

Abstract
Study Design Cross-sectional study.
Objective Sacropelvic parameters in various spine and hip disorders have been published in various studies. We aimed to study the normal sacropelvic parameters and curvatures of the spine and their correlation in asymptomatic Indian adults in relation to variations in sex and age.
Methods The study included 101 asymptomatic adults (50 men and 51 women with an average age of 47.16 and 48.59 years, respectively). For each subject, the thoracic kyphosis (TK), lumbar lordosis (LL), pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS) were measured from standing lateral radiographs. After stratification of the group by sex and age with a cutoff of 50 years, descriptive, correlation, and regression analysis were performed using SPSS software.
Results The average PI, SS, PT, LL, and TK values were 55.48 (±5.31), 35.99 (±7.53), 17.97 (±7.16), 48.84 (±9.82), and 32.55 (±10.92), respectively. No statistically significant difference was observed in these values with regards to sex and age < 50 years and > 50 years but the pelvic incidence was found to be higher in women. A positive correlation between the PI and SS and a negative correlation between the SS and PT was observed. A positive correlation between the TK and LL was found in subjects > 50 years. Simple and multiple regression analyses were also performed for different groups.
Conclusion The current study is the first of asymptomatic Indian adults and provides invaluable information to the clinicians about the normal range of sacropelvic and spinopelvic parameters, which is useful to plan spinal deformity corrections and to evaluate pathologic conditions associated with abnormal angular values.
Keywords: sacropelvic parameters, lumbar lordosis, thoracic kyphosis, asymptomatic adults
Introduction
The influence of sacropelvic balance and morphology in the evaluation and treatment of developmental spondylolisthesis,1 2 3 4 5 6 degenerative spondylolisthesis,7 adolescent idiopathic scoliosis,8 and adult spinal deformity has been investigated in various studies.9 The role of sacropelvic morphology and balance in the pathogenesis and surgical treatment of hip osteoarthritis has been stated in some reports.10 As a basis for comparison, it is therefore important to document the sacropelvic balance and morphology in the normal population. Few studies in the literature have noted the normal values of these parameters in adults,11 12 13 14 15 but no study has documented the normal sacropelvic parameters and their correlation in the Indian population. Boulay et al did not find any significant difference in the sacral slope (SS), pelvic tilt (PT), or pelvic incidence (PI) between adult women and men.12 On the contrary, Vialle et al found statistically significant differences in the SS and PI but not the PT between female and male subjects.14 A weak statistical relationship not likely to be clinically significant was observed between different age groups and the PI, SS, and PT. The SS and PT were not related to age. Hammerberg and Wood evaluated 50 asymptomatic subjects aged 70 to 85 years and did not find any relationship between increasing age and sacropelvic parameters of balance and morphology, with the mean PT and PI higher than those observed previously in younger adults.15 Mac-Thiong et al documented values for these parameters in their population and did not find any difference in these values between male and female subjects.16
With this background, we aimed to study the various sacropelvic parameters and the sagittal alignment of the spine in a prospective cohort of 101 normal asymptomatic subjects in the Indian population to provide a baseline value of the sacropelvic parameters.
Materials and Methods
A prospective cohort of 101 normal asymptomatic adults who attended the outpatient department of Sir Gangaram hospital from March 2013 to June 2013 with no complaints related to spine were included in the study after obtaining clearance from the Institute's ethical committee. Subjects included 50 men and 51 women with an average age of 47.16 and 48.59 years, respectively. A standing left lateral radiograph exposing C7 to S1 and both the hips with a long 36-inch cassette placed at 72 cm from the X-ray tube was performed by a single radiographer to avoid bias. The subjects were instructed to stand in a comfortable position with the hips and knees fully extended.17 The sacropelvic parameters were then measured by a single observer using the KEOPS software (Images Viewer v.3.2.1.0). For each subject, the thoracic kyphosis (TK), lumbar lordosis (LL), PI, PT, and SS were measured (Fig. 1).
Fig. 1.
