

Abstract
The lateral center edge angle (LCEA) and the anterior center edge angle (ACEA) are commonly used to assess acetabular coverage of the femoral head. There are two distinct methods found in the literature to obtain these angles, specifically, measuring to the most lateral bone edge versus the sclerotic lateral sourcil edge. A difference between these two methods may contribute to inconsistent estimates of acetabular coverage, and potentially lead to clinical misdiagnosis and treatment mismanagement. The objectives of this study were to quantify the difference between bone edge and sourcil edge measurements and to determine how the difference influences the classification of acetabular coverage in adult patients with suspected hip pathomorphology. Two observers completed the measurements independently using preoperative anteroposterior and false profile radiographs. Bland–Altman plots and paired t-tests were used to compare measurement methods. Bone and sourcil measurements of the LCEA and ACEA were significantly different (both P < 0.001). On average, the bone LCEA was 4° (95% limits of agreement = −2° to 10°) greater than the sourcil LCEA. The bone ACEA was, on average, 10° (95% limit of agreement = −2° to 22°) greater than the sourcil ACEA. The differences often led to different clinical classifications for the same hip. With a statistically and clinically significant difference in the quantification of acetabular coverage using bone edge versus sourcil edge methods for measuring the LCEA and ACEA in adult patients, it should be mandatory to clearly identify which method was used in each study.
INTRODUCTION
Some forms of hip pathomorphology, including hip dysplasia and pincer femoroacetabular impingement, are characterized by abnormal acetabular coverage of the femoral head. In 1939, Wiberg created the lateral center edge angle (LCEA) to quantify the lateral coverage of the acetabulum on anteroposterior (AP) radiographs [1]. Similarly, in 1961, Lequesne described the vertical–center–anterior margin angle or anterior center edge angle (ACEA) to assess anterior acetabular coverage on false profile (FP) radiographs [2]. Both of these measurements are central to the diagnosis of hip pathomorphology and play an important role in therapeutic decision-making, including selection of an appropriate surgical intervention [3].
Wiberg defined the LCEA as the angle formed by one line drawn through the center of the femoral head parallel to the longitudinal axis of the body, and a second line drawn from the center of the femoral head to the lateral edge of the acetabular roof [1]. He described the lateral edge as a point ‘where the curving of the acetabular border laterosuperiorly begins’ and ‘where the bony support may be considered to end’, and noted this point is easy to define on radiographs as it appears as the end of a dense shadow representing the acetabular roof [1]. We believe Wiberg’s text and figures describe the lateral boundary of the acetabular sourcil, the sclerotic line along the acetabular roof. However, others have interpreted Wiberg’s description to mean the lateral edge of the bone [4]. Notably, Ogata et al. reported that the lateral edge of the bone, used to measure Wiberg’s LCEA, is difficult to clearly define in pediatric hip dysplasia patients and proposed a ‘refined’ LCEA measured to the lateral point of bony condensation of the roof [4]. Ogata’s description highlights the confusion when measuring the LCEA.
Regardless if Wiberg intended the LCEA to be measured to the most lateral bone edge or sourcil boundary, both methods have been used to evaluate acetabular coverage in recent literature. Specifically, articles citing Wiberg’s 1939 article fall into three groups: those that do not include a clear text or figure example of how the LCEA was measured [3, 5–8], those that include a figure or diagram depicting the LCEA extending to the lateral edge of the acetabulum/bone [9–13] and those that illustrate and/or describe measuring to the sclerotic edge or sourcil [14–18]. Similar discrepancies exist for the ACEA, with descriptions of measurements to the bone edge [9, 19] and to the sclerotic edge [15, 16, 20, 21]. While the bone and sourcil edge measurements may be equivalent in some patients, this is not always the case in pediatric hip dysplasia patients [22]. However, it is unknown if the two methods could be used interchangeably in adult patients. Further, limited data exists comparing the measurements of the ACEA between methods [23].
