

Abstract
Background
Active commuting to school (ACS) increases students' daily physical activity, but associations between student weight and ACS are inconsistent. Few studies examining ACS and weight account for distance commuted. This study examines the association between students' weight status and ACS, taking into account distance to school.
Methods
In 2009–10 a random digit-dial household survey conducted in low-income minority cities collected information about ACS for 1 randomly selected school-going student per household. Parents provided measured heights and weights. Distance commuted was obtained using geocoded home and school addresses. Multivariate regression analyses assessed associations of ACS and distance commuted with weight status.
Results
36.6% of students were overweight/obese; 47.2% engaged in ACS. Distance walked/biked to school was associated with 7% lower odds of overweight/obesity (OR = 0.93, 95% CI: 0.88–0.99). Without distance commuted in the model, ACS was not associated with students' weight status. Compared with no ACS, ACS greater than a half-mile was associated with 65% lower odds of a student being overweight/obese (OR = 0.35, 95% CI: 0.16–0.78); ACS less than a half-mile was not.
Conclusions
ACS is significantly inversely associated with overweight/obesity among students who commute beyond a one-half mile threshold.
Keywords: walking school bus, overweight/obesity, physical activity
The prevalence of childhood obesity in the US has risen from approximately 6% in 19801 to its current 2014 rate of about 17%.2 Cross-sectional studies show an inverse association between objectively measured physical activity (PA) and measures of weight status in children.3 However, only 42% of 6- to 11-year-old children, and 8% of adolescents4 meet the PA recommendation of accumulating 60 or more minutes of moderate or vigorous activity each day.5
The 2010 White House Task Force on Childhood Obesity recognized children's daily commute to and from school as a natural, nonstructured opportunity to increase students' PA, and recommended setting a goal of a 50% increase by 2015 in the number of 5- to 18-year-old students walking or bicycling to and from school.6 This would result in 19.5% of trips to/from school being taken by walking, bicycling, skateboarding, or some other form of active transportation6 as opposed to the current rate of 12.7%.7
Students who engage in active commuting to school (ACS) have been shown to accumulate significantly more PA than do nonactive commuters.8,9 Research on the impact of ACS on children's body weight status, however, is not conclusive.10–20 A deeper understanding of contextual factors related to ACS is critical to successfully implement recommendations such as those put forth by the White House Task Force.6 For example, the design of interventions aimed at improving ACS to impact PA and weight status would benefit from assessments that examine how ACS affects students in different demographic groups, and how far and how frequently students must actively commute to achieve the desired benefits.
Frequency, duration, and intensity of PA are the 3 components that impact energy expenditure. While measuring the intensity of each student's active commute to school would be difficult, most children walk (the primary form of ACS7) at similar intensities,21 eliminating the need to include intensity as a covariate. However, the frequency with which students actively commute and the duration of the commute differ widely among students. A number of studies examining the association between ACS and weight status quantify the frequency with which students actively commute,10,18 but accounting for distance (a proxy for duration of the commute) is more challenging.11,15,20
This study addresses an important gap in the literature by not only examining the difference in weight status between students who do and do not actively commute, but by also investigating the association of weight status with objectively measured distances students actively commute between home and school. We hypothesized that greater distances of ACS would be associated with lower rates of overweight/obesity.
Methods
Household Survey
The data for this study were collected in 2009–10 from a random-digit-dial sample of 1408 households with landline telephones in 4 low-income cities in New Jersey (Camden, Newark, New Brunswick, and Trenton), having at least 1 child in the age range of 3 to 18 years. Survey questions focused on a randomly selected child (index child) from each household. Telephone interviews were conducted in either English or Spanish using a multicall design. The survey was implemented from June 2009 through March 2010. Participants were offered an incentive of $10 for completing the survey. The respondent was the adult who made most of the decisions about food shopping for the household (in 94% of the cases, this was the parent).
Survey questions used in the analysis include demographics, child food consumption and screen time behaviors, child's home address, and name of the child's school. Child's home and school location were geocoded for calculating distance between home and school. In this paper the child is referred to as ‘student.’ Survey fieldwork and initial geocoding were carried out by Abt SRBI Inc. Using standard calculations22 the survey had a response rate of 49%, which is similar to the response rate of 50.2% from the Center for Disease Control's (CDC) New Jersey Behavioral Risk Factor Surveillance System (BRFSS) for 2010.23
At the conclusion of the survey, respondents were asked to participate in a follow-up study in which they weighed and measured themselves and their children using instructions based on CDC guidelines,24 and a tape measure mailed to their homes along with a reporting worksheet. Parent-measured heights and weights of children have been reported to be highly correlated with professionally measured values25 and are more accurate than are parent-reported estimates.26 An additional $10 incentive was offered for completion of this task. Of the surveyed households who provided their mailing addresses, 40.5% (485 households) returned completed worksheets with measured heights and weights for the index child. As shown in Table 1, there were no statistical differences in the student- and parent-level characteristics between students whose parents provided measured heights and weights compared with those in the full sample. This study was approved by the Institutional Review Boards of Rutgers University and Arizona State University. Participants provided informed consent before the start of the study.