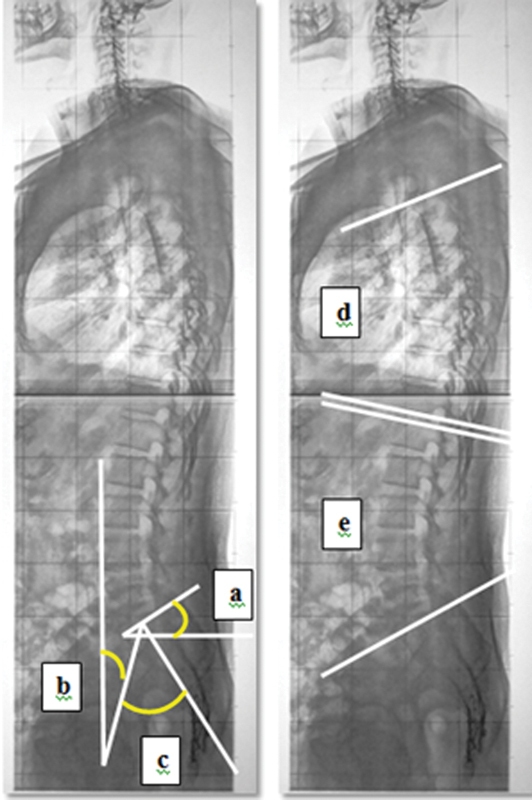
Angular parameters measured in standing whole-spine lateral view X-ray. (a) Sacral slope; (b) pelvic tilt; (c) pelvic incidence; (d) thoracic kyphosis; (e) lumbar lordosis.
The TK was measured from the superior end plate of T3 to the inferior end plate of T12. The LL was measured from the superior end plate of L1 to the superior end plate of S1 in standing lateral views. The PI was measured as the angle between two lines: the first line is from the middle of a line connecting the center of each femoral heads to the midpoint of the superior sacral end plate and the second line is perpendicular to the superior sacral end plate. The angle between the vertical and a line drawn from center of a line connecting the center of each femoral head to the midpoint of the superior sacral end plate was measured for obtaining the PT, and the angle between the horizontal line and the superior sacral end plate was used for SS (Fig. 1).
Statistical analyses were performed using the SPSS version 17.0 program for Windows. We conducted a Shapiro-Wilk test to verify the distribution of the data. All data was summarized as the mean ± standard deviation (SD). The chi-square test was used to compare the differences in variables between the two groups. The Student t test was used for continuous, normal variables. Pearson correlation analyses were used to assess the correlations among parameters. The variables were entered into a multiple linear regression analysis if their p value was less than 0.05 in the univariate analysis to assess independent association. The assumptions of regression model was also met; error terms were constant (homoscedasticity) and were normally distributed.
Results
The average PI was 55.48 (±5.31), SS was 35.99 (±7.53), PT was 17.97 (±7.16), LL was 48.84 (±9.82), and TK was 32.55 (±10.92; Table 1). The results revealed a statistically significant difference in PI between men and women with women having a higher PI. The PT, SS, LL, and TK did not show any statistically significant difference between sex and age (Tables 2 3 4 to 5). The average difference between LL and TK was −16 degrees. The SS was greater than half of PI.
Table 1. Values of various parameters.
| n | Minimum | Maximum | Mean | Standard deviation | |
|---|---|---|---|---|---|
| Age | 101 | 18 | 79 | 44.91 | 15.811 |
| Sacral slope (degrees) | 101 | 10 | 50 | 35.99 | 7.531 |
| Pelvic tilt (degrees) | 101 | 9 | 43 | 17.97 | 7.167 |
| Pelvic incidence (degrees) | 101 | 43 | 62 | 55.48 | 5.311 |
| Lumbar lordosis (degrees) | 101 | 27 | 78 | 48.84 | 9.827 |
| Thoracic kyphosis (degrees) | 101 | 10 | 59 | 32.55 | 10.927 |
Table 2. Values of the parameters in women.
| n | Minimum | Maximum | Mean | Standard deviation | |
|---|---|---|---|---|---|
| Age | 51 | 18 | 73 | 48.59 | 13.234 |
| Sacral slope (degrees) | 51 | 13 | 48 | 35.87 | 7.786 |
| Pelvic tilt (degrees) | 51 | 9 | 43 | 19.06 | 7.587 |
| Pelvic incidence (degrees) | 51 | 44 | 62 | 57.93 | 3.993 |
| Lumbar lordosis (degrees) | 51 | 29 | 78 | 50.53 | 9.301 |
| Thoracic kyphosis (degrees) | 51 | 12 | 59 | 33.91 | 11.264 |
Table 3. Values of the parameters in men.
