

Abstract
Resorbable plate systems combine the benefits of rigid internal fixation with the convenience of biodegradation; thus, precluding the need for removal and reducing their interference with craniofacial growth. However, in surgeries involving maxillofacial bone, when reduction or repositioning of the bone segment is inaccurate, refixation and rebending of the plate may be necessary. Here, we report using a temporary plate with self-tapping metal screws to avoid repeated rebending of the resorbable plate and using additional screws following inaccurate fixation in maxillofacial surgeries.
Keywords: Resorbable plate system, self-tapping metal screw, template, temporary fixation
INTRODUCTION
Resorbable plate systems have gained acceptance for managing patients requiring maxillofacial surgery as they have rigid internal fixation with the convenience of biodegradation, precluding the need for their removal and reducing their interference with craniomaxillofacial growth in children.[1,2] Therefore, these materials are safe, effective, and sufficiently flexible for use in many maxillofacial sites.[3,4] However, refixation and rebending of the resorbable plate may be necessary when reduction or repositioning of bone segments is inaccurate. Here, we report the feasible use of a temporary aluminum template with self-tapping metal screws (resorbable plate system) in maxillofacial surgery to avoid repeated rebending of resorbable plates and the use of additional screws following inaccurate fixation.
TECHNIQUE
We used a resorbable plate system made of a substantially amorphous linear copolymer consisting of 82% poly-L-lactic acid and 18% polyglycolic acid (LactoSorb; Lorenz Surgical, Jacksonville, FL, USA) in maxillofacial bone surgeries, such as orthognathic surgery and maxillofacial fracture treatment. Basically, according to commercial instructions, the shape of the resorbable plate is to be adjusted to match a contoured template [Figure 1] by bending or twisting it with the help of a water bath system used for heating. Thereafter, a drill bit is used to create a guide hole and a screw hole is carefully tapped. Finally, a screw is inserted using a torque driver to fasten the plate to the bone.
Figure 1.
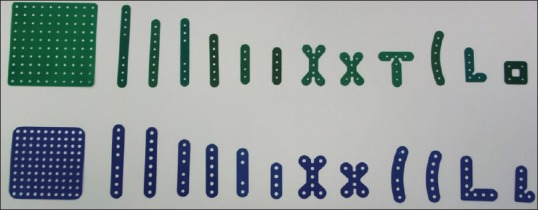
Aluminum template for forming the contour by bending or twisting
However, a problem could occur sometimes, if refixation and rebending of the resorbable plate might be necessary, such as in a clinical situation where the reduction or repositioning of bone segments is inaccurate or reconsidered. Because the resorbable plate system becomes a material which is characteristically unstable by four or more bending procedures, it cannot be bent several times (Biomet, Patient Risk Information - 01-50-1050, LactoSorb Trauma instruction manual; http://www.biomet.com/wps/wcm/connect/internet/1d851fd2-f51b-408a-b065-556e6cdc9afc/01-50-1050.pdf?MOD=AJPERES&CONVERT_TO=url&CACHEID=1d851fd2-f51b-408a-b065-556e6cdc9afc. Furthermore, the use of resorbable plate and screw system for bone fixation is much more expensive by about 10 more times than that of a titanium miniplate fixation and rather technically difficult for refixation.[5]
Thus, we modified the technique, wherein bone segments were first fixed using an aluminum template. Then, stainless steel self-tapping screws (1.5 or 2.0 mm in diameter) with the same thread form as that of resorbable screws were used for the temporary fixation of the template plate. Rebending or readjustment of the template was easily performed if reduction or repositioning of bone segments was inaccurate, and the stainless steel self-tapping screws were also used for refixation.
