

Abstract
Objective. To assess the characteristics of global experiential and didactic education offerings in the pharmacy curricula.
Methods. A 2-stage web-based review of US colleges and schools of pharmacy identified country locations of international advanced pharmacy practice experiences (APPE), globally focused didactic courses, and whether these offerings were interprofessional. Schools were contacted to confirm their offerings and were asked about student participation and demand.
Results. Sixty-four percent of responding schools confirmed an international APPE offering in 67 different countries with an average graduating class participation of 6.1%. Forty-seven percent of responding schools confirmed a globally focused course offering with an average graduating class participation of 13.1%. Almost two thirds of international APPEs and a majority of courses were designated as interprofessional. Student demand did not outweigh supply for either.
Conclusion. Colleges and schools of pharmacy in the United States are continuing to develop global education opportunities for students in the classroom and throughout the world.
Keywords: global health, global education, international practice experience, pharmacy education, didactic course
INTRODUCTION
Interest in global health experiences is rapidly increasing among health professional students in the United States.1-4 Academic institutions are integrating global health into their didactic instruction, experiential rotations, and research opportunities as they realize the importance of global engagement and recognize global health as an academic field.5 A 2011 review of 133 medical schools in the United States reported that 24% have structured programs in global health,6 and, in 2014, 29% of graduating US medical students took part in a global health experience.7 The increased demand for global education opportunities has now led to the exploration of global health educational competencies and approaches by organizations such as the Global Health Education Consortium (GHEC), the Association of Faculties of Medicine of Canada (AFMC), and the Consortium of Universities for Global Health (CUGH).2 The Association of Schools of Public Health (ASPH) recently developed a set of global health competencies that include capacity strengthening, collaborating and partnering, and health equity and social justice among others.8
Colleges and schools of pharmacy have also responded to the growing interest. An unpublished 2010 AACP survey of 114 schools of pharmacy in the United States found that 40 had an active global/international program.9 The results also showed an increase in the number with formal affiliation agreements with foreign institutions. The most common types of agreements included experiential rotations, research collaboration, and faculty and student exchanges. A majority of the respondents reported an increase or no change in their level of global and international affiliations during the year prior to the survey.9,10 Most global education opportunities within pharmacy focus on global health education and training where global health is defined as “an area for study, research, and practice that places a priority on improving health and achieving equity in health for all people worldwide.”11
The globalization of pharmacy education has also impacted national pharmacy associations. The American Association of Colleges of Pharmacy (AACP) responded to the increased interest in global health experiences by approving the establishment of the Global Pharmacy Education Special Interest Group. The purpose of the group is to “provide a forum for the exchange of information, ideas, and programs that pertain to pharmacy education, research, and healthcare on a global basis.”12 Several pharmacy associations such as AACP and the American College of Clinical Pharmacy (ACCP) are also incorporating more globally focused programming into their annual meetings and events. The 2015 AACP Annual Meeting had a global theme and jointly convened with the Association of Faculties of Pharmacy of Canada. The Accreditation Council for Pharmacy Education (ACPE) has begun to certify international pharmacy programs, and the American Society of Health-Systems Pharmacists (ASHP) has recently hired a director of international residency program development.
