

Abstract
Since physical inactivity especially prevails during winter months, we set out to identify outdoor alternatives to indoor cycling (IC) by comparing the metabolic and cardiorespiratory responses during alpine skiing (AS), cross-country skiing (XCS) and IC and analyse the effects of sex, age and fitness level in this comparison. Twenty one healthy subjects performed alpine skiing (AS), cross-country skiing (XCS), and IC. Oxygen uptake (VO2), total energy expenditure (EE), heart rate (HR), lactate, blood glucose and rate of perceived exertion (RPE) were determined during three 4-min stages of low, moderate and high intensity. During XCS and IC VO2max and EE were higher than during AS. At least 2½ hours of AS are necessary to reach the same EE as during one hour of XCS or IC. HR, VO2, lactate, and RPEarms were highest during XCS, whereas RPEwhole-body was similar and RPElegs lower than during AS and IC, respectively. Weight adjusted VO2 and EE were higher in men than in women while fitness level had no effect. Male, fit and young participants were able to increase their EE and VO2 values more pronounced. Both AS and XCS can be individually tailored to serve as alternatives to IC and may thus help to overcome the winter activity deficit. XCS was found to be the most effective activity for generating a high EE and VO2 while AS was the most demanding activity for the legs.
Key points.
During cross-country skiing and indoor cycling VO2max and energy expenditure were higher than during alpine skiing
Approximately 2½ hours of alpine skiing are necessary to reach the same energy expenditure of one hour of cross-country skiing or indoor cycling.
Alpine skiing and cross-country skiing can be individually tailored to serve as sports alternatives in winter to activity deficit.
By applying different skiing modes as parallel ski steering, carving long radii and short turn skiing, metabolic and cardiorespiratory response can be increased during alpine skiing.
Male, fit and young participants were able to increase their energy expenditure and VO2 more pronounced with an increase in intensity compared with their counterparts
Key words: Borg, blood lactate, cross-country skiing, cycling, energy expenditure, fitness level, oxygen uptake, gender
Introduction
During the winter season the frequency of participating in physical activity and the total daily energy expenditure has been shown to be reduced when compared with the summer months (Dannenberg et al., 1989, Merchant et al., 2007). Furthermore, blood pressure, cholesterol and body mass index tend to increase in all age groups and both sexes during winter months, leading to an increasing risk of chronic coronary disease and cardiac events (Ulmer et al., 2004). Physical inactivity is one of the main modifiable risk factors of cardiovascular diseases and has been reported to be as deleterious as tobacco smoking (Mendis et al., 2011). Therefore, there is a need to identify modes of exercise and sports that are attractive to the wider population with the potential to maintain if not even increase physical fitness during winter.
Indoor cycling (IC) might be regarded as the gold standard for physical training with no seasonal limitations and its feasibility for different target groups, i.e. those without access to mountains and snow or injuries and chronic disease that preclude them from participation in winter sports. Alpine and Nordic sports have a long standing tradition in alpine and Scandinavian countries. More than one third of all Austrians (~7.6 Million in the year 1986) think that alpine skiing (AS) is the best way to experience nature and freedom in the winter months (Bachleitner, 1998). AS has become the most popular winter sport world-wide, with more than eight million skiers visiting Austria each year (Burtscher et al., 2000). Alpine skiing is a leisure sport where gravity is the driving force and the work needed to raise the potential energy for the next downhill is provided by the chairlift not the skier as i.e. during alpine touring skiing or cross-country skiing (XCS). It is open to debate whether AS might provide sufficient cardiovascular and metabolic stimuli to achieve fitness gains. In the past few years, recent investigations have shown that AS is a suitable and safe recreational sport for an elderly and sedentary population (Kahn et al., 1993; Krautgasser et al., 2011; Müller et al., 2011; Pötzelsberger et al., 2015; Scheiber et al., 2009; 2012). However, Karlsson et al. (1978) listed some limitations for recreational skiers not being able to reach high intensities during skiing due to poor technique and strength when compared with professional skiers. While there are several studies that discuss the physiological response during XCS in general (e.g. Mygind et al., 1991, Mognoni et al., 2001, Welde et al., 2003, Larsson and Henriksson-Larsen, 2008), research about the effects of fitness level on physiological response during XCS or IC is missing.
Cross-country skiing can be regarded as the gold standard winter time aerobic exercise mode, with a high percentage of muscles in the whole body being activated (Rusko, 2008, Björklund et al., 2015, Stöggl et al., 2013, Björklund et al., 2010), and the highest VO2max values among all sports being measured in world class XCS athletes (Holmberg et al., 2007, Rusko, 2008, Saltin and Astrand, 1967). It is not known if AS can be used as an alternative to XCS and/or IC to fill the winter gap of physical activity and provide an alternative to indoor training.
There are many studies that have analyzed the physiological responses of AS, XCS and IC separately (e.g., Bergh, 1982; Hoffman, 1992; Holmberg, 2005; Impellizzeri and Marcora, 2007; Mujika and Padilla, 2001; Kahn et al., 1993; Krautgasser et al., 2011; Müller et al., 2011; Pötzelsberger et al., 2015; Scheiber et al., 2009; Vogt et al., 2005). However to the best of our knowledge, no direct comparisons within the same subjects were done while performing AS, XCS as well as IC. In addition, most of the previous studies included well-trained if not elite athletes, which is not representative of the common population. Furthermore, data about energy expenditure (EE) and MET values during AS are solely provided during the downhill phase (Ainsworth et al., 2011, Vogt et al., 2005) representing not a measure with sufficient external validity based on recovery periods while standing in line, taking a lift and short breaks during skiing of up to 67% of total skiing time (Müller et al., 2011). And lastly, sex, fitness and age aspects were largely neglected; and interactions of the above mentioned factors with exercise intensity and exercise mode (here IC vs. XCS vs. AS) are missing. Recently we have provided a first outline about the cardiorespiratory and metabolic response with AS, XCS and IC (Stöggl et al., 2015), however the detailed effects of exercise intensity, sex, age, fitness level and its interactions are open to be discussed. Therefore, in the current study we set out to 1) compare the metabolic and cardiorespiratory responses as well as rates of perceived exertion during AS to XCS and IC, 2) analyze the effects of gender, age and fitness level and its interaction with exercise intensity and exercise mode in this comparison, and 3) translate the duration of an AS session into isocaloric training sessions of XCS and IC.
Methods
Participants
Twenty-one volunteers were selected and included in this study according to the following criteria: written informed consent; >30 years; no abnormalities in the electrocardiogram (ECG); non-smoker for at least one year; proficiency in AS and XCS (>10 days of AS and XCS per season); no medical conditions which would conflict with participation in maximal indoor and outdoor exercise tests; no intake of anticoagulants including aspirin; no alcohol or drug abuse; and no severe obesity (BMI>40). Participants’ characteristics are presented in Table 1. Participants were stratified according to age (two age groups delineated by the median in age; Young: n = 11, age = 38 ± 4 yrs; Old: n = 10, age = 60 ± 6 yrs), fitness level (two levels according to relative VO2max; Fit: n = 11, age = 40 ± 7 yrs, VO2max = 49.2 ± 10.8 ml·kg-1·min-1; Unfit: n = 10, age = 54 ± 12 yrs, VO2max = 29.3 ± 7.8 ml·kg-1·min-1) and sex. The study received approval from the Ethical Committee and was conducted in accordance with the Declaration of Helsinki. This study is registered and published at ClinicalTrials.gov: NCT02082106.
Table 1.
