

Abstract
Background:
Esophageal cancer is the sixth cause of death in the world, there was a lack of population-based information on the trend and incidence rate of esophagus cancer, so this study aimed to determine the incidence and pathological changes of esophagus cancer in Iran.
Methods:
In this study, data were extracted from annual cancer registry reports of Iranian ministry of health between 2003 and 2008. Standardized incidence rates were calculated using the world standard population, and incidence rate was calculated by age groups, sex, and histological type. Data on epidemiologic trend and histology were analyzed using Joinpoint software package.
Results:
In this study, there were 18,177 recorded cases of esophagus cancer. Of all cases, 45.72% were females and 54.28% were males. Sex ratio was 1.19. The most common histological types related to squamous cell carcinoma NOS and adenocarcinoma NOS were 64.53% and 10.37%, respectively. The trend of annual changes of incidence rate significantly increased in both sexes. The annual percentage changes, the incidence rate was 7.9 (95% confidence interval [CI]: 3.3–12.6) for women and 9.6 (95% CI: 6.0–13.2) for men. The histology type of SCC, large cell, nonkeratinizing and SCC, keratinizing and SCC, NOS had a significant decreasing trend in total population (P < 0.05).
Conclusions:
According to this study, the trend of age-standardized incidence rate of esophagus cancer in Iran is rising. Hence, to prevent and control this cancer, it is necessary to investigate related risk factors and implement prevention programs in Iran.
Keywords: Epidemiology, esophagus cancer, histological change, Iran, trend
INTRODUCTION
It is estimated to increase the prevalence rate of cancer about 45% by 2025 in developed countries. Iran is one of developing countries, in which recently occurred the significant population growth and economic and social status changes.[1,2] Approximately, 51,000 new cases of all cancers were annually diagnosed in Iran. Nearly, 38% of these cancer cases in both sexes were due to gastrointestinal tract, of which 65,000 cases suffered from esophagus cancer.[3] Of yearly 35,000 death from cancer in Iran, 5800 cases were related to this cancer.[3] Esophagus cancer is the sixth cause of death in the world. About 407,000 people die from cancer worldwide.[4] Geographical distribution is one of the important factors in the incidence of cancers.[5,6,7,8] Esophagus cancer rarely occurs in Western countries, but it is considered one of the eight most common cancers in the world.[9] The highest incidence rate, 100–180/100,000, was observed in the North of Iran and North of China, while in the USA the rate was <5/100,000.[10]
The lack of early symptoms and the strong bilateral lymph flow of esophagus make the diagnosis to take place in advanced stages.[11] Both histological types of esophagus cancer (squamous cell carcinoma [SCC] and adenocarcinoma [ADC]) are very fatal, with 5 years survival <10%.[12]
In the past, 90% of cases of cancer were attributed to SCC. Over the past decades, ADC has increased, and recently constitutes 60% of the cancer cases.[2] In developing countries, such as Iran and China, SCC is the most common malignancy (90% of cases).[13] Recent studies in Iran showed that the prevalence of adenocarcinoma (ADS) is increasing.[14] This may be the improvement of public health, and epidemic of obesity and gastro-intestinal reflex diseases.[15]
Environmental factors, including Western lifestyles, are effective in the incidence and pathology of esophagus cancer, especially in developing countries such as Iran.[16] The lack of a comprehensive and population-based study on the incidence, pathological, and clinical aspects of esophagus cancer, this study investigated the epidemiological trend and pathological changes in esophagus cancer in Iran.
METHODS
Data source
This secondary data analysis study was carried out based on longitudinal program in Iran that have national registry of cancer (NCR) which is trying to identify all cases of cancer occurring in Iran. Data used in this study were obtained from NCR, and disease control and prevention of ministry of health and medical education in Iran for 2003–2008.[17] More details about cancer registry in Iran were previously published in the International Journal of Preventive Medicine.[18]
In this study, data on the incidence of esophageal cancer were selected according to the International Classification of Diseases-Oncology with the code C15 for age groups and sex.[19] Standardized incidence rates were calculated using the world standard population. The crude incidence data were also computed. Histological data, like squamous cell carcinoma NOS, SCC keratinizing, scc large cell nonkeratinizing, adenocarcinoma NOS, carcinoma NOS, also was extracted by sex and years of the study for the cancer.
