

Abstract
It has been suggested that consuming alcohol mixed with energy drink (AMED) may increase total alcohol consumption. Aims of this systematic review and meta‐analysis were (i) to compare alcohol consumption of AMED consumers with alcohol only (AO) consumers (between‐group comparisons), and (ii) to examine if alcohol consumption of AMED consumers differs on AMED and AO occasions (within‐subject comparisons). A literature search identified fourteen studies. Meta‐analyses of between‐group comparisons of N = 5212 AMED consumers and N = 12 568 AO consumers revealed that on a typical single drinking episode AMED consumers drink significantly more alcohol than AO consumers (p = 0.0001, ES = 0.536, 95%CI: 0.349 to 0.724). Meta‐analyses of within‐subject comparisons among N = 2871 AMED consumers revealed no significant difference in overall alcohol consumption on a typical drinking episode between AMED and AO occasions (p = 0.465, ES = −0.052, 95%CI: −0.192 to 0.088). In conclusion, between‐group comparisons suggest that heavy alcohol consumption is one of the several phenotypical differences between AMED and AO consumers. Within‐subject comparisons revealed, however, that AMED consumption does not increase the total amount of alcohol consumed on a single drinking episode. © 2016 The Authors. Human Psychopharmacology: Clinical and Experimental Published by John Wiley & Sons Ltd
Keywords: alcohol, energy drink, AMED, alcohol consumption
Introduction
There is controversy as to whether, compared with alcohol alone, consuming alcohol mixed with energy drink (AMED) increases total alcohol consumption (Verster et al. 2012). One hypothesis is that the stimulant effects of caffeine, one of the main ingredients of energy drinks, may counteract the depressant effects of alcohol. If this hypothesis is correct, it would be of concern as excessive alcohol consumption and its negative consequences are a serious health issue, particularly among adolescents and young adults.
An important cause of this controversy is the fact that different methodological approaches have been used to study the possible relationship between energy drink and alcohol consumption. One approach is to apply between‐group comparisons. Using this approach, alcohol consumption of AMED users is compared to alcohol consumption of those who never mix alcohol with energy drinks, i.e. consume alcohol only (AO). Because AMED users do not mix energy drinks with alcohol on all drinking occasions (e.g., de Haan 2012), an alternative, and arguably more powerful, approach is to apply within‐subject comparisons. Using this approach, alcohol consumption of AMED consumers is examined by comparing total alcohol consumption on occasions when they consume AMED, with occasions when they consume AO.
Between‐group comparisons may show that AMED consumers consume more or less alcohol than AO consumers. However, this analysis provides no evidence of the underlying cause(s) for the observed difference in alcohol consumption patterns. Any difference may be related to co‐consumption of energy drink; on the other hand various other ‘trait’ or ‘phenotypic’ differences in personality and behaviors between the groups may contribute to the observed difference in amounts of alcohol consumed. In other words, by using between‐group comparisons many differences can be identified but no information is obtained as to why these differences are present.
Within‐subject comparisons among AMED consumers comparing AMED and AO occasions may be more appropriate to look at the impact of co‐consumption of energy drinks. As the same individuals' behavior is evaluated on AMED and AO occasions, it can be argued that the only difference between the occasions is the co‐consumption of energy drinks. By definition stable personality traits will not differ between these occasions. The within‐subjects approach is therefore regularly favored in crossover studies. However, it can also be applied in surveys or interviews where participants retrospectively report on occasions in which they engage in different behaviors (in this case consuming AMED and consuming AO).
The aim of this systematic review is to draw on the extant literature to examine whether co‐consumption of energy drink has an impact on total alcohol consumption during single drinking occasions. Given the different methodological approaches, separate meta‐analyses will be presented of studies applying between‐group comparisons and those applying within‐subject comparisons.
Methods
A literature search was conducted (2 March 2015) on PubMed, PsycINFO, and Embase using the key words “energy drink” and “alcohol”. The search yielded 908 hits (313 PubMed, 268 Embase, 232 PsycINFO). After removing 95 duplicate items, the initial data base included 813 publications. To be included, studies and surveys had to be conducted in healthy volunteers and present (i) between‐group comparisons comparing AMED consumers with AO consumers or (ii) within‐subject comparisons among AMED consumers..