Characteristics of participants without dropouts at baseline examination. Data are means (±SE).
| Overall (n = 19) | Male (n = 12) | Female (n = 7) | |
|---|---|---|---|
| Age (years) | 47.6 (12.4) | 46.9 (12.0) | 48.9 (13.9) |
| Weight (kg) | 80.9 (14.5) | 85.3 (12.4) | 73.2 (15.6) |
| Height (m) | 1.76 (.09) | 1.80 (.07) | 1.68 (.08) |
| BMI (kg·m-²) | 26.2 (4.5) | 26.3 (3.5) | 26.1 (6.2) |
| Pmax (W) | 252.5 (93.7) | 299.3 (82.9) | 172.3 (43.1) |
| relPmax (W·kg-1) | 3.2 (1.2) | 3.6 (1.2) | 2.5 (.9) |
| HRmax (bpm) | 172(17) | 171(18) | 173(16) |
| VO2max (ml·kg-1·min-1) | 39.5 (12.9) | 44.2 (12.3) | 31.5 (10.3) |
| FEV1 (L) | 3.7 (.9) | 4.2 (.5) | 2.9 (.8) |
| FEV1/FVC (%) | 76.7 (6.3) | 78.7 (5.3) | 73.4 (6.9) |
| HDL (mg·dL-1) | 75.4 (22.7) | 67.2 (19.7) | 89.6 (21.5) |
| LDL (mg·dL-1) | 118.2 (31.0) | 122.3 (24.8) | 111.0 (40.8) |
| CHOL (mg·dL-1) | 218.2 (40.7) | 218.6 (22.8) | 217.6 (63.5) |
| CK (U·L-1) | 157.3 (105.8) | 175.8 (106.1) | 125.4 (105.2) |
BMI, body mass index; HRmax, maximal heart rate; Pmax, maximal power output; relPmax, relative maximal power output (per kg body weight); VO2max, relative maximal oxygen consumption (per kg body weight); FEV1, forced expiratory volume in the first second; CHOL, cholesterin; CK, creatinekinase; FVC, forced vital capacity; L/HDL, low/high density lipoprotein.
Overall design
The study was carried out during the winter months from January to March. Following the recruiting process every participant underwent a complete medical examination and a cycle ergometry ramp protocol until volitional exhaustion, all completed by a physician. Those who met all inclusion criteria performed an AS, XCS, and IC session in randomized order on three separate days with a minimum of 48 hours in between. During each session oxygen uptake (VO2), heart rate (HR), blood lactate, rating of perceived exertion (RPE, BORG scale: 6-20) for the whole body (RPEwhole-body), legs only (RPElegs) and arms only (RPEarms), and kinematic data of skiing (velocities, altitude meters, covered distances) were recorded. Each session commenced with a 10-min rest period, followed by 5 min of warm-up, three 4-min stages of low (LOW), moderate (MOD) and high (HIGH) intensity and a 10-min resting period at the end of HIGH for determination of excess post exercise O2 consumption (EPOC). For standardization purposes food intake was not permitted 4 h prior to testing, and participants were instructed not to change their diet and amount of physical activity throughout the examination period.
Baseline medical examination and VO2max ramp test
Baseline examinations (see Table 1) included completion of two questionnaires about physical activity (IPAQ) and training/competition history, routine blood analysis in a fasting state, determination of body mass, lung function testing (EasyOne, Medizintechnik, Switzerland), and an incremental cycling ergometry to volitional exhaustion (Ergoselect 200, Ergoline GmbH, Bitz, Germany) to assess maximal power output (Pmax), VO2max, HRmax and peak lactate. The testing protocol was adapted to sex and estimated physical fitness: for females, start: 50 W; increment: 15 W every 1 min; for unfit males, start: 50 W; increment: 20 W every 1 min; and for fit males, start: 50 W; increment: 25 W every 1 min (categorization for fit or unfit was based on the questionnaire data). HR (12-lead-ECG stress test system; Amedtec, Aue, Germany) and breath-by-breath spirometric data (MasterScreen CPX, Carl Reiner GmbH, Wien, Austria) were recorded continuously. The flow of the turbine was measured with the integrated automatic volume calibration program of the ergospirometry system. Gas calibration was performed with the automatic gas analyzer calibration procedure using standardized oxygen (16.00 vol %) and carbon dioxide (5.01 vol %) concentrations (rest volume: nitrogen). Both calibration procedures were performed directly before each test. A 15 s moving average was used for all cardiorespiratory data. Lactate as well as blood pressure was measured every two minutes, as well as three and five minutes after the completion of the test. For lactate analysis, a 20 µl blood sample from the earlobe was collected immediately after each second increment and quantified amperometric-enzymatically (Biosen S-Line Lab+, EKF-diagnostic GmbH, Magdeburg, Germany). The lactate sensor was calibrated before each test using a lactate standard sample of 12 mmol·L-1. Results within a range of ±0.1 mmol·L-1 were accepted.
Outdoor trials
Participants’ HR and GPS data (distance, skiing speed and altitude) were recorded by telemetry (Suunto Ambit 2.0, Helsinki, Finland) sampling at 1-s intervals. For altitude calculations automated barometric measurements and GPS data were used. VO2 was continuously recorded by a portable breath-by-breath spirometer (K4b2, Cosmed, Rome, Italy). For determination of lactate and blood glucose (see above) a sample was collected immediately after each intensity stage, as well as three, five and 10 minutes after the completion of the HIGH intensity stage during the EPOC phase.
Alpine skiing trials
Alpine skiing trials were performed on a slope with sufficient width (~50 m) and homogenous grade, allowing steady skiing of 4 min (~1.6 km with ~490 m altitude change, 17-18° grade). Each intensity trial was done in one separate descent. For LOW, the parallel ski steering (PSS) technique was used which is characterized by sliding on the ski-edges during each swing while skis are being kept in parallel position. For MOD, carving with long radii (CLR) was performed where the skier carves on the ski-edges avoiding skidding, trying to ski a full 180° curve each swing. HIGH was done using short turn skiing (ST) which is characterized by short but highly frequent turns at low skiing radii and using high dynamic whole body motion (up- down motion of the center of mass partly leading to a jump in between swings). For standardization all downhill trials were instructor paced, by a board certified Austrian alpine skiing instructor who adapted the skiing speeds to the skill level of the participant (Figure 1A).
Figure 1.

Illustration of the A) AS trials with the participant following the alpine skiing instructor and B) XCS trials where the examiner skies right next to the participant, monitoring and verbally communicating the participant’s HR (HR monitors worn both by the participant and examiner) for intensity control.
XCS trials
XCS sessions were performed on a 450 m-loop with a total altitude change of 6 m. All participants used the classical technique (mainly the diagonal stride in the skiers with lower fitness level, and according to the track topography a mix of diagonal stride, kick double poling and double poling in the fit skiers) and their own equipment. Following a 5-min warm-up at 60% HRmax, 4-min stages with LOW (70% HRmax), MOD (80% HRmax) and HIGH (90% HRmax) intensity with 2-min of active recovery at 60% HRmax in between stages were performed. Heart rate was monitored by a Suunto Ambit 2.0 monitor in paired fashion (i.e. HR belt worn by participant; HR monitors worn both by the participant and examiner) and verbally communicated by the examiner who was skiing right next to the participant (Figure 1B).
Indoor cycling ergometry sessions
Indoor cycling sessions were conducted on indoor cycle ergometers (Ergoselect 200, Ergoline GmbH, Bitz, Germany) following the same protocol as in XCS regarding stage duration and HR controlled exercise intensity.
Parameter calculations
During the ramp test Pmax was calculated by linear interpolation using the formula: Pmax = Pf + ((t/60)·ΔP), where Pf was the power output during the last workload completed, t the duration of this last workload (s) and ΔP the difference in power output during the last two workloads (Kuipers et al., 1985). The breath-by-breath values of the VO2 measurements were converted into a 1 Hz signal by linear interpolation. Furthermore, all cardiorespiratory data were smoothed by application of a 15 s moving average. Based on this smoothed data the mean and peak values over the single 4-min stages were calculated. The steady state values were based on the mean over 30 s prior to the end of each stage. The EPOC phase after HIGH consisted of 2 min low intensity activity (cycling at 60% HRmax, or walking to the shelter with a seat during AS and XCS) and 8 min sitting in an upright position with no talking being allowed. Energy expenditure (EE) was determined for each 4-min stage and also estimated for a 1-hr session based on the steady state values. The formula of Weir (1949) EE (kcal·day-1) = [(3.9·VO2 + 1.1·VCO2) · 1440], approximating a caloric equivalent of 21.1 kJ per L O2 was used. To get the EE values for the 4-min stages, the 1 Hz values (kcal·day-1) were converted to kcal·s-1 and then integrated over the 4-min. All these calculations were performed using the Ikemaster Software (IKE-Software Solutions, Salzburg, Austria).
