

Abstract
Neuroendocrine tumors are the most common primary tumors of the small bowel, but diagnosis is usually delayed as the lesions are small and symptoms are mild or nonspecific. Diagnosis of this disease is currently based on radiologic or endoscopic findings. Ultrasound (US) is used as a first-line examination in patients with abdominal symptoms, as this technique permits an overall view of the gastrointestinal tract providing diagnosis of inflammatory and/or neoplastic disorders in a large proportion of patients. The aim of this case report is to describe the feasibility and diagnostic accuracy of elastography in the diagnosis of a tumor of the ileum. The patient underwent conventional gray-scale US and elastography before surgery and these examinations were repeated postoperatively on the surgical specimen confirming preoperative outcome.
Keywords: Tumor, Neuroendocrine tumors, Small bowel, Ultrasound
Riassunto
Il tumore neuroendocrino, tra le neoplasie primitive dell’intestino tenue, è il più frequente, la diagnosi è usualmente tardiva per le piccole dimensioni e per la sintomatologia lieve, poco specifica. La diagnosi di questa forma morbosa si basa attualmente su metodiche radiologiche o endoscopiche. L’ecografia è indagine di primo livello in soggetti con sintomatologia addominale ed in una percentuale di soggetti permette anche lo studio del tubo digerente e la diagnosi di patologie neoplastiche o infiammatorie. Scopo del lavoro è di descrivere l’utilità della elastografia nella diagnosi di un tumore dell’ileo in cui l’esame ecografico convenzionale ed elastografico sono stati effettuati sul paziente prima dell’intervento chirurgico e successivamente sul pezzo operatorio con conferma dei riscontri precedenti all’intervento.
Introduction
Neuroendocrine tumors are the most common primary tumors of the small bowel. In most cases they are sporadic, the age at onset is advanced and diagnosis is often delayed due to the small size of the lesion and nonspecific symptoms. Carcinoid syndrome occurs only in about 10 % of patients with neuroendocrine tumor of the small bowel.
Ultrasound (US) is used as a first-line examination in patients with abdominal symptoms, as this technique permits an overall view of the gastrointestinal tract providing diagnosis of inflammatory or neoplastic disorders in a large proportion of patients.
The aim of this paper is to describe a case of neuroendocrine tumor of the ileum which was diagnosed with US imaging and to evaluate the contribution of elastography in the characterization of the tumor.
Case report
An 87-year-old man with ischemic heart disease associated with atherosclerotic peripheral arterial disease was hospitalized due to recurrent episodes of abdominal pain which was accentuated by eating.
Routine blood tests showed mild macrocytic anemia and mild to moderate renal insufficiency. The remaining blood chemistry data including common tumor markers (CEA, CA 19.9, CA 125) were within normal range.
After abdominal X-ray (two air-fluid levels in the left upper quadrant) and abdominal computed tomography (CT) revealing abnormal morphology of a portion of the small bowel with adjacent mesenteric lymphadenopathy (2 cm), the patient was referred to our section for abdominal US examination.
After overnight fasting, the patient underwent US examination and elastography focused on the abnormal portion of the small bowel, performed on Mylab Alpha scanner (Esaote Biomedica, Genoa, Italy) using a linear probe (SL 1543 13–4 MHz). These imaging examinations were repeated postoperatively on the adequately prepared surgical specimen.
Strain elastography is already used in clinical practice to study breast, thyroid and musculoskeletal lesions. This strain elasticity imaging method is defined as “quasi-static” and probe compression is applied to obtain a color elastogram showing the stiffness of the region of interest in comparison with the adjacent tissues.
Strain elastography is a qualitative examination and the elastic properties of the adjacent tissues is mapped in a color scale ranging from red indicating “maximum elasticity” to blue indicating “maximum stiffness”, including various shades of yellow, green and turquoise indicating intermediate stiffness values.
In this patient, gray-scale US imaging revealed a short (1 cm) pseudonodular thickening of the bowel wall (6 mm; Fig. 1) protruding into the lumen, loss of bowel wall stratification and the presence of enlarged lymph nodes, one of which was 2 cm in diameter. Color Doppler US showed irregular blood flow of the pseudonodular thickening of the bowel wall.
Fig. 1.
