

Abstract
Study Design Retrospective radiologic study.
Objective The sagittal alignment of the cervical spine can be evaluated using either a lateral cervical radiograph or a whole-spine lateral view on which the cervical spine is included. To our knowledge, however, no report has compared the two. The purpose of this work is to identify the difference in radiographic parameters between the cervical spine lateral view and the whole-spine lateral view.
Methods We retrospectively analyzed 59 adult patients suffering from neck pain with cervical spine lateral radiographs and whole-spine lateral radiographs from November 2007 to December 2011. The radiographs were measured using standard techniques to obtain the following parameters from the two different radiographs: occipital–C2 angle, C2–C7 angle, C7–sternal angle, sternal slope, T1 slope, C2 central offset distance, the distance between C2 and C7 plumb lines, C4 anteroposterior (AP) diameter, the ratio of C2 central off distance to C4 AP diameter, the ratio of plumb lines' distance to C4 AP diameter.
Results We found that the occipital–C2 angle, sternal slope, and C4 AP diameter were similar, but the C2–C7 angle, C7–sternal angle, T1 slope, C2 central offset distance, distance between C2 and C7 plumb lines, ratio of C2 central off distance to C4 AP diameter, and ratio of plumb lines' distance to C4 AP diameter were different. However, the error of measurement was greater than the small angular and linear differences between the two views.
Conclusions Most numerical values of the measured radiographic parameters appear to be different between the two views. However, the two views are comparable because the numerical differences were smaller than the errors of measurement.
Keywords: radiographic comparison, cervical spine lateral radiograph, whole-spine lateral radiograph
Introduction
The sagittal alignment of the spine has important ramifications to the health-related quality of life.1 It varies with age,2 3 gender,4 spinal disease,5 6 and body position.7 8 9 10 Many researchers have evaluated the sagittal alignment of the cervical spine. However, they used different neck positions,7 8 as well as different radiographic views. Most commonly, these are cervical spine lateral radiographs and whole-spine lateral radiographs.4 11 12 13 14 However, to the best of our knowledge, there is no literature comparing the sagittal cervical parameters between these two views. The purpose of this study is to determine if the radiographic parameters for sagittal cervical alignment are comparable between these two views.
Materials and Methods
Study Participants
This retrospective study included adult patients from a single institution who had the radiographs taken to evaluate the neck pain. The criteria for inclusion were as follows: (1) age 20 years or older at the time of evaluation; (2) no contraindication for radiographic exposure (e.g., pregnancy, tumor); (3) agreement of patients to take both radiographs. This study was approved by the institutional review board (2013-I093). All participants provided informed consent.
Radiographic Measurement
The radiographic protocol was standardized. For each subject, cervical spine lateral radiographs were obtained with a 10 × 12-inch cassette at a 72-inch (182 cm) distance with the radiographic tube centered at the C4–C5 disk space with no magnification (Fig. 1). Subjects were instructed to stand in a comfortable position and keep their eyes forward with their arms extended on their chests (Fig. 1). Immediately after taking the cervical lateral radiographs, whole-spine lateral radiographs were taken with a 14 × 17-inch cassette at a 98.4-inch (250 cm) distance with the tube centered at the xiphoid process and with the subjects in a comfortable standing position, keeping their eyes forward and their arms crossed upon their chests without magnification (Figs. 2, 3). These postures for the radiographs may be common in clinical practice. The digital X-ray images were obtained and measured on the PACS system (Π view, Infinitt, Seoul, Korea).
Fig. 1.

Cervical spine lateral radiographs were obtained with a 10 × 12-inch cassette at a 72-inch distance with the radiographic tube centered at the C4–C5 disk space with subjects in a comfortable standing position, keeping their eyes forward and their arms extended on their chests without magnification.
Fig. 2.

Whole-spine lateral radiographs were taken with a 14 × 17-inch cassette at a 98.4-inch distance with the tube centered at the xiphoid process with subjects in a comfortable standing position, keeping their eyes forward and their arms crossed upon their chests without magnification.
Fig. 3.

Whole-spine lateral radiographs.