Statistical analysis
We calculated crude incidence rate and the age-standardized incidence rate (ASIR)/100,000 persons. To describe incidence time trends for 6 years studied, we carried out joinpoint regression analysis using the software Joinpoint Regression Program, Version 4.1.1.1 October 2014.[20,21] As well to evaluate the histological changes, were obtained the percentage allocated for kind of histological types. So to analysis histology change percentage trends for 6 years, we used the software joinpoint regression program and carried out joinpoint regression analysis for data analysis. The test of significance uses a Monte Carlo permutation method (i.e., it finds “the best fit” line). Joinpoint regression analysis involves fitting a series of joined straight lines on a log scale to the trends. The final model selected was the most parsimonious of these, with the estimated annual percent change (APC) based on the trend within each segment. All statistical tests were two-sided. In describing trends, the terms “significant increase” or “significant decrease” signify that the slope of the trend was statistically significant (P < 0.05).
RESULTS
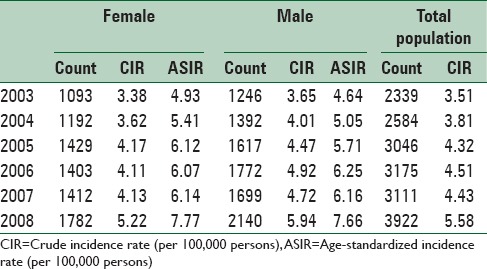
In this study, there were 18,177 recorded cases of esophagus cancer. Of all cases, 45.72% (8311 cases) were females and 54.28% (9866 cases) males. Sex ratio (male to female) was 1.19. The most common histological types related to squamous cell carcinoma NOS and adenocarcinoma NOS were 64.53% and 10.37%, respectively. Table 1 shows the number of cases, crude, and ASIRs.
Table 1.
Frequency, crude, and standardized incidence of esophagus cancer by sex, during the years 2003-2008
Epidemiological trend
To evaluate the changes in the incidence of esophageal cancer, comparison of ASIR indicated an increasing trend. In other words, the standardized incidence rate increased from 4.93 to 7.77 for women and from 4.64 to 7.66 for men. Results of joinpoint analysis revealed that the trend of annual changes of incidence rate significantly increased in both sexes. The Annual Percentage Changes (APC), the incidence rate was 7.9 (CI: 3.3-12.6) for women and 9.6 (CI: 6.0-13.2) for men [Figure 1].
Figure 1.
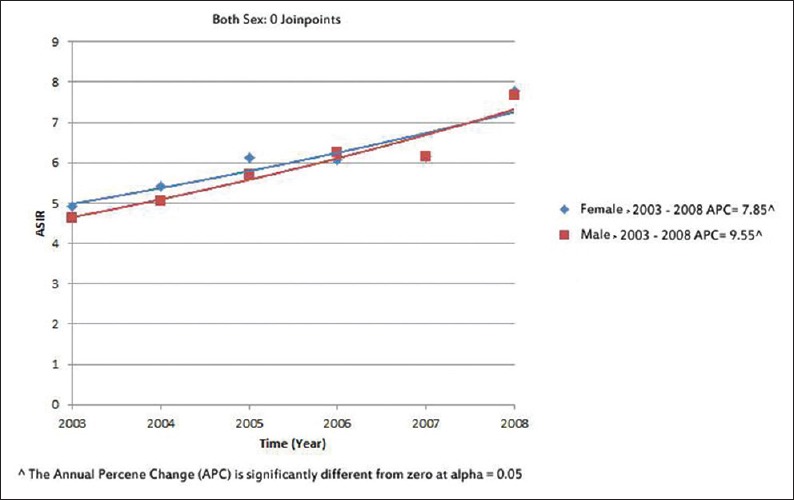
Joinpoint analysis for incidence of esophagus cancer (male and female) in Iran, 2003–2008; age-standardized rate/100,000 (using world standard population)
Histological trend
Two type of histology (squamous cell carcinoma NOS, and adenocarcinoma NOS) included 87.3%and 86.56% of the histology of esophageal cancer in women and men, respectively. The frequency of five common histological types of esophageal cancer is shown in Figure 2.
Figure 2.
