

Abstract
Study Design Systematic literature review and meta-analysis of studies published in English.
Objective This study evaluated differences in outcome variables between percutaneous and open pedicle screws for traumatic thoracolumbar fractures.
Methods A systematic review of PubMed, Cochrane, and Embase was performed. The variables of interest included postoperative visual analog scale (VAS) pain score, kyphosis angle, and vertebral body height, as well as intraoperative blood loss and operative time. The results were pooled by calculating the effect size based on the standardized difference in means. The studies were weighted by the inverse of the variance, which included both within- and between-study error. Confidence intervals were reported at 95%. Heterogeneity was assessed using the Q statistic and I 2.
Results After two-reviewer assessment, 38 studies were eliminated. Six studies were found to meet inclusion criteria and were included in the meta-analysis. The combined effect size was found to be in favor of percutaneous fixation for blood loss and operative time (p < 0.05); however, there were no differences in vertebral body height (VBH), kyphosis angle, or VAS scores between open and percutaneous fixation. All of the studies demonstrated relative homogeneity, with I 2 < 25.
Conclusions Patients with thoracolumbar fractures can be effectively managed with percutaneous or open pedicle screw placement. There are no differences in VBH, kyphosis angle, or VAS between the two groups. Blood loss and operative time were decreased in the percutaneous group, which may represent a potential benefit, particularly in the polytraumatized patient. All variables in this study demonstrated near-perfect homogeneity, and the effect is likely close to the true effect.
Keywords: thoracolumbar trauma, chance fracture, burst fracture, percutaneous fixation, spinal fracture, lumbar fracture, thoracic fracture, vertebral body fracture
Introduction
In an epidemiologic study by Hu et al,1 traumatic injuries to the thoracolumbar region comprised some 75% of total spinal skeletal injuries. Notably, a large portion of these thoracolumbar injuries specifically comprises the thoracolumbar junction (T10–L2). From a biomechanical perspective, the transfer of axially directly kinetic energy from a mobile lumbar spine to a stiff thoracic spine leads to a high incidence of injuries at this junction.2 3 Despite the propensity for fractures in this region, controversy continues to surround the treatment principles for these fractures.4 5 6 7
Open operative stabilization with pedicle instrumentation remains a familiar, prevalent treatment for thoracolumbar burst fracture. Denis et al recommended open prophylactic stabilization in thoracolumbar burst fractures even in the absence of neurologic deficit.4 The posterior open approach is considered appropriate for neurologically intact patients with burst fractures and posterior ligamentous complex injuries. The use of an open posterior approach for pedicle screw instrumentation and reduction of thoracolumbar fractures has shown good radiologic and clinical outcomes.8 9 10
With the advent of minimally invasive spine surgery, studies have evaluated the percutaneous approach versus the open approach for stabilization of thoracolumbar fractures. In a randomized controlled trial, Jiang et al found lower pain and better function in the percutaneous cohort.11 The minimally invasive surgery (MIS) approach to pedicle screw instrumentation of thoracolumbar fractures minimizes soft tissue injury, reduces intraoperative blood loss, and results in better postoperative pain scores than other approaches.5 11 12 13 14 15
To our knowledge, no systematic review or meta-analysis has evaluated comparative studies of the open versus percutaneous approach for thoracolumbar trauma. The primary goal of this study was to perform a meta-analysis to compare the clinical outcomes, blood loss, pain scores, and radiographic outcome scores defined by vertebral body height (VBH) and kyphosis deformity between the open and percutaneous transpedicular instrumentation and stabilization of thoracolumbar fractures.
Materials and Methods
Inclusion/Exclusion Criteria and Review Procedure
A systematic computerized Medline literature search was performed using PubMed, Cochrane Database of Systematic Reviews, and EMBASE. The electronic databases were searched for publication dates from January 1980 to June 2014. The searches were performed from Medical Subject Headings (MeSH) used by the National Library of Medicine. Specifically, MeSH terms “thoracolumbar trauma,” “thoracolumbar fracture,” “pedicle screw,” and “percutaneous pedicle screw” were used. The inclusion criteria in the meta-analysis included prospective randomized control trials or prospective/retrospective cohort studies, adult patients, thoracolumbar spine trauma, fixation with pedicle screws, a minimum of 6 months of follow-up, reported clinical outcomes, and a minimum of 10 patients for a given study.
Two independent authors reviewed abstracts of each article to determine which articles to include in the study. The authors jointly reviewed the full text of the articles meeting the inclusion criteria based on the abstract to determine agreement on the inclusion of the studies. In case of a discrepancy, a third author participated in the discussion until a consensus was reached.
Data Extraction
A meta-analysis database was created from the included studies with the following categories: (1) study ID to include author, journal, and year of publication; (2) reference; (3) study type and level of evidence; (4) study inclusion/exclusion criteria; (5) number of patients; (6) male-to-female ratio; (7) patient age; (8) length of follow-up; (9) open or percutaneous pedicle screw placement; (10) visual analog score (VAS) for pain; (11) average blood loss; (12) average length of surgery; (13) local kyphosis angle; (14) VBH.
Methodological Quality Assessment
Methodological quality assessment was accomplished using the Downs and Black checklist.16 The total cumulative score is comprised of a profile that measures quality of reporting, internal validity, and external validity. According to Downs and Black,16 the performance results of the checklist showed a high internal consistency (Kuder-Richardson Formula 20 = 0.89) and test–retest (r = 0.88) and interrater (r = 0.75) reliability. Specifically, the checklist consists of 27 items for which a “yes” answer is scored 1 and “no” or “unable to determine” answer is scored 0.
