

Abstract
Study Objectives:
While neck circumference (NC) is a useful predictor of obstructive sleep apnea (OSA) in adults, childhood OSA is difficult to predict clinically. We utilized the neck circumference-height ratio (NHR) to normalize NC in growing children. Our study aimed to determine if (1) NC is a reproducible clinical measurement; (2) NHR predicts OSA in children; (3) this metric translates to adults.
Methods:
For this retrospective study, paired NC measurements (from clinic and sleep laboratory) in 100 consecutive adult subjects were used to confirm inter-observer reproducibility. Polysomnographic (PSG) and anthropometric data from children aged 5–18 years presenting consecutively between July 2007 and February 2012 was obtained. Children with genetic syndromes, severe neurological disorders, craniofacial abnormalities, tracheostomy, past adenotonsillectomy, in-hospital PSG or sleep efficiency < 80% were excluded. Data were analyzed using χ2 test and logistic and linear regression models. These analyses were also applied to 99 adult patients with similar exclusion criteria.
Results:
Adult NC measurement had inter-observer correlation of 0.85 (N = 100). Among children, after correcting for BMI-Z scores, NHR conferred additional predictive value, in both logistic regression and linear models, for both apnea-hypopnea index (AHI) > 2 and > 5 (N = 507). In children, for NHR > 0.25, the odds ratio of AHI > 2 was 3.47. In adults, for NHR > 0.25, the odds ratio of AHI > 5 was 18.
Conclusions:
NHR can be included as a simple screening tool for OSA in children and adults, which along with other predictors, may improve the ability of clinicians to triage children and adults at risk for OSA for further evaluation with PSG.
Citation:
Ho AW, Moul DE, Krishna J. Neck circumference-height ratio as a predictor of sleep related breathing disorder in children and adults. J Clin Sleep Med 2016;12(3):311–317.
Keywords: obstructive sleep apnea, neck circumference, children
INTRODUCTION
Childhood obstructive sleep apnea (OSA) is a common condition occurring in approximately 2% of children.1 Whereas it has been classically reported in the adult OSA literature, obesity is increasingly noted to be comorbid with pediatric OSA as well. Relative contributions of central obesity to metabolic syndrome and other inflammatory markers are well known.2 While the polysomnogram (PSG) is the gold-standard for the diagnosis of OSA, the STOP-BANG questionnaire is now a popular tool for assessing OSA risk in adults.3 This screening tool includes measures for BMI and neck circumference. Yet, there is significant lack of data for the relative contribution of neck size to pediatric OSA.
Currently, the American Academy of Pediatrics (AAP) guides practitioners to consider PSG in snoring children who are clinically determined to be at risk for OSA.4 Given the significant cost of PSG and the relative paucity of pediatric sleep centers in the United States, methods for screening of children for OSA have been suggested.5 There remains, however, a need for better predictors of OSA to improve utilization of available resources.
While it has been demonstrated that clinical evaluation of pediatric patients is a relatively poor predictor of OSA,6 the suggested physical examination nevertheless routinely includes general observations such as obesity and BMI. The nasopharyngeal examination is critical, and attention to tonsil-lar size, nasal anatomy, tongue position, and dentition is emphasized.4 It has been suggested that soft-tissue changes, and potentially fat deposition in the upper airway may play a significant role in the observed differences in tonsillar and adenoidal size, and increased Mallampati scores between obese and nonobese children with OSA.7 Yet, neck circumference measurement is often described only in the context of adult patients. The Sleep Heart Health Study has in fact shown neck circumference to be the strongest predictor of OSA in adults when compared to other clinical parameters, such as snoring, gender, age, and BMI.8 Other studies have similarly shown that neck circumference is an independent risk factor for OSA in adults.9
BRIEF SUMMARY
Current Knowledge/Study Rationale: Clinical prediction of obstructive sleep apnea in children is difficult. Due to limited availability of overnight polysomnography, parameters have been suggested to help select candidates. In adults, neck circumference is a strong predictor, but normative data in children is limited.
Study Impact: Neck circumference-height ratio (NHR) can be a useful additional aid along with other predictors to predict obstructive sleep apnea in children. NHR > 0.25 places the odds ratio of apneahypopnea index > 2 at 3.47. This provides an inexpensive clinical tool to assist in triaging snoring children for confirmatory polysomnogram.
