

Abstract
The incidence of duplication of the vermiform appendix is reported as 0.004 %. Most anomalies of the appendix have been observed in adults and were noticed incidentally during surgery not primarily involving the appendix. Picoli in 1892 reported the first case of appendiceal duplication. Malformations of the appendix may be associated with other visceral anomalies. Several theories have been put forth to explain the developmental anomaly. Duplication of the appendix should be considered in the differential diagnosis of lower abdominal pain, even if the patient reports a previous appendicectomy. Surgeons should be aware of the potential anatomical variations of the vermiform appendix, and careful inspection of the caecum should be performed during laparotomy. Misdiagnosis can cause serious life-threatening complications for the patient and lead to medicolegal problems. This is a case report of a 24-year appendiceal duplication revealed on old female with appendicitis who had laparotomy.
Keywords: Appendiceal duplication, Inflammation, Anomaly, Medicolegal
Introduction
The incidence of duplication of the vermiform appendix is reported as 0.004 % [1]. Appendicular anomalies have been noticed incidentally in adults undergoing surgery for some other pathology not involving the appendix primarily.
Case Report
A 24-year-old female presented with 2 days of pain in the right iliac fossa, associated with nausea, three episodes of vomiting, and intermittent fever. The bowel habits were unaltered. On examination, tenderness was localized at McBurney’s point and rebound tenderness was evident along with guarding. Blood count revealed leukocytosis (WBC, 15,300/mm3). Ultrasound of the abdomen showed a dilated, noncompressible, thickened appendix. The patient was taken up for appendicectomy through a McBurney’s incision. Intraoperatively, there was evidence of seropurulent fluid collection in the right iliac fossa. An inflamed appendix with a perforated tip was evident with omental adhesions all around. On blunt dissection, another appendix was visualized. The two appendices were adherent to each other with flimsy adhesions. Both the appendices could be separated at the bases and were ligated individually (Figs. 1 and 2). The appendices were removed and sent for histopathological examination which confirmed the diagnosis of double appendix.
Fig. 1.

Two appendicular stumps (B2 type of anomaly)
Fig. 2.
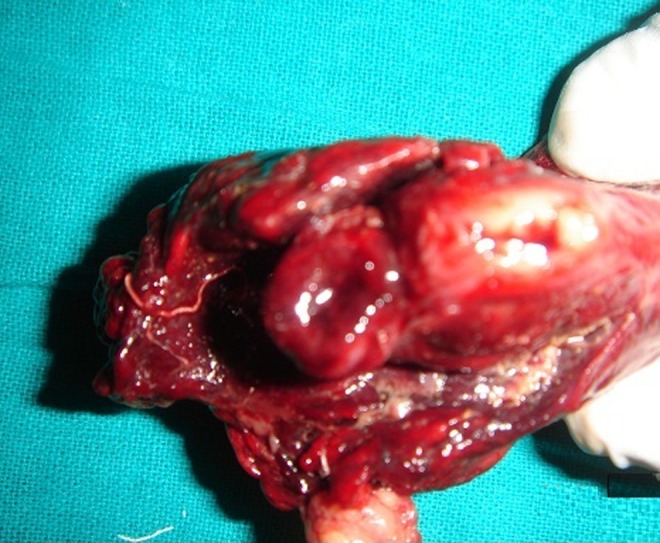
Resected specimen showing the lumens of the two appendices
Discussion
Picoli in 1892 reported the first case of appendiceal duplication in a female patient who had associated anomalies of duplication of entire large bowel, two uteri with two vaginae, ectopia vesicae, and exomphalos [2]. In 1936, Cave first classified appendix duplications which were later modified [1].
Classification of appendiceal duplication [1]:
| Type | Description |
| Type A | Single caecum with partial duplication of appendix |
| Type B | Single caecum with two obviously separate appendices |
| B1 | Two appendices arise on either side of the ileocaecal valve in a “bird-like” manner |
| B2 | In addition to a normal appendix arising from the caecum at the usual site, there is also a second, usually rudimentary appendix arising from the caecum along the lines of the taenia at a varying distance from the first |
| B3 | The second appendix is located along the taenia of the hepatic flexure of the colon |
| B4 | The second appendix is located along the taenia of the splenic flexure of the colon |
| Type C | Double caecum, each bearing its own appendix and associated with multiple duplication anomalies of the intestinal tract as well as the urinary tract |
| Type D | Horseshoe anomaly of the appendix (one appendix has two openings into a common caecum) [3] |
The B2 type of anomaly was noted in our case.
The surgeon has to be aware of such anomalies. A second laparotomy revealing “previously removed” appendix can cause medicolegal problems. In cases with appendiceal duplication, when only one appendix is inflamed, both should be removed to avoid a diagnostic dilemma that may arise later. However, noninflamed duplication found on exploration for some other condition need not be subjected to appendicectomy [4].
Conclusion
Duplication of the appendix should be considered in the differential diagnosis of lower abdominal pain, even if the patient reports a previous appendicectomy. Surgeons should be aware of the potential anatomical variations of the vermiform appendix, and careful inspection of caecum should be performed during laparotomy. Misdiagnosis can cause serious life-threatening complications for the patient and lead to medicolegal problems.
References
- 1.Mushtaque M, Mehraj A, Khanday SA, Dar RA. Double appendicitis. Int J Clin Med. 2012;3:60–61. doi: 10.4236/ijcm.2012.31013. [DOI] [Google Scholar]
- 2.Khanna AK. Appendix vermiformis duplex. Postgrad Med J. 1983;59:69–70. doi: 10.1136/pgmj.59.687.69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mesko TW, Luso R, Breitholtz T. Horseshoe anomaly of the appendix: a previously undescribed entity. Surgery. 1989;106:563–566. [PubMed] [Google Scholar]
- 4.Lin BC, Chen RJ, Fang F, et al. Duplication of the vermiform appendix. Eur J Surg. 1996;162:589–591. [PubMed] [Google Scholar]