| n | Minimum | Maximum | Mean | Standard deviation | |
|---|---|---|---|---|---|
| Age | 50 | 18 | 79 | 41.16 | 17.408 |
| Sacral slope (degrees) | 50 | 10 | 50 | 36.12 | 7.338 |
| Pelvic tilt (degrees) | 50 | 10 | 41 | 16.86 | 6.602 |
| Pelvic incidence (degrees) | 50 | 43 | 60 | 53.03 | 4.646 |
| Lumbar lordosis (degrees) | 50 | 27 | 71 | 47.12 | 10.140 |
| Thoracic kyphosis (degrees) | 50 | 10 | 55 | 31.17 | 10.504 |
Table 4. Values of the parameters in subjects < 50 years of age.
| n | Minimum | Maximum | Mean | Standard deviation | |
|---|---|---|---|---|---|
| Age | 52 | 18 | 48 | 32.17 | 10.401 |
| Sacral slope (degrees) | 52 | 16 | 50 | 36.02 | 7.324 |
| Pelvic tilt (degrees) | 52 | 9 | 41 | 17.55 | 6.767 |
| Pelvic incidence (degrees) | 52 | 45 | 60 | 53.57 | 4.365 |
| Lumbar lordosis (degrees) | 52 | 27 | 78 | 46.87 | 9.479 |
| Thoracic kyphosis (degrees) | 52 | 12 | 52 | 30.24 | 9.644 |
Table 5. Values of the parameters in subjects > 50 years of age.
| n | Minimum | Maximum | Mean | Standard deviation | |
|---|---|---|---|---|---|
| Age | 49 | 50 | 79 | 58.43 | 6.599 |
| Sacral slope (degrees) | 49 | 10 | 46 | 35.97 | 7.821 |
| Pelvic tilt (degrees) | 49 | 10 | 43 | 18.42 | 7.613 |
| Pelvic incidence (degrees) | 49 | 43 | 62 | 54.43 | 4.463 |
| Lumbar lordosis (degrees) | 49 | 29 | 76 | 50.94 | 9.848 |
| Thoracic kyphosis (degrees) | 49 | 10 | 59 | 35.00 | 11.747 |
Irrespective of age and sex, there was a positive correlation between the PI and SS (Tables 6 7 8 to 9). Regardless of age and sex, there was a statistically significant negative correlation between the SS and PT (Tables 6 to 9). There was no correlation between the PT and LL or TK. A statistically significant positive correlation was observed in our study between the LL and TK in subjects > 50 years of age (Tables 6 7 8 to 9). We did not find a significant correlation between the PI and LL. A regression analysis was performed using multiple variables to predict the SS, PT, and LL based on PI. A regression analysis was also performed to predict the LL based on age (Table 10). Equations were also calculated for predicting the PI based on the SS and the LL based on the TK for men, women, and subjects < 50 years and > 50 years of age (Tables 11 and 12).
Table 6. Correlation between the parameters in men.
| PI | SS | PT | LL | TK | |
|---|---|---|---|---|---|
| PI | 1 | 0.474a | 0.178 | 0.222 | 0.086 |
| SS | 1 | −0.781a | 0.141 | −0.132 | |
| PT | 1 | 0.000 | 0.096 | ||
| LL | 1 | 0.232 | |||
| TK | 1 |
Abbreviations: LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; TK, thoracic kyphosis.
p < 0.01.
Table 7. Correlation between the parameters in women.
| PI | SS | PT | LL | TK | |
|---|---|---|---|---|---|
| PI | 1 | 0.306a | 0.213 | 0.165 | 0.016 |
| SS | 1 | −0.865b | 0.099 | −0.072 | |
| PT | 1 | 0.015 | 0.082 | ||
| LL | 1 | 0.257 | |||
| TK | 1 |
Abbreviations: PI, pelvic incidence; LL, lumbar lordosis; PT, pelvic tilt; SS, sacral slope; TK, thoracic kyphosis.
p < 0.05.
p < 0.01.
Table 8. Correlation between the parameters in subjects with age < 50 years.
| PI | SS | PT | LL | TK | |
|---|---|---|---|---|---|
| PI | 1 | 0.421a | 0.190 | 0.246 | 0.044 |
| SS | 1 | −0.811a | 0.250 | −0.071 | |
| PT | 1 | 0.112 | 0.049 | ||
| LL | 1 | 0.115 | |||
| TK | 1 |
Abbreviations: LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; TK, thoracic kyphosis.
p < 0.01.