Visceral adiposity has been studied in children10,11 and waist circumference centiles for children are now available based upon methods described by the National Center for Health Statistics.12,13 However, the issue of measuring neck sizes in children is a priori complicated by the fact that no single neck size can be used as a cutoff in growing children. While normative Turkish data is available,14 the authors are not aware of age-related norms describing pediatric neck circumference in the United States.
One way to approach the distribution of fat in the human body is to analyze its relative distribution. If one imagines the neck as more or less a cylinder, then the “thickness” or circumference of the neck will be mathematically proportional to its length for any given neck mass. Further, since neck length is difficult to accurately and reproducibly measure, under an assumption of proportionality of the normal human body, neck length should be proportional to overall height, even under circumstances of obesity. Given these assumptions and the lack of normative data for neck circumference among children, we sought to study the relationship of the neck circumference-height ratio (NHR) and PSG variables (specifically, apnea-hypopnea index [AHI]) in children. An assumption of proportionality in growth as the child ages while not ideal, appears tantalizingly simple. In fact, the waist-height ratio has been used as a surrogate for visceral adiposity in obesity research.15 Further, the NHR has been used in adults to predict severity of OSA.9,16,17
Our study aimed to answer three questions:
Is neck circumference an easily reproducible measurement in routine clinical practice?
In children, does the relative neck size (measured as NHR) add risk or severity information, after adjusting for BMI?
Does the NHR metric in adults corroborate results of previous studies?
METHODS
This was a retrospective study utilizing the Cleveland Clinic Sleep Disorders Center (CCSDC) accredited sleep laboratory database and electronic medical records with institutional IRB approval. Scoring of the sleep study was performed according to the 2007 AASM guidelines,18 which was current for that time period. The AHI and other variables were derived from the clinical PSG report and archived for later potential retrieval within the CCSDC database.
Neck Circumference Reproducibility
For the initial part of the study, we compared measurements obtained in two different clinical scenarios on the same patient in order to determine if neck circumference was a reproducible measurement in routine clinical practice. Adult patients were used, rather than children, as the neck circumference was presumed to be more stable across time. We obtained a retrospective sample of 100 consecutive adult patients who had PSGs performed in the CCSDC starting January 1, 2013, who had also been assessed within the previous 1 year 9 months by a CCSDC staff physician with a neck circumference included in the clinical encounter. By CCSDC PSG protocol, height (cm) is measured without shoes, weight (kg) in street clothes without outerwear, and neck circumference (cm) was measured in the sleep laboratory by the technologist at the point just above the cricoid cartilage to the nearest 0.5 cm. Physicians had not necessarily been specifically instructed regarding the neck circumference measurement in clinic but were aware of the CCSDC laboratory protocol. The correlation between the 2 measurements was then calculated. For this and other analyses, the statistical package R, version 2.15.2 (2012-10-26), was utilized.
Childhood NHR and OSA Severity
In the next part of the study, we retrospectively queried the CCSDC database for PSGs in children. This comprised children referred by a clinician based on a suspicion of potential OSA (i.e., snoring). For the purposes of our study, we included only children between the ages of 5 and 18 years. This was due to the presumption that the neck circumference measurements as well as PSG data may be less reliable at younger ages. We included subjects who had anthropometric measurements, including height, weight, and neck circumference documented. Excluded were those with PSG showing < 80% sleep efficiency, in-hospital PSG, follow-up PSG (e.g., following tonsil-lectomy and adenoidectomy). We also excluded children who had genetic syndromes (e.g., Down syndrome, Prader-Willi syndrome), children with severe neurological disorders (e.g., neuromuscular disorders, cerebral palsy) and children who had a tracheostomy or craniofacial malformations, as these comorbid conditions could be considered potential confounders, when assessing the correlation of neck circumference to risk of OSA. A total of 1,939 charts were serially screened in chronological order starting in July 2007 to February 2012. Of these, 507 children satisfied the above inclusion and exclusion criteria and were included in the final analysis (Figure 1).
Figure 1. Inclusion and exclusion criteria applied to total number of pediatric polysomnograms.

