

Abstract
Self-determination theory and self-efficacy theory are prominent theories in the physical activity literature, and studies have begun integrating their concepts. Sweet, Fortier, Strachan and Blanchard (2012) have integrated these two theories in a cross-sectional study. Therefore, this study sought to test a longitudinal integrated model to predict physical activity at the end of a 4-month cardiac rehabilitation program based on theory, research and Sweet et al.’s cross-sectional model. Participants from two cardiac rehabilitation programs (N=109) answered validated self-report questionnaires at baseline, two and four months. Data were analyzed using Amos to assess the path analysis and model fit. Prior to integration, perceived competence and self-efficacy were combined, and labeled as confidence. After controlling for 2-month physical activity and cardiac rehabilitation site, no motivational variables significantly predicted residual change in 4-month physical activity. Although confidence at two months did not predict residual change in 4-month physical activity, it had a strong positive relationship with 2-month physical activity (β=0.30, P<0.001). The overall model retained good fit indices. In conclusion, results diverged from theoretical predictions of physical activity, but self-determination and self-efficacy theory were still partially supported. Because the model had good fit, this study demonstrated that theoretical integration is feasible.
Key words: exercise, theory integration, cardiac rehabilitation
Introduction
Physical activity (broadly defined in this paper to include structure exercise such as a cardiac rehabilitation program and leisure time physical activity that is participated outside of the program) has been linked to a multitude of physical and psychological health benefits, including improvements in cardiovascular outcome,1 and as a protective factor for coronary heart disease.2 As such, physical activity (e.g., a structured exercise program) is a central component of cardiac rehabilitation. In this context, physical activity/structured exercise has been found to prevent cardiac mortality, all-cause mortality and also lower total cholesterol, triglycerides and systolic blood pressure.3 Even though the benefits of physical activity are clear, physical activity still remains low in cardiac patients.4,5 Therefore, enhancing our understanding of the factors that help increase physical activity for individuals with cardiovascular disease is an important research priority.
Motivational variables have been found to be the strongest and most consistent predictors of physical activity in both healthy6,7 and cardiac populations.8 Because these motivational variables are modifiable and frequently have a theoretical base, they have been deemed crucial to investigate.9 Two strong motivational theories applied in the physical activity domain are self-efficacy theory (SET)10 and self-determination theory (SDT)11.
Recently, experts have urged that such theories be integrated to build on their strengths and thus gain more insight on the behavior change process.12,13 Moreover, SDT researchers14,15 have recently recommended the integration of SDT with other theories to improve our understanding of physical activity. Sweet, Fortier, Strachan and Blanchard have recently tested an SDT-SET integrated model and found support for the integrated model.16 However, this model was evaluated with a convenience sample of university students and used a cross-sectional design. The purpose of this study was to test a similar SDT and SET integrated model evaluated by Sweet and colleagues but with a longitudinal design. In addition, this study was conducted with cardiac rehabilitation participants to further understand physical activity in this population and to extend the integrated model to another population. To contextualize the integration of SET and SDT, the respective theories are described in the following sections, followed by recent integration studies which lead up to the purpose of the present study.
Self-efficacy theory
Within SET, behavior is influenced by both self-efficacy and outcome expectations, where outcome expectation mediates the self-efficacy-behavior relationship. Three common forms of self-efficacy are task, barrier and scheduling self-efficacy. Task self-efficacy refers to the general confidence in one’s ability to perform a task/behavior (e.g., physical activity).10 Barrier self-efficacy is defined by how confident an individual is to participate in physical activity when faced with specific barriers associated with physical activity (i.e., scared of having a cardiac event).17 Finally, scheduling self-efficacy examines one’s confidence to organize their time and responsibilities around physical activity.18,19
Overall, self-efficacy has been strongly linked with physical activity for both healthy adults and cardiac patients.7,8 Within a cardiac population, Millen and Bray demonstrated that barrier self-efficacy predicted cardiac rehabilitation attendance during the program as well as physical activity at 6 weeks post-program, while task self-efficacy influenced physical activity at 12 weeks post-program.20 Other studies supported the relationship between task and barrier self-efficacy on physical activity in cardiac individuals.17,21 Scheduling self-efficacy has also been found to positively predict physical activity in a cardiac population.19 Hoeever, few studies have tested this type of self-efficacy in predicting physical activity in a cardiac population, but its use is strongly recommended.20,22
Individuals perceptions of the benefits or costs associated with a behavior such as physical activity defines SET’s second construct outcome expectations. In SET, outcome expectations are set to predict the behavior; however, this link is not clearly established in physical activity research.23 As suggested by Williams and colleagues, outcome expectations may have a more important role in predicting self-efficacy than physical activity. Indeed, we confirmed this relationship in a cross-sectional analysis of SET.16 Based on the research presented, the model tested in this study had outcome expectations as a predictor of self-efficacy and self-efficacy holding direct relationship with physical activity.
Self-determination theory
As described in SDT, the sequence toward behavior change is explained by the relationships between: autonomy support → psychological needs → self-determined motivation → behavior (physical activity). Autonomy support is at its highest when an individual perceives that his/her social context provides choices and options, and acknowledges their feelings and perspectives.24 In SDT, higher levels of perception of autonomy support are purported to lead to greater satisfaction of the three psychological needs. The satisfaction of the needs of autonomy (i.e., feeling one has volition and is the source of his/her own actions), competence (i.e., feeling able and capable of experiencing opportunities), and relatedness (i.e., feeling connected with others) are then hypothesized to translate to self-determined forms of motivation.