Table 1. Description and Comparison of Explanatory Variables in the Full Sample and in the Subsample of Students for Whom Parent-Measured Heights and Weights Data Were Available.
| Full sample (n = 1408) | Sample with parent-measured student heights and weights (n = 485) | P | |
|---|---|---|---|
| City (%) | .41 | ||
| Camden | 28.4 | 27.0 | |
| Newark | 28.4 | 28.2 | |
| New Brunswick | 14.8 | 17.9 | |
| Trenton | 28.4 | 24.8 | |
| Age (years) | 10.6 ± 4.6 | 10.6 ± 4.5 | .99 |
| Females (%) | 48.6 | 48.2 | .94 |
| Race/Ethnicity (%) | .66 | ||
| Non-Hispanic white | 6.2 | 6.6 | |
| Non-Hispanic black | 48.2 | 48.9 | |
| Hispanic | 42.1 | 40.0 | |
| Other | 3.5 | 4.5 | |
| ≤200% federal poverty level (%) | 72.3 | 73.2 | .75 |
| Mother's education (%) | .95 | ||
| High school or less | 60.6 | 60.0 | |
| Some college | 24.0 | 24.1 | |
| College + | 15.3 | 15.9 | |
| Parent acculturation (%) | 1.00 | ||
| US born | 71.3 | 71.5 | |
| In US ≥ 10 yrs | 22.0 | 21.9 | |
| In US < 10 yrs | 6.7 | 6.6 | |
| Parent BMI (kg/m2) | 30.1 ± 7.3 | 30.1 ± 7.3 | .97 |
| Never actively commute to school (%) | 56.3 | 52.8 | .20 |
| Distance to school (miles) | 1.31 ± 1.1 | 1.22 ± 1.1 | .25 |
| Weekday screen time >2 hrs (%) | 30.4 | 34.7 | .35 |
| Fruit & vegetable consumption (times/day) | 4.44 ± 2.9 | 4.55 ± 3.1 | .46 |
| Fast food consumption (times/week) | 1.13 ± 1.5 | 1.17 ± 1.5 | .56 |
| Fruit favored drink consumption (times/day) | 0.89 ± 1.4 | 0.85 ± 1.3 | .63 |
| Soft drink consumption (times/day) | 0.32 ± 0.77 | 0.29 ± 0.56 | .47 |
Outcome Measures
The outcome variable was a dichotomous indicator of overweight/obese vs normal weight status. This classification was based on the age- and sex-specific percentile of the student's BMI, calculated with the measured height and weight provided on the parents' worksheet and the 2000 CDC Growth Charts.27 Students with a BMI below the 85th percentile are considered normal weight. Those at or above the 85th percentile are classified as overweight/obese. Students with any measured or calculated value identified as biologically implausible28 were excluded from the analysis.
Independent Variables
Parents were asked, “On how many days during a typical week does the index child walk, bicycle, or skateboard to or from school?” Similar questions have been used by most studies that examine the association between weight status and ACS,17,18,29–32 and have moderate test retest reliability (Kappa = 0.60).29 The distribution of responses was bimodal, with 53% answering 0 days/week, and 41% answering 5 days/week. Therefore, instead of using frequency of ACS as a continuous variable, and similar to other studies,11,29,30,33–38 actively commuting students (coded as 1) were defined as those who engaged in ACS 1 or more days per week, while those who never walked, bicycled, or skateboarded were coded as 0.
Distance to school for each student was calculated in roadway network miles based on the geocoded address of the home and school using ArcGIS software. A continuous ‘distance traveled’ variable was created by multiplying presence or absence of ACS (yes = 1; no = 0) by distance in tenths of a mile from a student's home to school. Distance traveled therefore captured the distance that active commuters traveled to school if they took the most direct roadway route, with a value of 0 for nonactive commuters. Descriptive and bivariate statistics are presented using distance in miles. For all multivariate models, distance was computed in units representing one-tenth of a mile.
When examining the effect of distance thresholds on overweight/obesity, sensitivity analyses were conducted by including only active commuters living at various distances from school, beginning with 1.5 miles and decreasing in 0.25 mile increments, in the model. One-half mile was the shortest distance at which significance was found. Therefore nonactive commuters, ≤0.5 mile commuters, and >0.5 mile commuters were entered into a logistic regression model to determine whether rates of overweight/obesity differed among these 3 conditions.
Covariates
Demographics
Demographic variables included the student's age in years; student's gender; mother's education (high school [referent], some college, college and advanced); student's race/ethnicity (non-Hispanic white [referent], non-Hispanic black, Hispanic, other); family income as a ratio of the US federal poverty level (FPL) (≤200% or >200% of FPL); number of years the parent has resided in the US as a measure of acculturation (US born [referent], <10 years in the US, ≥10 years in the US); parent's BMI; and city of residence (Newark [referent], Camden, New Brunswick, Trenton). Student race/ethnicity was determined based on parents' responses to survey questions about the child's ethnicity (Hispanic or not) and race (black/African American, white, American Indian/Native American/Alaskan or Eskimo, Asian/Pacific Islander, and other), which were later combined into the 4 student race/ethnicity categories described above. City of residence was included only to control for city-specific effects including policies (not captured in these data) associated with ACS.