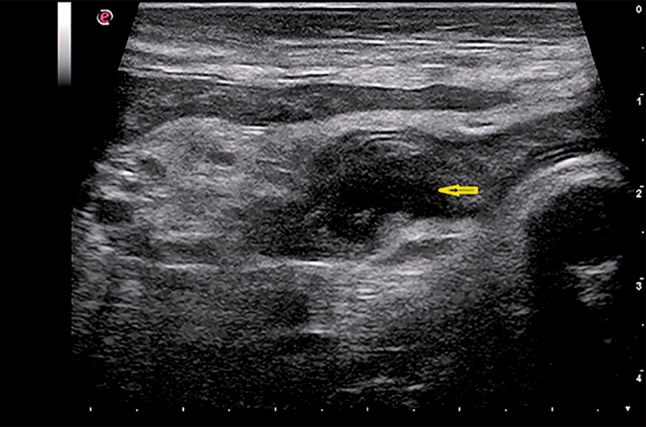
Gray-scale US scan shows pseudonodular hypoechoic thickening of the small bowel (arrow) with loss of bowel wall stratification
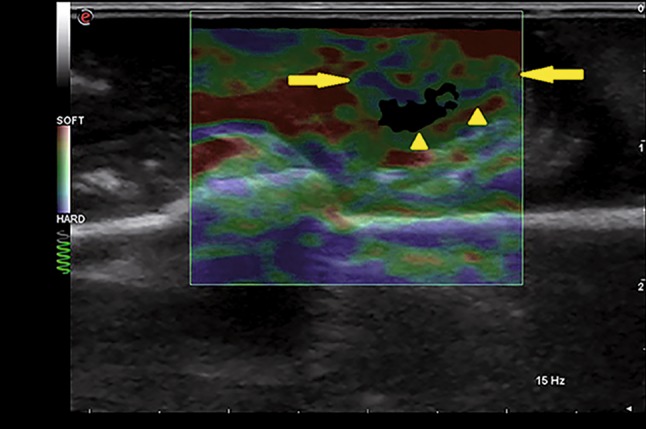
Elastography showed a mosaic color pattern of mainly green and blue in correspondence with the thickening of the bowel wall. This pattern suggested increased stiffness compared to the adjacent bowel wall, which presented a mosaic color pattern dominated by green with shades of yellow and red (Fig. 2). The color pattern of the lymph node was mainly green and turquoise with shades of blue (<30 %) (Fig. 3). These findings suggested neoplasia of the ileum with lymph node metastases.
Fig. 2.
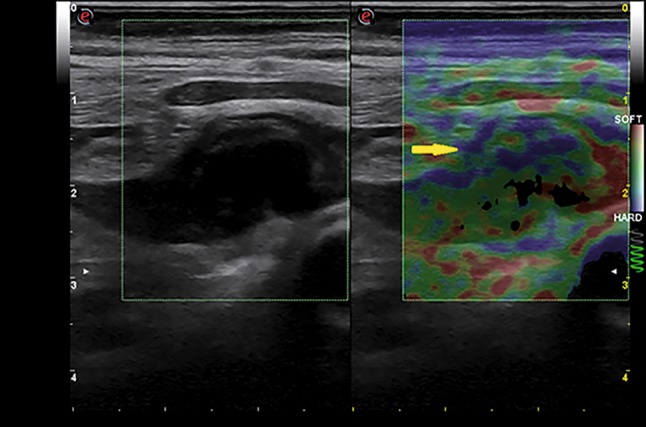
Elastography scan shows hypoechoic pseudonodular thickening of the small bowel (arrow) represented by a mosaic of mainly green and blue colors
Fig. 3.
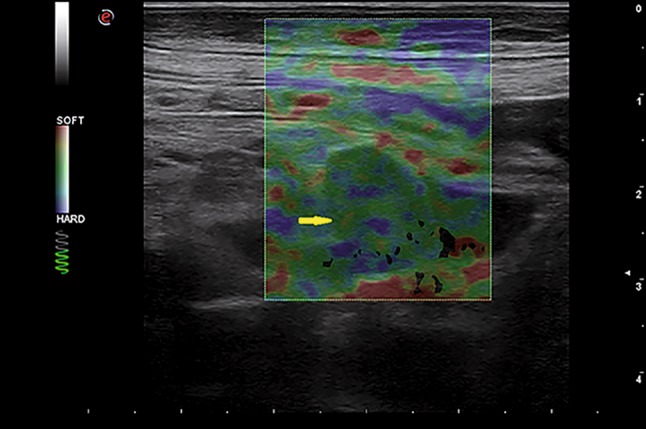
Near the tumor, elastography scan shows a lymph node (2 cm in diameter, arrow) represented by a mosaic of colors (green, turquoise and blue) suggestive of increased stiffness
After CT enterography and surgery, which confirmed the diagnosis, elastography was repeated on the adequately prepared surgical specimen. Preoperative elastographic findings were confirmed as the color pattern was mainly green, turquoise and blue which indicated a tumor of greater stiffness than the adjacent intestinal wall (Figs. 4, 5).