In SDT, there are two broad types of motivation, namely self-determined motivation and non self-determined motivation.25 On the one hand, self-determined motivation is characterized by one valuing the benefits of physical activity and/or deriving pleasure and satisfaction in its participation. On the other hand, non self-determined motivation is explained by external (e.g., following the doctor’s orders) and/or internal pressures (e.g., feeling of guilt) for engaging in physical activity. More self-determined forms of motivation lead to more positive consequences such as physical activity partecipation.
In a physical activity context, self-determined motivation has been found to predict physical activity adoption26,27 and maintenance.28 Although a limited number of studies have investigated SDT constructs in adults with cardiovascular disease, the few existing studies have demonstrated a significant and positive relationship between self-determined motivation and physical activity.28-30 In this study, the majority of SDT tenets were held constant with autonomy support linking with the psychological needs, which were then linked with motivation. Self-determined and non self-determined motivations were then set to predict physical activity.
Self-determination theory and self-efficacy theory
Because SDT and SET stem from the same meta-theoretical concept of agency, where humans are seen as active contributors of their behaviors, it is possible to integrate these theories. In addition, SDT and SET have received extensive support in physical activity research where some researchers have begun integrating concepts from both theories. For instance, the intrinsic motivation – physical activity relationship was found to be mediated by barriers self-efficacy in a community sample.31 Conversely, self-determined motivation was shown to mediate the relationship between barrier self-efficacy and long-term physical activity in adults with type 2 diabetes.32 In cardiac individuals, self-determined motivation and self-efficacy were revealed to be important predictors of physical activity changes after cardiac rehabilitation.28 In summary, these studies have demonstrated that the integration of SDT and SET concepts is a fruitful approach to predicting physical activity. However, these integration studies have mostly used specific concepts from each theory rather than testing entire theories.
As outlined by Noar and Zimmerman,12 it is best to test and integrate entire theories. This procedure was recently conducted by Sweet and colleagues with cross-sectional data.16 Specifically, each theory was tested separately and then integrated into one comprehensive model. This study revealed that theoretical integration was feasible as a similar amount of hypothesized relationships were found between the integrated model and the individual SDT and SET models. In addition, the integrated SDT-SET model accounted for more variance in physical activity, self-determined motivation and confidence than the individual theories and held well together in a path analytical model. Because the Sweet and colleagues study used cross-sectional data and that theoretical integration is at its infancy,16 it is imperative that a longitudinal investigation be conducted on this integration model, hence the purpose of this study.
Present study
The main objective of this study was to test a SDT and SET integrated longitudinal model to predict physical activity at 4 months (end of cardiac rehabilitation program). This study was the first to test an SDT-SET integrated model using longitudinal data. In addition, to extend the generalizability of the integrated model shown in Sweet and colleagues;16 a sample of cardiac rehabilitation participants was selected to test the model.
In line with SDT, we hypothesized that autonomy support will have a relationship with the needs of autonomy and relatedness. Both of these psychological needs were then expected to have a positive association with self-determined motivation and a negative one with non self-determined motivation. In this model, confidence (i.e., the integration of the need for competence in SDT and self-efficacy in SET) holds the assumption outlined in SET for self-efficacy. In this assumption, confidence plays an agency role, meaning that it drives behavior. Because confidence is placed in an agency role, the psychological needs of autonomy and relatedness were set to predict confidence, which remains consistent with Sweet and colleagues’ cross-section model.16 As outlined in the SET section, outcome expectations were hypothesized to be related with confidence.
Based on the tenets of SDT and results of past studies,28-30 self-determined and non self-determined motivations also assumed to hold an agency role and were hypothesized to have a positive and negative relationship with physical activity, respectively. Confidence was hypothesized to be directly linked with physical activity which is consistent with its agency role in SET and previous research.20 Overall, the hypothesized longitudinal SDT-SET integrated model, illustrated in Figure 1, is based on theory, past research and Sweet et al.’s cross-sectional SDT-SET integrated model.16
Figure 1.
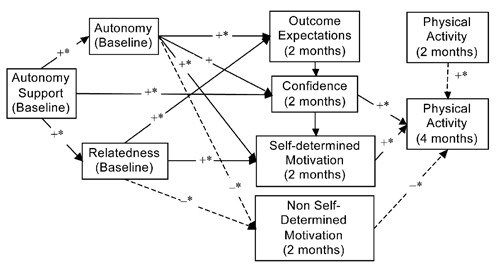
Hypothesized self-determination theory and self-efficacy theory models.
+* = positive significant relationship; + = positive non-significant relationship; – = negative non-significant relationship; → = path based on cross-sectional model; → = theoretical hypothesized path, not tested in cross-sectional model.
Materials and Methods
Procedures
All participants were referred by their physician to a center-based cardiac rehabilitation program. The cardiac rehabilitation program was an exercise-based program that was ran in a local fitness center. Participants were asked to attend two structured exercise sessions per week at the center and to participate in leisure time physical activity outside the sessions. Each participant received a tailored exercise program based on the participant’s cardiac profile. Participants were followed by a certified kinesiologist and nurse at each session for a 16 week period. The kinesiologist met regularly with the patient during the sessions to adjust the program accordingly (e.g., incorporate new activities such as resistance training). For this project, participants were approached during their first week at one of two 16-week center-based cardiac rehabilitation programs. Upon signing a consent form, a meeting was scheduled within the first two weeks for participants to answer the baseline questionnaire onsite [89% response rate (109/123)]. Everyone enrolled in the cardiac rehabilitation program was eligible, which included participants who had suffered a cardiac related event or were at high risk for cardiovascular disease. All questionnaires were answered at baseline, 2 months (mid-program) and 4 months (end of program). All steps were approved by the appropriate Research Ethics Board.