Food Consumption and Physical Activity Measures
Daily screen time was assessed by survey questions about the number of hours each day students spent watching television, playing video games, or using a computer other than for schoolwork. Assessments about food consumption were made by asking how often the student ate specific fruits and vegetables each day, how many times per week the student ate at a fast food restaurant, and how many times per day the student drank sugar-sweetened beverages. These questions were modeled after the food frequency questions used in the BRFSS39 and also derived from previous research.40
Statistical Analysis
The final analytical sample excluded students with CDC-determined biologically implausible values for height-for-age, weight-for-age, or BMI (n = 40);28 who were not attending a school, were home schooled, or who were younger than 5 years old (n = 40); whose parents did not provide a home address or school address (n = 113); and who had missing values for other variables included in the analyses (Figure 1).
Figure 1.
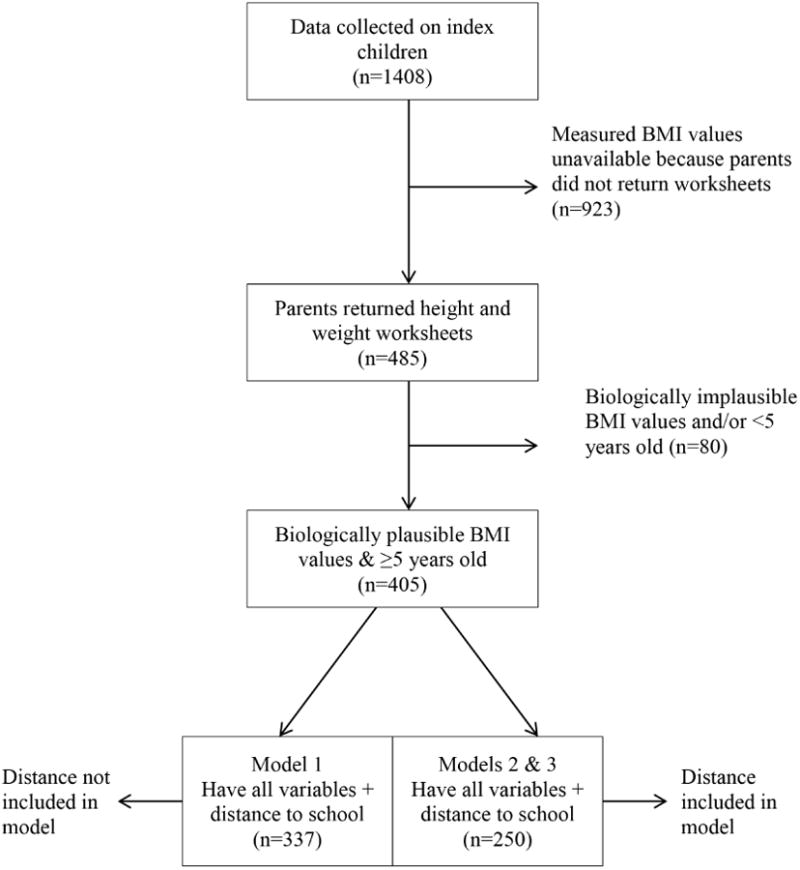
Flow diagram of participants included in the current analysis.
Comparisons between the full sample (n = 1408) and the sample with measured BMI values (n = 485), as well as comparisons between ACS (n = 210) and non-ACS (n = 189) were assessed using independent samples t-tests for continuous variables and chi-square tests for categorical variables.
Multivariate logistic regression analyses were used to examine associations of ACS and distance commuted with students' overweight/obese status. All models adjusted for city of residence, student's age, student's race/ethnicity, household income, parent's BMI, mother's education, acculturation, sedentary behavior (daily screen time), and dietary behaviors (fruit and vegetable intake, fast food consumption, and sugar-sweetened beverage consumption).
Clustering at the school level was not anticipated because of the sampling design. This was confirmed by the fact that the 485 students with measured heights and weights attended 125 different schools, with the vast majority of schools attended by only 1 to 5 students. Data were adjusted for the complex survey design using the svy command in Stata (version 12.0), specifying the student as the unit of analysis and adjusting for clustering of the sample at the city level. Significance was set at the P < .05 level.
Results
Table 2 presents unadjusted comparisons between students who engaged in ACS with those who did not. Active commuters were significantly older than and lived closer to school than did nonactive commuters (11.9 yrs vs 11.0 yrs [P < .05] and 0.96 miles vs 1.55 miles [P < .001], respectively). Significant differences were also observed by household income and mother's education level; students from higher income households and from households with higher levels of mother's education showed lower rates of ACS. There were no significant differences in overweight/obesity prevalence between ACS and non-ACS students.