Cervical radiologic parameters were measured by two observers. Cervical spinal morphology was measured using the standard techniques to obtain the following parameters for the two different radiographs:
Occipital–C2 angle: Cobb angle between the McGregor line and the inferior end plate of axis (Fig. 4)
C2–C7 angle: Cobb angle between the inferior end plate of C2 and the inferior end plate of C7 (Fig. 4)
C7–sternal angle: Cobb angle between the inferior end plate of C7 and the anterior border of sternum (Fig. 4)
Sternal slope: Cobb angle between the anterior border of sternum and the horizontal line (Fig. 4)
T1 slope: Cobb angle between the superior end plate of T1 body and the horizontal line (Fig. 5)
C2 central offset distance: the distance between the center of C2 body and the line tangential to the posterior cortex of C7 body (Fig. 5)
Distance between the C2 and C7 plumb lines (Fig. 6)
C4 anteroposterior (AP) diameter (Fig. 6)
Fig. 4.
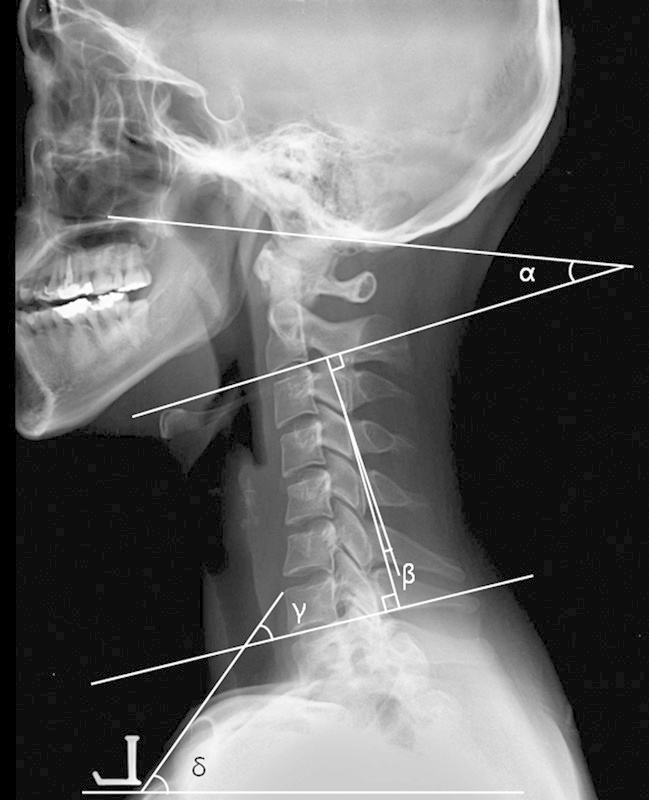
Angle α (occipital–C2) is formed by McGregor line and the inferior end plate of the axis; angle β (C2–C7), by the inferior end plate of C2 and inferior end plate of C7; angle γ (C7–sternal), by the inferior end plate of C7 and the anterior border of sternum; angle δ (sternal slope), by the anterior border of sternum and the horizontal line.
Fig. 5.

C2 central offset distance (a) is the distance between the center of C2 body and the line tangential to the posterior cortex of C7 body; T1 slope (ε) is the angle between the superior end plate of T1 body and the horizontal line.
Fig. 6.

The distance between C2 and C7 plumb lines (b to c) is the distance between C2 plumb line and C7 plumb line, the difference of b and c; C4 AP diameter (d) is anteroposterior diameter of C4 vertebral body.
Additionally, we calculated the ratio of C2 central offset distance to C4 AP diameter and the ratio of plumb lines' distance to C4 AP diameter to reduce the radiographic magnification (Figs. 5, 6).
Statistical Analysis
The statistical analysis was performed using SPSS version 13.0 (IBM corporation, Armonk, NY, United States). The differences in continuous variables between the two groups were examined with a paired t test. The power analysis was performed by G*Power version 3.1.5 (Universität Kiel, Germany). The power was 0.8 for paired t tests with the effect size of 0.5 and α error probability of 0.05. The sample size in each group should be more than 34. The statistical significance level was set at p < 0.05. The intraobserver and interobserver reliability were calculated using the reliability statistics by intraclass correlation for the Cobb angle and the distance. The intraclass correlation values were graded using previously described semiquantitative criteria: excellent for values in the 0.9 to 1.0 range, good for 0.7 to 0.89, fair/moderate for 0.50 to 0.69, low for 0.25 to 0.49, and poor for 0.0 to 0.24.
Finally, we compared the statistical difference of the previously mentioned parameters with the errors of measurement for the two different radiographs.
Results
Fifty-nine adults made up the study group (31 men and 28 women). The measurements of the Cobb angles in the cervical spine lateral radiographs had 0.979 intraobserver reliability and 0.966 interobserver reliability. The difference of the intraobserver measurements for the Cobb angles in the cervical spine lateral radiographs was 0.58 ± 2.74 degrees, and the difference of the interobserver measurements was 0.73 ± 3.43 degrees. The measurements of the C2 offset distance had 0.978 intraobserver reliability and 0.926 for interobserver reliability. The difference of the intraobserver measurements for the cervical spine distance in the lateral radiographs was 0.26 ± 3.05 mm, and the difference of the interobserver measurements was 0.90 ± 5.48 mm.