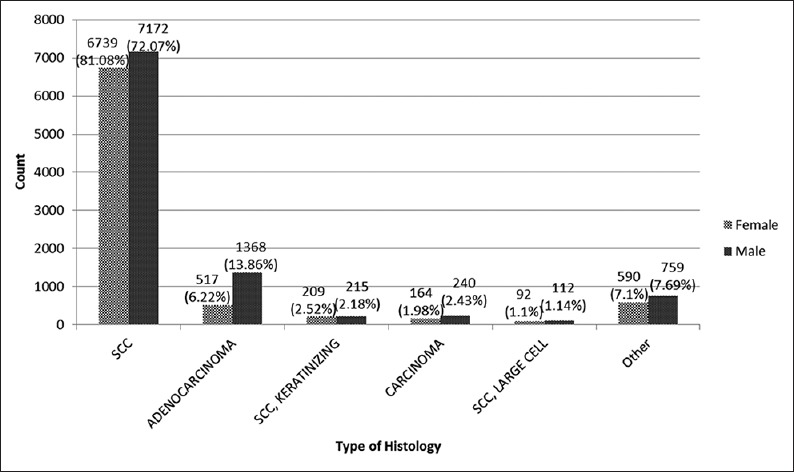
Distribution of histology esophageal cancer in Iran
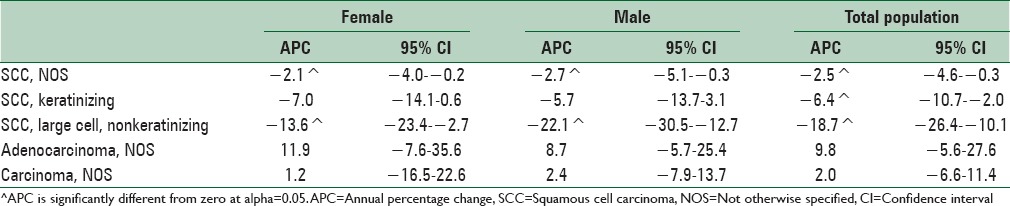
The percentage allocated to histology types of esophageal cancer was not constant during years studied. The percentage allocated for histology of squamous cell carcinoma NOS (SCC), and SCC large cell, and nonkeratinizing had a significant decreasing trend in both sexes (P < 0.05). The decreasing trend was quicker for scc large cell, and nonkeratinizing than SCC. The type of adenocarcinoma NOS increased in both sexes (P < 0.05) [Table 2].
Table 2.
Joinpoint analyses of cancer percentage allocated trend to the histology data for esophageal cancer in Iran (2003-2008)
DISCUSSION
Our study investigated the trend of incidence and pathological changes of esophagus cancer during 2003–2008 in Iran. Our findings showed that there was an increasing trend of esophageal cancer over 6 years. The incidence rate is also higher in men than women. The decreasing trend was quicker for SCC, large cell, and nonkeratinizing than SCC. ADC, NOS had an increasing trend in both sexes.
In this study, most cases were SCC (64.53%) followed by the AD (10.37%). There was a significant decreasing trend for SCC, while AD is significantly increased in both sexes. Incidence of esophageal cancer of AD is rising in many European countries.[9] AD incidence is enhancing in China.[22] In developing countries, including Iran and China, SCC is also the most common, and responsible for nearly 90% of cases.[13] The prevalence of this type of cancer is decreasing in the world. Also SCC type of esophagus cancer is declining, but ADC is increasing in Iran.[14] changes in the epidemiology of esophageal cancer in the world and Iran occurred two to three decades after health promotion and cultural, economic and social development. Obesity and acid reflux from the stomach into the esophagus are possible causes of this cancer.[15,23] In Iran and other developing countries, lifestyle changes and westernization lead to become the incidence of cancer similar to the developed countries.
The reported incidence rate of the cancer was 13.8/100,000 in men and 6.5/100,000 in women in developing countries. In developed countries, the rates were 6.5 and 1.3/100,000 in men and women, respectively.[24] Our results indicated that the rates were 7.56 and 7.77/100,000 in men and women, respectively. No difference was seen between them. Geographical distribution of esophageal cancer is different in Iran. Age-standardized rate (ASR) for women and men was 43.3 and -36.3/100,000, respectively, in the province of Golestan.[25] ASR was 15.4 and 14.4/100,000 in women and men, respectively, in the province of Ardebil.[26] In the province of Semnan, the rate was 11.7 and 8.8/100,000 in women and men, respectively.[27] The lowest in Kerman province rate was 3 and 2.1/100,000 in women and men, respectively.[28] The mentioned regions are the belt for esophageal cancer, especially the North East of Iran. Unlike SCC, with equal prevalence in men and women, male factor is considered an important risk factor for ADC.[29] According to globacan, AD more occurred in most countries in men.[24] Our study revealed that the prevalence of AD was 2.64 times more in men than women. However, the prevalence of SCC was 1.06 times more in men than women.