Participants
Study participants (N=109) enrolled in one of two cardiac rehabilitation programs were predominantly male (68%), French-speaking (68%), Caucasian (96%) and retired (64%) with a mean age of 62.28 years (SD=9.64). The majority of participants enrolled in the cardiac rehabilitation suffered a cardiac-related event (88%) while others were at high risk.
Measures
Physical activity
Using the Godin Leisure Time Exercise Questionnaire (GLTEQ),33 participants reported the number of days in a typical week in the past two months that they engaged in physical activity for more than 20 minutes for light, moderate and strenuous intensities. A total weekly leisure activity score was calculated by multiplying each frequency by three, five, and nine for mild, moderate and strenuous intensity, respectively, and then summing these scores. This questionnaire has been demonstrated as being valid and reliable.34,35
Self-determination theory variables
Autonomy support. At baseline, the Important Other Climate Questionnaire was used to assess participants’ perception of autonomy support.36 Each of the six items (e.g., My exercise important other listened to how I would like to do things regarding my physical activity) was anchored on a 7-point Likert scale ranging from strongly disagree (1) to strongly agree (7). A mean of the six items was calculated. The Cronbach’s alpha for this study was within acceptable range (alpha=0.81).
Psychological needs. At baseline, participants rated on a 6-point Likert scale ranging from 1 (false) to 6 (true) the 18 items from the validated Psychological Need Satisfaction in Exercise Scale.37 Each item reflected how participants might feel when they are physically active. For example, an item for autonomy (6 items) was I feel free to exercise in my own way, for competence (6 items) I feel that I am able to complete exercises that are personally challenging and for relatedness (6 items) I feel close to my exercise companions who appreciate how difficult exercise can be. A mean was calculated for each psychological need. For this study, high Cronbach’s alphas were found for autonomy (0.87), relatedness (0.90) and competence (0.90).
Motivations. Participants responded to the Behavioral Regulation Exercise Questionnaire-2 (BREQ-2) to measure motivation for physical activity at two months.38 On 5-point Likert scale ranging from 0 (not true for me) to 4 (very true for me), 19 items measured the types of motivational regulations on the self-determination continuum: amotivation (4 items, e.g. I think participating in physical activity is a waste of time), external regulation (4 items; e.g. I take part in physical activity because my friends/family/partner say I should), introjected regulation (3 items; e.g. I feel guilty when I don’t participate in physical activity), identified regulation (4 items; e.g. It’s important to me to participate in physical activity) and intrinsic regulation (4 items; e.g. I get pleasure and satisfaction from participating in physical activity). The BREQ-2 scale does not contain items measuring integrated regulation and thus four items from Wilson, Rodgers, Loitz, and Scime were included to assess this type of regulation (e.g. I consider exercise consistent with my values).39 The BREQ-2 and the additional integrated items have been shown to have good psychometric properties.38,39 The mean score of each motivational regulation was calculated. To test the findings from Sweet and colleagues16 and in line with previous research40 and SDT25 identified, integrated and intrinsic regulations were combined to created self-determined motivation (Cronbach’s alpha=0.89) while external and introjected regulation were aggregated for non self-determined motivation (Cronbach’s alpha=0.72).
Self-efficacy theory variables
Task self-efficacy. All SET variables were assessed at two months. Participants rated their confidence to engage in physical activity for more than 20 minutes during their free time for at least 1, 2, 3 up to 7 days per week over the next two months using a 0% (not at all confident) to 100% (completely confident) scale. This follows the graded approach recommended by Bandura.10 A mean percentage was calculated. In this study, this scale was reliable (Cronbach’s alpha=0.88).
Barrier self-efficacy. Using Blanchard and colleagues’17 validated barrier self-efficacy scale for individuals in cardiac rehabilitation, participants rated the degree of confidence to overcome nine different barriers over the next two months (e.g. fear of having a cardiac incident, bad weather, do not have time). Each item was rated on a scale ranging from 0 (not at all confident) to 100% (completely confident) and a mean of the nine items was calculated. This questionnaire was found to have good internal consistency (Cronbach’s alpha=0.89).
Scheduling self-efficacy. This seven-item measure was previously used in cardiac rehabilitation research to assess participants’ scheduling self-efficacy.18 Participants reported their confidence levels on a scale from 0 to 100% to all items for the next two months (e.g., organize time around each cardiac rehabilitation exercise session). The mean of the seven items was calculated. Good internal consistency was found for this scale (Cronbach’s alpha=0.88). Similar to the integration model from Sweet and colleagues, the need for competence and all three self-efficacies at 2-months were standardized and combined to create the concept of confidence (Cronbach’s alpha=0.92).
Outcome expectations. A 17-item validated scale assessed participants’ outcome expectations.41 This scale consisted of outcomes/benefits of physical activity (e.g.; less depressed, improve health/reduce disease risk). With a 5 point Likert scale (1 = strongly agree to 5 = strongly agree), participants rated their agreement of the impact of physical activity on each of these outcomes. A mean of the 17 items was calculated to create the score for outcome expectations. The internal consistency of this scale was good (Cronbach’s alpha=0.82).