The meta‐analyses were performed using Comprehensive Meta‐analysis (Biostat Inc., Englewood, NJ) as described by Borenstein and Rothstein (1999). Studies were included if the mean, standard deviation, and sample size were reported, or other outcome measures that could be used to calculate effect sizes (ES). The ES and corresponding 95% confidence interval (CI) were computed for each of the AMED versus AO comparisons. If the 95% CI did not include zero, the ES was considered statistically significant (p < 0.05). Homogeneity/heterogeneity analyses were performed to determine if each individual ES had the same distribution as the combined overall ES. In a homogenous distribution, the dispersion of ES around their mean is not greater than that expected from sampling error alone. If the Q statistic resulting from this analysis is not significant (p ≥ 0.05), a homogenous distribution can be assumed and a fixed effects model to perform the meta‐analysis is justified. However, if the Q statistic is significant (p < 0.05), variation in ES is greater than would be expected from subject‐level sampling error alone, and a random effects model is applied correcting for additional variation between the studies (Lipsey and Wilson, 2000).
Meta‐analyses were performed separately for studies applying a between‐group design and studies applying a within‐subject design, for (i) the typical number of alcoholic drinks, and (ii) the maximum number of alcoholic drinks consumed in a single drinking occasion.
Results
Fourteen studies were identified that examined alcohol consumption of AMED consumers. The studies were either surveys (N = 10), interviews (N = 1), or on‐premise interviews (N = 3), and were conducted in Australia (N = 5), The Netherlands (N = 3), USA (N = 3), Canada (N = 2), and Brazil (N = 1). The majority of participants were university and college students, aged 18 to 30 years old. The studies collected data on the typical amount of alcoholic drinks consumed in a single episode, usually during the last 30 days or past 12 months. Some studies also recorded the maximum number of alcoholic drinks consumed in a single episode during that period. The characteristics of each study are summarized in Table 1.
Table 1.
Overview of studies examining the total alcohol consumption of AMED consumers. If available, mean (SD) number of alcoholic drinks are reported, and corresponding p‐values
| Study | Year | Country | Design and recall period | Subjects | Between groups comparison | Within subjects comparison | Outcome |
|---|---|---|---|---|---|---|---|
| O'Brien et al. | 2008 | U.S.A. | Web‐based survey Recall period: past 30 days | College students. AO: N = 2.189 AMED: N = 697 | Typical number of alcoholic drinks on a single occasion. AO: 4.5 (7.0) AMED: 5.8 (4.5) p < 0.001 Maximum number of alcoholic drinks on a single occasion. AO: 6.1 (7.0) AMED: 8.3 (5.0) p < 0.001 | Not conducted | BG: AMED > AO |
| Price et al. | 2010 | Canada | Structured face‐to‐face interviews Recall period: past week | Past month ED consuming students AMED: N = 10 | Not conducted | Past week AMED and AO consumption on an average occasion. AO: 4.7 AMED: 8.6 p = 0.016 | WS: AMED > AO |
| Woolsey et al. | 2010 | U.S.A. | Web‐based survey Recall period: past 12 months | Student athletes AO: N = 165 AMED: N = 150 | Typical number of alcoholic drinks on a single occasion. AO: 5.20 (3.91) AMED: 8.40 (5.22) p < 0.0001 Maximum number of alcoholic drinks on a single occasion. AO: 9.80 (5.84) AMED: 18.35 (10.74) p < 0.0001 | N = 123 Typical number of alcoholic drinks on a single occasion. AO: 8.60 (5.14) AMED: 6.28 (4.41) Maximum number of alcoholic drinks on a single occasion (past 12 months) AO: 18.23 (10.56) AMED: 10.83 (7.94) | BG: AMED > AO WS: AMED < AO |
| Brache & Stockwell | 2011 | Canada | Web‐based survey Recall period: past 30 days | University students AO: N = 305 AMED: N = 105 | Typical number of alcoholic drinks on a single occasion. AO: 3.04 (2.04) AMED: 5.34 (3.52) p < 0.001 Maximum number of alcoholic drinks on a single occasion. AO: 6.32 (3.93) AMED:10.42 (5.31) p < 0.001 | Typical number of alcoholic drinks on a single occasion. AO: 5.29 (5.91) AMED: 6.5 (3.56) p < 0.01 | BG: AMED > AO WS: AMED > AO |