One suggested strategy for the globalization of the pharmacy profession is to empower students with the knowledge, experience, and skills, such as cultural sensitivity, necessary for future practitioners.13 Students who have participated in global health experiences report positive benefits including increased cultural awareness, enhanced community, social, and public health awareness, and more appreciation for global issues and challenges.14-17 In addition, these experiences can help build confidence and critical-thinking and problem-solving skills.18 Furthermore, international training experiences may be associated with future career choices in underserved or primary care settings.4,14,18 Beyond schools of pharmacy, student organizations recognize the value of establishing student exchange programs throughout the world.19 Finally, a brief exposure to global health education and training can impact medical students years after graduation with many reporting a continued awareness of cultural and socioeconomic factors.14 Along with benefits come challenges, however, including limited funding, language barriers, student safety, travel logistics, and preceptorship.19-21
The majority of publications in the pharmacy literature focus on various aspects of international experiential opportunities for students, but schools of pharmacy are also focused on didactic coursework.19 This is also true in medicine. A national survey found that 61 graduate medical education programs in the United States provided international electives, and 11 programs offered global health tracks.22
The findings of the 2010 AACP survey improved understanding of global affiliations at US schools of pharmacy, but did not assess specifics pertaining to global experiential or global didactic education. A review of the literature since the survey revealed limited information on the overall status of global education opportunities at US schools of pharmacy including where programs were sending students for international advanced pharmacy practice experiences (APPEs) and what global topics were being taught in the classroom. The objectives of this study were to assess global experiential and didactic education opportunities provided to students, determine whether these opportunities were interprofessional, and understand what level of participation and demand there was for such opportunities. This study differs from others in that it provides a representative depiction of global experiential and didactic education opportunities and their associated characteristics at US schools of pharmacy.
METHODS
A 2-stage web-based review of each US accredited or candidate status school of pharmacy as of February 1, 2014 (n=128) was conducted between February and March 2014. The first stage involved a review of each school’s official website using predetermined search terms. The second stage involved correspondence with each school to confirm and clarify their school-specific findings from the website review in stage one. The list of schools was divided between two investigators. Each investigator independently evaluated their respective schools’ websites with the following search terms in order: global health, international rotation, global education, international health, and international APPE. For each search term, the first 30 queries were evaluated. If the school’s website did not have a search box or if data could not be identified after all five search terms, a Google search was then conducted by placing the name of the school before each search term.
Data for each school was collected under two categories: global experiential education and global didactic education. For global experiential education, data was collected on country locations of offered international APPE rotations and the interprofessional designation of these rotations. For global didactic education, data was collected on globally focused courses offered, the interprofessional designation of these courses, and whether the course was required. The interprofessional designation of the rotation or course was determined by reading the description and the corresponding syllabus, if applicable. The data above was collected and stored on a secure electronic spreadsheet. On a separate physical sheet, an experiential education and a professional didactic education contact were identified from each school’s website along with their phone number and e-mail address. This information was stored in a locked file with the name of the school being the common link between the physical and electronic records.
Once stage one of the school’s web-based review was complete, stage two correspondence began with an e-mail sent to the experiential education and professional didactic education contact. The e-mail outlined the purpose of the study, the school-specific findings of the web-based review, and a voluntary request to participate in the study to confirm the stage-one results from the website. Contacts could reply back via e-mail or phone to confirm or clarify the findings if they wished to participate. If a respondent was not heard from within one week, a phone call was made and follow-up e-mail was sent to the contact. In addition, each contact was asked two questions in the e-mail regarding whether demand exceeded supply for international APPE rotations or globally focused courses and what percent of the graduating class completed an international APPE rotation or a globally focused course. Professional education contacts were also asked whether any globally focused courses were required. This study was reviewed and approved by the Institutional Review Board at the University of North Carolina at Chapel Hill.
RESULTS
Of the 128 schools that were e-mailed after the web-based review in stage one, 111 schools for global experiential education and 98 schools for global didactic education confirmed and clarified their school-specific findings during stage two correspondences yielding an 87% and 77% response rate, respectively.