Data analysis
Preiminary anayses
Following Tabachnick and Fidell’s data cleaning procedure,42 univariate and multivariate outliers, missing data, and normality of the variables were examined with SPSS v. 18 (IBM Corporation, 2010). Because recruitment and data collection were conducted at two different cardiac rehabilitation sites, a t-test was performed to determine if the outcome variable, physical activity at 4 months, differed between the two sites.
Man anayses
As previously mentioned, the integrated SDT-SET model is based on the model found in Sweet and colleagues16 and theoretical tenets (Figure 1). Due to the longitudinal nature of this study, we were able to enter physical activity at 2 months to predict physical activity at 4 months, creating a residual change score for physical activity at 4 months. Using Amos v. 18, the model was tested and further modified, if necessary, by removing non-meaningful paths and considering suggestions from the modification indices. Five goodness of fit indices: the chi-square goodness-of-fit, the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the standardized root mean residual (SRMR) were examined. Good model fit is indicated by a non-significant chi-square, a CFI of greater or equal to 0.90, a RMSEA of at least below 0.08, and a SRMR below 0.10 (preferably below 0.05).43
Results
Preliminary results
Two univariate outliers were reduced to one unit larger than the next highest value for the needs of autonomy at baseline and 2-month self-determined motivation and three univariate outliers were reduced for scheduling self-efficacy at 2 months. Differences in physical activity at 4 months were found by cardiac rehabilitation site, t=3.52, P<0.01. Therefore, a cardiac rehabilitation variable was entered in the model to control for this difference. Missing data ranged from 4.6% to 22.9% (mean percent missing: 15%; 97% complete baseline, 82% two months; 77% 4 months) and were found to be missing not at random. Specifically, those who were missing on physical activity had lower levels of confidence. Due to this result, the multiple imputation technique was conducted as it does not make assumptions about missing data pattern and is a respectable method of dealing with this type of missing data.42 This imputation technique resulted in the creation of five different imputed datasets. The model testing was conducted on each of the 5 datasets separately and the results were combined by averaging the corresponding regression coefficients, r-squared, and model fit indices. Standard errors were pooled using the equations outlined in Baraldi and Enders.44 These pooled standard errors were used to determine the significance of the path coefficients in the pooled model. The model of the imputed data was then compared to that of the original data (with missing values) to determine if the models differed. Once data were imputed, all variables were found to be normally distributed. One multivariate outlier was found which had a low autonomy support score with high levels of autonomy and low levels of relatedness. Because this combination is theoretically possible, the multivariate outlier was retained for the analyses.
Main analyses
Table 1 provides the means and correlations between study variables pooled across all five imputed datasets. The standardized beta coefficients, r-squares and model fit of each of the five datasets are in Table 2, while the averages of the standardized betas and r-squares are found on Figure 2. This figure illustrates the final SDT-SET integration model where non-meaningful links (standardized beta below ±0.10) are removed and modification indices were considered. Upon averaging the model fit indices of the five datasets, the final model was found to have good fit [chi-square (29) = 38.00, P=0.13; CFI=0.95; RMSEA=0.05, SRMR=0.08].
Table 1.
Means and correlations of self-determination theory and self-efficacy theory variables and physical activity included in the integrated model for the five pooled multiple imputation datasets.
| Variables | M | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Autonomy support (baseline) | 5.66 | - | 0.51* | 0.30* | 0.14 | 0.23* | 0.10 | 0.11 | -0.03 | -0.16 | 0.05 |
| Relatedness (baseline) | 4.75 | - | 0.51* | 0.12 | 0.20 | 0.04 | 0.19 | 0.04 | -0.14 | 0.14 | |
| Autonomy (baseline) | 5.14 | - | 0.19 | 0.25* | -0.10 | 0.26* | 0.03 | 0.02 | 0.09 | ||
| Confidence (2 months) | 0.00 | - | 0.34* | 0.15 | 0.38* | 0.29* | 0.11 | 0.01 | |||
| Self-determined motivation (2 months) | 3.07 | - | 0.22 | 0.33* | 0.07 | -0.11 | 0.19 | ||||
| Non self-determined motivation (2 months) | 1.50 | - | 0.02 | 0.01 | 0.01 | 0.01 | |||||
| Outcome expectations (2 months) | 4.07 | - | 0.03 | -0.17 | 0.24* | ||||||
| Physical activity (2 months) | 34.45 | - | 0.47* | -0.10 | |||||||
| Physical activity (4 months) | 34.52 | - | -0.24* | ||||||||
| Cardiac rehabilitation site | - | - |
*P<0.05.
Table 2.
Standardized coefficients and model fit indices for the five imputed datasets.