A number of case–control studies in Iran[30] and India[31] showed that drinking hot tea and coffee increases the risk of esophageal cancer. The results of case–control studies conducted in Golestan showed that drinking too hot has increased the risk of esophageal cancer about 10-fold.[32] Malnutrition and low fruit and vegetable intake increase the risk of SCC.[33] However, scientific evidences have not declared that regular consumption of vegetables and fresh fruits may reduce the risk of SCC.[34] A study performed in high-risk areas (such as Golestan) in Iran revealed that nitrosamine levels in the saliva of population were 4 times more than German population.[13] Poor oral hygiene is associated with the risk of the esophagus and stomach cancers.[35] There is a relationship between oral disease and tooth loss, and higher rates of mouth and stomach cancers. In China,[36] Latin America, Eastern Europe, and Japan, similar to Iran, inadequate oral hygiene was considered as a precursor of esophageal squamous dysplasia.[28]
Strong risk factor for AD may be obesity and the absence of helicobacter pylori infection.[37] Smoking and acid reflux from the stomach into the esophagus increases the risk of AD. Obesity and overweight are other major causes of AD. In the future, this type of esophagus cancer dramatically increases in Iran because of obesity and overweight epidemic associated with acid reflux from the stomach into the esophagus and reducing the amount of helicobacter pylori infection.[1,2]
Improving the cancer registration system may be one of the reasons of increasing the cancer. A study on the trend of skin cancer incidence performed in Italy declared that advances in diagnostic techniques and the development of cancer registration lead to a large proportion of the increase in the incidence of skin cancer.[38]
According to the report of Iranian ministry of health, the cancer registry in the country has increased from 18% in 1998 to 80% in 2005.[39] This may be due to improving the cancer registration system. Hence, in interpreting the results of studies regarding all cancers, the problems and of cancer registration should be considered. In other words, the share of the development of cancer registration and high proportion of the most difficult areas should be distinguished from each other.
The lack of population-based data regarding the prevalence and mortality is one of the major problems in esophageal cancer. In some low-income countries, there are the primary barriers such sanctions and racial and cultural beliefs, except for the diagnosis and effective management of cancer. Researchers believe that advances in cancer treatment, even in countries with limited resources, can helpful because early detection increases the effectiveness of treatment.
CONCLUSIONS
According to this study, the trend of ASIR of esophagus cancer in Iran is rising. Hence to prevent and control this cancer, it is necessary to investigate related risk factors and implement prevention programs in Iran.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. doi: 10.3322/canjclin.55.2.74. [DOI] [PubMed] [Google Scholar]
- 2.Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality, and prevalence across five continents: Defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol. 2006;24:2137–50. doi: 10.1200/JCO.2005.05.2308. [DOI] [PubMed] [Google Scholar]
- 3.Sadjadi A, Nouraie M, Mohagheghi MA, Mousavi-Jarrahi A, Malekezadeh R, Parkin DM. Cancer occurrence in Iran in 2002, an international perspective. Asian Pac J Cancer Prev. 2005;6:359–63. [PubMed] [Google Scholar]