Thus, the objective of this study was to compare the two methods, specifically the bone edge method and the sourcil edge method, of measuring the LCEA and ACEA in a retrospective review of radiographs from a symptomatic adult population. While detecting a statistically significant difference was important, we also wanted to evaluate if the difference in measurement methods was clinically significant. We believe a difference greater than 5° qualifies as being clinically significant, as a clinician using one measurement method could diagnose a hip as dysplastic (LCEA < 20°), while a clinician using the second method could classify the same hip as normal (LCEA > 25°) [1]. We hypothesized that there would be a statistically, and clinically, significant difference between the two methodologies.
MATERIALS AND METHODS
Preoperative standing AP and FP radiographs, obtained between July 2008 and September 2011 of adult patients (>18 years) who subsequently underwent arthroscopy by the senior author for hip pathomorphology, were reviewed for this study. Only the surgical hip was included in the analysis. For 17 subjects with bilateral symptoms, the first hip surgically treated was included.
An orthopaedic physician’s assistant (KMS) and a second year medical student (JAH) were trained by the senior author (SKA) and completed the radiographic measurements independently. The LCEA was measured on AP radiographs (Fig. 1) and the ACEA was measured on FP radiographs (Fig. 2). The LCEA and ACEA were measured to both to the edge of the bone and to the edge of the sourcil. To obtain the LCEA, the center of the femoral head was estimated from a circle fit to the medial and inferior contour of the femoral head. The longitudinal axis of the body was defined perpendicular to a line connecting the inferior ischial tuberosities. An alternative method (while not utilized herein) would be to define the longitudinal axis perpendicular to a line connecting the inferior margins of bilateral acetabular teardrops. The LCEA was measured between a line from the center of the femoral head parallel to the longitudinal axis and a line from the center of the femoral head to the most lateral aspect of the bone or the sourcil edge. A similar method was used to measure the bone and sourcil ACEAs on the FP radiograph (Fig. 2). However, for the ACEA, the longitudinal axis was defined by a vertical line on the radiograph.
Fig. 1.

Lateral center edge angle (LCEA) measured on an anteroposterior radiograph of a 40-year-old female. To obtain the LCEA, the center of the femoral head was estimated from a circle fit to the medial and inferior contour of the femoral head. The longitudinal axis of the body was defined perpendicular to a line connecting the inferior ischial tuberosities. The LCEA was measured between the line from the center of the femoral head parallel to the longitudinal axis and the line from the center of the femoral head to the most lateral aspect of the bone or the sourcil edge. The patient’s right hip can be classified as normal based on a sourcil (S) LCEA of 28°, but overcovered based on a bone (B) LCEA of 43°.
Fig. 2.

Anterior center edge angle (ACEA) measured on false profile radiograph of an 18-year-old female. To obtain the ACEA, the center of the femoral head was estimated from a circle fit to the medial and inferior contour of the femoral head. The ACEA was measured between a vertical line on the image and the line from the center of the femoral head to the most lateral aspect of the bone (B) or the sourcil (S) edge. For this patient, the bone VCA was 46° and the sourcil VCA was 34°.
The lateral coverage of each hip was classified using both the bone and sourcil LCEAs as follows: <20° dysplastic, ≥20° and ≤25° borderline dysplastic, >25° and ≤40° normal, and >40° over-covered [1, 24]. Anterior coverage was classified with the bone and sourcil ACEAs as follows: <20° under-covered, ≥20° and ≤40° normal, >40° over-covered [15, 16].
All statistical analyses were completed in Stata/MP 13.0 (StataCorp LP, College Station, TX, USA). Interobserver repeatability was assessed with the intraclass correlation coefficient, interpreted as follows: minimal <0.2, poor 0.2–<0.4, moderate 0.4–<0.6, strong 0.6–≤0.8 and almost perfect >0.8 [25]. Angles were averaged between the two observers for subsequent analysis. A paired t-test was used to identify differences in the LCEA and ACEA between the bone and sourcil measurement methods. Bland–Altman plots were generated to compare measurement methods [26].
