

Abstract
Background:
Hand eczema is one of the commonest eczemas encountered in dermatology practice. Contact allergens responsible for causing hand eczema vary from one geographical area of the world to another. Aim: The study tries to identify the commonest allergens causing hand eczema in ethnic Kashmiri population.
Material and Methods:
A total of 800 patients were patch tested at a sole patch testing facility for the local population over a 7-year period out of which 278 were diagnosed with hand eczema. The morphological type of hand eczema was noted and the patch testing results were analyzed. Past or present relevance of the patch-test result to the clinical diagnosis was also analyzed.
Results:
Hand eczema was the most common type of eczema patch tested over the 7-year period, constituting 34.75% of the patch-tested population. A positive patch-test result was obtained in 135 patients (48.5%) out of which it was found to be clinically relevant in about 65% cases. Nickel and potassium dichromate were found to be the two commonest allergens causing hand eczema in our population with positive patch test reactions in 45 and 27 patients respectively. Females showed a much higher incidence of hand eczema as well as higher patch test positivity than males (54.1% vs. 38.1%).
Conclusions:
Hand eczema with a positive patch-test report was found to be much more common in females than males and nickel and potassium dichromate were seen to be the commonest allergens causing hand eczema in ethnic Kashmiri population.
Keywords: Contact allergens, hand eczema, Kashmir valley, patch test
Introduction
What was known?
Hand eczema is one of the commonest eczemas encountered in clinical practice
Hand eczema is the commonest eczema encountered in patch test clinics outside India but in India footwear dermatitis and airborne contact dermatitis predominates
Male predominance is seen in hand eczema and chromate, fragrance mix and Nickel are commonest allergens seen in these cases.
Hand eczema is one of the commonest types of eczema encountered in dermatological practice.[1,2] The condition is associated with a lot of physical and psychological morbidity. Hand eczema is usually a chronic and recurring disorder with a prevalence of about 8% in adult population.[3]
Classification of hand eczema is done either on the basis of morphology or the etiological factors associated with it. Morphologically, hand eczema is divided into many types, the commonest of which are fingertip eczema, hyperkeratotic eczema, apron eczema, ring eczema and pompholyx. On the etiological front hand eczemas are classified into endogenous and exogenous eczemas with further subdivisions. A number of endogenous and exogenous factors play a role in the development of hand eczema. Atopy is the most important of the endogenous factors and among exogenous factors, contact sensitization to different allergens, either occupational or nonoccupational is the most important.[4,5] While contact sensitization is the primary cause of hand eczema in 20–60% cases, it also plays a crucial role in aggravation of other types of hand eczema.[5,6] That is the reason why patch testing is considered mandatory in all those patients in whom hand eczema persists for more than 1 month.[6]
Results obtained from a patch test have to be interpreted in a proper manner in patients with hand eczema. The most important part of this interpretation is the assessment of the relevance of patch test result with clinical condition. Only after assessing the relevance of the patch test result can a proper advice be given and thus the benefit of the test can be passed on to the patient. We are reporting hereby the results of patch testing in hand eczema patients over a period of 7 years in ethnic Kashmiri population.
Material and Methods
A total of 800 patients were seen at the contact dermatitis clinic of our institute from May 2006 to May 2013 out of which 278 patients had a primary diagnosis of hand eczema. The demographic profile and clinical details were filled in a preformed format at the first visit of each of these patients. These demographic details included the age, sex, occupation, rural/urban residence, hobbies and other daily activities of each patient. Clinical evaluation of the patients included the morphological type of eczema, the sites involved, the duration of eczema, the seasonal and photo-exposure related variation and any coexistent skin disorders including atopic diathesis.
All the patients were patch-tested using the Indian standard series as recommended by the Contact and Occupational Dermatosis Forum of India and marketed by Systopic Labs India Ltd. A standard protocol was employed in each patient wherein the test antigens were applied on the upper back in a prefixed pattern using aluminium patch-test chambers mounted on a micropore tape. The test patches were removed after 2 days and the sites were marked with a permanent marker pen. Readings were taken 15–30 min after removing the test patches on day 2 and then again on day 4 as well. The reactions were interpreted according to the International Contact Dermatitis Research Group criteria and graded accordingly. The patients were also told to report if there were any further reactions at the patch-test area on day 7.
After grading the test reactions, the relevance of the patch test report was analyzed by a thorough evaluation of the patient's clinical and exposure history and the details were added to the patient's data. The chronological association of the eczema and exposure to the probable allergen on the basis of patch test report was assessed and the relevance was thus reported as “present relevance,” “past relevance” or “probable relevance.”