Table 9. Correlation between the parameters in subjects with age > 50 years.
| PI | SS | PT | LL | TK | |
|---|---|---|---|---|---|
| PI | 1 | 0.340a | 0.239 | 0.178 | 0.144 |
| SS | 1 | −0.831a | 0.009 | 0.097 | |
| PT | 1 | 0.116 | 0.021 | ||
| LL | 1 | 0.318b | |||
| TK | 1 |
Abbreviations: LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; TK, thoracic kyphosis.
p < 0.01.
p < 0.05.
Table 10. Simple and multivariate linear correlations between various spinopelvic and sacropelvic parameters in entire study group.
| Linear regression models | Variable | R 2 |
|---|---|---|
| SS = 1.804 + 0.634 PI | PI | 0.145 |
| PT = − 0.739 + 0.347 PI | PI | 0.048 |
| LL = − 21.751 + 0.347 PI | PI | 0.051 |
| LL = − 42.926 − 0.127 age | Age | 0.042 |
Abbreviations: LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; TK, Thoracic kyphosis.
Table 11. Simple and multivariate linear correlations between various spinopelvic and sacropelvic parameters in men and women.
| Linear regression models | Variable | R 2 | Beta coefficient standard error |
|---|---|---|---|
| Men | |||
| PI = 42.183 + 0.300 SS | SS | 0.225 | 0.08 |
| LL = 40.154 + 0.224 TK | TK | 0.054 | 0.136 |
| Women | |||
| PI = 47.854 + 0.184 SS | SS | 0.06 | 0.104 |
| LL = 43.332 + 0.212 TK | TK | 0.066 | 0.114 |
Abbreviations: LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; TK, thoracic kyphosis.
Table 12. Simple and multivariate linear correlations between various spinopelvic and sacropelvic parameters in subjects < 50 years and subjects > 50 years of age.
| Linear regression models | Variable | R 2 | Beta coefficient standard error |
|---|---|---|---|
| <50 y | |||
| PI = 42.913 +0.283 SS | SS | 0.120 | 0.108 |
| LL = 43.438 + 0.113 TK | TK | 0.013 | 0.138 |
| >50 y | |||
| PI = 47.450 + 0.194 SS | SS | 0.116 | 0.078 |
| LL = 41.626 + 0.266 TK | TK | 0.101 | 0.116 |
Abbreviations: LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; TK, Thoracic kyphosis.
Discussion
The spinopelvic and sacropelvic parameters of the spine and pelvis have been emphasized in various studies in the literature. They play a vital role not only in the spinal pathology but also in the hip pathology. The normal values of these parameters have been described by several authors in their respective populations, but the current study presents the largest cohort of normal asymptomatic Indian adults for the evaluation of the spinopelvic and sacropelvic parameters. According to our study, there is no difference in the SS, PT, LL, and TK between men and women but the PI is higher in women compared with men. Similarly, we found no difference in the PI, PT, SS, LL, and TK between subjects < 50 years and subjects > 50 years of age.
Mac-Thiong et al and Zhu et al reported no difference in the PI, PT, or SS between men and women, revealing no relationship between sex and spinopelvic parameters.16 18 In contrast to these studies, we found that Indian women have a higher PI compared with men. According to Mac-Thiong et al, the mean ± 2 SD range was 52.6 ± 10.4 degrees, 13.0 ± 6.8 degrees, and 39.6 ± 7.9 degrees for the PI, PT, and SS, respectively,16 whereas the values given by Zhu et al were 44.6 ± 11.2 degrees for the PI, 11.2 ± 7.8 degrees for the PT, and 32.5 ± 6.5 degrees for the SS, respectively.18 Vialle et al postulated mean values ± 2 standard deviations as 60 ± 10 degrees for LL, 41 ± 8.4 degrees for the SS, 13 ± 6 degrees for the PT, 55 ± 10.6 degrees for the PI.14 A strong correlation was found between the SS and the PI (r = 0.8), between the maximum LL and SS (r = 0.86), between the PI and PT (r = 0.66), and between the LL and PI, PT, and TK (r = 0.9) in their study. However, comparison of these values between sex and different age groups were not formulated in these studies. Kim et al compared these parameters between the young and elderly and found that the TK and PI were higher in the elderly subjects.19 Our study showed a statistically significant positive correlation between the PI and SS, a negative correlation between the SS and PT irrespective of the age and sex, and a positive correlation between the LL and TK in subjects greater than 50 years of age. However, in contrast to other studies, our study did not show a statistically significant correlation between the LL and PI. As age advances, disk degeneration increases, resulting in loss of disk height and thus a loss of lordosis. To compensate, the TK also decreases to maintain the sagittal balance. This fact is clinically important when planning long segment fixations and fusions in elderly patients, so that adequate LL can be achieved along with an increased TK to prevent proximal junctional failures, which is a potential complication in these patients.