For the whole-spine lateral radiographs, the measurements of the Cobb angles had 0.969 intraobserver reliability and 0.803 interobserver reliability. The difference of the intraobserver measurements for the Cobb angles in the whole-spine lateral radiographs was 0.36 ± 3.65 degrees, and the difference of the interobserver measurements was 4.08 ± 7.78 degrees. The measurements of the C2 offset distance had 0.982 intraobserver reliability and 0.979 interobserver reliability. The difference of the intraobserver measurements for the distance in the whole-spine lateral radiographs was 4.67 ± 9.00 mm, and the difference of the interobserver measurements was 6.09 ± 9.48 mm.
The occipital–C2 angle, sternal slope, and C4 AP diameter were similar, but the C2–C7 angle, C7–sternal angle, T1 slope, C2 central offset distance, distance between C2 and C7 plumb lines, ratio of C2 central off distance to C4 AP diameter, and the ratio of plumb lines' distance to C4 AP diameter were statistically different (Table 1).
Table 1. Comparison of sagittal Cobb angles between the cervical spine lateral radiographs and whole-spine lateral standing radiographs.
| Cobb angles | Cervical spine lateral radiographs | Whole-spine lateral standing radiographs | Difference between two radiographs | p Value |
|---|---|---|---|---|
| Occipital–C2 angle (degrees) | −16.40 ± 6.93 | −15.42 ± 7.88 | −0.98 ± 6.52 | 0.254 |
| C2–C7 angle (degrees) | −8.35 ± 12.21 | −5.84 ± 12.24 | −2.51 ± 7.86 | 0.017 |
| C7–sternal angle (degrees) | 38.69 ± 7.70 | 42.42 ± 7.00 | −3.73 ± 6.71 | 0.000 |
| Sternal slope (degrees) | 62.74 ± 6.60 | 62.35 ± 5.73 | 0.39 ± 4.30 | 0.486 |
| T1 slope (degrees) | 25.15 ± 8.79 | 20.80 ± 9.18 | 4.35 ± 6.36 | 0.000 |
| C2 central off distance (mm) | −4.44 ± 13.56 | −0.06 ± 12.51 | −4.38 ± 10.04 | 0.001 |
| Distance between C2 and C7 plumb lines (mm) | 16.11 ± 11.52 | 11.70 ± 10.73 | 4.41 ± 7.63 | 0.000 |
| C4 AP diameter (mm) | 17.19 ± 4.65 | 16.93 ± 2.09 | 0.26 ± 3.90 | 0.611 |
| Ratio of C2 central off distance to C4 AP diameter | −0.30 ± 0.78 | −0.03 ± 0.75 | −0.27 ± 0.57 | 0.001 |
| Ratio of plumb lines' distance to C4 AP diameter | 0.92 ± 0.67 | 0.70 ± 0.65 | 0.22 ± 0.44 | 0.000 |
Abbreviation: AP, anteroposterior.
However, the error of measurement, especially interobserver measurements for the Cobb angles in the whole-spine lateral radiographs (4.08 ± 7.78 degrees) and distances (6.09 ± 9.48 mm), were greater than the angular statistical differences (−2.51 ± 7.86 degrees of C2–C7 angle) and linear statistical differences (−4.38 ± 10.04 mm of C2 central off distance) between the two types of radiographs (Table 1).
Discussion
Several methods have been described to evaluate the sagittal alignment of the cervical spine.4 7 8 11 12 13 However, they have used different neck positions and different radiographic techniques,7 8 including cervical spine lateral radiographs and whole-spine lateral radiographs.4 11 12 13 14 However, to the best of our knowledge, there is no literature comparing the sagittal cervical parameters obtained from cervical spine lateral views versus whole-spine lateral views.
In the current study, the occipital–C2 angle, sternal slope, and C4 AP diameter were similar. However, the C2–C7 angle, C7–sternal angle, T1 slope, C2 central offset distance, distance between C2 and C7 plumb lines, ratio of C2 central off distance to C4 AP diameter, and ratio of plumb lines' distance to C4 AP diameter were different. However, the angular and linear differences between the two types of radiographs were smaller than the error of measurement for the two types of radiographs.