Statistical analysis
All data exhibited a Gaussian distribution verified by the Shapiro-Wilk’s test and, accordingly, the values are presented as means (± SE). Repeated-measures ANOVAs (with 3 exercise modes and 3 intensities as repeated measures, and s as independent measures) were performed to test for main effects of sex, fitness level, age, exercise modes (IC, AS, XCS) and intensities (LOW, MOD, HIGH) as well as interactions between these factors. Following the identification of a significant main effect and/or interaction effect for exercise mode or intensity a one-way repeated-measures ANOVA with Bonferroni post hoc analysis were applied. An alpha value of < 0.05 was considered significant. The Statistical Package for the Social Sciences (Version 22.0; SPSS Inc., Chicago, IL, USA) and Office Excel 2010 (Microsoft Corporation, Redmond, WA, USA) were used.
Results
Patient characteristics (Table 1)
Of the 21 screened volunteers two had to be excluded during the initial medical examination, one due to uncontrolled type 2 diabetes mellitus and one because of signs of myocardial ischemia during exercise stress testing (n = 19).
Characterization of AS and XCS trials
During AS 4-min trials at LOW, MOD and HIGH intensity participants skied a distance of 1.57 ± 0.07, 1.60 ± 0.10 and 1.26 ± 0.05 km (F2,17 = 35, p < 0.001), with an altitude change of 384 ± 20, 380 ± 29 and 350 ± 19 m (F2,17 = 9.0, p = 0.002), a vertical speed of 96 ± 5, 95 ± 7 and 87 ± 5 m·min-1 (F2,17 = 8.6, p = 0.003), a mean skiing speed of 24.0 ± 1.0, 27.7 ± 1.7 and 21.1 ± 0.8 km·h-1 (F2,17 = 25, p < 0.001) and a peak skiing speed of 33.7 ± 1.6, 38.4 ± 2.0 and 28.5 ± 1.0 km·h-1 (F2,17 = 34, p < 0.001). Skiing time for each ride including skiing from the top of the chairlift to the start of the measuring site, and from the end of the 4-min stage to the bottom of the chairlift was 7:02 ± 1:46 min. Mean time for waiting in line and sitting on the chairlift was 8:57 ± 1:46 min. Active skiing time was 44 ± 5%. For XCS during the 4-min trials at LOW, MOD and HIGH intensity participants skied a distance of 0.55 ± 0.05, 0.63 ± 0.06 and 0.73 ± 0.07 km (F2,17 = 45, p < 0.001), with an altitude change of 11 ± 1, 12 ± 1 and 13 ± 2 m (F2,17 = 0.2, p = 0.814) and a mean skiing speed of 8.3 ± 0.8, 9.6 ± 0.9 and 11.0 ± 1.0 km·h-1 (F2,17 = 37, p < 0.001). Break time in between trials was 2:15 ± 0:10 min.
Main effects exercise mode (Table 2)
Table 2.
Cardiorespiratory and metabolic parameters for the pooled data during alpine skiing (AS), cross-country skiing (XCS) and indoor cycling (IC) (n = 19). Data are means (±SE).
| Exercise Mode | ANOVA | |||
|---|---|---|---|---|
| AS | XCS | IC | (F-value, p-value) | |
| HRpeak (bpm) | 151(3) | 153(2) | 143(3) * | F2,11=13, p=.001 |
| Rel. HRpeak (% HRmax) | 87(2) | 88(1) | 82(1) * | F2,11=11, p=.003 |
| Blood lactate (mmol·L-1) | 3.2 (.2) | 4.2 (.5) | 3.7 (.3) | F2,11=4.0, p=.049 |
| Rel. lactate (% peak lactate) | 39(3) | 48(6) | 44(4) | NS |
| Blood glucose (mmol·L-1) | 4.7 (.1) | 5.0 (.1) | 4.7 (.1) | NS |
| RERmean | .98 (.02) | 1.07 (.03) * | .95 (.01) | F2,8=14, p=.003 |
| VO2peak (ml·kg-1·min-1) | 28.2 (.9) * | 34.5 (1.2) * | 31.8 (.9) * | F2,8=13, p=.003 |
| VO2steadystate (ml·kg-1·min-1) | 24.1 (.7) * | 29.6 (1.1) | 28.4 (.8) | F2,8=11, p=.005 |
| Rel. VO2peak (%VO2max) | 74(3) | 89(3) * | 82(4) | F2,8=21, p=.001 |
| EEsteady state (kcal·h-1) | 584(25) * | 729(30) | 679(31) | F2,8=10, p=.006 |
| EE4 min (kcal) | 35.8 (1.4) * | 45.6 (1.8) | 43.0 (2.0) | F2,8=13, p=.003 |
| RPEwhole-body | 12.4 (.5) | 12.2 (.3) | 12.8 (.3) | NS |
| RPEarms | 9.3 (.5) | 11.6 (.5) * | 9.3 (.5) | F2,11=17, p<.001 |
| RPElegs | 15.1 (.5) * | 10.7 (.4) * | 13.4 (.2) * | F2,11=37, p<.001 |
| EPOC (L O2 ·10 min-1) | 3.6 (.3) * | 5.3 (.3) | 5.8 (.2) | F2,11=13, p=.001 |
| EPOC EE (kcal ·10 min-1) | 32.8(1.5) * | 44.4 (1.7) | 45.2 (1.4) | F2,11=11, p=.003 |
HT, heart rate; RER, respiratory exchange ratio; VO2, oxygen uptake; EE, energy expenditure; EEsteady_state, estimated energy expenditure over one hour based on the EE during the last minute of each intensity stage; EE4min, exact energy expenditure during each of the 4-min stages; EPOC, excess post exercise oxygen consumption;
*, different to all other exercise modes; NS, not significant.
When data for LOW, MOD, and HIGH were pooled within each mode of exercise (i.e. AS, XCS, and IC), with the exception of RPEwhole-body and relative lactate (% peak lactate) all variables demonstrated significant differences between AS, XCS and IC (Table 2). For the absolute VO2 values, AS resulted in lower values compared with XCS (all p < 0.001) and IC (p = 0.047 to 0.006), with no difference between XCS and IC. VO2peak in percent of VO2max demonstrated lowest values for AS (XCS: p < 0.001; IC: p = 0.070), followed by IC (XCS: p = 0.027), and XCS. Mean respiratory exchange ratio (RER) was higher in XCS compared with IC (p = 0.005) and AS (p = 0.001). Regarding HR parameters (peak and %HRmax), IC demonstrated lower values compared with XCS (p < 0.001) and AS (p = 0.031 to p = 0.029). RPEwhole-body was not different between exercise modes, while RPEarms was higher in XCS compared with both IC and AS (both p < 0.001). RPElegs was greatest in AS followed by IC (p = 0 .023) and XCS (p < 0.001 to both). EE was lower in AS compared with IC (p = 0.011 to 0.006) and XCS (p < 0.001) with no difference between the latter two. In AS, when considering the time for standing in line and sitting on the chair lift, the value would decrease to 279 ± 16 kcal·h-1. An AS duration of approximately 2:37, respectively 2:25 hrs, would be necessary to achieve comparable EE of 1 h of XCS or IC (Figure 2). There was a trend towards lower lactate values during AS compared with XCS (p = 0.072), while no difference was found when compared with IC. EPOC expressed in liter O2 or energy expenditure in kcal was lower in AS compared with XCS (p = 0.017 or < 0.001) and IC (p = 0.004 or p = 0.001) with no difference between the two latter.
Figure 2.
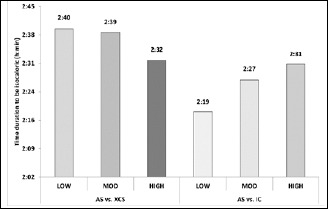
Estimated skiing time needed with alpine skiing (AS) to be isocaloric towards 1 hr cross-country skiing (XCS) or indoor cycling (IC) at low intensity (LOW), moderate intensity (MOD) and high intensity (HIGH).
During each mode of exercise, all measured metabolic and cardiorespiratory parameters increased with intensity (blood glucose: p = 0.006, all other parameters p < 0.001). Blood glucose was unchanged between LOW and MOD (4.74 ± 0.08 vs. 4.74 ± 0.10 mmol·L-1) but was increased at HIGH (4.91 ± 0.11 mmol·L-1) compared with LOW (p = 0.012) and MOD (p = 0.010) (Table 3).