Table 2. Unadjusted Comparisons of Active Commuting and Nonactive Commuting Students.
| % or mean (SD) of each category: ACS (n = 210) | % or mean (SD) of each category: non-ACS (n = 189) | Pa | |
|---|---|---|---|
| Child BMI category | |||
| <85th percentile | 48.4 | 51.6 | .585 |
| ≥85th percentile | 45.6 | 54.4 | |
| Demographics | |||
| Age | |||
| Mean (years) | 11.9 (3.9) | 11.0 (4.0) | .029 |
| 5–11 years | 42.1 | 57.9 | .039 |
| 12–19 years | 52.5 | 47.5 | |
| Sex | |||
| Female | 48.4 | 51.6 | .681 |
| Male | 46.4 | 53.6 | |
| Race/Ethnicity | |||
| Non-Hispanic white | 46.7 | 53.3 | .998 |
| Non-Hispanic black | 47.2 | 52.8 | |
| Hispanic | 47.9 | 52.1 | |
| Other | 46.1 | 54.9 | |
| Household income | |||
| ≤ 200% federal poverty level | 53.1 | 46.9 | <.001 |
| >200% federal poverty level | 32.7 | 67.3 | |
| Mother's education | |||
| High school or less | 56.0 | 44.0 | <.001 |
| Some college | 41.4 | 58.6 | |
| College + | 24.6 | 75.4 | |
| Parent acculturation | |||
| US born | 47.7 | 52.3 | .984 |
| In US ≥10 years | 47.1 | 53.0 | |
| In US <10 years | 46.1 | 53.9 | |
| Parent BMI (kg/m2) | 30.9 (7.5) | 29.7 (6.9) | .126 |
| Commuting | |||
| Distance to school | |||
| Mean (miles) | 0.90 (0.96) | 1.55 (1.09) | <.001 |
| Food consumption/sedentary behaviors | |||
| Screen time | |||
| Mean (hrs per week) | 20.1 (13.1) | 17.8 (12.1) | .077 |
| Fruit & vegetable consumption | |||
| Mean (number per day) | 4.0 (2.1) | 4.3 (2.2) | .153 |
| Fast food consumption | |||
| <1 time per week | 51.2 | 48.8 | .166 |
| ≥1 time per week | 44.2 | 55.8 | |
| Sugar-sweetened beverage consumption | |||
| <1 per day | 46.5 | 53.5 | .677 |
| ≥1 per day | 48.7 | 51.4 |
For categorical variables, P-values indicate whether a significant difference exists between groups in each category concerning whether students engage in ACS or not. For continuous variables, P-values indicate whether a significant difference exists between students who engage in ACS and students who do not.
Figure 2 illustrates the percent of students at each distance who actively commuted to school. The percent of students actively commuting decreased with each quarter-mile increase in distance from home to school. Prevalence of ACS did not vary significantly among students who lived at distances less than a half-mile from school (≤0.25, >0.25 to 0.5); students who lived farther than a half-mile from school (>0.5 to 0.75, >0.75 to 1, >1) had significantly lower ACS rates compared with those who lived at shorter distances.
Figure 2.
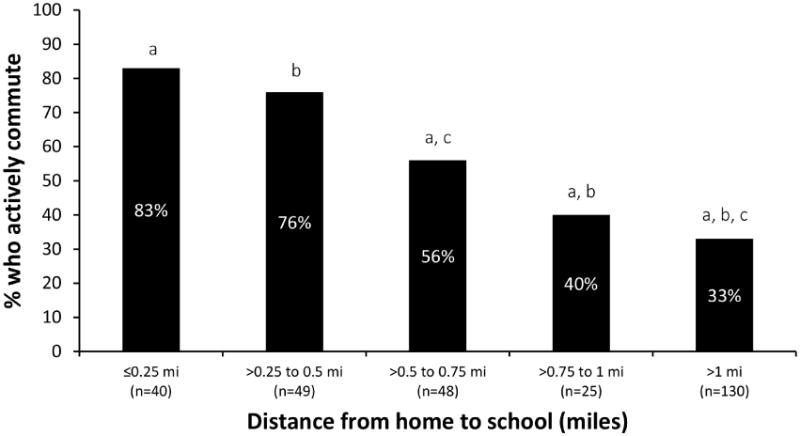
Percent of actively commuting students living at different distances from school. Significant differences were observed between bars marked with same letter.
Figure 3 shows the percentage of students who were overweight/obese under 3 different conditions. Forty percent of students who did not engage in ACS (n = 142; distance = 0 miles) were overweight/obese. Forty-seven percent and 24% of students who actively commuted a half-mile or less (n = 70) and more than a half-mile to school (n = 79), respectively, were overweight/obese. The rate of overweight/obesity was significantly lower in those who actively commuted more than a half-mile compared with both those who actively commuted a half-mile or less (P < .01) and those who did not engage in ACS (P < .05).
Figure 3.
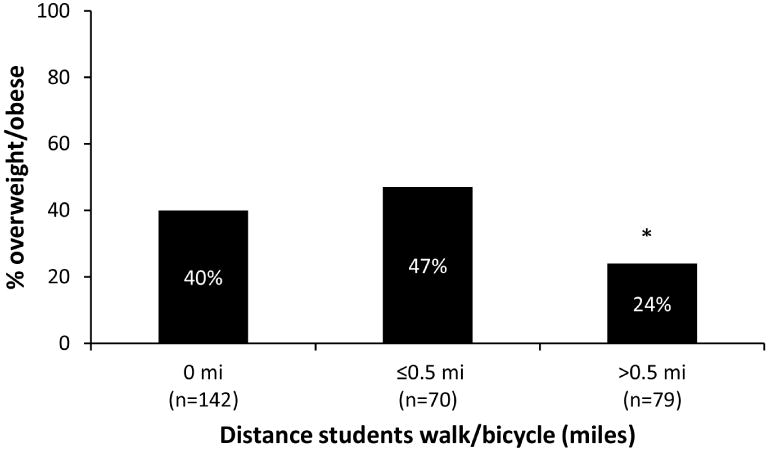
Percent of nonactive commuters and active commuters who are overweight/obese. * Significantly different than nonactive commuters (P < .05) and active commuters ≤ 1/2 mile (P < .01).