RESULTS
Preoperative AP radiographs were available for 188 subjects (109 female, 36.6 ± 11.4 years). Preoperative FP radiographs were available for 137 subjects (72 female, 35.9 ± 11.5 years).
Interobserver agreement was almost perfect for all radiographic measurements: bone LCEA = 0.92, sourcil LCEA = 0.92, bone ACEA = 0.91 and sourcil ACEA = 0.89.
Bone and sourcil measurements of the LCEA and ACEA were significantly different (both p < .001). On average, the bone LCEA was 4° (95% limits of agreement = −2° to 10°) greater than the sourcil LCEA (Fig. 3). The bone ACEA was, on average, 10° (95% limit of agreement = −2° to 22°) greater than the sourcil ACEA (Fig. 4).
Fig. 3.

Bland–Altman plot comparing the sourcil and bone measurements of the lateral center edge angle (LCEA).
Fig. 4.

Bland–Altman plot comparing the sourcil and bone measurements of the anterior center edge angle (ACEA).
Forty-six subjects (46/188, 24%) had a LCEA difference greater than 5° between methods. 107/137 (78%) subjects had an ACEA difference greater than 5° between methods. In contrast, the difference between methods was less than 1° in 47/188 (25%) subjects for the LCEA (Fig. 5) and 8/137 (6%) subjects for the ACEA.
Fig. 5.

Anteroposterior radiograph of a 26-year-old male demonstrating an equivalent bone (B) and sourcil (S) center edge angles of 31° for the right hip.
Differences in the bone and sourcil measurements of the LCEA and ACEA often led to different clinical classifications for the same hip (Tables I and II). For example, the 14 subjects with a sourcil LCEA <20° (dysplastic), only four had a bone LCEA also <20°. Similarly, of the 54 subjects with a sourcil LCEA ≤ 25° (dysplastic or borderline dysplastic), 32 had a sourcil LCEA > 25° (normal) (Table I). Six subjects had a bone LCEA > 25° (normal) but a sourcil LCEA < 20° (dysplastic) (Fig. 6). Of the 20 subjects with a bone LCEA > 40° (over-covered), 11 had a sourcil LCEA ≤ 40° (normal) (Fig. 1). Finally, all seven patients with a sourcil ACEA < 20° (dysplastic) had a bone ACEA ≥ 20° (normal), while only 12 of the 65 hips with a bone ACEA > 40° had a sourcil ACEA also > 40° (Table II).
Table I.
Number of hips in each clinical classification category according to LCEA measured to the sourcil edge and bone edge
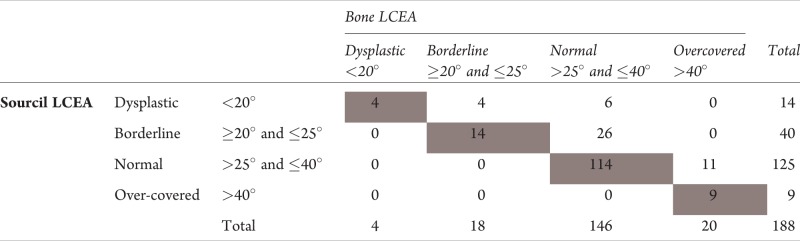 |
Hips in shaded cells along the diagonal have bone and sourcil LCEAs that fall into the same category.
Table II.
Number of hips in each clinical classification category according to ACEA measured to the sourcil edge and bone edge
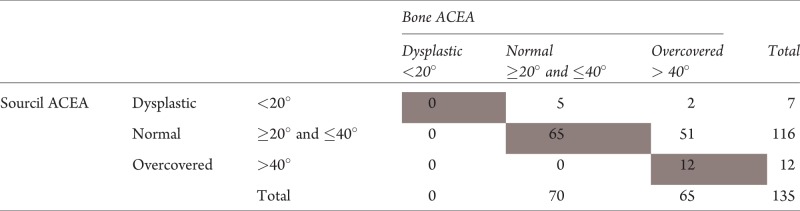 |
Hips in shaded cells along the diagonal represent have bone and sourcil ACEAs that fall into the same category.