| Penning et al. | 2011 | The Netherlands | Survey Recall period: variable | University students, 20.4 years old AO: N = 480 AMED: N = 24 | Number of alcoholic drinks the day before latest alcohol hangover: \AO: 10.9 (6.1) AMED: 8.5 (4.2) p = 0.056 | Not conducted | BG: AMED = AO |
| De Haan et al. | 2012 | The Netherlands | Web‐based survey Recall period: 30 days | University and college students, 18–30 years old AO: N = 3.185 AMED: N = 1.239 | Typical number of alcoholic drinks on a single occasion. AO: 4.1 (3.1) AMED: 6.0 (3.9) p < 0.001 Maximum number of alcoholic drinks on a single occasion. AO: 7.7 (6.0) AMED:10.7 (6.7) p < 0.001 | Typical number of alcoholic drinks on a single occasion (past 30 days). AO: 6.0 (3.9) AMED: 5.4 (3.7) p < 0.001 Maximum number of alcoholic drinks on a single occasion (past 30 days). AO: 10.7 (6.8) AMED:4.5 (5.7) p < 0.001 | BG: AMED > AO WS: AMED < AO |
| Peacock et al. | 2012 | Australia | Web‐based survey Recall period: past 6 months for AMED occasions, past month for alcohol only occasions. | Convenience sample, 18–35 years old AMED: N = 387 | Not conducted | Typical number of alcoholic drinks on a single occasion. AO: 6.5 (4.8) AMED: 7.1 (5.6) p = 0.012 | WS: AMED > AO |
| Lubman et al. | 2013a | Australia | Web‐based survey (Study A) Recall period: past 12 months | Convenience sample, 16–70 years old (mean age 26.5 years old) AO: N = 996 AMED: N = 731 | Typical number of alcoholic drinks on a single occasion. AO: 3.65 (2.84) AMED: 6.67 (3.93) p < 0.001 | N = 698 Typical number of alcoholic drinks on a single occasion. AO: 6.7 (4.0) AMED: 6.0 (4.2) p < 0.00 Maximum number of alcoholic drinks on a single occasion. AO: 14.7 (8.3) AMED: 8.3 (6.7) p < 0.001 | BG: AMED > AO WS: AMED < AO |
| Lubman et al. | 2013b | Australia | On‐premise interviews (Study B) Recall period: past 12 months and number of drinks consumed on premise on the interview day | Bar patrons, 16–55 years old (mean age 22.71 years old). Past 12 months: AO: 718 AMED: 474 On premise: AO: N = 887 AMED: N = 128 | Typical number of alcoholic drinks on a single occasion. AO: 7.42 (5.50) AMED:9.54 (5.62) p < 0.001 Number of alcoholic drinks consumed on premise: AO: 4.76 (5.46) AMED:5.65 (5.60) p < 0.01 | N = 358 Typical number of alcoholic drinks on a single occasion. AO: 9.7 (5.8) AMED: 8.4 (5.9) p < 0.001 | BG: AMED > AO WS: AMED < AO |
| Eckschmidt et al. | 2013 | Brazil | Survey Recall period: past 12 months and number of drinks consumed on premise on the interview day | College students AO: N = 4.192 AMED: N = 1.119 | Typical number of alcoholic drinks on a single occasion. AO: 3.3 (13.2)AMED: 6.1 (13.7) p < 0.001 | Not conducted | BG: AMED > AO |
| Lubman et al. | 2014 | Australia | On‐premise interview Recall period: number of drinks consumed on premise on the interview day | Secondary school completers, 17–18 years old AO: N = 471 AMED: N = 87 | Number of alcoholic drinks on the night of interview. AO: 8.30 AMED: 11.34 p < 0.001 | Not conducted | BG: AMED > AO |
| Trapp et al. | 2014 | Australia | Survey Recall period: not reported | Western Australian Pregnancy Cohort, 20 years old AO: N = 644 AMED: N = 590 | Total alcohol intake per day (g/day) AO: 12.1 (15.7) g AMED: 20.3 (19.7) g p < 0.001 | Not conducted | BG: AMED > AO |
| Verster et al. | 2015 | The Netherlands | On‐premise interview Recall period: number of drinks consumed on the interview day (at home and on premise) | Bar patrons, 18–30 years old AO: N = 482 AMED1: N = 185 (consumed AMED that day) AMED2: N = 246 (no AMED consumed that day) | Number of alcoholic drinks consumed on the day of the interview. AO: 8.8 (5.4) AMED1: 9.4 (6.3) AMED2: 10.1 (6.8)* p < 0.05 | AMED1: AO: 9.4 (5.9) AMED: 10.1 (6.8) p = 0.148 AMED2: AO: 9.4 (6.3) AMED: 9.8 (6.0) p = 0.360 | BG: AMED > AO WS: AMED = AO |
| Woolsey et al. | 2015 | USA | Web‐based survey Recall period: past 30 days | University students. AO: N = 174 AMED: N = 107 | Typical number of alcoholic drinks on a single occasion. AO: 3.35 (2.30) AMED: 5.42 (3.46) p < 0.0001 Maximum number of alcoholic drinks on a single occasion. AO: 4.62 (3.79) AMED:8.03 (5.84) p < 0.001 | Not conducted | BG: AMED > AO |
Abbreviations: ED, energy drink; AMED, alcohol mixed with energy drink; AO, alcohol only; WS, within‐subject comparison; BG, between‐group comparison.