In Le Fort I osteotomy for orthognathic surgery, precise skeletal analysis of movements was performed, and the repositioned maxillary model in the articulator was thoroughly discussed and confirmed with orthodontists in charge. However, the position of the maxillary segment may be adjusted during surgery based on the volume of soft tissues and/or localization of hard tissue identified in the perioperative X-rays. The technique used in this study has been described in the following section. The aluminum template was first tightly adapted to the bone at the appropriate position in the maxilla. Thereafter, temporary self-tapping metal screws were inserted into the template plate hole for temporary fixation of the nasomaxillary and/or zygomaticomaxillary buttress and drilling of the bone [Figure 2]. If no problems were identified during evaluation of facial soft tissues by intraoperative radiographs, the maxillary segment was secured to the rest of the nasomaxillary and zygomaticomaxillary buttresses using plates. If the maxillary repositioning was inaccurate, repositioning and temporary fixation were performed again without the additional use of the new resorbable plate and screws. Finally, after removal of the template and bending of the same shape resorbable plates accurately [Figure 3], actual resorbable screws were inserted into the holes formed by the self-tapping metal screws.
Figure 2.
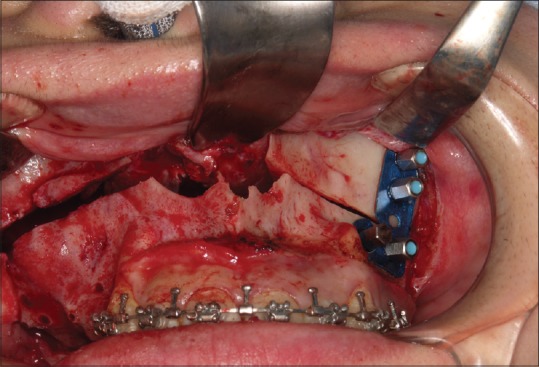
Temporary fixation using template and self-tapping metal screws. The template is easy to bend, flexible, and can be used repeatedly. It is possible to correct bending and facilitate precise positioning of bone fragments using a template meant for temporary fixing
Figure 3.

Resorbable plates that accurately reproduce the plate form determined by the template
The aluminum template used here is very easy to bend, flexible, and can be repeatedly used without extending the operating time. Inaccurate bending can be easily corrected and precise positioning of bone fragments can be facilitated using a template meant for temporary fixing. In case of inaccurate reduction or repositioning of bone segments, template and screws can either be reused or replaced without any new resorbable plate and screws for additional costs and time. In case of inaccurate fixation, temporary screws with the tapping function can be used to avoid the use of additional screws. Moreover, using temporary screw holes to insert the screw without tapping can shorten the operation time.
CONCLUSION
In this indication, it could be effective for three-dimensional complex jaw deformity treatment with the possibility of refixation and repositioning in the Le Fort I osteotomy. In addition, it can also be used when bone fixation is difficult in complex facial multiple fractures and is considered to be useful for surgical procedures using resorbable plate systems.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Eppley BL, Sadove AM. Effects of resorbable fixation on craniofacial skeletal growth: A pilot experimental study. J Craniofac Surg. 1992;3:190–6. doi: 10.1097/00001665-199212000-00003. [DOI] [PubMed] [Google Scholar]
- 2.Enislidis G, Pichorner S, Lambert F, Wagner A, Kainberger F, Kautzky M, et al. Fixation of zygomatic fractures with a new biodegradable copolymer osteosynthesis system. Preliminary results. Int J Oral Maxillofac Surg. 1998;27:352–5. doi: 10.1016/s0901-5027(98)80063-5. [DOI] [PubMed] [Google Scholar]
- 3.Sukegawa S, Kannno T, Kawai H, Shibata A, Takahashi Y, Nagatsuka H, et al. Long-term bioresorption of bone fixation devices made from composites of unsintered hydroxyapatite particles and poly-L-lactide. J Hard Tissue Biol. 2015;24:219–24. [Google Scholar]
- 4.Eppley BL. Resorbable biotechnology for craniomaxillofacial surgery. J Craniofac Surg. 1997;8:85–6. [PubMed] [Google Scholar]
- 5.Iwai T, Omura S, Aoki N, Tohnai I. Use of self-tapping metal screws for temporary fixation of a resorbable plate system in maxillofacial surgery. J Craniofac Surg. 2015;26:891–2. doi: 10.1097/SCS.0000000000001415. [DOI] [PubMed] [Google Scholar]