Results
Almost all age groups were represented in the study group with our youngest patient being just 12-year-old while the oldest patient having an age of 56 years. Majority of the patients, however, belonged to 3rd and 4th decade of their life.
Female sex was preponderant and in the 278 patients tested in the present study, 171 were females representing approximately 62% of the whole group [Table 1].
Table 1.
Patient profile
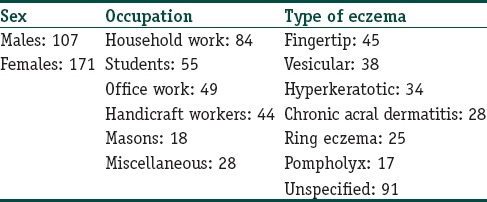
The commonest occupation group represented was housewives followed by manual workers, students, masons and office workers [Table 1]. Masons constituted about 17% of the male population in this study (18 out of 107 males).
The commonest morphological types of hand eczema seen were the finger-tip eczema, vesicular hand eczema and hyperkeratotic hand eczema in 45, 38 and 34 patients respectively [Figure 1]. Other morphological patterns of hand eczema seen were chronic acral dermatitis, ring eczema and pompholyx in 28, 25 and 17 patients respectively. In the remaining 91 patients (32.7%), the hand eczema could not be classified into any particular morphological type [Table 1].
Figure 1.

Hand eczema in a mason with chromate sensitivity
Atopic diathesis was not clinically evident in majority of the study population and only 11 patients had clinical features suggestive of atopy. All these atopic subjects had either pompholyx or hyperkaratotic pattern of eczema.
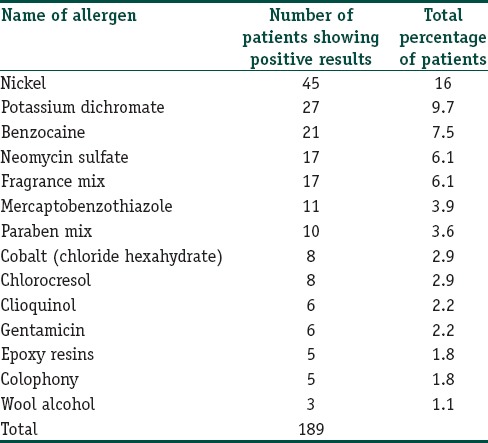
A positive patch-test report was obtained in 135 patients out of the total of 278 patients tested. Out of these, 97 patients showed a positive reaction to a single patch-test antigen while 38 others showed positive patch test reactions to multiple (2 or more) antigens. Thus, a total of 189 positive reactions were recorded in the study group.
Nickel and potassium dichromate were found to be the two commonest allergens in the study population with positive reactions in 45 and 27 patients respectively. Thus, nickel and potassium dichromate together accounted for about 38% of the total positive test reactions. Other common allergens found in our population included benzocaine, neomycin, fragrance mix, mercaptobenzothiazole and paraben mix in 21, 17, 17, 11 and 10 patients respectively. Other allergens found positive in the study population are as given in Table 2.
Table 2.
Contact allergen positivity in patients with hand eczema
Females were seen to show higher patch-test positivity then males. Out of a total of 171 females, a positive patch-test was seen in 94 (54.9%) patients while only 41 out of the107 males (38.3%) showed a positive patch test reaction. The commonest allergen found in female patients was nickel (in 35 patients) while in males, highest number of positive reactions were seen with potassium dichromate, nickel and fragrance mix in 14, 10 and 8 patients respectively.
The positive test reactions were analyzed for their clinical relevance and majority of these reactions were found to be clinically relevant. In fact, a total of 122 reactions out of 189 (64.5%) had either a present or past relevance to the clinical picture. The highest clinical relevance was seen in patients with metal sensitivity. In patients with chromate sensitivity, occupational exposure to relevant substances was seen in 14 patients (all masons) while 9 others had a nonoccupational exposure. Thus the overall relevance of this subgroup was about 80% (23 out of 27 patients). In patients with metal allergy on patch testing, clinical relevance was evident in 77.7% patients out of whom 35.5% had relevance to the current dermatitis while 42.2% others had a past relevance in the form of a past exposure to metallic substances especially in females in the form of ear piercing.
A peculiar finding that we observed in our patients was the simultaneous involvement of hands and lips in many patients with the primary diagnosis of hand eczema. These patients were seen to be predominantly sensitive to nickel and the involvement of lips was probably because of the use of metallic spoons for taking rice based diet which is the staple diet for ethnic Kashmiri population. However, dimethylglyoxamine test was not done to prove this association.