- 4.Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- 5.Rafiemanesh H, Rajaei-Behbahani N, Khani Y, Hosseini S, Pournamdar Z, Mohammadian-Hafshejani A, et al. Incidence trend and epidemiology of common cancers in the center of Iran. Glob J Health Sci. 2015;8:45917. doi: 10.5539/gjhs.v8n3p146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Adami HO, Hunter DJ, Trichopoulos D. USA: Oxford University Press; 2008. Textbook of Cancer Epidemiology. [Google Scholar]
- 7.Almasi Z, Rafiemanesh H, Salehiniya H. Epidemiology characteristics and trends of incidence and morphology of stomach cancer in Iran. Asian Pac J Cancer Prev. 2015;16:2757–61. doi: 10.7314/apjcp.2015.16.7.2757. [DOI] [PubMed] [Google Scholar]
- 8.Razi S, Rafiemanesh H, Ghoncheh M, Khani Y, Salehiniya H. Changing trends of types of skin cancer in Iran. Asian Pac J Cancer Prev. 2015;16:4955–8. doi: 10.7314/apjcp.2015.16.12.4955. [DOI] [PubMed] [Google Scholar]
- 9.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 10.Stathopoulos GP, Tsiaras N. Epidemiology and pathogenesis of esophageal cancer: Management and its controversial results (review) Oncol Rep. 2003;10:449–54. [PubMed] [Google Scholar]
- 11.Yarbro CH, Wujcik D, Gobel BH. USA: Jones and Bartlett Publishers; 2010. Cancer Nursing: Principles and Practice. [Google Scholar]
- 12.Samadi F, Babaei M, Yazdanbod A, Fallah M, Nouraie M, Nasrollahzadeh D, et al. Survival rate of gastric and esophageal cancers in Ardabil province, North-West of Iran. Arch Iran Med. 2007;10:32–7. [PubMed] [Google Scholar]
- 13.Kamangar F, Malekzadeh R, Dawsey SM, Saidi F. Esophageal cancer in Northeastern Iran: A review. Arch Iran Med. 2007;10:70–82. [PubMed] [Google Scholar]
- 14.Haghdoost AA, Hosseini H, Chamani G, Zarei MR, Rad M, Hashemipoor M, et al. Rising incidence of adenocarcinoma of the esophagus in Kerman, Iran. Arch Iran Med. 2008;11:364–70. [PubMed] [Google Scholar]
- 15.Malekzadeh R, Mohamadnejad M, Merat S, Pourshams A, Etemadi A. Obesity pandemic: An Iranian perspective. Arch Iran Med. 2005;8:1–7. [Google Scholar]
- 16.Keyghobadi N, Rafiemanesh H, Mohammadian-Hafshejani A, Enayatrad M, Salehiniya H. Epidemiology and trend of cancers in the province of Kerman: Southeast of Iran. Asian Pac J Cancer Prev. 2015;16:1409–13. doi: 10.7314/apjcp.2015.16.4.1409. [DOI] [PubMed] [Google Scholar]
- 17.Goya M. Iranian Annual Cancer Registration Report 2005/2006. Ministry of Health and Medical Education, Health Deputy. Center for Disease Control and Prevention. 2007 [Google Scholar]
- 18.Razi S, Enayatrad M, Mohammadian-Hafshejani A, Salehiniya H, Fathali-Loy-Dizaji M, Soltani S. The epidemiology of skin cancer and its trend in Iran. Int J Prev Med. 2015;6:64. doi: 10.4103/2008-7802.161074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin L, Parkin DM, et al. Geneva: WHO; 2000. International classification of diseases for oncology: ICD-O. [Google Scholar]
- 20.Enayatrad M, Amoori N, Salehiniya H. Epidemiology and trends in breast cancer mortality in Iran. Iran J Public Health. 2015;44:430–1. [PMC free article] [PubMed] [Google Scholar]
- 21.Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19:335–51. doi: 10.1002/(sici)1097-0258(20000215)19:3<335::aid-sim336>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 22.Zhang H, Chen SH, Li YM. Epidemiological investigation of esophageal carcinoma. World J Gastroenterol. 2004;10:1834–5. doi: 10.3748/wjg.v10.i12.1834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Malekzadeh R, Nasseri-Moghaddam S, Sotoudeh M. Gastroesophageal reflux disease: The new epidemic. Arch Iran Med. 2003;6:127–40. [Google Scholar]
- 24.Crew KD, Neugut AI, editors Epidemiology of upper gastrointestinal malignancies. Seminars in Oncology. WB Saunders: Elsevier. 2004;31:450–64. doi: 10.1053/j.seminoncol.2004.04.021. [DOI] [PubMed] [Google Scholar]