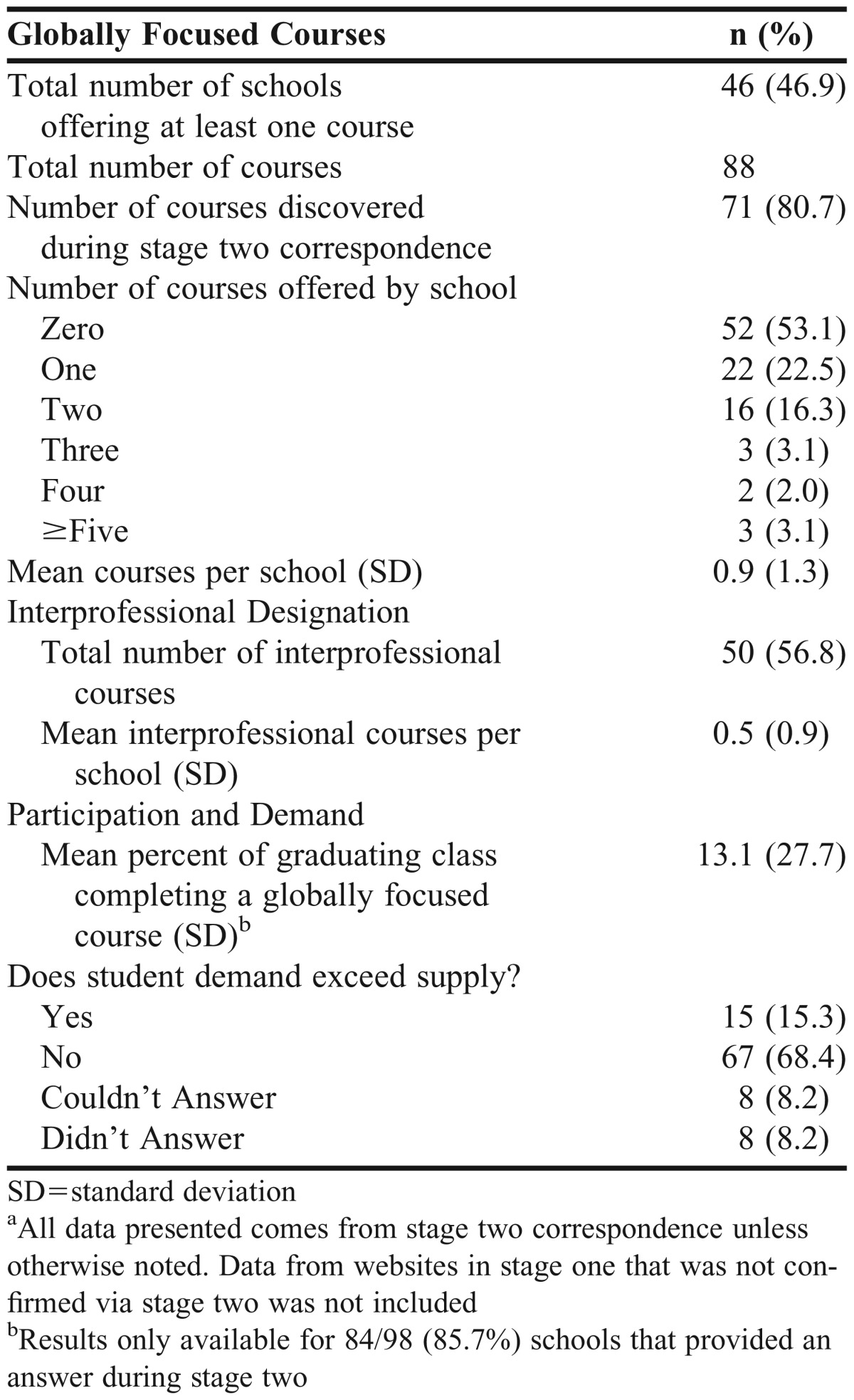
Tables 1 and 2 outline general information on the global experiential and global didactic education offerings at schools that confirmed and clarified their data from the web-based review during correspondence in stage two. Nearly two thirds of all documented international APPEs (173/271) and more than 80 percent (71/88) of globally focused courses were not found through the web-based review of stage one and were collected during correspondence in stage two. Several respondents noted their institution was in the process of either updating their website or that the information was password-protected and could only be viewed by faculty members and students attending that institution.
Table 1.