The lordotic curvature of the cervical spine is considered as normal3; however, the exact values and the recommended methods of measurement are not clearly described. Normal lordotic angles for C2–C7 have been reported to range from 20 to 35 degrees,13 but these values are highly related to the method of measurement used and the positioning of the patients while taking a radiograph. Moreover, the head posture can influence the sagittal curve of the cervical spine.8 In addition, the arm or shoulder posture can influence sagittal spinal balance.9 10 According to Vedantam et al,10 positioning the arms at 90 degrees rather than 30 degrees resulted in a negative shift of the sagittal vertical axis. According to Marks et al,9 shoulder flexion of 30 degrees is the best position to use when a lateral radiograph is made to repeatedly measure the sagittal vertical axis. Also, cervical lordosis is increased when the thoracic kyphosis of the trunk is increased.4 14 In analyzing spinal sagittal alignment, it is most important to standardize the patients' posture while taking radiographs. We tried to keep the patients' standing posture as identical as possible to limit the effect of positioning.
Spine radiographs can be distorted by parallax.15 To limit the distortion, one can move the X-ray source away from the patient to reduce the divergence of the beam (conventional teleradiography) or translate the multiple focuses and coupled receptors simultaneously to scan the entire spine (digitalized teleradiography).15 The reasons for the differences in measurements for the two views include the differences in the centering target of the radiation beam, the distance from X-ray source to the cassettes, and the posture of arms between the two radiographs. Cervical spine lateral radiographs were taken at a 72-inch distance from the radiograph tube and centered at the C4–C5 disk space with the subject in a comfortable standing position with eyes forward and arms extended upon their chests. Whole-spine lateral radiographs were taken at a 98.4-inch distance from the tube and centered at the xiphoid process of the subject with eyes forward and arms crossed upon their chests.
The 95% confidence limits for intra- and interobserver variability of the Cobb method in the cervical lateral radiographs were 5 and 9 degrees with the traditional manual method.16 In many cases, a 5-degree variation between the measurements in the whole-spine lateral radiographs by the traditional manual Cobb method is acceptable.17 In the current study, the mean difference of the intra- and interobserver measurements for the Cobb angles in the cervical spine lateral radiographs with digital methods was 0.58 and 0.73 degrees. The mean difference of the intra- and interobserver measurements for the Cobb angles in the whole-spine lateral radiographs was 0.36 and 4.08 degrees. The reproducibility of the Cobb angle measurements with digitalized images appears better than those with traditional manual methods.18 The difference in the intraobserver measurements on the digitalized images of the distance in the cervical spine lateral radiographs was 0.26 ± 3.05 mm and the difference in the interobserver measurements was 0.90 ± 5.48 mm in the current study. The reproducibility of the distance measurements with digitalized images may be better than those with traditional manual methods, similar to Cobb angle measurements in the current study. However, we did not compare the reproducibility of the distance measurements using digitalized images with those using traditional manual methods.
As with any study, the present investigation has limitations. Arm posture was one reason for the difference between the cervical and whole-spine lateral radiographs. Ideally, we should have taken the two radiographs in the same arm posture to reduce the variables. However, we tried to compare the real-life situation in clinical practice and clinical research. To the best of our knowledge, this study is the first comparing sagittal cervical parameters between the cervical spine lateral view and whole-spine lateral view.
In conclusion, most numerical values of parameters for the two radiographic views appear to be different. However, the angular and linear numerical differences between the two radiographic views were smaller than the inter- and intraobserver errors of measurement for the two radiographic views. The two types of radiographs are comparable in clinical practice. Our results suggest that to determine the alignment of only the cervical spine, there is no advantage to using whole-spine lateral radiographs. However, this finding does not take into account the overall spinal alignment, for which whole-spine lateral radiograph are necessary.