Three multivariate logistic regression models were used to predict the odds of overweight/obesity (Table 3). All models adjusted for city of residence, student demographics, household and parent demographics, student sedentary time, and student dietary behaviors.
Table 3. Multivariate Logistic Regression Analysis Assessing Associations of Active Commuting to School and Distance Commuted With Child Overweight/Obese Status.
| Adjusted OR (95% CI) | |
|---|---|
| Active commutinga (yes/no) (n = 337) | |
| No (referent) | 1 |
| Yes | 0.67 (0.42–1.09) |
| Distance traveled for ACSb (n = 250) [ACS (yes/no) × distance] | 0.93 (0.88–0.99) |
| Distance traveled thresholdsc (miles) (n = 250) | |
| 0 (no ACS) (referent) | 1 |
| ≤0.5 | 1.10 (0.57–2.14) |
| >0.5 | 0.35 (0.16–0.78) |
Separate models run for each. All models adjusted for city of residence, child's age, child's race/ethnicity, household income, parent's BMI, mother's education, acculturation, daily screen time, fruit and vegetable intake, fast food consumption, sugar-sweetened beverage consumption.
Model 1 used active commuting (yes/no; no distance component) as the predictor variable. Although those who engaged in ACS tended toward lower odds of being overweight/obese compared with those who never actively commuted, the association was not significant (OR = 0.67, 95% CI: 0.42 to 1.09).
Model 2 used distance traveled as a continuous variable (ACS [yes/no] × distance) as the predictor variable. In this model, each tenth of a mile increase in the distance a student actively commuted to school was associated with 7% (OR = 0.93, 95% CI: 0.88 to 0.99) lower odds of being overweight/obese. An age × distance commuted variable was entered into the model to examine if the relationship was confounded by age, but no interaction effect was observed (results not shown).
Model 3 examined whether a specific threshold existed for the association between distance traveled to school and overweight/obesity. Compared with students who never actively commuted to school, there was no association between overweight/obesity and ACS a half mile or less. Students who actively commuted more than a half-mile to school had 65% (OR = 0.35, 95% CI: 0.16 to 0.78) lower odds of being overweight/obese.
Discussion
This study found that, after adjusting for demographics, screen time, and dietary behavior, each one-tenth mile longer distance actively commuted by low-income, urban minority students was associated with 7% lower odds of being overweight/obese. However, no association between ACS and weight status was observed when active commuting was captured as a dichotomous (yes/no) variable. These findings suggest that it is not whether students engage in ACS that is critical for weight status, but rather it is the distance they actively commute that plays an important role.
To further illustrate this point, we also explored whether a certain distance threshold must be met before significant associations between ACS and weight status could be observed. Active commuters who lived greater than a half-mile from school had 65% lower odds of being overweight/obese when compared with students who did not actively commute to school. Conversely, no significant association was found between overweight/obesity and ACS among active commuters who lived within a half-mile from school. These results suggest that the benefits of ACS, in terms of lower weight status, may only be accrued by students who commute greater than half a mile to school. The lack of differentiation between active commuters who lived within a half-mile and those who lived farther than a half-mile may have prevented the association between ACS (yes/no) and weight status from reaching significance.
Heelan et al analyzed the association between ACS and weight status in K to 5th-grade students living within a half-mile from school, and 6th- to 8th-grade students living within a mile from school.20 While no association was observed between active commuting frequency and BMI z-scores in either age group, in the 6th- to 8th-grade students, greater distance from school in active commuters was inversely associated with BMI z-scores. Similar to the current study, commuting a half-mile or less to school (elementary school students) appeared to be below the threshold at which ACS was associated with weight status, whereas among those who lived up to a mile from school (middle school students), farther distances traveled were associated with lower weight status. Had Heelan et al20 not included distance as a predictor variable, active commuting, regardless of frequency, would appear to be unassociated with weight status.
To maximize the benefits of active commuting to school, policies and programs that encourage ACS should target not only students who live within a short distance (less than a half-mile) from school, but also students who live farther away. Although this is not feasible in every situation (eg, rural schools), schools may be able to tailor policies to fit their locations. The P.L. Robertson Public School in the Halton school district in Canada opened in 2009 as a ‘walk-to only’ school. No-stopping zones in front of the school prevent drop-offs at the door, and sidewalks leading to the school are designed to separate pedestrians from car traffic.41
About half of all states in the US have busing policies that require students to live a minimum distance from school to be eligible for bus pick-up and drop-off. This distance varies among states, from a mile to 2.5 miles.42 Combining school bus service and Walking School Buses (WSB), in which an adult walks to school with a group of students,43 is a potential strategy for enabling students living at all distances from school to actively commute at least a portion of the way. Implementation of WSBs has consistently been shown to increase ACS.43,44 This study and others20 provide evidence that locating bus stops a half-mile from school may have a positive impact on weight status among bus riders. In addition, remote drop-offs would improve air quality and reduce traffic around schools, increasing pedestrian safety.