Table 3.
Cardiorespiratory and metabolic parameters during alpine skiing (AS), cross-country skiing (XCS) and indoor cycling (IC) at low (70%HRmax), moderate (80% HRmax) and high (90% HRmax) intensity (n =19). Data are means (±SE).
| AS | XCS | IC | ANOVA (F-value, p-value) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Low | Mod | High | Low | Mod | High | Low | Mod | High | Modea | Intensityb | |
| HRpeak (bpm) | 138(4)* | 154(4) | 162(3) | 137(2)* | 152(2) | 170(2) | 124(3)* | 142(3) | 161(3) | F2,11=13, p=.001 | F2,11=262, p <.001 |
| Rel. HRpeak (% HRmax) | 79(2)* | 88(2) | 93(2) | 79(1)* | 87(1) | 98(1) | 71(1)* | 82(1) | 92(1) | F2,11=11, p=.003 | F2,11=240, p<.001 |
| Blood lactate (mmol·L-1) | 1.8 (.2)* | 3.3 (.2) | 4.6 (.5) | 2.4 (.3)* | 3.5 (.5) | 6.6 (.6) | 1.9 (.2)* | 3.3 (.3) | 6.0 (.5) | F2,11=4.0, p=.049 | F2,11=51, p<.001 |
| Rel. lactate (% peak lactate) | 23(3)* | 37(2) | 57(7) | 28(4)* | 40(7) | 76(7) | 22(3)* | 39(4) | 71(8) | NS | F2,11=50, p<.001 |
| Blood glucose (mmol·L-1) | 4.8 (.1) | 4.8 (.1) | 5.3 (.2) | 4.6 (.1) | 4.7 (.1) | 4.8 (.1)* | 4.8 (.1) | 4.7 (.2) | 4.6 (.2) | NS | F2,11=14, p=.006 |
| RERmean | .91 (.02)* | .95 (.01) | .98 (.02) | 1.02 (.03) | 1.05 (.03) | 1.14 (.03)* | .92 (.02) | 1.00 (.03) | 1.00 (.03) | F2,8=14, p=.003 | F2,8=14, P=.001 |
| VO2peak (ml·kg-1·min-1) | 23.7 (.9)* | 28.6 (1.1) | 32.4 (1.2) | 32.4 (1.1)* | 34.6 (1.4) | 36.4 (1.5) | 27.1 (.8*) | 31.7 (.9) | 36.7 (1.3) | F2,8=13, p=.003 | F2,8=47, p<.001 |
| VO2steadystate (ml·kg-1·min-1) | 19.0 (.5)* | 24.1 (.9) | 29.1 (1.1) | 26.6 (1.0)* | 29.8 (1.1) | 32.4 (1.2) | 23.7 (.8)* | 28.3 (.8) | 33.1 (1.0) | F2,8=11, p=.005 | F2,8=67, p<.001 |
| Rel. VO2peak %VO2max | 64(3)* | 74(4) | 84(4) | 84(4)* | 89(3) | 94(3) | 70(4)* | 82(4) | 94(3) | F2,8=21, p=.001 | F2,8=42, p<.001 |
| EEsteady state (kcal·h-1) | 448(21)* | 590(32) | 713(32) | 644(29)* | 731(29) | 813(33) | 558(28)* | 677(30) | 803(37) | F2,8=10, p=.006 | F2,8=71, p<.001 |
| EE4 min (kcal) | 27.9 (1.1)* | 35.6 (1.8) | 44.0 (1.8) | 40.3 (2.0)* | 45.6 (1.7) | 51.0 (2.0) | 36.2 (1.8)* | 42.8 (2.0) | 50.1 (2.3) | F2,8=13, p=.003 | F2,8=86, p<.001 |
| RPEwhole-body | 9.8 (.6)* | 12.3 (.6) | 14.9 (.6) | 9.3 (.4)* | 11.7 (.4) | 15.6 (.4) | 10.5 (.5)* | 13.0 (.2) | 15.0 (.4) | NS | F2,11=93, p<.001 |
| RPEarms | 7.9 (.5)* | 9.4 (.5) | 10.5 (.8) | 9.2 (.4)* | 11.1 (.6) | 14.4 (.6) | 7.9 (.6)* | 9.0 (.5) | 11.0 (.8) | F2,11=17, p<.001 | F2,11=44, p<.001 |
| RPElegs | 12.6 (.5)* | 16.1 (.6) | 16.8 (.6) | 8.8 (.4)* | 10.2 (.5) | 13.0 (.5) | 11.1 (.3)* | 13.6 (.3) | 15.5 (.5) | F2,11=37, p<.001 | F2,11=106, p<.001 |
HR, heart rate; RER, respiratory exchange ratio; VO2, oxygen uptake; EE, energy expenditure; EEsteady_state, estimated energy expenditure over one hour based on the EE during the last minute of each intensity stage; EE4min, exact energy expenditure during each of the 4-min stages; RPE, rate of perceived exertion.
a main effect of exercise mode.
b main effect of intensity.
*significantly different to the two other intensities in the same exercise mode. NS, not significant.
Effects of sex, age and fitness level (Table 4)
Table 4.
Cardiorespiratory and metabolic parameters for the pooled data during alpine skiing (AS), cross-country skiing (XCS) and indoor cycling (IC) for male (n=12) vs. female (n=7), young (n=10) vs. old (n=9), and fit (n=10) vs. unfit (n=9). Data are means (±SE).
| Gender | Age | Fitness Level | ANOVA (p-value) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Young | Old | Fit | Unfit | Gender | Age | Fitness | |
| HRpeak (bpm) | 145(3) | 155(4) | 156(3) | 139(3) | 149(3) | 149(3) | p=.042 | p=.002 | NS |
| Rel. HRpeak (% HRmax) | 84(1) | 88(1) | 85(1) | 87(1) | 83(1) | 87(1) | p=.023 | NS | p=.021 |
| Blood lactate (mmol·L-1) | 4.2 (.3) | 3.1 (.5) | 3.7 (.4) | 3.7 (.4) | 3.2 (.4) | 4.1 (.4) | NS | NS | NS |
| Rel. lactate (% peak lactate) | 45(4) | 42(6) | 38(5) | 51(5) | 32(5) | 52(5) | NS | NS | p=.015 |
| RERmean | 1.00 (.02) | .99 (.02) | .97 (.02) | 1.02 (.02) | .97 (.02) | 1.03 (.02) | NS | NS | NS |
| VO2peak (ml·kg-1·min-1) | 34.3 (1.1) | 25.9 (1.3) | 34.3 (1.1) | 28.7 (1.2) | 36.0 (1.3) | 27.0 (1.0) | p=.001 | p=.009 | p<.001 |
| VO2steadystate (ml·kg-1·min-1) | 29.8 (.9) | 22.4 (1.1) | 29.8 (.9) | 22.4 (1.1) | 29.8 (.9) | 22.4 (1.1) | p<.001 | p<.001 | p<.001 |
| Rel. VO2peak %VO2max | 80(4) | 86(5) | 85(4) | 79(4) | 79(5) | 84(4) | NS | NS | NS |
| EEsteady state (kcal·h-1) | 758(30) | 477(39) | 717(32) | 611(35) | 695(38) | 634(29) | p<.001 | NS | NS |
| EE4 min (kcal) | 51.5 (2.2) | 35.1 (3.3) | 44.8 (2.0) | 38.2 (2.1) | 43.4 (2.3) | 39.5 (1.8) | p=.002 | p=.049 | NS |
| RPEwhole-body | 12.9 (.3) | 11.9 (.5) | 12.2 (.4) | 12.8 (.4) | 13.0 (.4) | 12.1 (.4) | NS | NS | NS |
| RPEarms | 10.5 (.5) | 9.4 (.7) | 9.5 (.6) | 10.8 (.6) | 10.4 (.6) | 9.8 (.6) | NS | NS | NS |
| RPElegs | 13.5 (.3) | 12.5 (.4) | 13.0 (.4) | 13.2 (.3) | 13.8 (.3) | 12.5 (.4) | NS | NS | p=.022 |
HR, heart rate; RER, respiratory exchange ratio; VO2, oxygen uptake; EE, energy expenditure; EEsteady_state, estimated energy expenditure over one hour based on the EE during the last minute of each intensity stage; EE4min, exact energy expenditure during each of the 4-min stages; NS, not significant.