For the meta analyses, studies were included only if they applied a between‐group and/or within‐subject comparison of (i) the typical number of alcoholic drinks, and (ii) the maximum number of alcoholic drinks consumed in a single drinking occasion. Therefore, not all studies presented in Table 1 could be included. For example, Penning et al. (2011) did not examine alcohol consumption for a regular drinking episode but surveyed participants about their latest heavy drinking occasion that resulted in a hangover. As this drinking occasion cannot be regarded as representative for a typical (average) drinking episode, data from this study was omitted from the meta‐analysis. The on‐premise studies by Lubman et al. (2014) and Verster et al. (2015) did include questions about alcohol consumption on the night of the interview. It is however not sure whether the night of the interview can be viewed as a typical drinking episode. Therefore, data from these studies were also omitted from the meta‐analyses. Data from the other 11 studies were included in the meta‐analyses.
Between‐group comparisons
Nine studies provided data on typical alcohol consumption on a single drinking episode of AMED consumers in comparison to AO consumers and conducted between‐group comparisons (O'Brien et al. 2008, Woolsey et al. 2010, Brache and Stockwell 2011, De Haan et al. 2012, Eckschmidt et al. 2013, Lubman et al. 2013a, Lubman et al. 2013b, Trapp et al. 2014, Woolsey et al. 2015).
In total, alcohol intake of 5212 AMED consumers was compared to that of 12 568 AO consumers. The results of these between‐group comparisons were combined in a meta‐analysis (see Figure 1).
Figure 1.
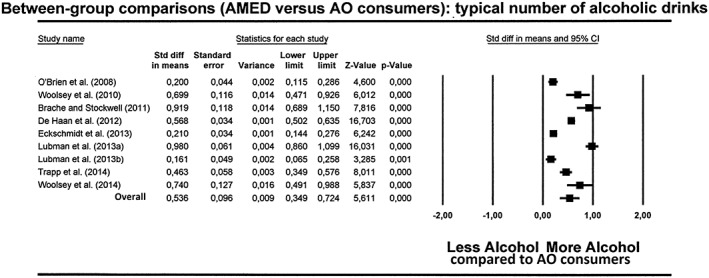
Meta‐analysis of between‐group comparisons of the typical number of alcoholic drinks on a single episode of alcohol mixed with energy drink (AMED) and alcohol only (AO) consumers
The results of the meta‐analysis confirm that AMED consumers drink significantly more alcohol than AO consumers on a typical drinking occasion (p = 0.0001, ES = 0.536, 95%CI: 0.349 to 0.724).
Five studies also provided between‐group data on the maximum number of alcoholic drinks consumed on a single episode (O'Brien et al. 2008, Woolsey et al. 2010, Brache and Stockwell 2011, De Haan et al. 2012, Woolsey et al. 2015). In total, maximum alcohol intake on a single episode of 2302 AMED consumers was compared with that of 6022 AO consumers. The meta‐analysis of these data revealed that AMED consumers reported a significantly higher maximum number of alcoholic drinks consumed on a single episode when compared to AO consumers (p = 0.0001, ES = 0.673, 95%CI: 0.464 to 0.882) (Figure 2).
Figure 2.