A prospective study of a school bus/WSB combination is needed to examine the feasibility of such a program. Safe drop-off areas away from traffic, and infrastructure such as sidewalks, crosswalks, traffic signals, and/or bike lanes would be necessary. Adult WSB leaders or crossing guards would also be required along the walking route. These safeguards would address the issues of crime and traffic safety that prevent parents from allowing their children to actively commute to school.7,45
While more studies should investigate the relationship of ACS distance with weight within specific age groups, we did not find an interaction effect of age with distance commuted, indicating that the relationship was consistent across age groups. Further studies in varying geographic areas and among diverse demographic populations should also be conducted to investigate whether a threshold distance exists that maximizes the benefits of ACS with regard to weight status. However, regardless of its impact on weight, PA has numerous health benefits and should be promoted especially in children.
Some limitations of this study include the inability of a cross-sectional design to discern directionality. It is unknown whether ACS over a greater distance accounts for the lower incidence of overweight/obesity, or whether normal weight students are more willing to walk, bicycle, or skateboard farther distances. Another limitation is the lack of objective energy intake and expenditure measures. However, the variables included provided reasonable proxies for survey-based assessments of sedentary behavior and nutrient-dense versus energy-dense foods. While this study used geocoding for precise measurements of the roadway distance from a student's home to the school s/he attends, students may take shortcuts through yards, or take longer routes to travel with friends. Further, this analysis used a subsample from the full sample, but the subsample was very similar to the full sample in all characteristics. Finally, the sample for the study was drawn from high-minority, low income, urban populations with a higher rate of ACS than that of the national average (47.2% vs 12.7%), and as such, the findings are generalizable to similar communities. The prevalence of overweight and obesity among US children is highest among such populations.2 Therefore, the findings presented here can be used to inform policies and programs in elementary, middle, and high schools, and may be particularly effective in low-income urban schools with high minority populations.
Conclusions
Actively commuting distances greater than a half-mile to school is associated with lower odds of being overweight or obese. School policies that discourage car traffic and make the area around the school safer for pedestrians and bicyclists is a possible strategy for increasing the number of students engaging in ACS. Requiring minimum busing distances may encourage students living greater distances from school to actively commute, and these students may receive the greatest benefit from ACS. Combining minimum busing distances with remote drop-off areas could increase the distance many students actively commute, and create opportunities for all students to walk at least part of the way to school.
Acknowledgments
Dr. Michael Yedidia, Center for State Health Policy, Rutgers University, provided useful comments and feedback on the manuscript. This research was supported by a grant (grant #64253) from the Robert Wood Johnson Foundation.
References
- 1.Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA. 2010;303(3):242–249. doi: 10.1001/jama.2009.2012. [DOI] [PubMed] [Google Scholar]
- 2.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999-2010. JAMA. 2012;307(5):E1–E8. doi: 10.1001/jama.2012.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jimenez-Pavon D, Kelly J, Reilly JJ. Associations between objectively measured habitual physical activity and adiposity in children and adolescents: systematic review. Int J Pediatr Obes. 2010;5:3–18. doi: 10.3109/17477160903067601. [DOI] [PubMed] [Google Scholar]
- 4.Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40(1):181–188. doi: 10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- 5.US Department of Health and Human Services. [Accessed July 5, 2014];physical activity guidelines for Americans. 2008 http://www.health.gov/paguidelines/guidelines/summary.aspx. Updated July 5, 2014.
- 6.White House Task Force on Childhood Obesity. [Accessed March 4, 2013];Solving the problem of childhood obesity within a generation. http://www.letsmove.gov/sites/letsmove.gov/fles/Obesity_update_report.pdf. Updated February 2011.