Meta-Analysis
The results were pooled by calculating the effect size based on the standardized difference in means using Comprehensive Meta Analysis, version 2.2.050 (Biostat, Englewood, New Jersey, United States). The studies were weighted in the meta-analysis by the inverse of the variance, which included both within- and between-study error. The effect size and confidence intervals were reported using Forest plots (Figs. 1 2 3 4 to 5). Confidence intervals were reported at 95% levels. Comparison between groups was performed using the Z distribution and a t test. A p value of 0.05 was set for significance. Heterogeneity was assessed using the Q statistic and I 2, where I 2 is the estimate of the percentage of error due to between-study variation. I 2 values below 25% generally indicate “excellent” consistency of results and homogeneous studies, and studies below 50% are described as “moderate” homogeneity according to Downs and Black.16 A priori we selected a random-effects model.
Fig. 1.
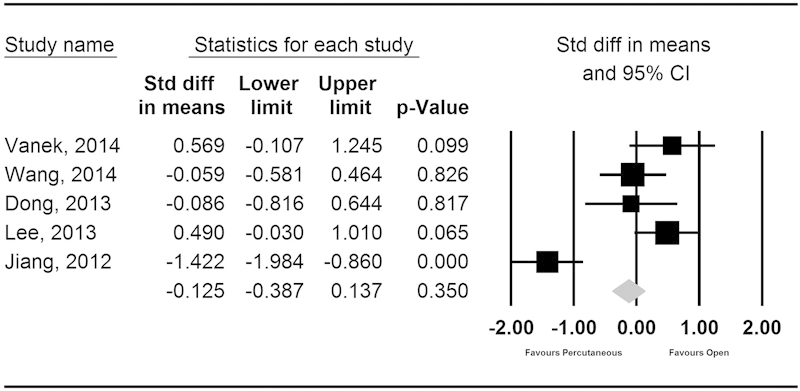
Forest plot of the standardized mean difference for vertebral body height. Abbreviations: CI, confidence interval; Std diff, standard deviation.
Fig. 2.
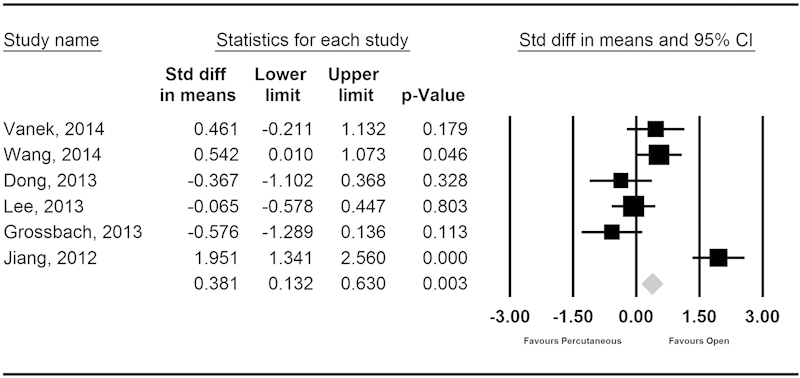
Forest plot of the standardized mean difference for post-operative kyphosis angle. Abbreviations: CI, confidence interval; Std diff, standard deviation.
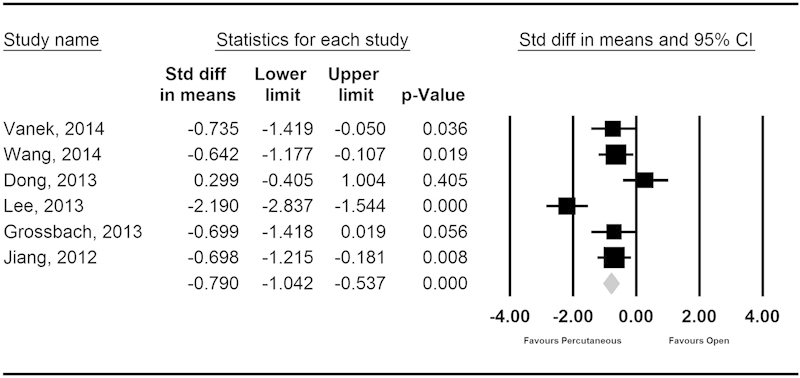
Fig. 3.
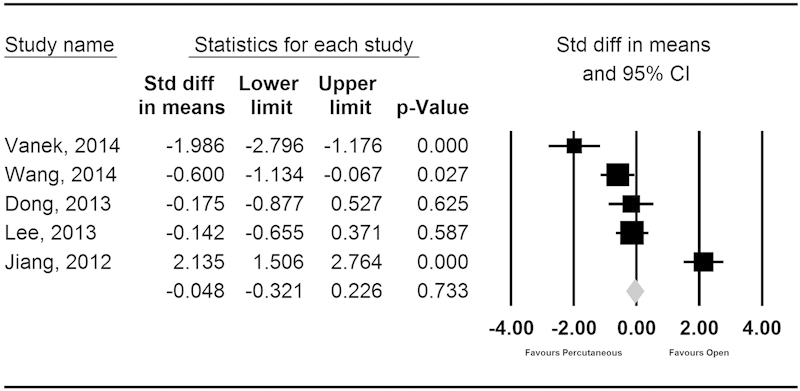
Forest plot of the standardized mean difference for visual analog scale. Abbreviations: CI, confidence interval; Std diff, standard deviation.
Fig. 4.
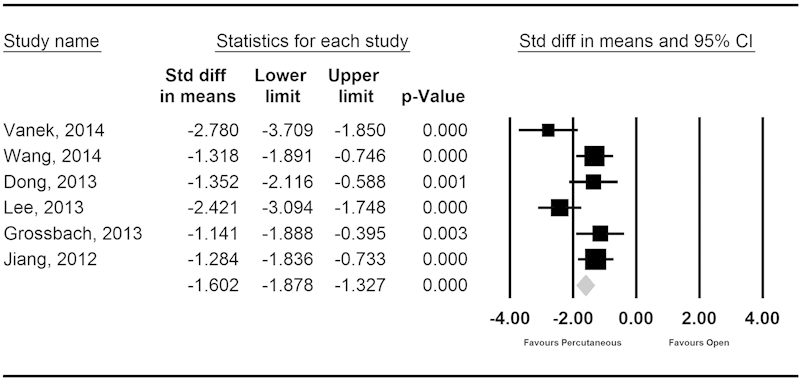
Forest plot of the standardized mean difference in blood loss. Abbreviations: CI, confidence interval; Std diff, standard deviation.