Characteristics of Global Experiential Education Rotationsa (N=271)
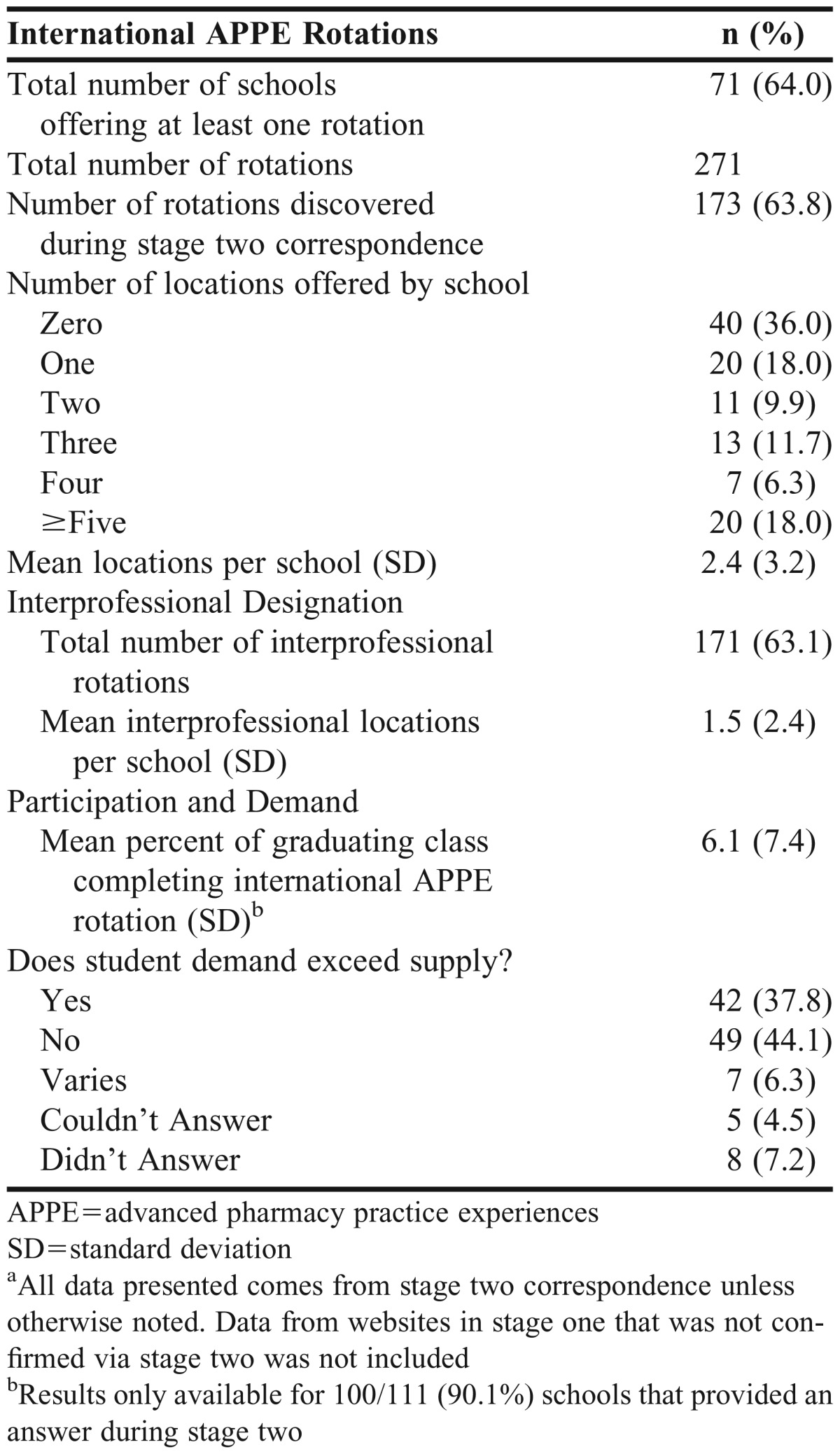
Table 2.