| MI 1 | MI 2 | MI 3 | MI 4 | MI 5 | |
|---|---|---|---|---|---|
| Paths | |||||
| Autonomy support → Autonomy | 0.29* | 0.27* | 0.29* | 0.31* | 0.32* |
| Autonomy support → Relatedness | 0.56* | 0.53* | 0.54* | 0.47* | 0.45* |
| Autonomy → Outcome expectations | 0.18 | 0.33* | 0.21* | 0.29* | 0.18 |
| Autonomy → Self-determined motivation | 0.04 | 0.17 | 0.22* | 0.08 | 0.22* |
| Autonomy → Non self-determined motivation | -0.24* | -0.20 | -0.18 | 0.13 | -0.08 |
| Relatedness →Self-determined motivation | 0.20 | -0.02 | 0.06 | 0.06 | 0.04 |
| Relatedness → Non self-determined motivation | 0.16 | 0.21 | 0.15 | 0.25 | -0.10 |
| Outcome expectations → Confidence | 0.48* | 0.37* | 0.34* | 0.34* | 0.30* |
| Confidence → Self-determined motivation | 0.27* | 0.22* | 0.32* | 0.40* | 0.28* |
| Confidence → Physical activity (2 months) | 0.25* | 0.30* | 0.32* | 0.33* | 0.28* |
| Self-determined motivation → Physical activity (4 months) | -0.12 | -0.13 | -0.08 | -0.18* | -0.09 |
| Physical activity (2 months)→ Physical activity (4 months) | 0.46* | 0.48* | 0.45* | 0.49* | 0.47* |
| Cardiac rehabilitation → Physical activity (4 months) | -0.19* | -0.15 | -0.20* | -0.16 | -0.18* |
| Cardiac rehabilitation → Self-determined motivation | 0.08 | 0.26** | 0.15 | 0.11 | 0.11 |
| Cardiac rehabilitation → Outcome satisfaction | 0.26* | 0.19* | 0.21* | 0.24* | 0.18 |
| Model fit indices | |||||
| Chi-square (df) | 34.66(29) | 41.25(29) | 40.47(29) | 35.36(29) | 38.25(29) |
| CFI | 0.97 | 0.93 | 0.94 | 0.96 | 0.93 |
| SRMR | 0.07 | 0.09 | 0.08 | 0.08 | 0.08 |
| RMSEA | 0.04 | 0.06 | 0.06 | 0.05 | 0.05 |
MI, multiple imputation; CFI, comparative fit index; RMSEA, root mean square error of approximation; SRMR, standardized root mean residual.
*P<0.05.
Figure 2.

Final self-determination/self-efficacy theory integrated model. Numbers in parentheses are derived from the dataset that included missing values. tP=0.06; *P<0.05
The results from the multiple imputation and original data compare favorably as most coefficients are similar aside from the relationship between baseline autonomy and 2-month non self-determined motivation and 2-month self-determined motivation and 4-month physical activity which were not significant for the imputation method but significant for the original data set with missing values (the imputation model was referred as the main model throughout the manuscript, as this imputation technique is more reliable than listwise deletion).45 In line with the hypothesized model, autonomy support predicted the needs of autonomy and relatedness and outcome expectation was related to confidence. In addition, the need of autonomy was a positive, although not significant, predictor of self-determined motivation. Confidence was significantly related to self-determined motivation. Contrary to the hypothesized model, the need of relatedness did not have a meaningful relationship with self-determined motivation, confidence and outcome expectations. Similarly, 2-month confidence was a predictor of 2-month physical activity rather than residual change in 4-month physical activity as highlighted by the modification indices. Two-month self-determined motivation was not significantly related to residual change in 4-month physical activity, and non self-determined motivation did not have a meaningful relationship with physical activity. Since 2-month physical activity accounted for a large amount of variance in 4-month physical activity, a regression analysis revealed a non-significant relationship (unstandardized beta=-3.54, t=-1.11, P>0.05) between 2-month self-determined motivation and 4-month physical activity (not controlling for 2-month physical activity).
Discussion
This study aimed to test a longitudinal integrated self-determination theory – self-efficacy theory model to predict physical activity at the end of a 4-month cardiac rehabilitation program. Therefore, this longitudinal integration model extends the previous Sweet and colleagues’16 study which was conducted with cross-sectional data. To our knowledge, the current study was the first to test a fully integrated model of SDT and SET in a physical activity context while using longitudinal data. Previous longitudinal studies combining these theories only tested specific concepts from each theory rather than all theoretical constructs from SDT and SET.28,32 In addition, this research answered the call from SDT researchers for integrating SDT with other prominent theories as well as added to the general literature on theory integration.12,14,15 The overall findings partially supported the hypothesized model. Specifically, the longitudinal model had good fit supporting the integration of the constructs from both theories in one integrated model and therefore supported Sweet and colleagues.16 Starting with autonomy support, it was found to predict the psychological needs of autonomy and relatedness which is in line with our hypotheses which were based on Sweet and colleagues.16 In addition, this relationship corroborated SDT and past research.46,47 Health care professionals should be autonomy supportive by acting in a warm and caring way (relatedness), expressing empathy (relatedness), minimizing pressure and control (autonomy), maximizing patients’ choice while providing a rationale for suggestions (autonomy) in order to increase satisfaction of these psychological needs. Next, confidence, which is comprised of competence from SDT, was the only psychological need that significantly predicted self-determined motivation. This significant relationship is congruent with Sweet et al.,16 previous research and SDT.48,49 However, autonomy and relatedness was not significantly related with self-determined motivation which was contrary to SDT. This finding is similar to Russel and Bray,30 who also found that only confidence was linked with self-determined motivation when all three needs were entered in one model. Therefore, it appears that for cardiac patients, competence is the key variable linking self-determined motivation. Given the limited amount of studies based in SDT in a cardiac setting, more research is needed to ascertain the true relationship between these constructs.
Moreover, outcome expectation was found to be a strong predictor of confidence, which is contrary to SET, but supports findings from Sweet and colleagues16 and suggestions by Williams and colleagues.23 Therefore, it appears that outcome expectation plays a role in predicting self-efficacy in a physical activity context. Based on these findings, interventions could therefore focus on fostering positive outcome expectations in order to build confidence.