- 7.McDonald NC, Brown AL, Marchetti LM, Pedroso MS. US school travel, 2009: an assessment of trends. Am J Prev Med. 2011;41(2):146–151. doi: 10.1016/j.amepre.2011.04.006. [DOI] [PubMed] [Google Scholar]
- 8.Lee MC, Orenstein MR, Richardson MJ. Systematic review of active commuting to school and children's physical activity and weight. J Phys Act Health. 2008;5(6):930–949. doi: 10.1123/jpah.5.6.930. [DOI] [PubMed] [Google Scholar]
- 9.Faulkner GEJ, Buliung RN, Flora PK, Fusco C. Active school transport, physical activity levels and body weight of children and youth: a systematic review. Prev Med. 2009;48:3–8. doi: 10.1016/j.ypmed.2008.10.017. [DOI] [PubMed] [Google Scholar]
- 10.Evenson KR, Huston SL, McMillen BJ, Bors P, Ward DS. Statewide prevalence and correlates of walking and bicycling to school. Arch Pediatr Adolesc Med. 2003;157:887–892. doi: 10.1001/archpedi.157.9.887. [DOI] [PubMed] [Google Scholar]
- 11.Heelan KA, Donnelly JE, Jacobsen DJ, Mayo MS, Wasburn R, Greene L. Active commuting to and from school and BMI in elementary school children—preliminary data. Child Care Health Dev. 2005;31(3):341–349. doi: 10.1111/j.1365-2214.2005.00513.x. [DOI] [PubMed] [Google Scholar]
- 12.Fulton JE, Shisler JL, Yore MM, Caspersen CJ. Active transportation to school: findings from a national survey. Res Q Exerc Sport. 2005;76(3):352–357. doi: 10.1080/02701367.2005.10599306. [DOI] [PubMed] [Google Scholar]
- 13.Rosenberg DE, Sallis JF, Conway TL, Cain KL, McKenzie TL. Active transportation to school over 2 years in relation to weight status and physical activity. Obesity (Silver Spring) 2006;14(10):1771–1776. doi: 10.1038/oby.2006.204. [DOI] [PubMed] [Google Scholar]
- 14.Ford P, Bailey R, Coleman D, Woolf-May K, Swaine I. Activity levels, dietary energy intake, and body composition in children who walk to school. Pediatr Exerc Sci. 2007;19(4):393–407. doi: 10.1123/pes.19.4.393. [DOI] [PubMed] [Google Scholar]
- 15.Landsberg B, Plachta-Danielzik S, Much D, Johannsen M, Lange D, Muller MJ. Associations between active commuting to school, fat mass and lifestyle factors in adolescents: the Kiel Obesity Prevention Study (KOPS) Eur J Clin Nutr. 2008;62:739–747. doi: 10.1038/sj.ejcn.1602781. [DOI] [PubMed] [Google Scholar]
- 16.Pabayo R, Gauvin L, Barnett TA, Nikiéma B, Séguin L. Sustained active transportation is associated with a favorable body mass index trajectory across the early school years: findings from the Quebec longitudinal study of child development birth cohort. Prev Med. 2010;50(Suppl 0):S59–S64. doi: 10.1016/j.ypmed.2009.08.014. [DOI] [PubMed] [Google Scholar]
- 17.Mendoza JA, Watson K, Nguyen N, Cerin E, Baranowski T, Nicklas TA. Active commuting to school and association with physical activity and adiposity among US youth. J Phys Act Health. 2011;8(4):488–495. doi: 10.1123/jpah.8.4.488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Drake KM, Beach ML, Longacre MR, et al. Influence of sports, physical education, and active commuting to school on adolescent weight status. Pediatrics. 2012;130(2):e296–e304. doi: 10.1542/peds.2011-2898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Saksvig BI, Webber LS, Elder JP, et al. A cross-sectional and longitudinal study of travel by walking before and after school among eighth-grade girls. J Adolesc Health. 2012;51(6):608–614. doi: 10.1016/j.jadohealth.2012.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Heelan K, Combs HJ, Abbey BM, Burger P, Bartee T. Evaluation of school transportation patterns and the associated impact on BMI in 2 Midwestern communities. J Phys Act Health. 2013;10:632–640. doi: 10.1123/jpah.10.5.632. [DOI] [PubMed] [Google Scholar]
- 21.Harrell JS, McMurray RG, Baggett CD, Pennell ML, Pearce PF, Bangdiwala SI. Energy costs of physical activities in children and adolescents. Med Sci Sports Exerc. 2005;37(2):329–336. doi: 10.1249/01.MSS.0000153115.33762.3F. [DOI] [PubMed] [Google Scholar]
- 22.The American Association for Public Opinion Research. [Accessed March 4, 2013];Standard definitions: Final dispositions of case codes and outcome rates for surveys. 2009 Available at: http://www.aapor.org/AAPORKentico/Communications/AAPOR-Journals/Standard-Definitions.aspx. Updated 2011.
- 23.Schneider KL, Clark MA, Rakowski W, Lapane KL. Evaluating the impact of non-response bias in the behavioral risk factor surveillance system (BRFSS) J Epidemiol Community Health. 2012;66:290–295. doi: 10.1136/jech.2009.103861. [DOI] [PubMed] [Google Scholar]
- 24.Centers for Disease Control and Prevention. [Accessed October 1, 2014];Measuring children's height and weight accurately at home. http://www.cdc.gov/healthy-weight/assessing/bmi/childrens_bmi/measuring_children.html. Updated 2014.
- 25.Carnell S, Wardle J. Appetite and adiposity in children: evidence for a behavioral susceptibility theory of obesity. Am J Clin Nutr. 2008;88:22–29. doi: 10.1093/ajcn/88.1.22. [DOI] [PubMed] [Google Scholar]
- 26.Huybrechts I, Himes JH, Ottevaere C, et al. Validity of parent-reported weight and height of preschool children measured at home or estimated without home measurement: a validation study. BMC Pediatr. 2011;11:63. doi: 10.1186/1471-2431-11-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Centers for Disease Control and Prevention, National Center for Health Statistics. [Accessed July 4, 2013];CDC growth charts: United States. http://www.cdc.gov/growthcharts/cdc_charts.htm. Updated 2010.
