI] [PubMed] [Google Scholar]
- 4.Seghi RR, Rosenstiel SF, Bauer P. Abrasion of human enamel by different dental ceramics in vitro . J Dent Res. 1991;70:221–5. doi: 10.1177/00220345910700031301. [DOI] [PubMed] [Google Scholar]
- 5.Lambrechts P, Braem M, Vanherle G. Buonocore memorial lecture. Evaluation of clinical performance for posterior composite resins and dentin adhesives. Oper Dent. 1987;12:53–78. [PubMed] [Google Scholar]
- 6.Okeson JP. Management of Temporo-mandibular Disorders and Occlusion. St. Louis: Mosby; 1989. pp. 259–60. [Google Scholar]
- 7.Heintze SD. How to qualify and validate wear simulation devices and methods. Dent Mater. 2006;22:712–34. doi: 10.1016/j.dental.2006.02.002. [DOI] [PubMed] [Google Scholar]
- 8.Wiley MG. Effects of porcelain on occluding surfaces of restored teeth. J Prosthet Dent. 1989;61:133–7. doi: 10.1016/0022-3913(89)90360-0. [DOI] [PubMed] [Google Scholar]
- 9.On WS, Delong R, Kenneth J. Anusavice: Effect of restorative materials on wear of human enamel. J Prosthet Dent. 2002;64:194–203. [Google Scholar]
- 10.Jagger DC, Harrison A. An in vitro investigation into the wear effects of unglazed, glazed, and polished porcelain on human enamel. J Prosthet Dent. 1994;72:320–3. doi: 10.1016/0022-3913(94)90347-6. [DOI] [PubMed] [Google Scholar]
- 11.al-Hiyasat AS, Saunders WP, Smith GM. Three-body wear associated with three ceramics and enamel. J Prosthet Dent. 1999;82:476–81. doi: 10.1016/s0022-3913(99)70037-5. [DOI] [PubMed] [Google Scholar]
- 12.Elmaria A, Goldstein G, Vijayaraghavan T, Legeros RZ, Hittelman EL. An evaluation of wear when enamel is opposed by various ceramic materials and gold. J Prosthet Dent. 2006;96:345–53. doi: 10.1016/j.prosdent.2006.09.002. [DOI] [PubMed] [Google Scholar]
- 13.Phillips RW. Skinners Science of Dental Materials. W. B. Saunders Co. Hartcourt Brace and Co. Int; 1982. [Google Scholar]
- 14.Ahmad R, Morgano SM, Wu BM, Giordano RA. An evaluation of the effects of handpiece speed, abrasive characteristics, and polishing load on the flexural strength of polished ceramics. J Prosthet Dent. 2005;94:421–9. doi: 10.1016/j.prosdent.2005.08.014. [DOI] [PubMed] [Google Scholar]
- 15.Monasky GE, Taylor DF. Studies on the wear of porcelain, enamel, and gold. J Prosthet Dent. 1971;25:299–306. doi: 10.1016/0022-3913(71)90191-0. [DOI] [PubMed] [Google Scholar]