- 25.Semnani S, Sadjadi A, Fahimi S, Nouraie M, Naeimi M, Kabir J, et al. Declining incidence of esophageal cancer in the Turkmen Plain, Eastern part of the Caspian Littoral of Iran: A retrospective cancer surveillance. Cancer Detect Prev. 2006;30:14–9. doi: 10.1016/j.cdp.2005.11.002. [DOI] [PubMed] [Google Scholar]
- 26.Sadjadi A, Malekzadeh R, Derakhshan MH, Sepehr A, Nouraie M, Sotoudeh M, et al. Cancer occurrence in Ardabil: Results of a population-based cancer registry from Iran. Int J Cancer. 2003;107:113–8. doi: 10.1002/ijc.11359. [DOI] [PubMed] [Google Scholar]
- 27.Babaei M, Mousavi S, Malek M, Tosi G, Masoumeh Z, Danaei N, et al. Cancer occurrence in Semnan province, Iran: Results of a population-based cancer registry. Asian Pac J Cancer Prev. 2005;6:159–64. [PubMed] [Google Scholar]
- 28.Sadjadi A, Zahedi M, Nouraie M, Alimohammadian M, Ghorbani A, Bahmanyar S, et al. The first population-based cancer survey in Kerman Province of Iran. Iran J Public Health. 2007;36:26–34. [Google Scholar]
- 29.Derakhshan MH, Malekzadeh R, Watabe H, Yazdanbod A, Fyfe V, Kazemi A, et al. Combination of gastric atrophy, reflux symptoms and histological subtype indicates two distinct aetiologies of gastric cardia cancer. Gut. 2008;57:298–305. doi: 10.1136/gut.2007.137364. [DOI] [PubMed] [Google Scholar]
- 30.Cook-Mozaffari PJ, Azordegan F, Day NE, Ressicaud A, Sabai C, Aramesh B. Oesophageal cancer studies in the Caspian Littoral of Iran: Results of a case-control study. Br J Cancer. 1979;39:293–309. doi: 10.1038/bjc.1979.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ganesh B, Talole SD, Dikshit R. Tobacco, alcohol and tea drinking as risk factors for esophageal cancer: A case-control study from Mumbai, India. Cancer Epidemiol. 2009;33:431–4. doi: 10.1016/j.canep.2009.09.002. [DOI] [PubMed] [Google Scholar]
- 32.Islami F, Pourshams A, Nasrollahzadeh D, Kamangar F, Fahimi S, Shakeri R, et al. Tea drinking habits and oesophageal cancer in a high risk area in Northern Iran: Population based case-control study. BMJ. 2009;338:b929. doi: 10.1136/bmj.b929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.González CA, Pera G, Agudo A, Bueno-de-Mesquita HB, Ceroti M, Boeing H, et al. Fruit and vegetable intake and the risk of stomach and oesophagus adenocarcinoma in the European Prospective Investigation into Cancer and Nutrition (EPIC-EURGAST) Int J Cancer. 2006;118:2559–66. doi: 10.1002/ijc.21678. [DOI] [PubMed] [Google Scholar]
- 34.Riboli E, Norat T. Epidemiologic evidence of the protective effect of fruit and vegetables on cancer risk. Am J Clin Nutr. 2003;78:559S–69S. doi: 10.1093/ajcn/78.3.559S. [DOI] [PubMed] [Google Scholar]
- 35.Abnet CC, Kamangar F, Dawsey SM, Stolzenberg-Solomon RZ, Albanes D, Pietinen P, et al. Tooth loss is associated with increased risk of gastric non-cardia adenocarcinoma in a cohort of Finnish smokers. Scand J Gastroenterol. 2005;40:681–7. doi: 10.1080/00365520510015430. [DOI] [PubMed] [Google Scholar]
- 36.Akbari MR, Malekzadeh R, Nasrollahzadeh D, Amanian D, Islami F, Li S, et al. Germline BRCA2 mutations and the risk of esophageal squamous cell carcinoma. Oncogene. 2008;27:1290–6. doi: 10.1038/sj.onc.1210739. [DOI] [PubMed] [Google Scholar]
- 37.Lagergren J. Adenocarcinoma of oesophagus: What exactly is the size of the problem and who is at risk? Gut. 2005;54(Suppl 1):i1–5. doi: 10.1136/gut.2004.041517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Mousavi SM, Gouya MM, Ramazani R, Davanlou M, Hajsadeghi N, Seddighi Z. Cancer incidence and mortality in Iran. Ann Oncol. 2009;20:556–63. doi: 10.1093/annonc/mdn642. [DOI] [PubMed] [Google Scholar]
- 39.Sadjadi A, Semnani S, Nouraie SM, Khademi H, Bahadori M. Cancer registry in Iran: A brief overview. Arch Iran Med. 2008;11:577. [PubMed] [Google Scholar]