- 28.Centers for Disease Control and Prevention. [Accessed July 4, 2013];Cut-offs to define outliers in the 2000 CDC growth charts. http://www.cdc.gov/nccdphp/dnpa/growthcharts/resources/BIV-cutoffs.pdf.
- 29.Evenson KR, Birnbaum AS, Bedimo-Rung AL, et al. Girls' perception of physical environmental factors and transportation: Reliability and association with physical activity and active transport to school. Int J Behav Nutr Phys Act. 2006;3:28. doi: 10.1186/1479-5868-3-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Babey SH, Hastert TA, Huang W, Brown R. Sociodemographic, family, and environmental factors associated with active commuting to school among US adolescents. J Public Health Policy. 2009;30:S203–S220. doi: 10.1057/jphp.2008.61. [DOI] [PubMed] [Google Scholar]
- 31.Aires L, Silva G, Gaya AR, Santos MP, Ribeiro JC, Mota J. A 3-year longitudinal analysis of changes in body mass index. Int J Sports Med. 2010;31:133–137. doi: 10.1055/s-0029-1243255. [DOI] [PubMed] [Google Scholar]
- 32.Lubans DR, Boreham CA, Kelly P, Foster CE. The relationship between active travel to school and health-related fitness in children and adolescents: a systematic review. Int J Behav Nutr Phys Act. 2011;8:5. doi: 10.1186/1479-5868-8-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kerr J, Rosenberg D, Sallis JF, Saelens BE, Frank LD, Conway TL. Active commuting to school: associations with environment and parental concerns. Med Sci Sports Exerc. 2006;38(4):787–794. doi: 10.1249/01.mss.0000210208.63565.73. [DOI] [PubMed] [Google Scholar]
- 34.Robertson-Wilson JE, Leatherdale ST, Wong SL. Social-ecological correlates of active commuting to school among high school students. J Adolesc Health. 2008;42:486–495. doi: 10.1016/j.jadohealth.2007.10.006. [DOI] [PubMed] [Google Scholar]
- 35.Voorhees CC, Ashwood S, Evenson KR, et al. Neighborhood design and perceptions: relationship with active commuting. Med Sci Sports Exerc. 2010;42(7):1253–1260. doi: 10.1249/MSS.0b013e3181cd5dfd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Rossen LM, Pollack KM, Curriero FC, et al. Neighborhood incivilities, perceived neighborhood safety, and walking to school among urban-dwelling children. J Phys Act Health. 2011;8(2):262–271. doi: 10.1123/jpah.8.2.262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Gallimore JM, Brown BB, Werner CM. Walking routes to school in new urban and suburban neighborhoods: an environmental walk-ability of blocks and routes. J Environ Psychol. 2011;31:184–191. doi: 10.1016/j.jenvp.2011.01.001. [DOI] [Google Scholar]
- 38.Martin SL, Lee SM, Lowry R. National prevalence and correlates of walking and bicycling to school. Am J Prev Med. 2007;33(2):98–105. doi: 10.1016/j.amepre.2007.04.024. [DOI] [PubMed] [Google Scholar]
- 39.US Department of Health and Human Services, Centers for Disease Control and Prevention. [Accessed February 4, 2014];Behavioral risk factor surveillance system survey questionnaire. Available at: http://www.cdc.gov/brfss/questionnaires.htm. Updated July 1, 2013.
- 40.Nelson MC, Lytle LA. Development and evaluation of a brief screener to estimate fast-food and beverage consumption among adolescents. J Am Diet Assoc. 2009;109(4):730–734. doi: 10.1016/j.jada.2008.12.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Lay J, Kennedy J, Jenkins J. Influencing the school trip: evidence-based results and techniques from national and regional school-based transportation demand management projects. Influencing travel choice and behavior session; Halifax, Nova Scotia. 2010; Annual conference of the Transportation Association of Canada.. [Google Scholar]
- 42.Chriqui JF, Taber DR, Slater SJ, Turner L, Lowrey KM, Chaloupka FJ. The impact of state Safe Routes to School-related laws on active travel to school policies and practices in US elementary schools. Health Place. 2012;18:8–15. doi: 10.1016/j.healthplace.2011.08.006. [DOI] [PubMed] [Google Scholar]
- 43.Mendoza JA, Watson K, Baranowski T, Nicklas TA, Uscanga DK, Hanfling MJ. The walking school bus and children's physical activity: a pilot cluster randomized controlled trial. Pediatrics. 2011;128(3):e537–e544. doi: 10.1542/peds.2010-3486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Heelan KA, Abbey BM, Donnelly JE, Mayo MS, Welk GJ. Evaluation of a walking school bus for promoting physical activity in youth. J Phys Act Health. 2009;6(5):560–567. doi: 10.1123/jpah.6.5.560. [DOI] [PubMed] [Google Scholar]
- 45.Rodríguez A, Vogt CA. Demographic, environmental, access, and attitude factors that influence walking to school by elementary school-aged children. J Sch Health. 2009;79(6):255–261. doi: 10.1111/j.1746-1561.2009.00407.x. [DOI] [PubMed] [Google Scholar]