Pooled data for all three intensities and three exercise modes for sex, age and fitness level are presented in Table 4. Male participants revealed higher VO2, EE and EPOC (all p < 0.001). Both absolute and relative HR were lower in men (p < 0.05). No sex differences were found for relative VO2 (% VO2max), RER, RPE, lactate and blood glucose (all p > 0.05). The younger participants demonstrated higher absolute VO2 (p < 0.01), absolute HR (p < 0.01), EE (p < 0.05) and EPOC (p < 0.05) than the older participants with no further differences in the other measured parameters. Compared to the unfit, the fit participants had higher absolute VO2 (p < 0.001) and RPElegs (p = 0.022). Additionally, relative HR (%HRmax) and relative lactate (%peak lactate) were reduced in the fit group (all p < 0.05).
Interaction effects
The interaction between exercise mode x fitness level was significant for RPEwhole-body (p = 0.004), RPEarms (p = 0.030) and RPElegs (p = 0.015). For both RPEwhole-body and RPElegs equal values for fit and unfit were found for IC while during XCS and AS the fit had higher values. For RPEarms equal levels between fit and unfit were found during IC and AS while the fit revealed increased values during XCS.
Interaction effects between fitness level x exercise intensity, sex x exercise intensity and age x exercise intensity were found for absolute VO2 (p = 0.002 to 0.026), and EE (p = 0.004 to 0.025) demonstrating a more pronounced increase in the fit, respectively male and young participants when intensity was increased when compared with the unfit, respectively female and older participants (see Figure 3A-C).
Figure 3.
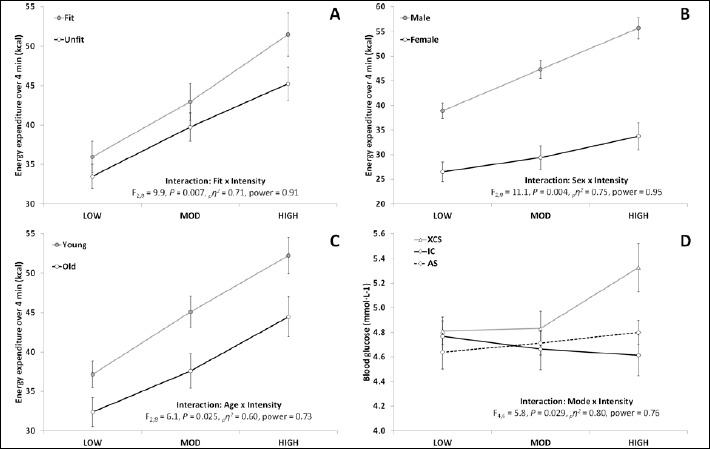
Interaction between A) fitness level and exercise intensity, B) sex and exercise intensity, C) age and exercise intensity and D) exercise mode (XCS, cross-country skiing; IC, indoor cycling; AS, alpine skiing) and exercise intensity [low intensity (LOW), moderate intensity (MOD) and high intensity (HIGH)] with regards to energy expenditure during the 4-min trials.
Among all measured parameters, interactions between exercise mode x exercise intensity were found only for blood glucose (p = 0.029, Figure 3D), lactate (p = 0.033) and RER (p = 0.020) demonstrating a more pronounced increase with a greater exercise increase during XCS compared with IC and AS.
Discussion
The main findings of our study are: 1) XCS and IC are generally more demanding for the cardiorespiratory system than AS, i.e. VO2 and EE are higher; 2) This might be partially due to the high levels of RPElegs during AS, which might result in an attenuated increase in cardiorespiratory output based on muscular limitations as compared to XCS and IC; 3) with XCS, even though VO2, HR and lactate were higher compared to both or at least one of the exercise modes IC and AS, RPEwhole-body was equal and RPElegs lower compared with AS and IC; 4) RPEarms was only high during XCS and was also paralleled by increased blood glucose and lactate levels during the high intensity trial compared with the other exercises; 5) absolute and relative (% body weight) values of VO2, EE and EPOC were higher in men; 6) unfit had higher relative lactate levels (% peak lactate), lower VO2 but equal EE values, 7) younger participants demonstrated higher VO2, HR, EE and EPOC at similar relative HR (% HRmax), and 8) young, fit and male participants were able to increase their EE and VO2 more pronounced compared with their old, unfit and female counterparts.
Energy expenditure and cardiorespiratory parameters
In the current study, VO2 and EE were similar during XCS and IC, but significantly higher than during AS. Also, VO2 and EE during AS-HIGH compared well to XCS-MOD and IC-MOD, while AS-MOD was comparable to XCS-LOW and IC-LOW. However, this calculation is just valid when estimating the EE per hr based on the 4-min active skiing interval and neglecting the recovery period while standing in line or taking a lift. Müller et al. (2011) demonstrated that this systematic change from relatively high load (~73% HRmax ~7 min) followed by a pronounced recovery (~59% HRmax, ~13 min) happens between 9-10 times during a ski day. Therefore, a 3.5 hrs ski day consists of 68 min skiing (33%), 120 min recovery time (56%) and 23 min rest or extended recovery (11%). In this study, active skiing time was slightly higher with 44 ± 5%. Based on this data, to achieve equal EE at the three different intensities during AS compared with one hour of XCS or IC, AS (including both active and recovery time) has to be performed 2:37 and 2:25 hrs, respectively.
In the literature, there is little data available on EE during AS, XCS and IC in elite athletes, let alone leisure time skiers. Jeukendrup and Gleeson (2010) reported estimated energy cost for AS in relation to body weight (50-90 kg) of 270 – 500 kcal·h-1 for low intensity downhill skiing and 440-828 kcal·h-1 for high intensity downhill skiing. Therefore, based on the current studies results, by using a skiing style like CLR and ST continuously over 4 min, EE values comparable or even higher as during racing might be achieved.
In our study, relative HR (%HRmax) during AS were 79%, 88% and 93% for PSS, CLR and ST, and thus higher than those also documented in elderly skiers by Scheiber et al. (2009) and Müller et al. (2011). Müller et al. (2011) reported mean HR values during the active skiing time of 73% HRmax and Scheiber et al. (2009) values of 62-68% and 69-75% during PSS and CLR on beginner slopes, and 70-76% and 80-81% during PSS and CLR on steeper slopes. Furthermore, in the study by Scheiber et al. (2009) mean VO2 values ranged from approximately 13-19 ml·kg-1·min-1 across all analyzed skiing situations with significantly higher values for CLR (13-17 ml·kg-1·min-1) compared to PSS (16-19 ml· kg-1·min-1). Those values compare well with the current study demonstrating increased VO2 values with CLR compared with PSS (23.7 vs. 28.6 ml·kg-1·min-1). In addition, it was demonstrated that by skiing with ST even a further increase in VO2 up to 32.4 ml·kg-1·min-1 was possible. As with HR values, %VO2max of 64-84% were distinctly higher compared to the study by Scheiber et al. (2009) who demonstrated values of 38-42% and 45-49 % for PSS and CLR on beginner slopes, and 42-46% and 50-52% during PSS and CLR on steeper slopes. Therefore, in the current study, continuous skiing over 4 min with different intensities posed a greater physiological challenge. This might be attributed to the more dynamic skiing during CLR and ST and the younger participants (47.6 vs. 62.2 yrs) compared with the study by Scheiber et al. (2009). Also, during AS racing, %VO2max were documented to be between 68-88% (Vogt et al., 2005, Karlsson et al., 1978). Therefore, ST constitutes comparable loading as compared with AS racing.