The NHR (cm/cm) as well as the BMI-Z score was calculated for each patient. PSG data including AHI and oxygen saturation nadir, were extracted from our database. Using a cutoff AHI of 2, a baseline logistic regression model was used to ascertain if BMI-Z scores were predictive of OSA. The NHR was added to this baseline model. The interaction between BMI-Z score and AHI was also assessed in a later model. The same models were then applied using an AHI cutoff of 5. Similarly, linear models were then used to examine whether BMI-Z score and NHR was predictive of AHI. The odds ratio and both positive and negative predictive values of having AHI > 2, if NHR > 0.25 were calculated based on the χ2 table of our 507 pediatric subjects.
Adult NHR and OSA Severity
In the final part of the study, to assess if similar methodology and NHR cutoffs could be used in adults, data from PSGs of adult patients were screened starting January 1, 2013, to ascertain fulfillment of inclusion and exclusion criteria, until 99 subjects were recruited. The analytical methods used were as described for the children, with the exception of using the Fisher exact test to calculate the odds ratio.
RESULTS
Bivariate Comparisons
Neck Circumference Reproducibility
In the adult sample of 100 subjects, the inter-rater correlation of neck circumference measurements was 0.85, with the Bland-Altman plot (Figure 2) indicating overall measurement reliability across neck sizes.
Figure 2. Bland-Altman plot: adult neck circumference.

Bland-Altman plot of neck circumference (cm) in 100 adult patients measured in sleep clinic vs. sleep laboratory.
Childhood NHR and OSA Severity
For the children, Figure 1 demonstrates the number of studies included and excluded in the final analysis based on the criteria stated in the Methods section. For the remaining children, Table 1 details demographics, mean neck circumferences, and BMI-Z scores. The majority of NHR fell between 0.2 and 0.25. NHR, when box-plotted by age (Figure 3) or scatter-plotted against height (Figure 4), appeared both age- and height-invariant, respectively. When box-plotted by AHI < 2 or > 2 (see Figure 5), more children with OSA had NHR exceeding 0.25. In the 4-way table of NHR (< versus > 0.25) and OSA (< versus > 2) (Table 2), the odds ratio of 3.47 (i.e., 39/12) was noted among those with NHR > 0.25. The positive predictive value for a child with a NHR > 0.25 having OSA was 76%; the negative predictive value of a NHR < 0.25 was 52%.
Table 1.
Pediatric patient characteristics.

Figure 3. Agegroup box plots of neck-to-height ratios.

Box plot of neck circumference-height ratio (cm-cm) vs. age in pediatric patients ages 5 to 18 years old.
Figure 4. Neck-height ratio versus height.
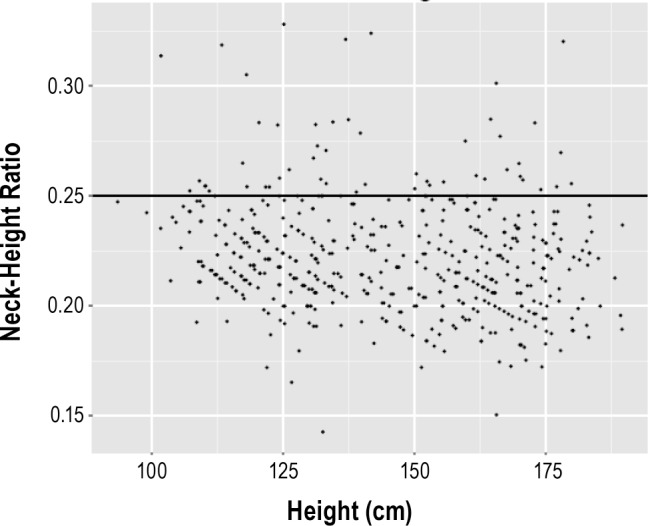
Scatter plot of neck circumference-height ratio (cm-cm) vs. height (cm) in pediatric patients ages 5 to 18 years old.
Figure 5. Neck-height ratio versus AHI diagnoses.
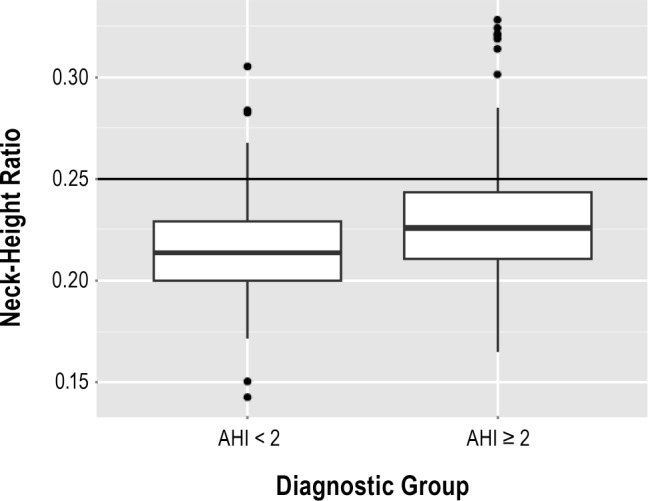
Box plot of neck circumference-height ratio (cm-cm) vs. apnea-hypopnea index (AHI) in pediatric patients ages 5 to 18 years old.