Characteristics of Global Didactic Education Coursesa (N=88)
For global experiential education, 71 of the 111 schools (64%) that received correspondence in stage two offered at least one international APPE rotation in one of 67 different countries and territories (Figure 1). Countries that had the highest number of schools offering an international APPE were England (13), China (12), Thailand (11), Australia (10), Guatemala (10), and Honduras (10). East Asia had the highest geographic concentration of schools offering an international APPE; yet no schools offered an international APPE in central Asia or central Africa. By continent, South America had the fewest number of international APPE rotations, while Asia had the most.
Figure 1.

International Advanced Pharmacy Practice Experiences (APPE) Locations.
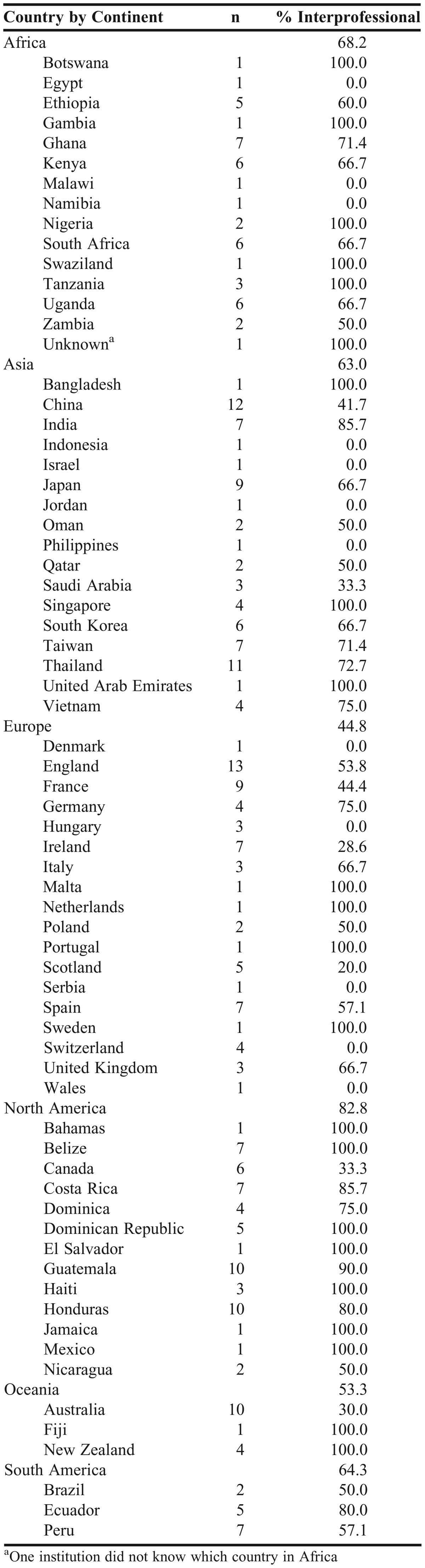
Almost two thirds of all international APPE rotations were designated as interprofessional. More than 80% of APPEs offered in North America were interprofessional, and less than 45% of APPEs were interprofessional in Europe. As seen in Table 3, countries with the highest percent of interprofessional APPEs where at least six schools offer a rotation were Belize (100%), Guatemala (90%), Costa Rica (85.7%), India (85.7%), Honduras (80%) and Thailand (72.7%). Those with the lowest percent were France (44.4%), China (41.7%), Canada (33.3%), Australia (30%), and Ireland (28.6%).
Table 3.
International Advanced Pharmacy Practice Experiences (APPE) Rotations by Country and Continent
The average percent of the graduating class that completed an international APPE was 6.1%. Forty-four percent of schools stated that student demand did not exceed supply. It was often brought up in follow-up correspondence that demand was impacted by the financial burden placed on the students. It was also mentioned that a lack of institutional infrastructure resulting from a shortage of dedicated faculty members and resources for international APPE development could have influenced demand as well.