Discussion
Kashmir valley is a province of Jammu and Kashmir state with a temperate climate and it has a population of about 7 million with a unique ethnic character. A good proportion of the adult population in the valley is involved with agriculture, horticulture and handicraft sectors. The custom of ear-piercing is almost universal in females in this population. This custom is completed in early childhood in most of the females and by the age of 10 years almost all females are through with this procedure. Additionally, the female population is also almost universally involved with cooking meals at home and in the villages these females are also involved with gardening and farming practices.
Our institute was the first to start a patch testing facility in the valley about 8 years back and we have been able to patch test about 800 individuals belonging to the ethnic Kashmiri population till date. We found “hand eczema” to be quite common in this population and in fact, it formed the commonest diagnosis in patients who underwent patch testing at our institute. This finding is in conformity with many similar studies from different parts of the world.[7,8,9] On the other hand, in Indian context, footwear dermatitis and air-borne contact dermatitis are the two commonest eczemas seen in patch-tested patients.[10,11] The high incidence of hand eczema in our patch-tested population, in fact, formed the basis of conducting this study as we tried to figure out the reasons behind this high incidence and the allergens responsible for it in this population. We patch-tested all population and occupational groups and the study population included students, office-goers, handicraft workers, housewives, farmers and other occupational groups as well.
About 48.5% of hand eczema patients that we patch tested showed one or more positive reactions in this study. This figure is comparable to those quoted by most of the studies especially on this subject.[12,13,14] We found hand eczema to be more common in our female population than males. This is probably because of a much higher incidence of nickel sensitivity in our female population. In fact, nickel proved to be the predominant allergen causing hand eczema in females irrespective of their occupational status. All this can be easily explained on the basis of the universal practice of ear-piercing in our female population. The custom of wearing jewellery especially on religious festivals and marriage ceremonies adds to the chances of developing a nickel-sensitivity in this population subgroup. Additionally, the earthen-ware that was used commonly for cooking purposes in the past has been replaced totally by steel utensils over the last 2-3 decades.
In males the patch test results were mixed as there was no single predominant allergen and potassium dichromate, para-phenylenediamine and fragrance mix were the commonest allergens in this sub-group. Additionally, males showed a significantly less incidence of positive reactions to the patch-test allergens than females, a phenomenon that has been reported in many studies till date.[15,16] This sex-disparity has been explained on the basis of a relatively much higher rate of nickel sensitivity in females and this was evident in our series as well.[16]
Among topical antimicrobials neomycin was the commonest allergen with 17 patients (6.1%) showing a positive reaction to this compound. In all these patients, there was a history of using topical antimicrobial combinations and thus the patch test result had a strong clinical relevance in all of them. The importance of gentamicin and neomycin emerging as common sensitizers has been stressed upon in many studies from India and abroad.[16,17,18]
Eight of our patients with hand eczema tested positive for chlorocresol. This allergen, in addition to being a constituent of many cosmetic products, cross reacts with chloroxylenol, an active ingredient of “Dettol,” the use of which has increased dramatically in recent years.[19] An interesting fact that we observed in our patients was that there was a tendency to switch over to “Dettol soap” or at least add “Dettol” solution to bath water as the first measure to tackle any dermatitis.
Conclusions
Hand eczema is more common in females than males in ethnic Kashmiri population and females also show a higher rate of patch test positivity in this population. Nickel and potassium dichromate constitute the two commonest allergens responsible for hand eczema, nickel being especially common in females.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
What is new?
Hand eczema is the commonest eczema seen in a patch test clinic in Kashmir valley
Females predominate and even show more patch test positivity in Kashmiri patients with hand eczema
Nickel is the commonest allergen followed by potassium dichromate in these cases.