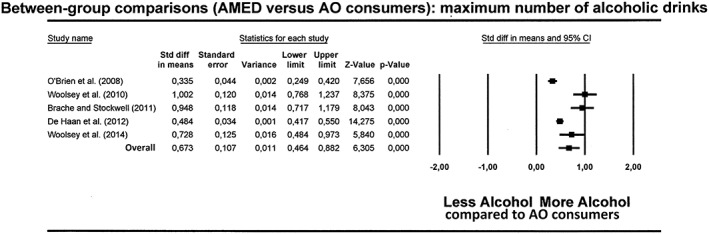
Meta‐analysis of between‐group comparisons of the maximum number of alcoholic drinks on a single episode of alcohol mixed with energy drink (AMED) and alcohol only (AO) consumers
Within‐subject comparisons
Seven studies used a within‐subject comparison among AMED consumers to compare alcohol consumption on a typical AMED and a typical AO occasion (Price et al. 2010, Woolsey et al. 2010, Brache and Stockwell 2011, Peacock et al. 2012, De Haan et al. 2012, Lubman et al. 2013a, Lubman et al. 2013b). In total, alcohol intake of 2871 AMED consumers was analyzed, comparing alcohol consumption on AMED occasions with AO occasions. Results from the meta‐analysis are shown in Figure 3.
Figure 3.
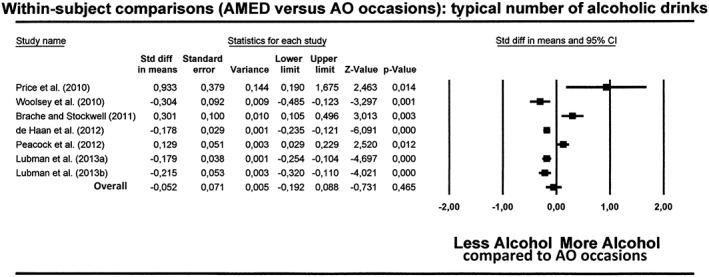
Meta‐analysis of within subject‐comparisons examining the typical number of alcoholic drinks on alcohol mixed with energy drink (AMED) versus alcohol only (AO) occasions
The meta‐analysis revealed no significant difference in overall alcohol consumption on typical drinking occasions between AMED and AO occasions (p = 0.465, ES = −0.052, 95%CI: −0.192 to 0.088).
Three studies also provided data on the maximum number of alcoholic drinks consumed on a single episode (Woolsey et al. 2010, De Haan et al. 2012, Lubman et al. 2013a). In total, data from 2.011 AMED consumers were analyzed. The meta‐analysis revealed that the maximum number of drinks on AMED occasions was significantly lower than on AO occasions (p = 0.0001, ES = −0.742, 95%CI: −1.015 to −0.468) (Figure 4).
Figure 4.
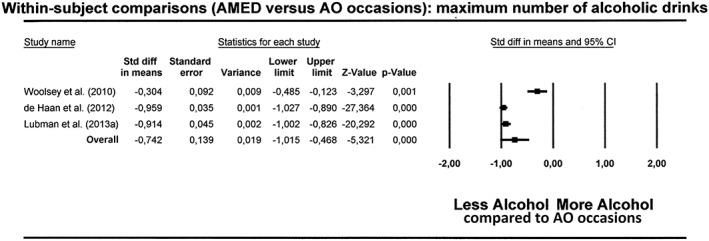
Meta‐analysis of within‐subject comparisons examining the maximum number of alcoholic drinks on alcohol mixed with energy drink (AMED) versus alcohol only (AO) occasions
Omitted studies
When including the three omitted studies (Penning et al. 2011, Lubman et al. 2014, Verster et al. 2015) no relevant changes were seen in the overall outcome of the meta‐analyses. Again, the meta‐analysis of between‐group comparisons revealed that AMED consumers on a typical drinking occasion consume significantly more alcohol than AO consumers (p = 0.0001, ES = 0.453, 95%CI = 0.289 to 0.617). The meta‐analysis of within‐subject comparisons amongst AMED consumers revealed no significant difference in the amount of alcohol consumed on a typical AMED and AO occasion (p = 0.380, ES = −0.055, 95%CI = −0.179 to 0.068). The studies provided no data on the maximum number of alcoholic drinks consumed.
Discussion
Studies using between‐group comparisons show that AMED consumers drink significantly more alcohol than people who consume AO. However, within‐subject comparisons show that AMED consumers drink the same typical amount of alcohol on AMED occasions as they do on AO occasions. Taken together, these analyses suggest that there are phenotypical differences between AMED consumers and AO consumers. One of these differences is that AMED consumers drink significantly more alcohol in general. They do this, however, irrespective of whether alcohol is mixed with energy drink or not.