In contrast to AS, XCS and IC are typical endurance sports with constant or varying loads and a high demand on the cardio-respiratory and musculoskeletal system. A high percentage of the whole body musculature is activated during XCS (Rusko, 2008). Jeukendrup and Gleeson (2010) reported weight dependent (50 – 90 kg) values of 530-950 kcal·h-1 during XCS and for cycling 200-360 kcal·h-1 at 9 km·h-1 h, 260-570 kcal·h-1 at 15 km·h-1 and 530-950 kcal·h-1 during racing. Based on measurements of carbohydrate and fat utilization during XCS, Van Hall et al. (2003) reported EE of approximately 1220 kcal·h-1 during whole body (diagonal stride), and 287 kcal·h-1 during arm work (double poling), which compared well with the data measured in our study. Interestingly, the relative VO2 values in the current study (94% VO2max) during both IC and XCS were similar to those in previous studies during XCS racing (Stöggl et al., 2007).
The EPOC was lower in AS compared with XCS and IC which might be mainly attributed towards the greater physiological loading during the latter two. To the best of our knowledge no comparable data about EPOC in these exercise modes is available. Vogt et al. (2005) distinguished between active phase and EPOC phase during slalom racing, but no separate data was presented in the results.
Rating of perceived exertion
Whole body RPE was similar between the three exercise modes, however XCS was the only exercise mode where participants reported exertion of the upper body, and AS was the mode of exercise with the greatest subjective exertion for the legs, which was followed by IC and XCS. The former finding is associated with the whole body involvement during XCS, where a greater part of the upper body, lower body and trunk muscles are engaged (Rusko, 2008, Holmberg et al., 2005). Interestingly, even though HR, VO2 and lactate were slightly higher in XCS, especially when compared with AS, this was not reflected in the whole-body and leg RPE values. Therefore, during XCS high metabolic and respiratory loading can be achieved at a comparatively moderate level of exertion. Already during low intensity XCS (e.g. slow walking on skis in some of the participants) EE was as high as 644 kcal·h-1. The fact that RPElegs was greatest during AS can be explained by the mix of static and dynamic muscle activity of the lower extremities (Müller and Schwameder, 2003, Kröll et al., 2010) with both moderate to high concentric and eccentric loading (Tesch, 1995) in contrast to mainly dynamic and cyclic muscle loading during XCS and IC. This type of muscle loading during AS might be associated with the attenuated increase in cardiorespiratory output based on muscular limitations as compared to XCS and IC.
Effects of intensity and its interaction with exercise mode
It is well known that an increase in exercise intensity leads to an increase in metabolic and cardiorespiratory parameters alike. Whereas during XCS and IC the exercise intensity can easily be modified by altering the slope gradient or changing the speed of travel, during AS this cannot so easily be done. Previous investigations demonstrated that skiing styles and steepness of the terrain play important roles on the physiologic response of older recreational skiers (Scheiber et al., 2009). The current study demonstrates that an increase in the physiological responses can be induced by choosing different skiing styles, i.e. PSS, CLR and ST without relevant changes in skiing speed (vertical speeds: 96, 95, and 87 m·min-1; mean skiing speed: 24, 28 and 21 km·h-1). Since ST induced a pronounced physiological response (91% HRmax and 84% VO2max) and participants were able to maintain skiing at such high intensity for 4 min, it might lend itself to high intensity interval training during AS.
During XCS, blood lactate and glucose were increased more pronounced with an increase in exercise intensity when compared with IC and AS, where especially blood glucose values remained stable across intensities (Fig. 3D). This increase might be explained by the greater involvement of total muscle mass—especially in the upper body and trunk—during XCS compared with the other two exercise modes. In this context, Van Hall et al. (2003) demonstrated that when using the double poling technique—which puts large emphasis on upper body muscles—arterial lactate was 2.5 fold greater when compared with the whole body exercise diagonal stride. In addition, Richter et al. (1988) have shown that the net glucose uptake into the muscle decreases with an increase of active muscle mass. This decrease in uptake may depend on the catecholamine stimulation of glycolysis. This glucose sparing effect could also be triggered by increasing lactate levels. Similar results of a post-exercise hyperglycemia were described after long-distance XCS races (Ronsen et al., 2004) as well as for type-I diabetics (Adolfsson et al., 2011, Turner et al., 2015). The question here arises if exercise induced increases in blood glucose level might be seen as positive or negative especially when considering risk groups (e.g. diabetic patients). Nonetheless, increased blood glucose values during XCS at HIGH intensity in this group of healthy participants were still in a normal range when comparing to diabetic reference values of normal fasting blood glucose <5.5 mmol·L-1 (Alberti and Zimmet, 1998). Additionally, Hawley and Gibala (2009) postulated in their review that high intensity exercise is possibly more efficient in reducing diabetic long-term markers such as HbA1c.
Effects of gender
Even though male participants demonstrated lower HR and similar relative VO2 (% VO2max) values compared with females, men exercised at ~33% higher absolute VO2, with 47-59% greater EE and 56-87% higher EPOC. Therefore, in one hour of steady activity men would have burned almost 300 kcal·h-1 more than women. Even when values were adjusted for body weight, men expended significantly greater amounts of energy compared to women (9.5 vs. 7.0 kcal·h-1·kg-1), which could be explained by the generally greater percentage of body fat and lesser muscle mass in relation to body size in women as compared to men (Katch et al., 2011).
Effects of fitness level
It is known that EE is related to exercise intensity, body weight (Jeukendrup and Gleeson, 2010, Katch et al., 2011), sex, and age (Katch et al., 2011). However, there is paucity of data about the effects of fitness level on EE. In the current study, even though VO2 was higher in the fit group, no differences were found in EE and EPOC between fit and unfit. This might be based on the trend (p < 0.1) towards a higher RER during exercise in the unfit group when compared with the fit. Furthermore, the unfit were loaded at a greater % of their peak lactate. Therefore, unfit participants demonstrated lower economy for performing the same task as the fit. These data refer to an augmented glycolytic energy turn-over during exercise at similar %HRmax in the unfit. However, based on this data no matter if fitness level is high or low, equal EE and EPOC is possible independent of the exercise mode.
Interestingly, the fit participants were – independent from exercise mode - able to increase their EE and VO2 more pronounced when exercise intensity was increased compared with the unfit. This is in part in contrast to previous investigations during AS demonstrating that fitness level does not play an important role on the physiologic response of older recreational skiers (Scheiber et al., 2009). However, our finding is supported by Karlsson et al. (1978) describing As an effective recreational winter sport with performance enhancing effects, however with some limitations for recreational skiers compared to professional skiers (Karlsson et al., 1978). Those authors stated that professional skiers normally have high strength and coordinative capacities, which enables them to ski in a very active and exhausting skiing style, while recreational skiers often have limited strength and coordinative skills. Therefore, low level skiers might not reach high intensities during skiing – which may be necessary for training adaptations especially for the cardiopulmonary system – due to poor technique and strength. Based on the exercise independent interaction, this finding might be transferred also to XCS and IC.
During both IC and AS the fitness level had no effect on the subjective loading of the arms, however during XCS, the fitter participants reported greater RPEarms compared with the unfit. This might point again towards a greater technical skill level, coupled with a greater application of the upper body and possibly also a greater amount of double poling during the XCS trials in the fit group. For the subjective demand on the whole body and the legs there was no difference between fit and unfit during IC, however during both XCS and AS the fit demonstrated greater levels. Therefore, in the more technical demanding exercises AS and XCS a higher fitness level leads to an increased possibility to greater exert the body. This might again be related to the aspects about technical skills mentioned above, but also on the possibly higher skiing velocities, a greater number of more dynamic turns and consequently greater muscle loads.
Effect of age
Recent investigations have shown that AS is a suitable and a safe recreational sport for an elderly and a sedentary population (Krautgasser et al., 2011, Müller et al., 2011, Scheiber et al., 2009, Scheiber et al., 2012, Kahn et al., 1993, Pötzelsberger et al., 2015). However, a direct comparison between the physiological loading of young and elderly participants during winter sports is lacking. In the current study the younger participants demonstrated ~19% greater absolute VO2, ~13% greater absolute HR values, 17-27% greater EE, and 15-18% greater EPOC values compared with the older participants. This goes in line with the documented decline in basal metabolic rate (Katch et al., 2011) and aerobic fitness (Jackson et al., 2009) with increase in age. Special attention should be paid upon the great discrepancy between absolute and relative HR values between young and elderly, especially when trying to control intensity during guided skiing/training. The older the participants the earlier the limits of HR will be reached.