Fig. 6.

Anteroposterior radiograph of a 43-year-old female. The patient’s right hip can be classified as normal based on a bone (B) center edge angle of 27°, but dysplastic based on a sourcil (S) center edge angle of 18°.
DISCUSSION
Discrepancies in the methodology to quantify acetabular coverage of the femoral head with the LCEA and ACEA exist in current literature. Specifically, these radiographic angles have been calculated from the longitudinal axis of the body to either the edge of the lateral acetabular bone boundary or to the lateral edge of the sclerotic sourcil. The objective of this study was to compare the bone edge and sourcil edge methods in an adult population with hip complaints and illustrate how discrepancies could affect the classification of hip coverage. We found that the bone edge measurements were significantly greater than the sourcil edge measurements. This difference was clinically significant (greater than 5°) in 24% of LCEA measurements and 78% of ACEA measurements.
While the average difference in LCEA between the bone and sourcil methods was only 4°, almost a quarter of hips analyzed had a difference greater than 5° between methods. To illustrate the clinical significance of these findings, consider a patient with a bone LCEA measuring 30° and a sourcil LCEA measuring 19° (Fig. 6). Using the bone LCEA, the hip would be classified as normal [1]. However, the sclerotic LCEA would indicate this hip is dysplastic [1] and could possibly benefit from a periacetabular osteotomy [27]. Our data showed that this was the case for six hips analyzed herein, representing 43% of hips with a sourcil LCEA less than 20°. In contrast, consider an individual with a bone LCEA of 43° and a sourcil LCEA of 28° (Fig. 1). Using the bone LCEA, the patient would potentially qualify for an acetabuloplasty to address pincer femoroacetabular impingement [28], although the sourcil edge measurement would suggest normal acetabular coverage. Nearly half the hips analyzed herein with a bone LCEA greater than 40° had a sourcil LCEA less than 40°. Nonetheless, we acknowledge that the LCEA is rarely used alone in the diagnosis and treatment selection of patients with suspected hip pathomorphology. The determination of under- or over-coverage should be made in the context of other radiographic or 3D imaging measures, the patient history and clinical exam findings.
To our knowledge, the only published comparisons of the bone and sourcil LCEA measurements have been completed in pediatric patients with developmental dysplasia of the hip. Nearly half of the 56 hips analyzed by Ogata et al. had equivalent bone and sourcil measurements, while the remaining exhibited an average difference of ∼10° [4]. In the latter cases, the authors suggested the difference could be caused by an oblique or irregular acetabulum in which the most lateral portion of the acetabular rim was found anterior to the most superior portion of the roof. Omeraglu et al. identified an average difference of 8.3° in patients <20 years, but found the difference was more pronounced in younger patients (13.2° in 3–8 year olds) than older patients (5.7° in 9–18 year olds) [22]. Similarly, Kim et al. reviewed sequential radiographs of dysplastic patients and found that the average difference in bone and sourcil measurements decreased from 5.8° at age 4 to 2.3° at age 12 [29]. They suggested that the sourcil LCEA corresponds to the lateral edge of the mid-superior portion of the acetabulum and that the bone LCEA corresponds to the anterolateral portion of the acetabulum [29]. Further research is needed to determine if these previous suggestions also explain the differences in bone and sourcil measurements in adult hips. Other explanations, such as osteophyte formation at the lateral aspect of the acetabulum [30, 31], may also contribute to the differences observed in the adult population.