Fig. 5.
Forest plot of the standardized mean difference for operative time. Abbreviations: CI, confidence interval; Std diff, standard deviation.
Sensitivity analysis was performed by varying the assumptions used in the meta-analysis and by single elimination of the studies. Funnel plots of effect size versus standard error were assessed by visual inspection to determine publication bias.
Results
Systematic Review
The initial PubMed, Cochrane Review, and EMBASE search resulted in 44 articles.5 7 11 12 13 14 15 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 After two-reviewer assessments, 26 articles were eliminated after abstract review.18 19 20 21 22 25 27 28 29 30 32 34 37 38 39 41 42 44 45 46 47 51 52 53 54 Twelve additional studies were eliminated based on the inclusion criteria of the systematic review.17 23 24 26 31 33 35 36 40 43 47 50 Six studies were identified as meeting all of inclusion requirements.5 11 12 13 14 15 Descriptive information for each of the included studies is given in Tables 1 and 2.
Table 1. Summary of the demographic information for studies included in the meta-analysis.
| Study | Level of evidence | No. of patients | Age (y) | Duration of follow-up (mo) | Fracture type | Neurologic deficit | Fusion | Operative fixation |
|---|---|---|---|---|---|---|---|---|
| Vanek et al 201413 | II | A: 18; B:17 | A: 39.4; B: 45.6 | 24 | Thoracolumbar AO A3.1–A3.3 | No | No | A: open short-segment pedicle screw; B: MIS short-segment pedicle screw |
| Wang et al 201414 | III | A: 22; B: 39 | A: 46; B: 41.3 | A: 22.6; B: 21.7 | Thoracolumbar AO type A | No | No | A: open short-segment 4 pedicle screws; B: MIS short-segment 4 or 6 pedicle screws |
| Dong et al 201315 | III | A: 17; B: 21 | A: 36.3; B: 36.3 | 17.3 | Thoracolumbar AO type A, B1.2, or B2.3 | No | No | A: open short-segment pedicle screw; B: MIS short-segment pedicle screw |
| Lee et al 20135 | III | A: 32; B: 27 | A: 36.3; B: 36.3 | A: 30.2; B: 39.7 | Single-level thoracolumbar (T11–T12) | No | No | A: open short-segment pedicle screw; B: MIS short-segment pedicle screw |
| Grossbach et al 201312 | III | A: 11; B: 27 | A: 40.1; B: 27.4 | A: 9; B: 18.5 | Thoracolumbar flexion-distraction (AO B1.2 most common) | No | No | A: open short-segment pedicle screw; B: MIS short-segment pedicle screw |
| Jiang et al 201211 | I | A: 31; B: 30 | A: 42.4; B: 42.4 | 59 | Single-level thoracolumbar (T11–L2) | No | No | A: open short-segment pedicle screw; B: MIS short-segment pedicle screw |
Abbreviations: A, group A, open pedicle screw placement; B, group B, percutaneous pedicle screw placement; MIS, minimally invasive surgery.
Table 2. Summary of the statistics from the included studies.
| Study | Postoperative VBH | Postoperative kyphosis angle | Postoperative VAS | Postoperative blood loss (mL) | Operative time (min) |
|---|---|---|---|---|---|
| Vanek et al 201413 | A: 82 ± 3; B: 80 ± 3.99 | A: 4.2 ± 4.8; B: 2 ± 4.75 | A: 1.2 ± 0.3; B: 1.75 ± 0.25 | A: 56 ± 17; B: 331 ± 141 | A: 53 ± 10; B: 60 ± 9 |
| Wang et al 201414 | A: 88 ± 9.4; B: 88.6 ± 10.7 | A: 6.2 ± 6.2; B: 2.3 ± 7.7 | A: 0.7 ± 0.6; B: 1.1 ± 0.7 | A: 49.3 ± 34; B: 311.5 ± 246.5 | A: 98.4 ± 35.9; B: 140.3 ± 76.8 |
| Dong et al 201315 | A: 92.7 ± 9.3; B: 93.5 ± 9.3 | A: 3.8 ± 4.9; B: 5.9 ± 6.1 | A: 0.33 ± 0.49; B: 0.43 ± 0.60 | A: 18.3 ± 4.9; B: 27.6 ± 7.5 | A: 51.7 ± 11.2; B: 49.1 ± 7.5 |
| Lee et al 20135 | A: 91.2 ± 3.4; B: 89.6 ± 3.1 | A: 6.2 ± 5.1; B: 6.5 ± 3.9 | A: 1.7 ± 1.1; B: 1.9 ± 1.7 | A: 262.5 ± 34; B: 684.3 ± 239.9 | A: 83.2 ± 26.1; B: 154.9 ± 39.2 |
| Grossbach et al 201312 | – | A: 1.45 ± 7.98; B: 6.26 ± 8.48 | – | A: 93.6 ± 66.2; B: 498 ± 415 | A: 195 ± 42; B: 257 ± 101 |
| Jiang et al 201211 | A: 84.23 ± 9.47; B: 96.36 ± 7.48 | A: −0.39 ± 2.7; B: −9.25 ± 6.15 | A: 0.65 ± 0.15; B: 0.35 ± 0.13 | A: 79 ± 40.4; B: 145 ± 60.7 | A: 79.7 ± 12.7; B: 89.8 ± 16.1 |
Abbreviations: A, group A, open pedicle screw placement; B, group B, percutaneous pedicle screw placement; VAS, visual analog scale; VBH, vertebral body height.