Finally, male, fit and young participants were able to increase their EE and VO2 more pronounced with an increase in intensity compared with their counterparts (See Figures 3A-C). This might be based on the ability of this group to push themselves harder when exercise intensity is increased, a lower fear level (e.g. when skiing speed and dynamics are increasing), a greater reserve to their maximal effort based on higher work economy (less anaerobic contribution as discussed above) and again a higher skill level and therefore less technical limitations when exercise intensity and speed gets high.
Limitations
Possible limitations of the study can be seen in the mismatch between men (n = 12) and women (n = 7) and the effects of wearing the equipment and the mask, which might have led to augmented subjective loading and might have influenced the sight especially during AS. Furthermore, the physiological responses between XCS and IC are comparable based on the defined exercise intensities, while during AS intensity was based on application of specific skiing techniques. This was done based on security reasons, due to that the participant had to focus on the slope conditions, the instructors pace and also other skiers in the measurement zone and not on the HR monitor.
Conclusion
There were greater demands on the cardiorespiratory system at all three intensities during XCS and IC compared to AS. However, by applying the skiing modes parallel ski steering, carving long radii and short turn skiing a significant increase in metabolic and cardiorespiratory response was achievable, allowing even high intensity training (i.e. HR > 90% HRmax) of adequately long duration without relevant changes in skiing speed. EE during AS can be maximized by using only short or no breaks during the downhill phases and by choosing a more dynamic skiing mode, i.e. carving or short turn skiing. Since the active skiing time was approximately 44%, an AS duration of more than 2:30 h is needed to equalize EE of one hour of XCS or IC. Therefore, when applying distinct skiing modes and the terrain allows steady skiing over a longer period, AS might provide sufficient stimulus for the cardiologic and metabolic system to enhance fitness and reduce cardiovascular risk. Consequently, besides a popular leisure activity to experience nature and freedom in the winter months, AS might also serve as a fitness workout (e.g. “cardio-skiing”). Furthermore, XCS was found to be the most effective activity for generating a high EE and VO2 while AS was the most demanding activity for the legs. This aspect should be considered when choosing an activity for mainly leg training purposes.
Acknowledgements
We would like to thank Manuel Hirner, Kathrin Hirner, Stephanie Feuchter and Markus Förmer for their assistance during the measurements, the participants for their enthusiasm and cooperation and the ski resorts of Saalbach Hinterglemm and Flachau Winkel for granting us free access. The current study complies with Austrian ethical standards and laws. This study was supported in part by an unrestricted grant of the State of Salzburg
Biographies

Thomas STÖGGL
Employment
Associate Professor at the Department of Sport Science and Kinesiology, University of Salzburg.
Degree
Assoc. Prof. Mag. Dr.
Research interests
Biomechanics and physiology of winter sports in elite athletes and sedentary people; training intensity distribution among elite endurance athletes; Exercise Physiology.
E-mail: thomas.stoeggl@sbg.ac.at

Christoph SCHWARZL
Employment
Sports Physiotherapist
Degree
Msc
Research interests
Elite Sports; Sports injury

Edith E. MÜLLER
Employment
Research associate
Degree
Dr.
Research interests
exercise intervention; cardiovascular risk

Masaru NAGASAKI
Employment
Associate Professor at the Department of Health Science, Faculty of Psychological and Physical Science, Aichi Gakuin University
Degree
Associate Professor, PhD
Research interests
Physiology of alpine skiing; Exercise physiology; Diabetes

Julia STÖGGL
Employment
Strength and Conditioning Coach
Degree
Msc
Research interests
Performance diagnostics; exercise physiology.

Peter SCHEIBER
Employment
University of Salzburg, Department of Sport Science and Kinesiology
Degree
Dr.
Research interests
Biomechanics and Physiology in Alpine Skiing

Martin SCHÖNFELDER
Employment
Scientific assistant
Degree
SD, Dr. rer. Nat.
Research interests
exercise physiology, sports science, molecular sports biology
E-mail:martin.schoenfelder@tum.de

Josef NIEBAUER
Employment
Full professor and chair; University Institute of Sports Medicine, Prevention and Rehabilitation, Paracelsus Medical University, Salzburg, Austria
Degree
MD PhD MBA
Research interests
Antiatherogenic effects of exercise training; endothelial function; sports cardiology; pre-participation examination
E-mail: j.niebauer@salk.at
References
- Adolfsson P., Nilsson S., Lindblad B. (2011) Continuous glucose monitoring system during physical exercise in adolescents with type 1 diabetes. Acta Paediatrica 100, 1603-1609. [DOI] [PubMed] [Google Scholar]
- Ainsworth B.E., Haskell W.L., Herrmann S.D., Meckes N., Bassett D.R., Jr., Tudor-Locke C., Greer J.L., Vezina J., Whitt-Glover M.C., Leon A.S. (2011) 2011 Compendium of Physical Activities: a second update of codes and MET values. Medicine and Science in Sports and Exercise 43, 1575-1581. [DOI] [PubMed] [Google Scholar]
- Alberti K. G., Zimmet P. Z. (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabetic Medicine: a Journal of the British Diabetic Association 15, 539-553. [DOI] [PubMed] [Google Scholar]
- Bachleitner R. (1998) Alpiner Wintersport: eine sozial-, wirtschafts-, tourismus- und ökowissenschaftliche Studie zum alpinen Skilauf, Snowboarden und anderen alpinen Trendsportarten [Alpine wintersports: a social, economic, touristic and ecological study for alpine skiing, snowboarding and other alpine trendsports], Innsbruck-Wien, Studien Verlag Ges.m.b.H. [Google Scholar]
- Bergh U. (1982) Physiology of cross-country ski racing, Champaign, Illinois, Human Kinetics. [Google Scholar]
- Björklund G., Holmberg H. C., Stöggl T. (2015) The effects of prior high intensity double poling on subsequent diagonal stride skiing characteristics. Springerplus 4, 40 (1-12). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Björklund G., Stöggl T., Holmberg H. C. (2010) Biomechanically influenced differences in O2 extraction in diagonal skiing: arm versus leg. Medicine and Science in Sports and Exercise 42, 1899-1908. [DOI] [PubMed] [Google Scholar]
- Burtscher M., Pachinger O., Mittleman M. A., Ulmer H. (2000) Prior myocardial infarction is the major risk factor associated with sudden cardiac death during downhill skiing. International Journal of Sports Medicine 21, 613-615. [DOI] [PubMed] [Google Scholar]
- Dannenberg A.L., Keller J.B., Wilson P.W., Castelli W.P. (1989) Leisure time physical activity in the Framingham Offspring Study. Description, seasonal variation, and risk factor correlates. American Journal of Epidemiology 129, 76-88. [DOI] [PubMed] [Google Scholar]
- Hawley J. A., Gibala M. J. (2009) Exercise intensity and insulin sensitivity: how low can you go? Diabetologia 52, 1709-1713. [DOI] [PubMed] [Google Scholar]
- Hoffman M.D. (1992) Physiological comparisons of cross-country skiing techniques. Medicine and Science in Sports and Exercise 24, 1023-1032. [PubMed] [Google Scholar]
- Holmberg H.C. (2005) Physiology of cross-country skiing - with special emphasis on the role of the upper body. Karolinska Institutet. [Google Scholar]
- Holmberg H. C., Lindinger S., Stöggl T., Eitzlmair E., Müller E. (2005) Biomechanical analysis of double poling in elite cross-country skiers. Medicine and Science in Sports and Exercise 37, 807-818. [DOI] [PubMed] [Google Scholar]