Table 2.
AHI vs NHR in children 5 to 18 years old.

Adult NHR and OSA Severity
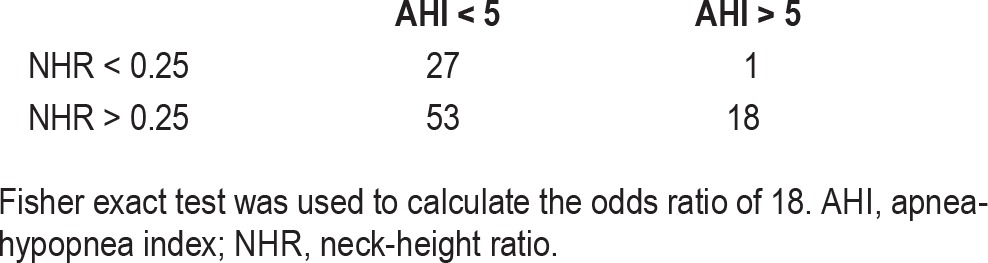
In a parallel analysis in adults (Table 3), again using the NHR cutoff of 0.25, but now using an AHI cutoff of 5, Fisher exact test showed that the NHR effect was significant (p = 0.012), with odds ratio estimated as 18 of having OSA among adults with a NHR > 0.25. Although the odds ratio in adults compared to the children was much higher (18 vs 3.47), the positive predictive value was only 25%, but conversely had a very high negative predictive value at 96%.
Table 3.
AHI vs NHR in adults.
Modeling Studies
Childhood NHR and OSA Severity
In the pediatric sample, when using a baseline logistic regression model in which yes/no response was, if AHI was > 2, the NHR parameter predicted (0.067 [0.016], z = 4.11 df = 506, p < 0.001) the presence/absence of OSA. When augmenting this baseline model, the addition of the BMI-Z score parameter provided an overall model improvement (deviance = 9.56, df = 1, p = 0.002), with the NHR parameter becoming not statistically significant (p = 0.13). However further model augmentation with a BMI-Z:NHR interaction term was significant (17.9, 1, p < 0.001), with now the reversed main effects of neck size (−0.06537 [0.031], −2.1, p = 0.03) and BMI-Z score (−1.58 [0.46], −3.43, p < 0.001) counteracting a strong NHR:BMI-Z score positive interaction (0.062 [0.015], 4.04, p < 0.001). In the model series using an AHI of 5 as cutoff, both main effects were maintained, but with the main effect of NHR becoming nonsignificant in the interaction model. In the linear regression modeling strategy (i.e., modeling AHI as continuous), the NHR parameter was statistically significant in the baseline model (0.38 [0.085], t = 4.5, df = 505, p < 0.001). The addition of the BMI-Z score improved the overall model fit (F = 4.39, p = 0.02), with NHR (0.24 [0.1], t = 2.29, p = 0.2) and BMI-Z (1.02 [0.45], t = 2.26, p = 0.02) parameter estimates remaining significant. The model then adding the BMI-Z:NHR interaction term was also significant (F = 20.8, p < 0.001), with NHR (−0.29 [0.15], t = 1.87, p = 0.06) effect changing direction at trend-level significance, and with BMI-Z scored also reversing effect direction (−8.26 [2.08], t = −3.96, p < 0.001), to counteract a more significant positive NHR:BMI-Z interaction term (0.21 [0.07], t = 4.8, p < 0.001). This again highlighted the synergistic, con-joint effect of NHR and BMI-Z score that were the strongest predictor of having higher AHI values in the pediatric sample. Using an AHI cutoff of 5 yielded similar results.