Lafage et al emphasized the importance of the spinopelvic parameters in the treatment of patients with deformities and also their influence in osteotomies in these patients.20 Glattes et al showed that patients who were slightly kyphotic at the proposed proximal junction compared with the average sagittal alignment in a normal population were not at a higher risk for developing a junctional kyphosis.21
Surgeries to correct the spinal deformities ideally should aim at a proper relationship between the sacropelvic parameters and the TK and LL, but a pronounced breach in this relationship can result in a less favorable clinical outcome. No studies in the literature have given the correlation between these parameters and the spinal curvatures, especially in asymptomatic subjects. This study is the first to correlate these parameters, which will give an insight about the amount of osteotomy required to correct deformities and in cases requiring long segment instrumentation and fusions. A positive correlation between the PI and SS was found in our study, which indicates that subjects with a high PI tend to have higher values of SS. Similarly, a negative correlation between the SS and PT implies that as the SS increases, the PT decreases and vice versa to maintain a constant PI. Hence, while planning for fixation and fusion in patients with a high PI, an adequate SS should be attained intraoperatively by maintaining adequate lordosis, failure of which will result in pelvic retroversion as a result of compensatory increase in the PT. There was a significant positive correlation between the LL and the TK in subjects > 50 years of age. Hence, while planning for long segment fixations in the elderly population, an adequate LL corresponding to the TK should be achieved to avoid proximal junctional failures and other complications.
Conclusion
The current study presents the largest cohort of normal asymptomatic subjects for the evaluation of the sacropelvic and spinopelvic parameters in the Indian population. The range of values of the PI, PT, and SS corresponding to the mean ± 2 SD can provide invaluable information to clinicians about the normal range of values expected in 95% of the population, thus serving as a baseline in the evaluation and management of spinal disorders. The correlations between these parameters is of profound importance in calculating the corrections required in spinal deformities.
Footnotes
Disclosures G. Sudhir, none Shankar Acharya, none Kalra K.L., none Rupinder Chahal, none
References
- 1.Hresko M T, Labelle H, Roussouly P, Berthonnaud E. Classification of high-grade spondylolistheses based on pelvic version and spine balance: possible rationale for reduction. Spine (Phila Pa 1976) 2007;32(20):2208–2213. doi: 10.1097/BRS.0b013e31814b2cee. [DOI] [PubMed] [Google Scholar]
- 2.Jackson R P, Phipps T, Hales C, Surber J. Pelvic lordosis and alignment in spondylolisthesis. Spine (Phila Pa 1976) 2003;28(2):151–160. doi: 10.1097/00007632-200301150-00011. [DOI] [PubMed] [Google Scholar]
- 3.Labelle H, Roussouly P, Berthonnaud E. et al. Spondylolisthesis, pelvic incidence, and spinopelvic balance: a correlation study. Spine (Phila Pa 1976) 2004;29(18):2049–2054. doi: 10.1097/01.brs.0000138279.53439.cc. [DOI] [PubMed] [Google Scholar]
- 4.Labelle H, Roussouly P, Chopin D, Berthonnaud E, Hresko T, O'Brien M. Spino-pelvic alignment after surgical correction for developmental spondylolisthesis. Eur Spine J. 2008;17(9):1170–1176. doi: 10.1007/s00586-008-0713-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mac-Thiong J-M, Wang Z, de Guise J A, Labelle H. Postural model of sagittal spino-pelvic alignment and its relevance for lumbosacral developmental spondylolisthesis. Spine (Phila Pa 1976) 2008;33(21):2316–2325. doi: 10.1097/BRS.0b013e318186b236. [DOI] [PubMed] [Google Scholar]