Footnotes
Disclosures Moon Soo Park, none Seong-Hwan Moon, none Tae-Hwan Kim, none Jae Keun Oh, none Hwa Jun Kang, none K. Daniel Riew, none
References
- 1.Mac-Thiong J M, Transfeldt E E, Mehbod A A. et al. Can c7 plumbline and gravity line predict health related quality of life in adult scoliosis? Spine (Phila Pa 1976) 2009;34(15):E519–E527. doi: 10.1097/BRS.0b013e3181a9c7ad. [DOI] [PubMed] [Google Scholar]
- 2.Okada E, Matsumoto M, Ichihara D. et al. Aging of the cervical spine in healthy volunteers: a 10-year longitudinal magnetic resonance imaging study. Spine (Phila Pa 1976) 2009;34(7):706–712. doi: 10.1097/BRS.0b013e31819c2003. [DOI] [PubMed] [Google Scholar]
- 3.Mac-Thiong J M, Roussouly P, Berthonnaud E, Guigui P. Age- and sex-related variations in sagittal sacropelvic morphology and balance in asymptomatic adults. Eur Spine J. 2011;20 05:572–577. doi: 10.1007/s00586-011-1923-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Park M S, Moon S H, Lee H M. et al. The effect of age on cervical sagittal alignment: normative data on 100 asymptomatic subjects. Spine (Phila Pa 1976) 2013;38(8):E458–E463. doi: 10.1097/BRS.0b013e31828802c2. [DOI] [PubMed] [Google Scholar]
- 5.Rajnics P, Templier A, Skalli W, Lavaste F, Illes T. The importance of spinopelvic parameters in patients with lumbar disc lesions. Int Orthop. 2002;26(2):104–108. doi: 10.1007/s00264-001-0317-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Barrey C Jund J Perrin G Roussouly P Spinopelvic alignment of patients with degenerative spondylolisthesis Neurosurgery 2007615981–986., discussion 986 [DOI] [PubMed] [Google Scholar]
- 7.Harrison D E, Harrison D D, Janik T J, Holland B, Siskin L A. Slight head extension: does it change the sagittal cervical curve? Eur Spine J. 2001;10(2):149–153. doi: 10.1007/s005860000228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dvorak J, Froehlich D, Penning L, Baumgartner H, Panjabi M M. Functional radiographic diagnosis of the cervical spine: flexion/extension. Spine (Phila Pa 1976) 1988;13(7):748–755. doi: 10.1097/00007632-198807000-00007. [DOI] [PubMed] [Google Scholar]
- 9.Marks M, Stanford C, Newton P. Which lateral radiographic positioning technique provides the most reliable and functional representation of a patient's sagittal balance? Spine (Phila Pa 1976) 2009;34(9):949–954. doi: 10.1097/BRS.0b013e318199650a. [DOI] [PubMed] [Google Scholar]
- 10.Vedantam R, Lenke L G, Bridwell K H, Linville D L, Blanke K. The effect of variation in arm position on sagittal spinal alignment. Spine (Phila Pa 1976) 2000;25(17):2204–2209. doi: 10.1097/00007632-200009010-00011. [DOI] [PubMed] [Google Scholar]
- 11.Knott P T, Mardjetko S M, Techy F. The use of the T1 sagittal angle in predicting overall sagittal balance of the spine. Spine J. 2010;10(11):994–998. doi: 10.1016/j.spinee.2010.08.031. [DOI] [PubMed] [Google Scholar]
- 12.Kuntz C IV, Levin L S, Ondra S L, Shaffrey C I, Morgan C J. Neutral upright sagittal spinal alignment from the occiput to the pelvis in asymptomatic adults: a review and resynthesis of the literature. J Neurosurg Spine. 2007;6(2):104–112. doi: 10.3171/spi.2007.6.2.104. [DOI] [PubMed] [Google Scholar]
- 13.Erkan S, Yercan H S, Okcu G, Ozalp R T. The influence of sagittal cervical profile, gender and age on the thoracic kyphosis. Acta Orthop Belg. 2010;76(5):675–680. [PubMed] [Google Scholar]
- 14.Hardacker J W Shuford R F Capicotto P N Pryor P W Radiographic standing cervical segmental alignment in adult volunteers without neck symptoms Spine (Phila Pa 1976) 199722131472–1480., discussion 1480 [DOI] [PubMed] [Google Scholar]
- 15.Morvan G, Mathieu P, Vuillemin V. et al. Standardized way for imaging of the sagittal spinal balance. Eur Spine J. 2011;20 05:602–608. doi: 10.1007/s00586-011-1927-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Silber J S, Lipetz J S, Hayes V M, Lonner B S. Measurement variability in the assessment of sagittal alignment of the cervical spine: a comparison of the gore and cobb methods. J Spinal Disord Tech. 2004;17(4):301–305. doi: 10.1097/01.bsd.0000095824.98982.53. [DOI] [PubMed] [Google Scholar]
- 17.Cobb J R. Ann Arbor, MI: American Academy of Orthopedic Surgeons; 1948. Outline for the study of scoliosis; pp. 261–275. [Google Scholar]
- 18.Stokes I A, Aronsson D D. Computer-assisted algorithms improve reliability of King classification and Cobb angle measurement of scoliosis. Spine. 2006;31(6):665–670. doi: 10.1097/01.brs.0000203708.49972.ab. [DOI] [PubMed] [Google Scholar]