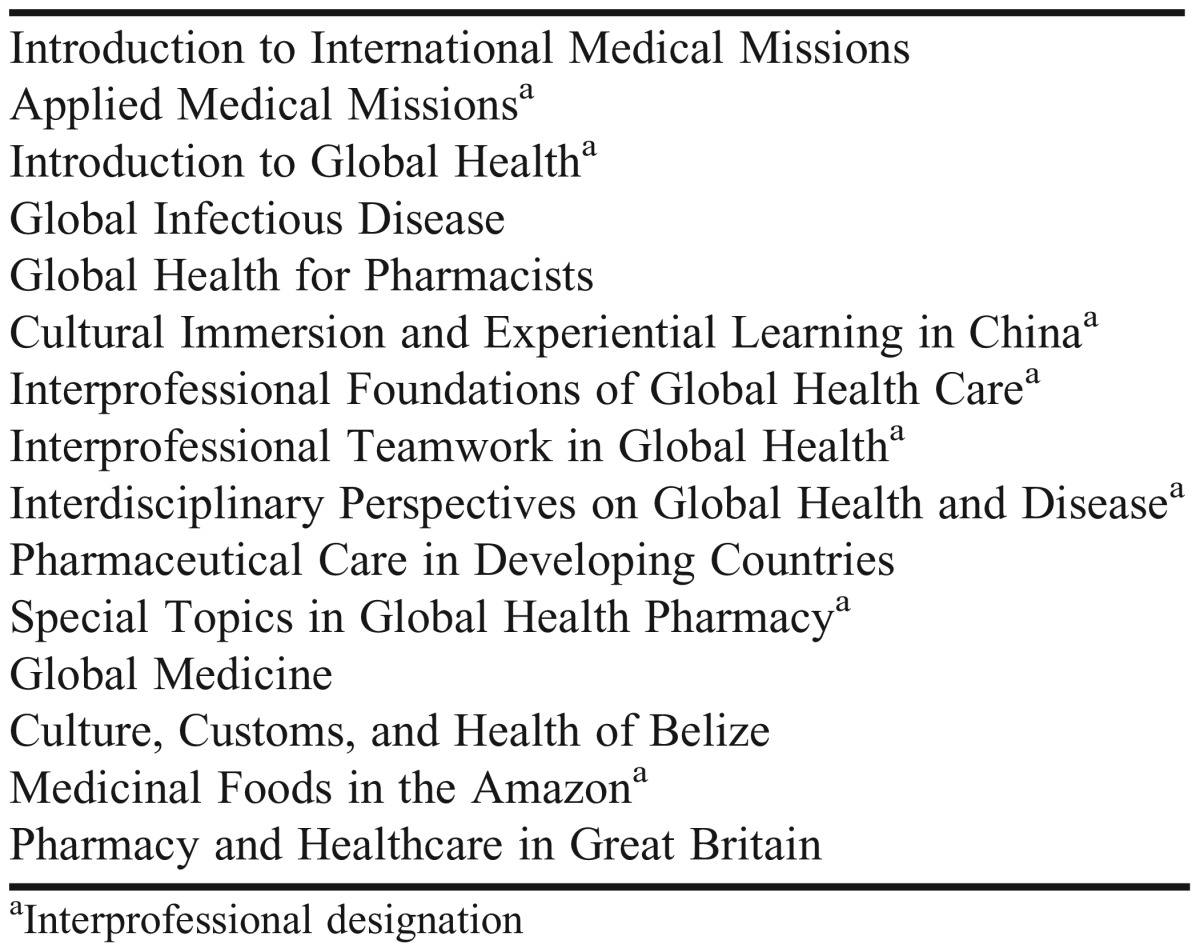
For global didactic education, 46 of the 98 schools (47%) that received correspondence in stage two offered at least one globally focused didactic course. A majority of the courses documented were designated as interprofessional, and almost all courses were considered elective courses. Nearly 30 percent of the elective global didactic courses included an experiential component such as a short-term medical mission trip, and approximately 10% of the courses focused on a particular country or geographic area. Table 4 provides a representative overview of some of the names of the didactic courses. During correspondence in stage two, several school contacts noted that the interprofessional courses were coordinated by a discipline outside of pharmacy such as medicine, nursing, or public health, among others.