With regards to physical activity at four months, this longitudinal model revealed that neither self-determined motivation nor confidence at two months significantly predicted residual change in physical activity at four months. First, the non-significant relationship between 2-month self-determined motivation and residual change in 4-month physical activity is contrary to SDT and previous physical activity research,40 including studies with a cardiac sample.29,30 However, another longitudinal study also reported a non-significant link between self-determined motivation and physical activity change.50 One explanation for this non-significant result is that self-determined motivation may be more important in the long-term27 and the follow-up period in the present study may not have been long enough to capture this relationship. Indeed, self-determined motivation has been hypothesized to play a larger role in maintaining health behaviors such as physical activity.51 In support of this premise, a recent study demonstrated that regular exercisers have stronger self-determined motivation compared to exercise initiates.52 Specific to cardiac individuals, self-determined motivation was shown to be an important predictor of physical activity maintenance after cardiac rehabilitation.28 Therefore, self-determined motivation may in fact play out in the later phases of behavior change. Future research should test an integrated SDT and SET model to predict long-term physical activity (i.e., 12 months).
Second, 2-month confidence had a significant relationship with 2-month physical activity rather than residual change at 4-month. This result is not consistent with our hypothesis, SET10 and past research.20 The non-significant relationship between the motivational variables of confidence and self-determined motivation with physical activity could be explained by a motivational-behavior gap. Therefore, the presence of other mediating /indirect factors might need to be considered to address this gap. Possible mediating factors are intentions and planning. Intentions have been found to mediate the relationship between self-determined motivation with physical activity.50 Another study with a cardiac population revealed that self-determined motivation had a stronger relationship with planning than with intentions.53 Other studies with cardiac rehabilitation participants have highlighted the role planning has played in predicting physical activity.54,55 Furthermore, a recent review of physical activity interventions demonstrated that self-regulation variables (such as planning) had the most support for a mediating effect on the intervention-physical activity relationship.56 Therefore, a more in depth investigation of the processes between motivational variables of self-determined motivation and confidence with physical activity is warranted.
Finally, past physical activity was found to be the sole significant predictor of physical activity at four months. This finding is consistent with previous research and SET.10,57 It is important to include past physical activity as prior studies often omitted this variable from analytical models despite being a consistent predictor of future behavior.57
Strengths, limitation and future research
The use of theory in predicting health behaviors such as physical activity is a strength of this study as theories have been underutilized in health behavior research.58,59 As previously mentioned, fully testing the integration model was a clear strength of this study due to the recent calls for theory integration.12,13 Although Sweet and colleagues16 integrated SDT and SET, they used a cross-sectional sample. Therefore, using longitudinal data in this study adds to the cross-sectional integration model and hints at the sequencing between constructs. In addition, using a longitudinal design fills a gap in the cardiac literature, since most studies with a cardiac population are cross-sectional in nature.8
The use of objective physical activity data would be needed in future research as the current investigation was based on a self-report physical activity questionnaire. This study had a small sample size which limited the analyses. With a larger and more diverse sample, future studies could retest this integrated model using structural equation modeling. Furthermore, a larger sample would allow future studies to test the longitudinal integrated model using an autoregressive/cross lagged model. This type of analysis would be of great benefit as it could determine what the best sequence is between all variables over the entire length of the 4-month program. Finally, this study was limited to four months and therefore future studies could focus on longer-term physical activity, especially post-cardiac rehabilitation program.
Conclusions
Although the motivational constructs did not predict residual change in 4-month physical activity, the integrated model still partially supported SDT and SET and had good model fit, suggesting that combining SDT and SET can hold together in one model. This integrative insight is especially important when looking at the broader social problem of physical inactivity. Instead of accumulating mini-literatures for each specific theory, as indicated by Noar and Zimmerman,12 we may gain more insight and knowledge on the physical activity behavior change process if we begin to join theoretical forces. Future research testing integrative models is still needed to augment our understanding of the constructs leading to physical activity participation.
Acknowledgements
The authors would like to thank study participants for their involvement in this study and the employees of the cardiac rehabilitation center. The authors would like to acknowledge Eva Guérin, Mélanie Perras, Alex Bernard and Isabelle Soucy for their research assistance throughout the project. This project was funded by the Social Science and Humanities Research Council of Canada (SSHRC) and MSF was the principal investigator. SNS was supported by a doctoral fellowship from SSHRC.