Five studies reported postoperative VAS scores.5 11 13 14 15 Similarly, five studies reported postoperative VBH.5 11 13 14 15 Six studies reported information on operative time, blood loss, and postoperative kyphosis angle.5 11 12 13 14 15
Summary of Investigations
Wang et al retrospectively reviewed 100 patients who were treated with open or percutaneous pedicle screws after a thoracolumbar fracture.14 All fractures were Arbeitsgemeinschaft für Osteosynthesefragen (AO) type A fractures, and no patient had a neurologic deficit. Patients underwent either short-segment open pedicle instrumentation or MIS short-segment pedicle fixation with four or six screws. A fusion was not performed. Postsurgical improvement in the clinical outcomes was seen in terms of blood loss, operation time, postoperative hospital stay, and VAS scores (p < 0.05) in favor of the MIS group. Radiographically, postoperative sagittal Cobb's angle, vertebral body angle, and anterior VBH were similar between all treatment arms. In the open group, one patient had poor wound healing and one patient had a loose screw. In the four pedicle screw MIS group, pedicle screws broke in two patient, likely related to heavy activity.
Lee et al retrospectively found that postsurgical correction loss revealed no significant difference between MIS or the open group at final follow-up.5 All patients had single-level thoracolumbar fractures at T11–T12 without neurologic deficit. All patients underwent either open or MIS short-segment pedicle fixation without fusion. However, clinically, the authors observed a significant decrease in intraoperative blood loss and operation time in the MIS group. VAS outcomes became similar to those of the open group at final follow-up. One screw-rod failure with nonunion and two postoperative infections developed in the open surgery group. One case of screw pullout was observed in the percutaneous group, which was treated conservatively.
Vanek et al looked at 37 patients treated with either percutaneous or open posterior short-segment pedicle screw fixation without fusion.13 All patients were thoracolumbar AO type A3.1 to A3.3 without neurologic deficit. The authors found a significant decrease in mean surgical duration and mean perioperative blood loss in the MIS group. The VAS scores were also significantly lower in the first 7 postoperative days in the MIS group (p < 0.001). Notably, there were no significant differences between the groups in vertebral body index and Cobb's angle during follow-up. A comparison between those patients in whom pedicle screws were placed too medially on postoperative imaging showed no significant difference between groups (2 of 72 in the minimally invasive treatment group versus 5 of 68 in the control group; p = 0.265).
Grossbach et al, in a study evaluating 38 patients with flexion-distraction injuries (AO B1.2 was the most common), found no significant differences in the degree of kyphotic angulation between the MIS and open surgery groups.12 All patients underwent short-segment open or MIS pedicle fixation without fusion. The authors noted a significant decrease in perioperative blood loss in the MIS group compared with the open surgery group. In the open group, one patient developed a surgical site infection. One patient in each group (open and MIS) required revision for misplaced pedicle screws. Two patients in the MIS group underwent removal of hardware after their injuries were healed.
Dong et al evaluated 39 patients with thoracolumbar AO type A, B1.2, or B2.3 vertebral fractures without neurologic deficit.15 All patients underwent open or MIS short-segment pedicle fixation without fusion. The MIS group showed a significantly lower intraoperative blood loss and less severe postsurgical pain. No significant difference was observed in the operating time, postoperative relative vertebral height (p = 0.668), and regional kyphotic angle (p = 0.235) in the immediate postoperative and final follow-up period.
Jiang et al noted significantly less intraoperative blood loss and a shorter duration of surgery and hospitalization in the MIS group.11 All patients in this study sustained a fracture at T11–T12 without neurologic deficit. All patients underwent either open or MIS short-segment pedicle fixation without fusion. At final follow-up, both groups had similar VAS scores (p > 0.05). Open surgery produced a significantly better correction of kyphosis (local kyphosis angle, LKA) and restoration of VBH compared with the percutaneous approach at final follow-up (each p < 0.001). There were no instances of hardware failure before instrument removal in either group. Grade II screw misplacement was observed in 6/124 (4.8%) pedicle screws in the percutaneous group and 4/120 (3.3%) in the paraspinal group.
Quality Assessment of Included Studies
The quality index score of our six studies ranged from 14 to 18. We calculated an average score of 16.6 and a standard deviation of 1.5. We defined a higher-quality study as a score of 16 to 18, a moderate-quality study as a score of 13 to 15, and a poorer-quality study as a score of 8 to 12. There were five higher-quality studies and one moderate-quality study.
Meta-Analysis Results
Vertebral Body Height
Five studies reported the means and standard deviations for VBH. The point estimate for the effect size was −0.107, which was in favor of the percutaneous group, though not statistically significant (p = 0.773; Table 3; Fig. 1). There was perfect homogeneity among the studies for the assessment of VBH with a Q value of 3.767 and I 2 value of 0 (Table 3).
Table 3. Summary of the calculated effect sizes based on the standardized difference in means and assessment of study heterogeneity.
| Hedges' g effect size | 95% confidence intervals | ||||||
|---|---|---|---|---|---|---|---|
| Number of studies | Point estimate | Lower limit | Upper limit | p Value | Q value | I 2 | |
| VBH | 5.000 | −0.107 | −0.832 | 0.618 | 0.773 | 3.767 | 0 |
| Kyphosis angle | 6.000 | 0.335 | −0.376 | 1.045 | 0.356 | 5.242 | 4.616 |
| VAS | 5.000 | −0.142 | −1.325 | 1.041 | 0.814 | 4.781 | 16.337 |
| Blood loss | 6.000 | −1.673 | −2.175 | −1.171 | <0.0001 | 5.695 | 12.206 |
| Operative time | 6.000 | −0.782 | −1.383 | −0.181 | 0.011 | 5.554 | 9.975 |
Abbreviations: VAS, visual analog scale; VBH, vertebral body height.
Kyphosis Angle
Six studies reported the postoperative kyphosis angles after pedicle screw fixation. The point estimate for the effect size was 0.335, in favor of the open group (Table 3; Fig. 2); however, this difference was not statistically significant (p = 0.356). There was minimal heterogeneity among the studies with a Q value of 5.242 and I 2 value of 4.616 (Table 3).