Adult NHR and OSA Severity
In the adult sample of 99 subjects, the model series were investigated with BMI in baseline models, owing to BMI being more firmly established as a predictor of OSA in adults. Using an AHI cutoff of 5, the baseline logistic model was significant overall, and its BMI parameter estimate was also significant (0.14 [0.048], z = 2.8, p = 0.005). In the augmented significant (Dev = 15.96, p < 0.001) model, the BMI parameter term became nonsignificant, with the NHR becoming highly significant (67.6 [19.5], z = 3.46, p < 0.001). The subsequent interaction model was non-significant. Similar results were obtained for an AHI cutoff of 15. In the linear model series, the baseline model found the BMI parameter to be significant (0.017 [0.0055], t = 3.09, p = 0.003). Adding the NHR term in the augmented model improved overall model fit (F = 17.2, p < 0.001) with a significant NHR parameter term (9.58 [2.36], t = 4.06, p < 0.001), but with BMI parameter nonsignificant, serving instead as a mere term to control for possible confounding. With the addition of a further BMI: NHR interaction term, the augmented model was found to be significant (F = 5.2, p = 0.02). In this interaction model, the main effect of NHR (23.7 [6.6], t = −3.58, p < 0.001) appeared to be larger than for BMI itself (0.11 [0.05], t = 2.24, p = 0.03), but with the NHR:BMI interaction term now suggesting its possible mild protective effect (−0.45 [0.196], t = 2.28, p = 0.02) in adults.
Overall, in these several model series, NHR played a key predictive role in diagnostic outcome prediction, despite corrections for BMI score, in both children and adults.
DISCUSSION
The AAP suggests screening for OSA in all children. This begins with screening for snoring. Certain other clinical findings increase the suspicion and merit consideration of confirmatory testing by PSG4. These include, among others, the presence of excessive daytime sleepiness, headaches on awakening, labored breathing during sleep, witnessed apneas during sleep, tonsillar hypertrophy, retrognathia or micrognathia, high arched palate, and failure to thrive, or conversely, an elevated BMI. In this study we present the additional utility of NHR in this regard. Within our approach we imagine the neck as a cylinder, with “thickness” of the cylinder expressed as a ratio of circumference over length. It is difficult to accurately measure the length of the neck, but one can assume that it is proportional to the height of the body in most cases, barring genetic syndromes and skeletal or neuromuscular disorders. Thus, body height can be used as a surrogate for neck length. Accordingly, in this study, children with genetic syndromes and significant neuromuscular disorders were excluded. Thus, a NHR of 0.25 and higher as a predictor for OSA may not be applicable outside the studied population. Furthermore, other anatomical factors (e.g., thyromegaly or other neck mass) need to be considered in formulating a clinical judgment.
While some of the weaknesses of our study lie in its retrospective design and clinically measured anthropometrics in a busy office setting, we submit it mimics a scenario where we believe this measure will find greatest application. Furthermore, our large sample size should minimize any bias this approach may introduce. We have demonstrated that neck circumference is a reproducible measurement between different providers in clinical practice. This simple metric, in conjunction with the height may be converted to the NHR, and in this manner can be a useful aid to predict the presence of OSA.
Our study identified NHR of 0.25 and higher as a predictor of OSA, and it appears that this ratio may be universally applicable across the age spectrum. This approach circumvents the need for normative data on neck circumferences in children, which to the best of our knowledge is currently unavailable for the U.S. population and has only been published for a population sample of normal Turkish children.11 A comparison of the neck circumference means shown in our study (Table 1), and those in the Turkish study, demonstrates a consistently larger neck circumference by approximately 0.5 to 3 cm, with greater differences at the older end of the age spectrum. Although we recognize this is not a completely equitable comparison, given that our study consists of a referred population of children, until such U.S. data are available, it may suggest that using norms from other countries may not be applicable. Even with the development of normative data for a U.S. population, using a NHR approach also has the advantage that it corrects for children of different heights at the same age. For instance, a “normal” neck circumference in a 7-year old whose height is at the 95th centile, may in fact be a large neck for the same aged child whose height is at the 5th centile.