References
- 1.Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry 2005;18:189-93. [DOI] [PubMed] [Google Scholar]
- 2.Popkin BM, Kim S, Rusev ER, et al. Measuring the full economic costs of diet, physical activity and obesity-related chronic diseases. Obes Rev 2006;7:271-93. [DOI] [PubMed] [Google Scholar]
- 3.Taylor R, Brown A, Ebrahim S, et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med 2004;116:682-92. [DOI] [PubMed] [Google Scholar]
- 4.Wofford TS, Grennlund KJ, Croft JB, Labarthe DR. Diet and physical activity of U.S. adults with heart disease following preventive advice. Prev Med 2007;45:295-301. [DOI] [PubMed] [Google Scholar]
- 5.Zhao G, Ford ES, Li C, Mokdad AH. Are United States adults with coronary heart disease meeting physical activity recommendations? Am J Cardiol 2008;101:557-61. [DOI] [PubMed] [Google Scholar]
- 6.Pan SY, Cameron C, DesMeules M, et al. Individual, social, environmental, and physical environmental correlates with physical activity among Canadians: a cross-sectional study. BMC Public Health 2009;9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Trost SG, Owen N, Bauman AE, et al. Correlates of adults’ participation in physical activity: review and update. Med Sci Sports Exerc 2002;34:1996-2001. [DOI] [PubMed] [Google Scholar]
- 8.Petter M, Blanchard C, Kemp KAR, et al. Correlates of exercise among coronary heart disease patients: review, implications and future directions. Eur J Cardiovasc Prev Rehabil 2009;16:515-26. [DOI] [PubMed] [Google Scholar]
- 9.Baranowski T, Cullen K, Nicklas T, Thompson DB, J. Are current heath behaviour change models in guiding prevention of weight gain efforts? Obes Res 2003;11: S23-S43. [DOI] [PubMed] [Google Scholar]
- 10.Bandura A. Self-efficacy: the exercise of control. New York: Freeman and Company; 1997. [Google Scholar]
- 11.Deci EL, Ryan RM. Handbook of self-determination research. Rochester: University of Rochester Press; 2002. [Google Scholar]
- 12.Noar SM, Zimmerman RS. Health behavior theory and cumulative knowledge regarding health behaviors: are we moving in the right direction? Health Educ Res 2005;20:275-90. [DOI] [PubMed] [Google Scholar]
- 13.Nigg C, Allegrante JP, Ory M. Theory-comparison and multiple-behavior research: common themes advancing health behavior research. Health Educ Res 2002;17:670-9. [DOI] [PubMed] [Google Scholar]
- 14.Hagger MS, Chatzisarantis N. Self-determination theory and the psychology of exercise. Int Rev Sport Exerc Psychol 2008;1:79-103. [Google Scholar]
- 15.Wilson PM, Mack DE, Grattan KP. Understanding motivation for exercise: A self-determination theory perspective. Can Psychol 2008;49:250-6. [Google Scholar]
- 16.Sweet SN, Fortier MS, Strachan SM, Blanchard CM. Testing and integrating Self-Determination Theory and Self-Efficacy Theory in a physical activity context. Can Psychol 2012;53:319-27. [Google Scholar]
- 17.Blanchard CM, Rodgers WM, Courneya KS, et al. Does barrier efficacy mediate the gender-exercise adherence relationship during phase II cardiac rehabilitation? Rehabil Psychol 2002;47:106-20. [Google Scholar]
- 18.DuCharme KA, Brawley LR. Predicting the intentions and behavior of exercise initiates using two forms of self-efficacy. J Behav Med 1995;18:479-97. [DOI] [PubMed] [Google Scholar]
- 19.Woodgate J, Brawley LR, Weston ZJ. Maintenance cardiac rehabilitation exercise adherence: Effects of tasks and self-regulatory self-efficacy. J Appl Soc Psychol 2005;35:183-97. [Google Scholar]
- 20.Millen JA, Bray SR. Self-efficacy and adherence to exercise during and as a follow-up to cardiac rehabilitation. J Appl Soc Psychol 2008;38:2072-87. [Google Scholar]
- 21.Evon DM, Burns JW. Process and outcome in cardiac rehabilitation: an examination of cross-lagged effects. J Consult Clin Psychol 2004;72:605-16. [DOI] [PubMed] [Google Scholar]
- 22.Woodgate J, Brawley LR. Self-efficacy for exercise in cardiac rehabilitation: review and recommendations. J Health Psychol 2008;13:366-87. [DOI] [PubMed] [Google Scholar]
- 23.Williams DM, Anderson ES, Winett RA. A review of the outcome expectancy construct in physical activity research. Ann Behav Med 2005;29:70-9. [DOI] [PubMed] [Google Scholar]
- 24.Vansteenkiste M, Sheldon KM. There’s nothing more practical than a good theory: Integrating motivational interviewing and self-determination theory. Br J Clin Psychol 2006;45:63-82. [DOI] [PubMed] [Google Scholar]
- 25.Deci EL, Ryan RM. Facilitating optimal motivation and psychological well-being across life’s domains. Can Psychol 2008;49:14-23. [Google Scholar]
- 26.Fortier MS, Sweet SN, O’Sullivan TL, Williams GC. A self-determination process model of physical activity adoption in the context of a randomized controlled trial. Psychol Sport Exerc 2007. 9;8:741-57. [Google Scholar]
- 27.Teixeira PJ, Carraca EV, Markland D, et al. Exercise, physical activity, and self-determination theory: A systematic review. Int J Behav Nutr Phys Act 2012;9:78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mildestvedt T, Meland E, Eide GE. How important are individual counselling, expectancy beliefs and autonomy for the maintenance of exercise after cardiac rehabilitation? Scand J Public Health 2008;36:832-40. [DOI] [PubMed] [Google Scholar]
- 29.Russell KL, Bray SR. Promoting self-determined motivation for exercise in cardiac rehabilitation: The role of autonomy support. Rehabil Psychol 2010;55:74-80. [DOI] [PubMed] [Google Scholar]
- 30.Russell KL, Bray SR. Self-determined motivation predicts independent, home-based exercise following cardiac rehabilitation. Rehabil Psychol 2009;54:150-6. [DOI] [PubMed] [Google Scholar]