The notion that there are various phenotypical differences between AMED consumers and AO consumers in demographics (e.g., gender and age), personality, and risk‐taking profiles has already been raised previously as an explanation for the observed differences between AMED and AO consumers (Verster et al. 2012). Indeed, research has revealed that AMED consumers were significantly more often Caucasian (Berger et al. 2011), young (Berger et al. 2011, Wells et al. 2013), male (Berger et al. 2011, Cheng et al. 2012, Wells et al. 2013, Eckschmidt et al. 2013), have a lower income and education level (Cheng et al. 2012), were single (Eckschmidt et al. 2013), use illicit drugs (De Haan et al. 2012, Snipes and Benotsch 2013) smoke (De Haan et al. 2012), and engage in high risk taking behavior (Woolsey et al. 2010, Brache and Stockwell 2011, De Haan et al. 2012, Eckschmidt et al. 2013, Snipes and Benotsch 2013). Examples for more frequently seen risk taking behaviors amongst AMED consumers are having unprotected sex or being engaged in other sexual risk taking behaviors (Miller 2012, Berger et al. 2013, Snipes and Benotsch 2013), and driving while intoxicated (O'Brien et al. 2008, Woolsey et al. 2010, Woolsey et al. 2015). The observed differences between AMED and AO consumers underline that the groups differ in many aspects from each other. One of these differences is the fact that AMED consumers drink more alcohol. It has been suggested that these differences between AMED and AO consumers may be caused by underlying personality characteristics that might differ between the groups, for instance levels of risk‐taking behavior (Verster et al. 2012). Recent research supports this hypothesis by showing that level of risk taking behavior is an independent predictor of binge drinking per se, even after controlling for demographics and lifestyle factors (De Haan et al. 2015). In other words, consumption of AMED is one of a cluster of behavioral manifestations of an underlying phenotype which appears to also include a higher risk‐taking personality.
Between‐group comparisons show that phenotypical differences exist between the groups (e.g., differences in alcohol consumption), but do not provide information on why the observed differences exist. Within‐subject comparisons among AMED consumers suggest that there is no causal relationship between consuming energy drinks and increased alcohol consumption. By using within‐subject comparisons these differences between AMED and AO consumers do not contribute to the study outcome, as two drinking occasions of the same subjects are compared of which the only difference is whether or not energy drinks are co‐consumed. The meta‐analyses of these data reveal that co‐consumption of energy drinks has no significant influence on total alcohol consumption on a typical single drinking occasion.
There are several limitations to our research that should be addressed. First, it can be argued that recall bias may have interfered with obtaining reliable survey data. Not all studies used the same recall period (see Table 1), and it may be that last week recall is easier and more reliable than last year recall. However, when applying a within‐subject design, there is no reason to assume that participants will recall consumption characteristics differently between AMED or alcohol‐only occasions, with the caveat that AMED occasions tend to be less frequent. Moreover, to recall “typical use” it is not necessary to recall each individual drinking occasion. It is an estimated average of number of drinks by the subjects. Hence, the frequency of the occasions is less important. The maximum number of alcoholic drinks are consumed on a single occasion. As this occasion is not a regular drinking day, it is likely that this day is recalled relatively well (for example, because it was a birthday or special party night). To avoid the possibility of recall bias entirely, prospective study designs with recordings while drinking or next day consumption recordings may be a solution.
The included studies used different ways to question participants about their typical and maximum alcohol and energy drink consumption. Some studies used standardized and validated questionnaires such as the Quick Drinking Screen (e.g., Woolsey et al 2010, De Haan et al. 2012), whereas other composed their own questions. Most studies did not report if questions were taken from validated scales or designed by the researchers. In future research, it may be best to use standardized questions (e.g., the Quick Drinking Screen), and have a standard recall period (e.g. past 30 days).
Most studies did not report on how AMED consumption was defined and whether they only included people that actually mixed alcohol with energy drink or also included people who consumed energy drink (not mixed) in between of consuming AO drinks. As caffeine has a relative long half‐life, and the drinks do mix in the stomach, this is important to take into account. From the publications and surveys examined, this was clearly taken into account by only two studies (Woolsey et al. 2010, de Haan et al. 2012). Both studies defined co‐consumption as consuming energy drinks or other non‐alcoholic beverages either 2 h before or 2 h after drinking alcohol, representing a relatively conservative definition of ‘mixing’. It is important to implement clear definitions of mixing in future research.
Regarding the generalizability of the results, it should be mentioned that most studies were conducted among students or young adults aged 18 to 30 years old. Although these represent a big segment of energy drink consumers, other age groups were not investigated. Nevertheless, the studies revealed similar findings across the world in surveys conducted in USA, Europe, and Australia, suggesting that the outcome of the meta‐analyses is representative for this age group.