In this study, the average difference between the bone and sourcil ACEA measurements was 10° and 78% of patients had a difference greater than 5°. These discrepancies were greater than those observed for the LCEA. Li et al. notes that it is difficult to establish the rotation of the pelvis during the acquisition of false-profile radiographs [32]. It is possible that subtle differences in rotational positioning amongst subjects may contribute to greater differences in the appearance and location of bone edge and sourcil edge observed in false profile compared to AP radiographs. Clinically, all hips classified herein as dysplastic according to their sourcil ACEA would be considered normal according to their bone ACEA [2, 19, 23]. Sakai et al. found that in female patients with hip pain but normal lateral coverage (LCEA >20°), the bone ACEA more accurately represented actual anterior coverage as quantified using 3D CT reconstructions [23]. However, in patients with insufficient lateral coverage (LCEA <20°), neither the bone nor sourcil ACEAs accurately quantified anterior coverage [23].
Our data for both the LCEA and ACEA showed high interobserver repeatability with similar ICCs for the two methods. In comparison, Omereglu et al. concluded that measuring the LCEA to the edge of the bone had slightly higher intraobserver and interobserver agreement (3.1° and 4.0° respectively) than using the sclerotic edge method (3.8° and 5.1°, respectively). Sakai et al., found that the bone ACEA was more repeatable (inter and intraobserver r = 0.88–0.90) than the sourcil ACEA (inter and intraobserver r = 0.64–0.77).
This study has a few limitations that warrant discussion. First, radiographs were not corrected or standardized for pelvic tilt. However, recent studies have shown that changes in pelvic tilt do not cause clinically significant differences in the LCEA [33–35]. In addition, all radiographs were obtained in the standing position. This functional position has been suggested to reduce confounding in ACEA measurements due to variable pelvic tilt [20]. Next, there were limited subjects with dysplasia (only 14 had sourcil LCEA <20° sclerotic) and pincer FAI (only 20 patients with bone LCEA >40°). Most of the subjects evaluated herein fell within the normal range of LCEA and therefore, would be less affected (in terms of radiographic preoperative planning) by discrepancies in the measurement techniques. However, there was no significant linear relationship between the difference and average of the bone and sourcil measurements [26]. Therefore, the differences between measurement methods appear to be consistent over the range of hip classifications. Finally, three-dimensional imaging, which may help identify the anatomical features resulting in the discrepancy between methods, was not evaluated.
In conclusion, although we found that the bone edge and sourcil edge methods for measuring the LCEA and ACEA are repeatable, there was a statistically and clinically significant difference between the two in adult patients with suspected hip pathomorphology. Specifically, the bone edge measurements were significantly greater on average, and this difference often led to different clinical classifications for the same hip. As we believe Wiberg originally described the measurement of LCEA to the edge of the sourcil [1], and previous studies comparing the measurements have found that the bone LCEA may overestimate coverage in children with dysplasia [4, 22], we suggest measuring the LCEA to the edge of the sourcil. However, further investigation is needed to determine which measurement method is a more accurate representation of acetabular coverage. Further studies should also focus on determining how the two measurements correlate with three-dimensional acetabular morphology, as it is possible both measurements may be important in identifying coverage in different regions of the acetabulum (i.e. anterior, central, posterior). With respect to the ACEA, Sakai et al. suggest that the bone edge is more representative of true acetabular coverage in normal hips [23]. Nonetheless, when using the LCEA and ACEA clinically, these measures should be interpreted in the context of the patient history, physical exam findings and other radiographic or three-dimensional imaging measures to determine the appropriate diagnosis and treatment. Finally, when reporting these angles, it should be mandatory to clearly identify with a text description and/or radiographic figure which method is being used to estimate acetabular coverage.