Fig. 4.
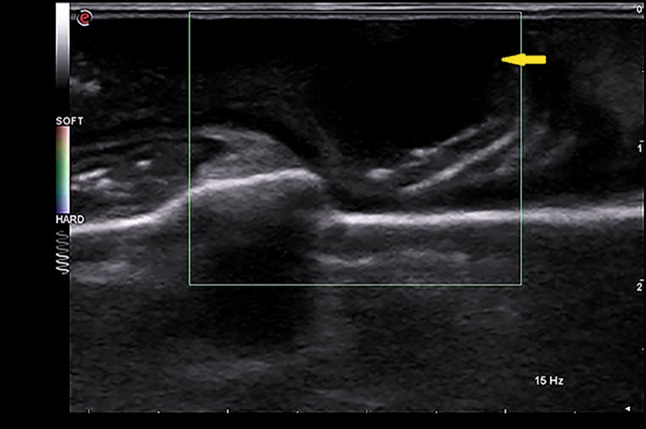
Gray-scale US scan performed on the adequately prepared surgical specimen. The tumor is evidenced as a hypoechoic thickening (arrow) with loss of bowel wall stratification
Fig. 5.
Elastography scan performed on the adequately prepared surgical specimen. The tumor (arrows and arrowheads) is represented by a mosaic of colors (mainly green, turquoise and blue) suggestive of a greater stiffness than the adjacent wall (mainly red)
Final diagnosis based on gross and microscopic examination of the surgical specimen was neuroendocrine neoplasia of the ileum with lymph node metastases.
Histological examination revealed the presence of an expansive lesion with irregular margin, consisting of small cells arranged in islands, nests and trabeculae with peripheral palisade appearance, uniform nuclei and rare mitoses. Neoplastic aggregates appeared embedded in fibroconnective tissue and were associated with areas of smooth muscle hyperplasia. This was probably the reason for the increased stiffness detected at elastography (Figs. 6, 7). Macroscopically these findings corresponded to a narrowing of the intestinal lumen.
Fig. 6.
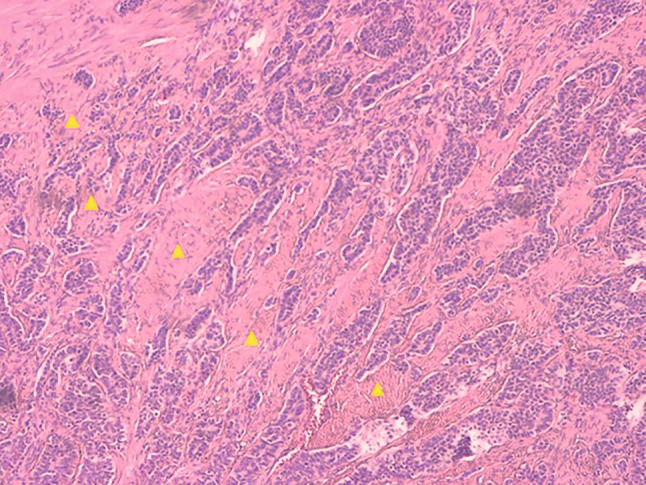
Hematoxylin–eosin, ×10 magnification. Islands and trabeculae of neoplastic cells with eosinophilic cytoplasm, minimal pleomorphism and rare mitosis embedded in abundant fibroconnective stroma (arrowheads), which separates the neoplastic aggregates
Fig. 7.