VAS
Five studies reported the postoperative VAS scores. The point estimate for the effect size was −0.142, in favor of the percutaneous group (Table 3; Fig. 3). The difference between the two groups was not statistically significant (p = 0.814). There was minimal heterogeneity among the studies with a Q value of 4.781 and I 2 value of 16.337 (Table 3).
Blood Loss
Six studies reported the intraoperative blood loss. The point estimate for the effect size was −1.673 in favor of the percutaneous group, which was statistically significant (p < 0.0001; Table 3; Fig. 4). There was minimal heterogeneity among the studies with a Q value of 5.695 and I 2 value of 12.206 (Table 3).
Operative Time
Six studies reported the operative time. The point estimate for the effect size was −0.782 in favor of the percutaneous group, which was statistically significant (p = 0.011; Table 3; Fig. 5). There was minimal heterogeneity among the studies with a Q value of 5.554 and I 2 value of 9.975 (Table 3).
Sensitivity Analysis and Publication Bias
Single elimination of each study did not impact the overall results of the analysis for any of the five variables of interest. The percutaneous group maintained a statistically significant difference with respect to blood loss and operative time when compared with the open group. There was no statistical difference between the two groups for kyphosis angle, VBH, or VAS scores.
The funnel plats were symmetric about the mean effect for clinical success indicating an absence of publication bias within the studies.
Discussion
The operative treatment of thoracolumbar fractures requires a choice by the treating physician as to the optimal approach and means of fixation. Alvine et al and Esses et al both demonstrated good clinical and radiologic outcomes following the open instrumentation of thoracolumbar fractures.8 9 Advocates of the percutaneous technique cite decreased operative time, decreased blood loss, and decreased disruption of the already traumatized soft tissues. Conversely, opponents of the MIS technique cite the long surgeon learning curve and the possibility of inadequate restoration of VBH and local kyphosis.
The use of meta-analyses allows for the pooling of data from multiple studies to evaluate whether there is a significant effect and if so, the magnitude of the effect. Furthermore, the meta-analysis allows for the assessment of the heterogeneity, or variability within the studies, which further validates the effect size. In this study, we selected a random-effects model a priori. Unlike a fixed-effect model, the random-effects model allows that the true effect may vary from study to study.
When assessing the five variables of interest in our model, only blood loss and operative time were found to be significantly different among the two groups (Figs. 4 and 5). There were no significant differences between the two approaches in regards to restoration of VBH, local kyphosis angle, and postoperative VAS scores (Figs. 1 2 3). These results indicate that at a minimum, percutaneous fixation of thoracolumbar fractures results in equivalent biomechanics and clinical outcomes as the open group. In fact, Jiang et al showed no difference in the loss of VBH height correction at the latest follow-up between the two groups.11 Similarly, Lee et al showed a loss of 3.1 degrees in the percutaneous group versus 3.5 degrees in the open group for local kyphosis angle.5 Dong et al concluded that the percutaneous and open techniques did not result in significant differences in the curative effect or radiologic measurement data and that both approaches achieve a good curative effect.15
Lee et al, Vanek et al, and Dong et al all noted a significant difference in the immediate postoperative period in the VAS scores between the percutaneous and open groups, with significantly lower VAS scores noted in the percutaneous group.5 13 15 These scores tended to normalize around 6 months, with no differences in any study at the time of latest follow-up. The authors concluded that the early results are likely the result of early recovery of back muscle pain and function in the percutaneous group and that the extent of paraspinal muscle dissection continues to define the early clinical outcomes between the two groups. In a separate study, Kim et al reported percutaneous fixation caused less paraspinal muscle injury than did open fixation.55 The extent of paraspinal muscle injury was positively correlated with postoperative back muscle performance.
With the exception of Dong et al,15 every study demonstrated a significant decrease in operative time in the percutaneous group. Rahamimov et al and Smith et al reported that percutaneous pedicle screw placement in thoracolumbar burst fractures was a more time-consuming and technically demanding procedure.41 56 Although the results of our meta-analysis are unable to comment on the technical challenges faced during percutaneous pedicle screw placement, the results indicate that percutaneous pedicle screws require less operative time. The meta-analysis, however, is not powered to model any potential impact of an initial surgeon learning curve. Knox et al, Patel et al, and Park et al all commented on the challenges faced in the initial cases performed by a surgeon.57 58 59 The authors report an increased incidence of complications caused by screw misplacement, facet joint violations, and subsequent need for additional operative procedures.
In assessing the variability inherent among the studies, we found almost perfect homogeneity for all five of the variables. It can be assumed that the results reported for each study are consistent and likely represent the true effect. Furthermore, the results of this meta-analysis are validated through the performance of the sensitivity analysis. Single elimination of studies did not change the validity of the model for any variable.
Limitations are inherent with all meta-analyses, including the heterogeneity of the included studies, missed studies within our search, and unknown biases within the primary studies. A random-effects model was selected to control for some of the inherent heterogeneity among the studies; however, there was variability in the number of involved levels among cases, unspecified fracture types in many studies, and length of fixation constructs, and not all of the studies were stratified based on the number of levels treated. Furthermore, the use of surgical adjuncts, notably vertebroplasty or kyphoplasty, was poorly defined in the studies and could represent a potential confounder when discussing postoperative biomechanics stability.
Conclusion
Patients with thoracolumbar fractures can be effectively managed with percutaneous or open pedicle screw placement. There are no differences in VBH, kyphosis angle, or postoperative midterm VAS between the two groups. Blood loss and operative time were decreased in the percutaneous group, which may represent a potential benefit, particularly in the polytraumatized patient.