References
- 1.Albert MR, González S, González E. Patch testing reactions to a standard series in 608 patients tested from 1990 to 1997 at Massachusetts General Hospital. Am J Contact Dermat. 1998;9:207–11. [PubMed] [Google Scholar]
- 2.al-Sheikh OA, Gad el-Rab MO. Allergic contact dermatitis: Clinical features and profile of sensitizing allergens in Riyadh, Saudi Arabia. Int J Dermatol. 1996;35:493–7. doi: 10.1111/j.1365-4362.1996.tb01664.x. [DOI] [PubMed] [Google Scholar]
- 3.Meding B, Lidén C, Berglind N. Self-diagnosed dermatitis in adults. Results from a population survey in Stockholm. Contact Dermatitis. 2001;45:341–5. doi: 10.1034/j.1600-0536.2001.450604.x. [DOI] [PubMed] [Google Scholar]
- 4.Agner T, Andersen KE, Brandao FM, Bruynzeel DP, Bruze M, Frosch P, et al. Contact sensitisation in hand eczema patients-relation to subdiagnosis, severity and quality of life: A multi-centre study. Contact Dermatitis. 2009;61:291–6. doi: 10.1111/j.1600-0536.2009.01630.x. [DOI] [PubMed] [Google Scholar]
- 5.Lerbaek A, Kyvik KO, Ravn H, Menné T, Agner T. Clinical characteristics and consequences of hand eczema - An 8-year follow-up study of a population-based twin cohort. Contact Dermatitis. 2008;58:210–6. doi: 10.1111/j.1600-0536.2007.01305.x. [DOI] [PubMed] [Google Scholar]
- 6.Rietschel RL, Fowler JF., Jr . Fisher's Contact Dermatitis. 5th ed. Philadelphia: Lippincott Williams and Wilkins; 2001. Hand dermatitis due to contactants: Special considerations; pp. 261–78. [Google Scholar]
- 7.Holness DL, Nethercott JR, Adams RM, Belsito D, Deleo V, Emmett EA, et al. Concomitant positive patch test results with standard screening tray in North America 1985-1989. Contact Dermatitis. 1995;32:289–92. doi: 10.1111/j.1600-0536.1995.tb00783.x. [DOI] [PubMed] [Google Scholar]
- 8.Marks JG, Belsito DV, DeLeo VA, Fowler JF, Jr, Fransway AF, Maibach HI, et al. North American Contact Dermatitis Group patch test results for the detection of delayed-type hypersensitivity to topical allergens. J Am Acad Dermatol. 1998;38:911–8. doi: 10.1016/s0190-9622(98)70587-0. [DOI] [PubMed] [Google Scholar]
- 9.Meding B, Järvholm B. Hand eczema in Swedish adults: Changes in prevalence between 1983 and 1996. J Invest Dermatol. 2002;118:719–23. doi: 10.1046/j.1523-1747.2002.01718.x. [DOI] [PubMed] [Google Scholar]
- 10.Sharma VK, Sethuraman G, Garg T, Verma KK, Ramam M. Patch testing with the Indian standard series in New Delhi. Contact Dermatitis. 2004;51:319–21. doi: 10.1111/j.0105-1873.2004.0459k.x. [DOI] [PubMed] [Google Scholar]
- 11.Singhal V, Reddy BS. Common contact sensitizers in Delhi. J Dermatol. 2000;27:440–5. doi: 10.1111/j.1346-8138.2000.tb02202.x. [DOI] [PubMed] [Google Scholar]
- 12.Li LF, Wang J. Contact hypersensitivity in hand dermatitis. Contact Dermatitis. 2002;47:206–9. doi: 10.1034/j.1600-0536.2002.470403.x. [DOI] [PubMed] [Google Scholar]
- 13.Kishore NB, Belliappa AD, Shetty NJ, Sukumar D, Ravi S. Hand eczema: Clinical patterns and role of patch testing. Indian J Dermatol Venereol Leprol. 2005;71:207–8. doi: 10.4103/0378-6323.16244. [DOI] [PubMed] [Google Scholar]
- 14.Suman M, Reddy BS. Pattern of contact sensitivity in Indian patients with hand eczema. J Dermatol. 2003;30:649–54. doi: 10.1111/j.1346-8138.2003.tb00453.x. [DOI] [PubMed] [Google Scholar]
- 15.Hammershøy O. Standard patch test results in 3,225 consecutive Danish patients from 1973 to 1977. Contact Dermatitis. 1980;6:263–8. doi: 10.1111/j.1600-0536.1980.tb04927.x. [DOI] [PubMed] [Google Scholar]
- 16.Bajaj AK, Saraswat A, Mukhija G, Rastogi S, Yadav S. Patch testing experience with 1000 patients. Indian J Dermatol Venereol Leprol. 2007;73:313–8. doi: 10.4103/0378-6323.34008. [DOI] [PubMed] [Google Scholar]
- 17.Shenoi DS, Srinivas CR, Balachandran C. Results of patch testing with a standard series of allergens at Manipal. Indian J Dermatol Venereol Leprol. 1994;60:133–5. [Google Scholar]
- 18.Morris SD, Rycroft RJ, White IR, Wakelin SH, McFadden JP. Comparative frequency of patch test reactions to topical antibiotics. Br J Dermatol. 2002;146:1047–51. doi: 10.1046/j.1365-2133.2002.04662.x. [DOI] [PubMed] [Google Scholar]
- 19.Burry JN, Kirk J, Reid J, Turner T. Chlorocresol sensitivity. Contact Dermatitis. 1975;1:41–2. doi: 10.1111/j.1600-0536.1975.tb05309.x. [DOI] [PubMed] [Google Scholar]