Finally, regarding the possible influence of industry funding on the studies included in the meta‐analysis, it should be noted that only 1 out of the 10 studies that were included in the meta‐analyses was supported by industry (De Haan et al. 2012). All other studies were funded by government or universities with authors that have no relationship with energy drink industry.
Although our analyses show that mixing alcohol with energy drink does not lead to increased alcohol consumption, the data do indicate that both AMED and AO consumers drink much more alcohol than is generally recommended as safe. This pattern of heavy drinking is consistent across drinking occasions, irrespective of whether alcohol is consumed by itself, mixed with energy drinks, or mixed with other nonalcoholic beverages such as cola or tonic (Verster et al. 2014). Future research might therefore usefully focus on excessive alcohol consumption per se, given that the group of AO consumers (70.7% of the whole sample) is substantially larger than the group of AMED consumers (29.3%). As discussed above, several papers suggest that personality aspects such as a high risk taking profile may be related to increased alcohol consumption. Identifying the personality characteristics that result in increased alcohol consumption may be an important goal for future research, as this may help to screen for individuals at risk for excessive alcohol consumption.
Taken together, between‐group comparisons suggest that overall alcohol consumption is one of the many phenotypical differences between AMED and AO consumers. Within‐subject comparisons amongst AMED consumers reveal, however, that mixing alcohol with energy drink has no significant impact on total alcohol consumption on a typical single drinking occasion.
Disclosure of Interests
This research was conducted at Utrecht University, Swinburne University, and the University of the West of England. There was no industry involvement in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Joris Verster has received grants/research support from The Dutch Ministry of Infrastructure and the Environment, Janssen Research and Development, Nutricia Research, Takeda, Red Bull, and has acted as a consultant/expert advisor to Canadian Beverage Association, Centraal Bureau Drogisterijbedrijven, Coleman Frost, Danone Research, Deenox, Eisai, Jazz, Purdue Pharma, Red Bull, Sanofi‐Aventis, Sepracor, Takeda, Transcept, and Trimbos Institute. Andrew Scholey has held research grants from Abbott Nutrition, Bayer Healthcare, Cognis, Cyvex, GlaxoSmithKline, Kemin, Naturex, Nestlé, Martek, Masterfoods, Wrigley, and has acted as a consultant/expert advisor to Abbott Nutrition, Barilla, Bayer Healthcare, Danone, Flordis, GlaxoSmithKline Healthcare, Masterfoods, Martek, Novartis, Unilever, Wrigley. Chris Alford has received funding from the UK Ministry of Defence Innovate UK, Red Bull, and Sanofi‐Aventis. Sean Johnson has undertaken sponsored research for Pfizer, AstraZeneca, Merck, Gilead, Novartis, Roche, and Red Bull GmbH.
Verster, J. C. , Benson, S. , Johnson, S. J. , Scholey, A. , and Alford, C. (2016) Mixing alcohol with energy drink (AMED) and total alcohol consumption: a systematic review and meta‐analysis. Hum. Psychopharmacol Clin Exp, 31: 2–10. doi: 10.1002/hup.2513.