Footnotes
Disclosures Steven J. McAnany, none Samuel C. Overley, none Jun S. Kim, none Evan O. Baird, none Sheeraz A. Qureshi, Consultant: Stryker, Medtronic, Orthofix, Zimmer Paul A. Anderson, Consultant: Stryker, Pioneer, Aesculap; Royalties: Stryker, Pioneer; Stock/stock options: Si-Bone, Expanding Orthopedics, Titan Surgical
References
- 1.Hu R, Mustard C A, Burns C. Epidemiology of incident spinal fracture in a complete population. Spine (Phila Pa 1976) 1996;21(4):492–499. doi: 10.1097/00007632-199602150-00016. [DOI] [PubMed] [Google Scholar]
- 2.Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine (Phila Pa 1976) 1983;8(8):817–831. doi: 10.1097/00007632-198311000-00003. [DOI] [PubMed] [Google Scholar]
- 3.Ghobrial G M, Jallo J. Thoracolumbar spine trauma: review of the evidence. J Neurosurg Sci. 2013;57(2):115–122. [PubMed] [Google Scholar]
- 4.Denis F, Armstrong G W, Searls K, Matta L. Acute thoracolumbar burst fractures in the absence of neurologic deficit. A comparison between operative and nonoperative treatment. Clin Orthop Relat Res. 1984;(189):142–149. [PubMed] [Google Scholar]
- 5.Lee J K Jang J W Kim T W Kim T S Kim S H Moon S J Percutaneous short-segment pedicle screw placement without fusion in the treatment of thoracolumbar burst fractures: is it effective? Comparative study with open short-segment pedicle screw fixation with posterolateral fusion Acta Neurochir (Wien) 2013155122305–2312., discussion 2312 [DOI] [PubMed] [Google Scholar]
- 6.McLain R F Functional outcomes after surgery for spinal fractures: return to work and activity Spine (Phila Pa 1976) 2004294470–477., discussion Z6 [DOI] [PubMed] [Google Scholar]
- 7.Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003;85-A(5):773–781. doi: 10.2106/00004623-200305000-00001. [DOI] [PubMed] [Google Scholar]
- 8.Alvine G F, Swain J M, Asher M A, Burton D C. Treatment of thoracolumbar burst fractures with variable screw placement or Isola instrumentation and arthrodesis: case series and literature review. J Spinal Disord Tech. 2004;17(4):251–264. doi: 10.1097/01.bsd.0000095827.98982.88. [DOI] [PubMed] [Google Scholar]
- 9.Esses S I, Botsford D J, Kostuik J P. Evaluation of surgical treatment for burst fractures. Spine (Phila Pa 1976) 1990;15(7):667–673. doi: 10.1097/00007632-199007000-00010. [DOI] [PubMed] [Google Scholar]
- 10.Marco R A, Kushwaha V P. Thoracolumbar burst fractures treated with posterior decompression and pedicle screw instrumentation supplemented with balloon-assisted vertebroplasty and calcium phosphate reconstruction. J Bone Joint Surg Am. 2009;91(1):20–28. doi: 10.2106/JBJS.G.01668. [DOI] [PubMed] [Google Scholar]
- 11.Jiang X Z, Tian W, Liu B. et al. Comparison of a paraspinal approach with a percutaneous approach in the treatment of thoracolumbar burst fractures with posterior ligamentous complex injury: a prospective randomized controlled trial. J Int Med Res. 2012;40(4):1343–1356. doi: 10.1177/147323001204000413. [DOI] [PubMed] [Google Scholar]
- 12.Grossbach A J, Dahdaleh N S, Abel T J, Woods G D, Dlouhy B J, Hitchon P W. Flexion-distraction injuries of the thoracolumbar spine: open fusion versus percutaneous pedicle screw fixation. Neurosurg Focus. 2013;35(2):E2. doi: 10.3171/2013.6.FOCUS13176. [DOI] [PubMed] [Google Scholar]
- 13.Vanek P, Bradac O, Konopkova R, de Lacy P, Lacman J, Benes V. Treatment of thoracolumbar trauma by short-segment percutaneous transpedicular screw instrumentation: prospective comparative study with a minimum 2-year follow-up. J Neurosurg Spine. 2014;20(2):150–156. doi: 10.3171/2013.11.SPINE13479. [DOI] [PubMed] [Google Scholar]
- 14.Wang H Zhou Y Li C Liu J Xiang L Comparison of open versus percutaneous pedicle screw fixation using the sextant system in the treatment of traumatic thoracolumbar fractures J Spinal Disord Tech 2014; July 11 (Epub ahead of print) [DOI] [PubMed] [Google Scholar]
- 15.Dong S H, Chen H N, Tian J W. et al. Effects of minimally invasive percutaneous and trans-spatium intermuscular short-segment pedicle instrumentation on thoracolumbar mono-segmental vertebral fractures without neurological compromise. Orthop Traumatol Surg Res. 2013;99(4):405–411. doi: 10.1016/j.otsr.2012.12.020. [DOI] [PubMed] [Google Scholar]
- 16.Downs S H, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–384. doi: 10.1136/jech.52.6.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chen Z, Zhao J Q, Fu J W, Yang X M, Chen Q. [Modified minimally invasive percutaneous pedicle screws osteosynthesis for the treatment of thoracolumbar fracture without neural impairment] Zhonghua Yi Xue Za Zhi. 2010;90(21):1491–1493. [PubMed] [Google Scholar]
- 18.Chou D, Lu D C. Mini-open transpedicular corpectomies with expandable cage reconstruction. Technical note. J Neurosurg Spine. 2011;14(1):71–77. doi: 10.3171/2010.10.SPINE091009. [DOI] [PubMed] [Google Scholar]
- 19.Citak M, Stubig T, Kendoff D. et al. Navigated minimally invasive thoracolumbar pedicle screw placement with flat panel 3-D imaging. A feasibility study. Technol Health Care. 2010;18(2):101–110. doi: 10.3233/THC-2010-0572. [DOI] [PubMed] [Google Scholar]