In the linear and logistic regression models we corrected for BMI, as neck circumference and BMI are plausibly correlated. However, the same premise does not apply to adenotonsillar hypertrophy, and there is potential that adding a tonsillar size grading parameter and Mallampati score could be a route to further refine the predictive value of the neck circumference model in the pediatric population, creating a composite score from multiple variables, similar to the STOP-BANG in adults. Further analysis in this regard is warranted. The odds ratio for predicting OSA with NHR > 0.25 is higher in adults than in children (18 vs. 3.47), and a reasonable postulate for this would be that adenotonsillar hypertrophy is a relative non-factor in adults, as opposed to children where it may at times override the obesity and NHR factors. This would suggest that in the absence of significant adenotonsillar hypertrophy, neck circumference and NHR are indeed strongly predictive of OSA.
Our study demonstrates that NHR is a better predictive tool in adults than in children, corroborating the long-standing use of absolute neck circumference measurements in adults in the clinical evaluation of potential OSA. Thus, although NHR > 0.25 is helpful in predicting those children who are at higher risk of OSA, there are still a significant number of children with NHR < 0.25, as shown by the low negative predictive value of 52%, who by standard definition also have OSA. Thus, use of NHR should not trump clinical index of suspicion, and polysomnography remains the gold standard in assessing children for OSA. However, in a setting of limited resources for pediatric polysomnography, we have shown that NHR can be a useful and clinically amenable tool, in addition to our standard armamentarium, to further refine the probability of OSA.
Given the global epidemic of childhood obesity, public health screening for obesity and its related complications take on an even greater relevance. While it has already been suggested that neck circumference could be a simple screening tool for high BMI19 and cardiovascular risk in children,20 our study underscores potential utility of this easily obtainable metric to assist in OSA screening in broader population groups. In such situations, screening for snoring and an elevated NHR may provide justification for focused referral for further testing for OSA. To determine if the results of our study can be applied in such a manner, further study in the relation of NHR as a predictor of OSA could be conducted in a population-based sample of children.
CONCLUSION
In this study we report NHR of 0.25 or greater is a helpful predictor for OSA in children, and is even more so in adults. Both neck circumference and height measurements may be easily obtained in the clinical setting. Thus, NHR is an additional easily performed screening tool that can be used, along with other predictors, in busy clinical practices to aid in determining which children and adults should be referred for further PSG evaluation.
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest. Research was conducted at the Cleveland Clinic Sleep Disorders Center, Cleveland, OH. Author contributions: Dr. Ho performed collection of data, co-drafted the initial manuscript, and approved the final manuscript as submitted; Dr. Moul suggested use of neck-height ratio to normalize data across the age spectrum studied, performed the statistical analyses, reviewed and revised the manuscript, and approved the final manuscript as submitted. Dr. Krishna served as senior author and mentor for Dr. Ho, conceptualized the project, co-drafted the initial manuscript, reviewed and revised the manuscript, and approved the final manuscript as submitted.
ACKNOWLEDGMENTS
The authors acknowledge Alan Kominsky, MD, for suggesting the analysis of the NHR in adults, and Nengah Hariadi, BSECE, MBA, for extracting and supplying the raw polysomnographic data from the CCSDC database.
ABBREVIATIONS
- AHI
apnea-hypopnea index
- BMI
body mass index
- NHR
neck circumference-height ratio
- OSA
obstructive sleep apnea
- PSG
polysomnogram
REFERENCES
- 1.Redline S, Tishler PV, Schluchter M, Aylor J, Clark K, Graham G. Risk factors for sleep-disordered breathing in children: associations with obesity, race and respiratory problems. Am J Respir Crit Care Med. 1999;159:1527–32. doi: 10.1164/ajrccm.159.5.9809079. [DOI] [PubMed] [Google Scholar]