- Holmberg H. C., Rosdahl H., Svedenhag J. (2007) Lung function, arterial saturation and oxygen uptake in elite cross country skiers: influence of exercise mode. Scandinavian Journal of Medicine & Science in Sports 17, 437-444. [DOI] [PubMed] [Google Scholar]
- Impellizzeri F. M., Marcora S. M. (2007) The physiology of mountain biking. Sports Medicine 37, 59-71. [DOI] [PubMed] [Google Scholar]
- Jackson A. S., Sui X., Hebert J. R., Church T. S., Blair S. N. (2009) Role of lifestyle and aging on the longitudinal change in cardiorespiratory fitness. Archives of Internal Medicine 169, 1781-1787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeukendrup A., Gleeson M. (2010) Sport Nutrition. Leeds - UK, Human Kinetics. [Google Scholar]
- Kahn J. F., Jouanin J. C., Espirito-Santo J., Monod H. (1993) Cardiovascular responses to leisure alpine skiing in habitually sedentary middle-aged men. Journal of Sports Sciences 11, 31-36. [DOI] [PubMed] [Google Scholar]
- Karlsson J., Eriksson A., Forsberg A., Kallberg L., Tesch P. A. (1978) The Physiology of Alpine Skiing, Stockholm, Trygg-Hansa Insurance Company. [Google Scholar]
- Katch V.L., McArdle W.D., Katch F.I. (2011) Essentials of Exercise Physiology. Baltimore, MD, Wolters Kluwer/Lippincott Williams & Wilkins Health. [Google Scholar]
- Krautgasser S., Scheiber P., von Duvillard S. P., Müller E. (2011) Physiological responses of elderly recreational Alpine skiers of different fitness and skiing abilities. Journal of Sports Science and Medicine 10, 748-753. [PMC free article] [PubMed] [Google Scholar]
- Kröll J., Wakeling J. M., Seifert J. G., Müller E. (2010) Quadriceps Muscle Function during Recreational Alpine Skiing. Medicine and Science in Sports and Exercise 42, 1545-1556. [DOI] [PubMed] [Google Scholar]
- Kuipers H., Verstappen F. T., Keizer H. A., Geurten P., van Kranenburg G. (1985) Variability of aerobic performance in the laboratory and its physiologic correlates. International Journal of Sports Medicine 6, 197-201. [DOI] [PubMed] [Google Scholar]
- Larsson P., Henriksson-Larsen K. (2008) Body composition and performance in cross-country skiing. International Journal of Sports Medicine 29, 971-975. [DOI] [PubMed] [Google Scholar]
- Mendis S., Puska P., Norrving B. 2011. Global atlas on cardiovascular disease prevention and control. Geneva: World Health Organization. [Google Scholar]
- Merchant A. T., Dehghan M., Akhtar-Danesh N. (2007) Seasonal variation in leisure-time physical activity among Canadians. Canadian Journal of Public Health. Revue Canadienne de Sante Publique 98, 203-208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mognoni P., Rossi G., Gastaldelli F., Canclini A., Cotelli F. (2001) Heart rate profiles and energy cost of locomotion during cross-country skiing races. European Journal of Applied Physiology 85, 62-67. [DOI] [PubMed] [Google Scholar]
- Mujika I., Padilla S. (2001) Physiological and performance characteristics of male professional road cyclists. Sports Medicine 31, 479-487. [DOI] [PubMed] [Google Scholar]
- Müller E., Gimpl M., Pötzelsberger B., Finkenzeller T., Scheiber P. (2011) Salzburg Skiing for the Elderly Study: study design and intervention--health benefit of alpine skiing for elderly. Scandinavian Journal of Medicine & Science in Sports 21(Suppl 1), 1-8. [DOI] [PubMed] [Google Scholar]
- Müller E., Schwameder H. (2003) Biomechanical aspects of new techniques in alpine skiing and ski-jumping. Journal of Sports Sciences 21, 679-692. [DOI] [PubMed] [Google Scholar]
- Mygind E., Larsson B., Klausen T. (1991) Evaluation of a specific test in cross-country skiing. Journal of Sports Sciences 9, 249-257. [DOI] [PubMed] [Google Scholar]
- Pötzelsberger B., Stöggl T., Lindinger S. J., Dirnberger J., Stadlmann M., Buchecker M., Hofstaedter T., Gordon K., Müller E. (2015) Alpine Skiing With total knee ArthroPlasty (ASWAP): effects on strength and cardiorespiratory fitness. Scandinavian Journal of Medicine & Science in Sports 25(Suppl 2), 16-25. [DOI] [PubMed] [Google Scholar]
- Richter E. A., Kiens B., Saltin B., Christensen N. J., Savard G. (1988) Skeletal muscle glucose uptake during dynamic exercise in humans: role of muscle mass. The American Journal of Physiology 254, E555-561. [DOI] [PubMed] [Google Scholar]
- Ronsen O., Borsheim E., Bahr R., Klarlund Pedersen B., Haug E., Kjeldsen-Kragh J., Hostmark A. T. (2004) Immuno-endocrine and metabolic responses to long distance ski racing in world-class male and female cross-country skiers. Scandinavian Journal of Medicine & Science in Sports 14, 39-48. [DOI] [PubMed] [Google Scholar]
- Rusko H. (2008) Handbook of Sports Medicine and Science, Cross Country Skiing, Oxford, UK, Blackwell Science. [Google Scholar]
- Saltin B., Astrand P. O. (1967) Maximal oxygen uptake in athletes. Journal of Applied Physiology 23, 353-358. [DOI] [PubMed] [Google Scholar]
- Scheiber P., Krautgasser S., von Duvillard S. P., Müller E. (2009) Physiologic responses of older recreational alpine skiers to different skiing modes. European Journal of Applied Physiology 105, 551-558. [DOI] [PubMed] [Google Scholar]
- Scheiber P., Seifert J., Müller E. (2012) Relationships between biomechanics and physiology in older, recreational alpine skiers. Scandinavian Journal of Medicine & Science in Sports 22, 49-57. [DOI] [PubMed] [Google Scholar]
- Stöggl T., Björklund G., Holmberg H. C. (2013) Biomechanical determinants of oxygen extraction during cross-country skiing. Scandinavian Journal of Medicine & Science in Sports 23, e9-20. [DOI] [PubMed] [Google Scholar]
- Stöggl T., Lindinger S., Müller E. (2007) Analysis of a simulated sprint competition in classical cross country skiing. Scandinavian Journal of Medicine & Science in Sports 17, 362-372. [DOI] [PubMed] [Google Scholar]
- Stöggl T., Schwarzl C., Müller E. E., Nagasaki M., Stöggl J., Scheiber P., Schönfelder M., Niebauer J. (2015) Effects of skiing on cardiorespiratory and metabolic responses in middle-aged subjects with increased cardiovascular risk. International Journal of Cardiology 203, 618-620. [DOI] [PubMed] [Google Scholar]
- Tesch P. A. (1995) Aspects on muscle properties and use in competitive Alpine skiing. Medicine and Science in Sports and Exercise 27, 310-314. [PubMed] [Google Scholar]
- Turner D., Luzio S., Gray B. J., Dunseath G., Rees E. D., Kilduff L. P., Campbell M. D., West D. J., Bain S. C., Bracken R. M. (2015) Impact of single and multiple sets of resistance exercise in type 1 diabetes. Scandinavian Journal of Medicine & Science in Sports 25, e99-109. [DOI] [PubMed] [Google Scholar]
- Ulmer H., Kelleher C., Diem G., Concin H., Ruttmann E. (2004) Estimation of seasonal variations in risk factor profiles and mortality from coronary heart disease. Wiener Klinische Wochenschrift 116, 662-668. [DOI] [PubMed] [Google Scholar]
- Van Hall G., Jensen-Urstad M., Rosdahl H., Holmberg H. C., Saltin B., Calbet J. A. (2003) Leg and arm lactate and substrate kinetics during exercise. American Journal of Physiology. Endocrinology and Metabolism 284, E193-205. [DOI] [PubMed] [Google Scholar]
- Vogt M., Puntschart A., Angermann M., Jordan K., Spring H., Müller E., Hoppeler H. (2005) Metabolische konsequenzen eines wettkampfmäßigen Slalomtrainings bei Nachwuchs-Skiathleten [Metabolic consequences of a simulated slalom competition training of recreational alpine skiers]. Leistungssport 35, 48-54. [Google Scholar]
- Weir J. B. (1949) New methods for calculating metabolic rate with special reference to protein metabolism. The Journal of Physiology 109, 1-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Welde B., Evertsen F., Von Heimburg E., Ingulf Medbo J. (2003) Energy cost of free technique and classical cross-country skiing at racing speeds. Medicine and Science in Sports and Exercise 35, 818-825. [DOI] [PubMed] [Google Scholar]