- 20.Court C, Vincent C. Percutaneous fixation of thoracolumbar fractures: current concepts. Orthop Traumatol Surg Res. 2012;98(8):900–909. doi: 10.1016/j.otsr.2012.09.014. [DOI] [PubMed] [Google Scholar]
- 21.Cox J B, Yang M, Jacob R P, Pincus D W. Temporary percutaneous pedicle screw fixation for treatment of thoracolumbar injuries in young adults. J Neurol Surg A Cent Eur Neurosurg. 2013;74(1):7–11. doi: 10.1055/s-0032-1330123. [DOI] [PubMed] [Google Scholar]
- 22.Dahdaleh N S, Smith Z A, Hitchon P W. Percutaneous pedicle screw fixation for thoracolumbar fractures. Neurosurg Clin N Am. 2014;25(2):337–346. doi: 10.1016/j.nec.2013.12.011. [DOI] [PubMed] [Google Scholar]
- 23.Fang L M, Zhang Y J, Zhang J. et al. [Minimally invasive percutaneous pedicle screw fixation for the treatment of thoracolumbar fractures and posterior ligamentous complex injuries] Beijing Da Xue Xue Bao. 2012;44(6):851–854. [PubMed] [Google Scholar]
- 24.Fuentes S, Metellus P, Fondop J, Pech-Gourg G, Dufour H, Grisoli F. [Percutaneous pedicle screw fixation and kyphoplasty for management of thoracolumbar burst fractures] Neurochirurgie. 2007;53(4):272–276. doi: 10.1016/j.neuchi.2007.04.006. [DOI] [PubMed] [Google Scholar]
- 25.Giorgi H, Blondel B, Adetchessi T, Dufour H, Tropiano P, Fuentes S. Early percutaneous fixation of spinal thoracolumbar fractures in polytrauma patients. Orthop Traumatol Surg Res. 2014;100(5):449–454. doi: 10.1016/j.otsr.2014.03.026. [DOI] [PubMed] [Google Scholar]
- 26.Grass R, Biewener A, Dickopf A, Rammelt S, Heineck J, Zwipp H. [Percutaneous dorsal versus open instrumentation for fractures of the thoracolumbar border. A comparative, prospective study] Unfallchirurg. 2006;109(4):297–305. doi: 10.1007/s00113-005-1037-6. [DOI] [PubMed] [Google Scholar]
- 27.Gu Y, Zhang F, Jiang X, Jia L, McGuire R. Minimally invasive pedicle screw fixation combined with percutaneous vertebroplasty in the surgical treatment of thoracolumbar osteoporosis fracture. J Neurosurg Spine. 2013;18(6):634–640. doi: 10.3171/2013.3.SPINE12827. [DOI] [PubMed] [Google Scholar]
- 28.He D, Wu L, Sheng X. et al. Internal fixation with percutaneous kyphoplasty compared with simple percutaneous kyphoplasty for thoracolumbar burst fractures in elderly patients: a prospective randomized controlled trial. Eur Spine J. 2013;22(10):2256–2263. doi: 10.1007/s00586-013-2972-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.He Q Y, Xu J Z. Short segmental pedicle screw fixation combined with percutaneous vertebroplasty in treatment of nonadjacent thoracolumbar fractures. Chin J Traumatol. 2009;12(3):138–141. [PubMed] [Google Scholar]
- 30.Heintel T M, Berglehner A, Meffert R. Accuracy of percutaneous pedicle screws for thoracic and lumbar spine fractures: a prospective trial. Eur Spine J. 2013;22(3):495–502. doi: 10.1007/s00586-012-2476-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Huang Q S, Chi Y L, Wang X Y. et al. [Comparative percutaneous with open pedicle screw fixation in the treatment of thoracolumbar burst fractures without neurological deficit] Zhonghua Wai Ke Za Zhi. 2008;46(2):112–114. [PubMed] [Google Scholar]
- 32.Koreckij T, Park D K, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. [DOI] [PubMed] [Google Scholar]
- 33.Li C, Xu H Z, Wang X Y. et al. [Comparison of the paraspinal muscle change of percutaneous and open pedicle screw fixation in the treatment for thoracolumbar fractures] Zhonghua Wai Ke Za Zhi. 2007;45(14):972–975. [PubMed] [Google Scholar]
- 34.Li F, Zheng Z. [Advancement in the repair and reconstruction of the injured spine and spinal cord] Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2006;20(4):324–330. [PubMed] [Google Scholar]
- 35.Luo P, Xu L F, Ni W F. et al. [Therapeutic effects and complications of percutaneous pedicle screw fixation for thoracolumbar fractures] Zhonghua Wai Ke Za Zhi. 2011;49(2):130–134. doi: 10.3760/cma.j.issn.0529-5815.2011.02.007. [DOI] [PubMed] [Google Scholar]
- 36.Ma Y Q, Li X L, Dong J, Wang H R, Zhou X G, Li C. [Comparison of percutaneous versus open monosegment instrumentation in the treatment of incomplete thoracolumbar burst fracture] Zhonghua Yi Xue Za Zhi. 2012;92(13):904–908. [PubMed] [Google Scholar]
- 37.Mattei T A Hanovnikian J, H Dinh D. Progressive kyphotic deformity in comminuted burst fractures treated non-operatively: the Achilles tendon of the Thoracolumbar Injury Classification and Severity Score (TLICS) Eur Spine J 201423112255–2262. [DOI] [PubMed] [Google Scholar]
- 38.Ni W F, Huang Y X, Chi Y L. et al. Percutaneous pedicle screw fixation for neurologic intact thoracolumbar burst fractures. J Spinal Disord Tech. 2010;23(8):530–537. doi: 10.1097/BSD.0b013e3181c72d4c. [DOI] [PubMed] [Google Scholar]
- 39.Oner F C Verlaan J J Verbout A J Dhert W J Cement augmentation techniques in traumatic thoracolumbar spine fractures Spine (Phila Pa 1976) 200631(11, Suppl):S89–S95., discussion S104 [DOI] [PubMed] [Google Scholar]