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
- 1.Wiberg G. Studies on dysplastic acetabula and congenital subluxation of the hip joint: with special reference to the complication of osteoarthritis. Acta Chir Scand 1939; 83(Suppl 58): 1–135. [Google Scholar]
- 2.Lequesne M, de S. False profile of the pelvis. A new radiographic incidence for the study of the hip. Its use in dysplasias and different coxopathies. Rev Rhum Mal Osteoartic 1961; 28: 643–52. [PubMed] [Google Scholar]
- 3.Ross JR, Zaltz I, Nepple JJ, et al. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med 2011; 39(Suppl): 72s–8s. [DOI] [PubMed] [Google Scholar]
- 4.Ogata S, Moriya H, Tsuchiya K, et al. Acetabular cover in congenital dislocation of the hip. J Bone Joint Surg Br 1990; 72: 190–6. [DOI] [PubMed] [Google Scholar]
- 5.Nepple JJ, Brophy RH, Matava MJ, et al. Radiographic findings of femoroacetabular impingement in National Football League Combine athletes undergoing radiographs for previous hip or groin pain. Arthroscopy 2012; 28: 1396–403. [DOI] [PubMed] [Google Scholar]
- 6.Polkowski GG, Novais EN, Kim YJ, et al. Does previous reconstructive surgery influence functional improvement and deformity correction after periacetabular osteotomy? Clin Orthop Relat Res 2012; 470: 516–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kappe T, Kocak T, Bieger R, et al. Radiographic risk factors for labral lesions in femoroacetabular impingement. Clin Orthop Relat Res 2011; 469: 3241–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ross JR, Nepple JJ, Baca G, et al. Intraarticular abnormalities in residual Perthes and Perthes-like hip deformities. Clin Orthop Relat Res 2012; 470: 2968–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dolan MM, Heyworth BE, Bedi A, et al. CT reveals a high incidence of osseous abnormalities in hips with labral tears. Clin Orthop Relat Res 2011; 469: 831–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Philippon MJ, Wolff AB, Briggs KK, et al. Acetabular rim reduction for the treatment of femoroacetabular impingement correlates with preoperative and postoperative center-edge angle. Arthroscopy 2010; 26: 757–61. [DOI] [PubMed] [Google Scholar]
- 11.Al-Ghamdi A, Rendon JS, Al-Faya F, et al. Dega osteotomy for the correction of acetabular dysplasia of the hip: a radiographic review of 21 cases. J Pediatr Orthop 2012; 32: 113–20. [DOI] [PubMed] [Google Scholar]
- 12.Hosalkar H, Munhoz da Cunha AL, Baldwin K, et al. Triple innominate osteotomy for Legg-Calve-Perthes disease in children: does the lateral coverage change with time? Clin Orthop Relat Res 2012; 470: 2402–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Werner CM, Copeland CE, Ruckstuhl T, et al. Relationship between Wiberg's lateral center edge angle, Lequesne's acetabular index, and medial acetabular bone stock. Skeletal Radiol 2011; 40: 1435–9. [DOI] [PubMed] [Google Scholar]
- 14.Sankar WN, Brighton BK, Kim YJ, et al. Acetabular morphology in slipped capital femoral epiphysis. J Pediatr Orthop 2011; 31: 254–8. [DOI] [PubMed] [Google Scholar]
- 15.Anderson LA, Gililland J, Pelt C, et al. Center edge angle measurement for hip preservation surgery: technique and caveats. Orthopedics 2011; 34: 86. [DOI] [PubMed] [Google Scholar]