- 2.Okosun IS, Liao Y, Rotimi CN, Prewitt TE, Cooper RS. Abdominal adiposity and clustering of multiple metabolic syndrome in White, Black and Hispanic Americans. Ann Epidemiol. 2000;10:263–70. doi: 10.1016/s1047-2797(00)00045-4. [DOI] [PubMed] [Google Scholar]
- 3.Chung F, Yegneswaran B, Liao P, et al. A Tool to Screen Patients for Obstructive Sleep Apnea. Anesthesiology. 2008;108:812–21. doi: 10.1097/ALN.0b013e31816d83e4. [DOI] [PubMed] [Google Scholar]
- 4.Marcus CL, Brooks LJ, Draper KA, et al. American Academy of Pediatrics. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130:576–84. doi: 10.1542/peds.2012-1671. [DOI] [PubMed] [Google Scholar]
- 5.Kaditis A, Kheirandish-Gozal L, Gozal D. Algorithm for the diagnosis and treatment of pediatric OSA: a proposal of two pediatric sleep centers. Sleep Med. 2012;13:217–27. doi: 10.1016/j.sleep.2011.09.009. [DOI] [PubMed] [Google Scholar]
- 6.Marcus CL, Brooks LJ, Draper KA, et al. American Academy of Pediatrics. Technical report: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130:e714–55. doi: 10.1542/peds.2012-1672. [DOI] [PubMed] [Google Scholar]
- 7.Dayyat E, Kheirandish-Gozal L, Sans Capdevila O, Maarafeya MM, Gozal D. Obstructive sleep apnea in children: relative contributions of body mass index and adenotonsillar hypertrophy. Chest. 2009;136:137–44. doi: 10.1378/chest.08-2568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Caffo B, Diener-West M, Punjabi NM, Samet J. A novel approach to prediction of mild obstructive sleep disordered breathing in a population-based sample: the Sleep Heart Health Study. Sleep. 2010;33:1641–8. doi: 10.1093/sleep/33.12.1641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ahbab S, Ataoğlu HE, Tuna M, et al. Neck circumference, metabolic syndrome and obstructive sleep apnea syndrome; evaluation of possible linkage. Med Sci Monit. 2013;19:111–7. doi: 10.12659/MSM.883776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Owens S, Gutin B, Ferguson M, Allison J, Karp W, Le NA. Visceral adipose tissue and cardiovascular risk factors in obese children. J Pediatr. 1998;133:41–5. doi: 10.1016/s0022-3476(98)70175-1. [DOI] [PubMed] [Google Scholar]
- 11.Goran MI, Gower BA. Relation between visceral fat and disease risk in children and adolescents. Am J Clin Nutr. 1999;70:149S–56S. doi: 10.1093/ajcn/70.1.149s. [DOI] [PubMed] [Google Scholar]
- 12.Fernandez JR, Redden DT, Pietrobelli A, Allison DB. Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J Pediatr. 2004;145:439–44. doi: 10.1016/j.jpeds.2004.06.044. [DOI] [PubMed] [Google Scholar]
- 13.National Health and Nutrition Examination Survey. Anthropometry Procedures Manual. Available online at: http://www.cdc.gov/nchs/data/nhanes/nhanes_07_08/manual_an.pdf.
- 14.Mazicioglu MM, Kurtoglu S, Ozturk A, Hatipoglu N, Cicek B, Ustunbas HB. Percentiles and mean values for neck circumference in Turkish children aged 6-18 years. Acta Paediatr. 2010;99:1847–53. doi: 10.1111/j.1651-2227.2010.01949.x. [DOI] [PubMed] [Google Scholar]
- 15.Savva SC, Tornaritis M, Savva ME, et al. Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. Int J Obes Relat Metabol Disord. 2000;24:1453–8. doi: 10.1038/sj.ijo.0801401. [DOI] [PubMed] [Google Scholar]
- 16.Kawaguchi Y, Fukumoto S, Inaba M, et al. Different impacts of neck circumference and visceral obesity on the severity of obstructive sleep apnea syndrome. Obesity (Silver Spring) 2011;19:276–82. doi: 10.1038/oby.2010.170. [DOI] [PubMed] [Google Scholar]
- 17.Simpson L, Mukherjee S, Cooper MN, et al. Sex differences in the association of regional fat distribution with the severity of obstructive sleep apnea. Sleep. 2010;33:467–74. doi: 10.1093/sleep/33.4.467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Iber C, Ancoli-Israel S, Chesson AL, Jr., Quan SF for the American Academy of Sleep Medicine. 1st ed. Westchester, IL: American Academy of Sleep Medicine; 2007. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. [Google Scholar]
- 19.Nafiu OO, Burke C, Lee J, Voepel-Lewis T, Malviya S, Tremper KK. Neck circumference as a screening measure for identifying children with high body mass index. Pediatrics. 2010;126:e306–10. doi: 10.1542/peds.2010-0242. [DOI] [PubMed] [Google Scholar]
- 20.Androutsos O, Grammatikaki E, Moschonis G, et al. Neck circumference: a useful screening tool of cardiovascular risk in children. Pediatr Obes. 2012;7:187–95. doi: 10.1111/j.2047-6310.2012.00052.x. [DOI] [PubMed] [Google Scholar]