- 40.Pelegri C, Benchikh El Fegoun A, Winter M. et al. [Percutaneous osteosynthesis of lumbar and thoracolumbar spine fractures without neurological deficit: surgical technique and preliminary results] Rev Chir Orthop Repar Appar Mot. 2008;94(5):456–463. doi: 10.1016/j.rco.2008.03.035. [DOI] [PubMed] [Google Scholar]
- 41.Rahamimov N, Mulla H, Shani A, Freiman S. Percutaneous augmented instrumentation of unstable thoracolumbar burst fractures. Eur Spine J. 2012;21(5):850–854. doi: 10.1007/s00586-011-2106-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Roy-Camille R. [Current trends in surgery of the spine] Int Orthop. 1989;13(2):81–87. doi: 10.1007/BF00266367. [DOI] [PubMed] [Google Scholar]
- 43.Shui X L, Xu H Z, Chi Y L. et al. [The application of minimally invasive surgery for different type of thoracolumbar fractures] Zhonghua Wai Ke Za Zhi. 2011;49(12):1086–1090. [PubMed] [Google Scholar]
- 44.Takami M, Yamada H, Nohda K, Yoshida M. A minimally invasive surgery combining temporary percutaneous pedicle screw fixation without fusion and vertebroplasty with transpedicular intracorporeal hydroxyapatite blocks grafting for fresh thoracolumbar burst fractures: prospective study. Eur J Orthop Surg Traumatol. 2014;24 01:S159–S165. doi: 10.1007/s00590-013-1266-2. [DOI] [PubMed] [Google Scholar]
- 45.Verheyden P, Katscher S, Schulz T, Schmidt F, Josten C. Open MR imaging in spine surgery: experimental investigations and first clinical experiences. Eur Spine J. 1999;8(5):346–353. doi: 10.1007/s005860050186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Wang H W, Li C Q, Zhou Y, Zhang Z F, Wang J, Chu T W. Percutaneous pedicle screw fixation through the pedicle of fractured vertebra in the treatment of type A thoracolumbar fractures using Sextant system: an analysis of 38 cases. Chin J Traumatol. 2010;13(3):137–145. [PubMed] [Google Scholar]
- 47.Wang J, Zhou Y, Zhang Z F, Li C Q, Zheng W J, Liu J. Radiological study on disc degeneration of thoracolumbar burst fractures treated by percutaneous pedicle screw fixation. Eur Spine J. 2013;22(3):489–494. doi: 10.1007/s00586-012-2462-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Wang M Y. Percutaneous thoracolumbar pedicle screw fixation: is it time to revisit spinal fracture treatment? World Neurosurg. 2010;74(6):570–571. doi: 10.1016/j.wneu.2010.04.019. [DOI] [PubMed] [Google Scholar]
- 49.Wang W, Yao N, Song X, Yan Y, Wang C. External spinal skeletal fixation combination with percutaneous injury vertebra bone grafting in the treatment of thoracolumbar fractures. Spine (Phila Pa 1976) 2011;36(9):E606–E611. doi: 10.1097/BRS.0b013e3181f92dac. [DOI] [PubMed] [Google Scholar]
- 50.Wimmer C. [Percutaneous fusion technique on the thoracolumbar spine with the Expedium LIS] Oper Orthop Traumatol. 2008;20(6):511–524. doi: 10.1007/s00064-008-1507-4. [DOI] [PubMed] [Google Scholar]
- 51.Xu Z, Xu W, Wang C, Luo H, Li G, Chen R. [Effectiveness of long segment fixation combined with vertebroplasty for severe osteoporotic thoracolumbar compressive fractures] Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013;27(11):1331–1337. [PubMed] [Google Scholar]
- 52.Yang W E, Ng Z X, Koh K M. et al. Percutaneous pedicle screw fixation for thoracolumbar burst fracture: a Singapore experience. Singapore Med J. 2012;53(9):577–581. [PubMed] [Google Scholar]
- 53.Zairi F, Aboukais R, Marinho P, Allaoui M, Assaker R. Minimally invasive percutaneous stabilization plus balloon kyphoplasty for the treatment of type A thoracolumbar spine fractures: minimum 4 year's follow-up. J Neurosurg Sci. 2014;58(3):169–175. [PubMed] [Google Scholar]
- 54.Zhang Z C, Sun T S, Liu Z, Guo Y Z, Li L H. [Minimally invasive percutaneous cannulated pedicle screw system fixation for the treatment of thoracolumbar flexion-distraction fracture without neurologic impairment] Zhongguo Gu Shang. 2011;24(10):802–805. [PubMed] [Google Scholar]
- 55.Kim D Y, Lee S H, Chung S K, Lee H Y. Comparison of multifidus muscle atrophy and trunk extension muscle strength: percutaneous versus open pedicle screw fixation. Spine (Phila Pa 1976) 2005;30(1):123–129. [PubMed] [Google Scholar]
- 56.Smith Z A, Sugimoto K, Lawton C D, Fessler R G. Incidence of lumbar spine pedicle breach following percutaneous screw fixation: a radiographic evaluation of 601 screws in 151 patients. J Spinal Disord Tech. 2014;27(7):358–363. doi: 10.1097/BSD.0b013e31826226cb. [DOI] [PubMed] [Google Scholar]
- 57.Park Y, Ha J W, Lee Y T, Sung N Y. Cranial facet joint violations by percutaneously placed pedicle screws adjacent to a minimally invasive lumbar spinal fusion. Spine J. 2011;11(4):295–302. doi: 10.1016/j.spinee.2011.02.007. [DOI] [PubMed] [Google Scholar]
- 58.Patel R D, Graziano G P, Vanderhave K L, Patel A A, Gerling M C. Facet violation with the placement of percutaneous pedicle screws. Spine (Phila Pa 1976) 2011;36(26):E1749–E1752. doi: 10.1097/BRS.0b013e318221a800. [DOI] [PubMed] [Google Scholar]
- 59.Knox J B, Dai J M III, Orchowski J R. Superior segment facet joint violation and cortical violation after minimally invasive pedicle screw placement. Spine J. 2011;11(3):213–217. doi: 10.1016/j.spinee.2011.01.024. [DOI] [PubMed] [Google Scholar]