- 31.McNeill LH, Wyrwich KW, Brownson RC, et al. Individual, social environmental, and physical environmental influences on physical activity among black and white adults: a structural equation analysis. Ann Behav Med 2006;31:36-44. [DOI] [PubMed] [Google Scholar]
- 32.Sweet SN, Fortier MS, Guérin E, et al. Understanding physical activity in adults with type 2 diabetes after completing an exercise intervention trial: a mediation model of self-efficacy and autonomous motivation. Psychol Health Med 2009;14:419-29. [DOI] [PubMed] [Google Scholar]
- 33.Godin G, Shepard RJ. A simple method to assess exercise behavior in the community. Can J Appl Sport Sci 1985;10:141-6. [PubMed] [Google Scholar]
- 34.Jacobs DR, Ainsworth BE, Hartman TJ, Leon AS. A simultaneous evaluation of ten commonly used physical activity questionnaires. Med Sci Sports Exerc 1993;25:81-91. [DOI] [PubMed] [Google Scholar]
- 35.Kriska AM, Caspersen CJ. A collection of physical activity questionnaires for health-related research. Med Sci Sports Exerc 1997;29:S36-8. [PubMed] [Google Scholar]
- 36.Williams GC, Lynch MF, McGregor HA, et al. Validation of the important other climate questionnaire: Assessing autonomy support for health-related change. Fam Syst Health 2006;24:179-94. [Google Scholar]
- 37.Wilson PM, Rogers T, Rodgers WM, Wild TC. The psychological need satisfaction in exercise scale. J Sport Exerc Psychol 2006;28:231-51. [Google Scholar]
- 38.Markland D, Tobin V. A modification to the behavioural regulation in exercise questionnaire to include an assessment of amotivation. J Sport Exerc Psychol 2004;26:191-96. [Google Scholar]
- 39.Wilson PM, Rodgers WM, Loitz CC, Scime G. It’s who I am … really! The importance of integrated regulation in exercise contexts. J Appl Biobehav Res 2006;11:79-104. [Google Scholar]
- 40.Barbeau A, Sweet SN, Fortier M. A path-analytic model of self-determination theory in a physical activity context. J Appl Biobehav Res 2009;14:103-18. [Google Scholar]
- 41.Rogers LQ, Matevey C, Hopkins-Price P, et al. Exploring social cognitive theory constructs for promoting exercise among breast cancer patients. Cancer Nurs 2004;27:462-73. [DOI] [PubMed] [Google Scholar]
- 42.Tabachnick BG, Fidell LS. Using multivariate statistics. 5th ed. Boston: Allyn & Bacon; 2007. [Google Scholar]
- 43.Kline RB. Principles and practice of structural equation modeling. 2nd ed. New York: Guilford Press; 2005. [Google Scholar]
- 44.Baraldi AN, Enders CK. An introduction to modern missing data analyses. J School Psychol 2010;48:5-37. [DOI] [PubMed] [Google Scholar]
- 45.Schlomer GL, Bauman S, Card NA. Best practices for missing data management in counseling psychology. J Couns Psychol 2010;57:1-10. [DOI] [PubMed] [Google Scholar]
- 46.Markland D, Tobin VJ. Need support and behavioural regulations for exercise among exercise referral scheme clients: the mediating role of psychological need satisfaction. Psychol Sport Exerc 2010;11:91-9. [Google Scholar]
- 47.Silva MN, Markland D, Vieira PN, et al. Helping overweight women become more active: Need support and motivational regulations for different forms of physical activity. Psychol Sport Exerc 2010;11:591-601. [Google Scholar]
- 48.Edmunds JK, Ntoumanis N, Duda JL. A test of self-determination theory in the exercise domain. J Appl Soc Psychol 2006;36:2240-65. [Google Scholar]
- 49.Wilson PM, Rodgers WM, Blanchard CM, Gessell J. The relationship between psychological needs, self-determined motivation, exercise attitudes, and physical fitness. J Appl Soc Psychol 2003;33:2373-92. [Google Scholar]
- 50.Fortier MS, Kowal J, Lemyre L, Orpana HM. Intentions and actual physical activity behavior change in a community-based sample of middle-aged women: contributions from the theory of planned behavior and self-determination theory. Int J Sport Exerc Psychol 2009;9:46-67. [Google Scholar]
- 51.Rothman AJ, Baldwin AS, Hertel AW. Self-regulation and behavior change: distengangling behavioral initiation and behavioral maintenance. Baumeister R, Vohs K, eds. Handbook of self-regulation: research, theory and applications New York: Guilford; 2004. pp 130-148. [Google Scholar]
- 52.Rodgers WM, Hall CR, Duncan LR, et al. Becoming a regular exerciser: examining change in behavioural regulations among exercise initiates. Psychol Sport Exerc 2010;11:378-86. [Google Scholar]
- 53.Slovinec D’Angelo M, Reid RD, Pelletier LG. A model for exercise behavior change regulation in patients with heart disease. J Sport Exerc Psychol 2007;29:208-24. [DOI] [PubMed] [Google Scholar]
- 54.Sniehotta F, Scholz U, Schwarzer R. Action plans and coping plans for physical exercise: A longitudinal intervention study in cardiac rehabilitation. Br J Health Psychol 2006;11:23-37. [DOI] [PubMed] [Google Scholar]
- 55.Sniehotta F, Scholz U, Schwarzer R. Bridging the intention-behaviour gap: planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychol Health 2005;20:143-60. [Google Scholar]
- 56.Rhodes RE, Pfaeffli LA. Mediators of physical activity behaviour change among adult non-clinical populations: a review update. Int J Behav Nutr Phys Act 2010;7:37-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Weinstein ND. Misleading tests of health behavior theories. Ann Behav Med 2007;33:1-10. [DOI] [PubMed] [Google Scholar]
- 58.Painter JE, Borba CPC, Hynes M, et al. The use of theory in health behavior research from 2000 to 2005: A Systematic Review. Ann Behav Med 2008;35:358-62. [DOI] [PubMed] [Google Scholar]
- 59.Michie S, Johnston M, Abraham C, et al. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care 2005;14:26-33. [DOI] [PMC free article] [PubMed] [Google Scholar]