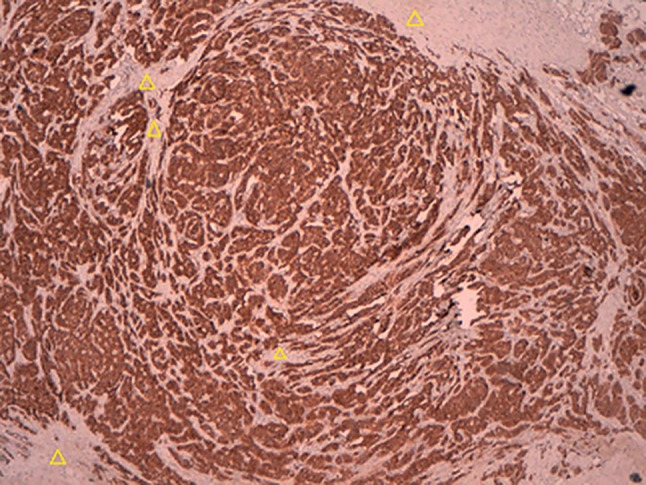
Immunohistochemical staining of CD56 (neuroendocrine tumor marker), ×10 magnification. The epithelial component shows positive staining for CD56, but not the stromal component (arrowheads)
Discussion
Diagnosis of small bowel tumors is mainly based on specific diagnostic imaging methods such as magnetic resonance imaging (MRI) enterography, CT enterography or endoscopic techniques, such as video capsule endoscopy or double-balloon enteroscopy. The aim of this paper is to evaluate the usefulness of elastography in characterizing the tissue of a small bowel tumor already detected at gray-scale US.
Elastography generally presents additional difficulties in the study of the gastrointestinal tract as the bowel walls are thin and due to the presence of gas and peristalsis. However, these difficulties are reduced in the presence of pathology because of increased thickness of the bowel walls, absent or reduced peristalsis and reduced lumen.
In the present case, the data obtained at strain elastography performed before surgery suggested a greater stiffness of the tissue in question; this outcome was confirmed after surgery. The different stiffness of the tumor compared to the adjacent bowel wall can be explained by histological features of multiple fibroconnective tissue septa in the tumor.
Increased stiffness of a focal lesion detected at elastography is usually suggestive of malignancy in other applications of the method, such as breast, thyroid and lymph node diseases. However, few data are reported in the literature on the use of elastography in neoplastic diseases of the gastrointestinal tract.
The recent European Guidelines suggest the use of elastography in the characterization of focal lesions of the digestive tract and in the differentiation between inflammatory and fibrotic stenosis in patients with Crohn’s disease (2013, [1]) Havre et al. [2] performed elastography on adequately prepared surgical specimens from 27 patients (18 specimens of adenocarcinoma, 4 specimens of adenoma and 16 specimens from patients with intestinal stenosis in Crohn’s disease) encountering increased stiffness compared to the adjacent bowel wall in both adenocarcinoma and intestinal stenosis in Crohn’s disease.
Waage et al. [3] studied a series of patients using an endorectal probe. Elastography presented a diagnostic accuracy of about 94 % in differentiating rectal adenomas (n = 23) from rectal carcinomas (n = 45).
Recently Cantisani et al. [4] published a case report describing a patient with gastric tumor. The lesion was characterized using CEUS, and elastography and was found stiffer than the adjacent tissues.
These preliminary data reported in the literature and the fact that the method is noninvasive, inexpensive, repeatable and presents no risk to the patient, do in our opinion justify that elastography should be considered a valid tool in the evaluation of focal lesions of the gastrointestinal tract.
Acknowledgments
Conflict of interest
Andrea Giannetti, Paola Randisi, Michela Stumpo, Francesco Coratti declare that they have no conflict of interest related to this paper. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. The patient provided written informed consent to the publication of this paper and to the inclusion in this article of information and images that could potentially lead to his identification.
References
- 1.Cosgrove D, Piscaglia F, Bamber J, et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 2: clinical application. Ultraschall Med. 2013;34(3):238–253. doi: 10.1055/s-0033-1335375. [DOI] [PubMed] [Google Scholar]
- 2.Havre RF, Leh S, Gilja OH, Ødegaard S, Waage JE, Baatrup G, Nesje LB. Strain assessment in surgically resected inflammatory and neoplastic bowell lesions. Ultraschall Med. 2011;35(2):149–158. doi: 10.1055/s-0032-1325535. [DOI] [PubMed] [Google Scholar]
- 3.Waage J, Havre R, Ødegaard S, Leh S, Eide GE, Baatrup G. Endorectal elastography in the evaluation of rectal tumours. Colorectal Dis. 2011;13:1130–1137. doi: 10.1111/j.1463-1318.2010.02440.x. [DOI] [PubMed] [Google Scholar]
- 4.Cantisani V, Rubini A, Miniaggio G. CEUS and strain elastography in gastric carcinoma. J Ultrasound. 2013;16:123–125. doi: 10.1007/s40477-013-0024-y. [DOI] [PMC free article] [PubMed] [Google Scholar]