- 6.Mac-Thiong J-M Labelle H Parent S Hresko M T Deviren V Weidenbaum M; members of the Spinal Deformity Study Group. Reliability and development of a new classification of lumbosacral spondylolisthesis Scoliosis 2008319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Barrey C Jund J Perrin G Roussouly P Spinopelvic alignment of patients with degenerative spondylolisthesis Neurosurgery 2007615981–986., discussion 986 [DOI] [PubMed] [Google Scholar]
- 8.Mac-Thiong J-M, Labelle H, Charlebois M, Huot M P, de Guise J A. Sagittal plane analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type. Spine (Phila Pa 1976) 2003;28(13):1404–1409. doi: 10.1097/01.BRS.0000067118.60199.D1. [DOI] [PubMed] [Google Scholar]
- 9.Gottfried O N, Daubs M D, Patel A A, Dailey A T, Brodke D S. Spinopelvic parameters in postfusion flatback deformity patients. Spine J. 2009;9(8):639–647. doi: 10.1016/j.spinee.2009.04.008. [DOI] [PubMed] [Google Scholar]
- 10.Lazennec J Y, Riwan A, Gravez F. et al. Hip spine relationships: application to total hip arthroplasty. Hip Int. 2007;17 05:S91–S104. [PubMed] [Google Scholar]
- 11.Mac-Thiong J-M, Labelle H, Berthonnaud E, Betz R R, Roussouly P. Sagittal spinopelvic balance in normal children and adolescents. Eur Spine J. 2007;16(2):227–234. doi: 10.1007/s00586-005-0013-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Boulay C, Tardieu C, Hecquet J. et al. Sagittal alignment of spine and pelvis regulated by pelvic incidence: standard values and prediction of lordosis. Eur Spine J. 2006;15(4):415–422. doi: 10.1007/s00586-005-0984-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Berthonnaud E, Dimnet J, Roussouly P, Labelle H. Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. J Spinal Disord Tech. 2005;18(1):40–47. doi: 10.1097/01.bsd.0000117542.88865.77. [DOI] [PubMed] [Google Scholar]
- 14.Vialle R, Levassor N, Rillardon L, Templier A, Skalli W, Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am. 2005;87(2):260–267. doi: 10.2106/JBJS.D.02043. [DOI] [PubMed] [Google Scholar]
- 15.Hammerberg E M, Wood K B. Sagittal profile of the elderly. J Spinal Disord Tech. 2003;16(1):44–50. doi: 10.1097/00024720-200302000-00008. [DOI] [PubMed] [Google Scholar]
- 16.Mac-Thiong J M, Roussouly P, Berthonnaud E, Guigui P. Age- and sex-related variations in sagittal sacropelvic morphology and balance in asymptomatic adults. Eur Spine J. 2011;20 05:572–577. doi: 10.1007/s00586-011-1923-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Vialle R, Levassor N, Rillardon L, Templier A, Skalli W, Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am. 2005;87(2):260–267. doi: 10.2106/JBJS.D.02043. [DOI] [PubMed] [Google Scholar]
- 18.Zhu Z, Xu L, Zhu F. et al. Sagittal alignment of spine and pelvis in asymptomatic adults: norms in Chinese populations. Spine (Phila Pa 1976) 2014;39(1):E1–E6. doi: 10.1097/BRS.0000000000000022. [DOI] [PubMed] [Google Scholar]
- 19.Kim W J, Kang J W, Yeom J S. et al. A comparative analysis of sagittal spinal balance in 100 asymptomatic young and older aged volunteers. Journal of Korean Society of Spine Surgery. 2003;10(4):327–334. [Google Scholar]
- 20.Lafage V, Ames C, Schwab F. et al. Changes in thoracic kyphosis negatively impact sagittal alignment after lumbar pedicle subtraction osteotomy: a comprehensive radiographic analysis. Spine (Phila Pa 1976) 2012;37(3):E180–E187. doi: 10.1097/BRS.0b013e318225b926. [DOI] [PubMed] [Google Scholar]
- 21.Glattes R C, Bridwell K H, Lenke L G, Kim Y J, Rinella A, Edwards C II. Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: incidence, outcomes, and risk factor analysis. Spine (Phila Pa 1976) 2005;30(14):1643–1649. doi: 10.1097/01.brs.0000169451.76359.49. [DOI] [PubMed] [Google Scholar]