- 16.Clohisy JC, Carlisle JC, Beaule PE, et al. A systematic approach to the plain radiographic evaluation of the young adult hip. J Bone Joint Surg Am 2008; 90(Suppl 4): 47–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hansen BJ, Harris MD, Anderson LA, et al. Correlation between radiographic measures of acetabular morphology with 3D femoral head coverage in patients with acetabular retroversion. Acta Orthop 2012; 83: 233–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jessel RH, Zurakowski D, Zilkens C, et al. Radiographic and patient factors associated with pre-radiographic osteoarthritis in hip dysplasia. J Bone Joint Surg Am 2009; 91: 1120–9. [DOI] [PubMed] [Google Scholar]
- 19.Crockarell JR, Jr., Trousdale RT, Guyton JL. The anterior centre-edge angle. A cadaver study. J Bone Joint Surg Br 2000; 82: 532–4. [DOI] [PubMed] [Google Scholar]
- 20.Zingg PO, Werner CM, Sukthankar A, et al. The anterior center edge angle in Lequesne's false profile view: interrater correlation, dependence on pelvic tilt and correlation to anterior acetabular coverage in the sagital plane. A cadaver study. Arch Orthop Trauma Surg 2009; 129: 787–91. [DOI] [PubMed] [Google Scholar]
- 21.Chosa E, Tajima N. Anterior acetabular head index of the hip on false-profile views. New index of anterior acetabular cover. J Bone Joint Surg Br 2003; 85: 826–9. [PubMed] [Google Scholar]
- 22.Omeroglu H, Bicimoglu A, Agus H, et al. Measurement of center-edge angle in developmental dysplasia of the hip: a comparison of two methods in patients under 20 years of age. Skeletal Radiol 2002; 31: 25–9. [DOI] [PubMed] [Google Scholar]
- 23.Sakai T, Nishii T, Sugamoto K, et al. Is vertical-center-anterior angle equivalent to anterior coverage of the hip? Clin Orthop Relat Res 2009; 467: 2865–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Anderson LA, Peters CL, Park BB, et al. Acetabular cartilage delamination in femoroacetabular impingement. Risk factors and magnetic resonance imaging diagnosis. J Bone Joint Surg Am 2009; 91: 305–13. [DOI] [PubMed] [Google Scholar]
- 25.Rosenkrantz AB, Lim RP, Haghighi M, et al. Comparison of interreader reproducibility of the prostate imaging reporting and data system and likert scales for evaluation of multiparametric prostate MRI. AJR Am J Roentgenol 2013; 201: W612–8. [DOI] [PubMed] [Google Scholar]
- 26.Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res 1999; 8: 135–60. [DOI] [PubMed] [Google Scholar]
- 27.Cooperman DR, Wallensten R, Stulberg SD. Acetabular dysplasia in the adult. Clin Orthop Relat Res 1983; 175: 79–85. [PubMed] [Google Scholar]
- 28.Matsuda DK, Gupta N, Hanami D. Hip arthroscopy for challenging deformities: global pincer femoroacetabular impingement. Arthrosc Tech 2014; 3: e197–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kim HT, Kim JI, Yoo CI. Diagnosing childhood acetabular dysplasia using the lateral margin of the sourcil. J Pediatr Orthop 2000; 20: 709–17. [DOI] [PubMed] [Google Scholar]
- 30.Arden N, Nevitt MC. Osteoarthritis: epidemiology. Best Pract Res Clin Rheumatol 2006; 20: 3–25. [DOI] [PubMed] [Google Scholar]
- 31.Jacobson JA, Girish G, Jiang Y, et al. Radiographic evaluation of arthritis: degenerative joint disease and variations. Radiology 2008; 248: 737–47. [DOI] [PubMed] [Google Scholar]
- 32.Li PL, Ganz R. Morphologic features of congenital acetabular dysplasia: one in six is retroverted. Clin Orthop Relat Res 2003; 416: 245–53. [DOI] [PubMed] [Google Scholar]
- 33.Tannast M, Fritsch S, Zheng G, et al. Which radiographic hip parameters do not have to be corrected for pelvic rotation and tilt? Clin Orthop Relat Res 2015; 473: 1255–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Troelsen A, Jacobsen S, Romer L, et al. Weightbearing anteroposterior pelvic radiographs are recommended in DDH assessment. Clin Orthop Relat Res 2008; 466: 813–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Pullen WM, Henebry A, Gaskill T. Variability of acetabular coverage between supine and weightbearing pelvic radiographs. Am J Sports Med 2014; 42: 2643–8. [DOI] [PubMed] [Google Scholar]