References
- Berger LK, Fendrich M, Chen H‐Y, Arria AM, Cisler RA. 2011. Sociodemographic correlates of energy drink consumption with and without alcohol: results of a community survey. Addict Behav 36: 516–519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borenstein M, Rothstein H. 1999. Comprehensive Meta‐analysis. A computer program for research synthesis. Biostat Inc.: USA. [Google Scholar]
- Brache K, Stockwell T. 2011. Drinking patterns and risk behaviors associated with combined alcohol and energy drink consumption in college drinkers. Addict Behav 36: 1133–1140. [DOI] [PubMed] [Google Scholar]
- Cheng W‐J, Cheng Y, Huang M‐C, Chen C‐J. 2012. Alcohol dependence, consumption of alcoholic energy drinks and associated work characteristics in the Taiwan working population. Alcohol Alcohol 47: 372–379. [DOI] [PubMed] [Google Scholar]
- De Haan L, de Haan HA, van der Palen J, Olivier B, Verster JC. 2012. The effects of consuming alcohol mixed with energy drinks (AMED) versus consuming alcohol only on overall alcohol consumption and alcohol‐related negative consequences. International Journal of General Medicine 5: 953–960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Haan L, Egberts AC, Heerdink ER. 2015. The relation between risk‐taking behavior and alcohol use in young adults is different for men and women. Drug Alcohol Depend. DOI:10.1016/j.drugalcdep.2015.07.013. [DOI] [PubMed] [Google Scholar]
- Eckschmidt F, De Andrade AG, Dos Santos B, De Oliveira LG. 2013. The effects of alcohol mixed with energy drinks (AmED) on traffic behaviors among Brazilian college students: a national survey. Traffic Inj Prev 14: 671–679. [DOI] [PubMed] [Google Scholar]
- Lipsey MW, Wilson D. 2000. Practical Meta‐Analysis (Applied Social Research Methods). Sage Publications, Inc.: London. [Google Scholar]
- Lubman DL, Peacock A, Droste N, Pennay A, Miller P, Bruno R, Lloyd B, Hyder S, Roxburgh A, Wadds P, Tomsen S, Brown J. 2013. Alcohol and energy drinks in NSW. (a,b). Available at: www.health.nsw.gov.au
- Lubman DI, Droste N, Pennay A, Hyder S, Miller P. 2014. High rates of alcohol consumption and related harm at schoolies week: a portal study. Aust N Z J Public Health 38: 536–541. [DOI] [PubMed] [Google Scholar]
- Miller KE. 2012. Alcohol mixed with energy drink use and sexual risk‐taking: casual, intoxicated, and unprotected sex. Journal of Caffeine Research 2: 62–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Brien MC, McCoy TP, Rhodes SD, Wagoner A, Wolfson M. 2008. Caffeinated cocktails: energy drink consumption, high‐risk drinking, and alcohol‐related consequences among college students. Acad Emerg Med 15: 453–460. [DOI] [PubMed] [Google Scholar]
- Peacock A, Bruno R, Martin FH. 2012. The subjective physiological, psychological, and behavioral risk‐taking consequences of alcohol and energy drink co‐ingestion. Alcohol Clin Exp Res 36: 2008–2015. [DOI] [PubMed] [Google Scholar]
- Penning R, de Haan L, Verster JC. 2011. Caffeinated drinks, alcohol consumption, and hangover severity. The Open Neuropsychopharmacology Journal 4: 36–39. [Google Scholar]
- Price SR, Hilchey CA, Darredeau C, Fulton HG, Barrett SP. 2010. Energy drink co‐administration is associated with increased reported alcohol ingestion. Drug Alcohol Rev 29: 331–333. [DOI] [PubMed] [Google Scholar]
- Snipes DJ, Benotsch EG. 2013. High‐risk cocktails and high‐risk sex: examining the relation between alcohol mixed with energy drink consumption, sexual behavior, and drug use in college students. Addict Behav 38: 1418–1423. [DOI] [PubMed] [Google Scholar]
- Trapp GS, Allen KL, O'Sullivan T, Robinson M, Jacoby P, Oddy WH. 2014. Energy drink consumption among young Australian adults: associations with alcohol and illicit drug use. Drug Alcohol Depend 134: 30–37. [DOI] [PubMed] [Google Scholar]
- Verster JC, Aufricht C, Alford C. 2012. Energy drinks mixed with alcohol: misconceptions, myths, and facts. Int J Gen Med 5: 187–198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verster JC, Benson S, Scholey A. 2014. Motives for mixing alcohol with energy drink (AMED) and other non‐alcoholic beverages, and consequences for overall alcohol consumption. International Journal of General Medicine 7: 285–293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verster JC, Benjaminsen JME, van Lanen JHM, van Stavel NMD, Olivier B. 2015. Effects of mixing alcohol with energy drink on objective and subjective intoxication: results from a Dutch on‐premise study. Psychopharmacology (Berl) 232: 835–842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wells BE, Kelly BC, Pawson M, LeClair A, Parsons JT, Golub SA. 2013. Correlates of concurrent energy drink and alcohol use among socially active adults. Am J Drug Alcohol Abuse 39: 8–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woolsey C, Waigandt A, Beck NC. 2010. Athletes and energy drinks: reported risk‐taking and consequences from the combined use of alcohol and energy drinks. J Appl Sport Psychol 22: 65–71. [Google Scholar]
- Woolsey CL, Jacobson BH, Williams RD, Jr , et al. 2015. A comparison of the combined‐use of alcohol & energy drinks to alcohol‐only on high‐risk drinking and driving behaviors. Subst Use Misuse 50: 1–7. [DOI] [PubMed] [Google Scholar]