Table 4.
Names of Globally Focused Courses
The average percent of the graduating class that completed a globally focused didactic course was 13.1%. Sixty-eight percent of schools stated that student demand did not exceed supply. Several schools noted that although student demand was low, they predicted an increased interest in this field in the coming years, and some were in the process of developing a globally focused course, especially if one did not already exist. Respondents also noted that development of a globally focused course coordinated through the school of pharmacy depended upon faculty interest and experience.
DISCUSSION
The responding schools of pharmacy sent students on international APPE rotations to one third of the world’s countries along a varied pattern of distribution. Asia, along with Europe, had the highest number of countries represented (17), and more than 80% of those countries were located in East or Southeast Asia. These results correlate with the 2010 AACP survey in which US schools of pharmacy had the most global partnerships with countries in Asia. This may reflect the growing interest in US schools forming relationships with countries in that part of the world as many Asian countries continue to evolve their pharmacy education model in order to provide more clinical and cognitive pharmacy services.23,24 In fact, three out of the four internationally certified pharmacy programs by ACPE are located in Asia.25
Many schools were also offering international APPE rotations in English speaking countries such as England and Australia, which could signify an interest in establishing international APPE locations with reduced language barriers. The advantage of having English as a lingua franca could allow for an easier cultural transition and enable students to more readily communicate with patients, peers, and preceptors. Future research may need to examine whether students prefer to participate and whether institutions prefer to coordinate international APPE rotations in English speaking countries. While there was a concentration of international APPE rotations in English speaking countries, there seemed to be a relative lack of opportunities in central Asia, central Africa, and parts of South America. This may be attributable to geopolitical and safety concerns present in those parts of the world.
Of the 67 different countries, 40 (59.7%) were considered to be low to middle income countries (LMICs) by the World Bank.26 This is a slightly higher percent than the 2010 AACP survey that indicated 56.3% of global affiliations were with LMICs. In the 2007 AACP global affiliations survey,9 there were only five African countries represented, and in our study, there were 14 African countries to which schools sent students to for international APPE rotations. A survey conducted by Arif in 2011 documented 52 countries where students went for international experiences, of which 30 (57.7%) were LMICs.19 An increasing presence in LMICs could indicate that many countries, despite their economic standing, have similar pharmacy aspirations and issues, such as ensuring a competent and capable workforce.27 While relationships with LMICs may initially result from faculty connections, they have the opportunity to expand into student opportunities. By sending students to countries with limited resources, students may develop new cognitive frameworks that, when applied in their home country, may solve existing challenges with innovative solutions. Experience in LMICs can also help further define the role of the pharmacist in global health.28
Almost two thirds of all international APPE rotations were classified as interprofessional which is consistent with Cisneros et al’s study.21 Global health interventions necessitate interdisciplinary collaboration and interprofessionalism, which the World Health Organization (WHO) emphasized as being integral for health care professionals on collaborative practice teams.29 Students participating in interprofessional international experiences also report significant benefit from working in teams and learning more about each discipline’s role. Arif reported that interdisciplinary collaboration could be a valuable part of the student international experience.19 More than 70% of the rotations offered in LMIC countries were classified as interprofessional compared to just over 50% for high-income countries. The disparity may indicate a stronger need for interprofessional collaboration in resource-limited settings. It should also be recognized that health care education and systems are designed to address local needs, which differ from country to country. Therefore, the application of concepts to address those needs, such as interprofessional collaboration, may vary.
North America had the highest average concentration of interprofessional rotations of all the continents which could be attributed to the interprofessional nature of medical mission trips that often occur in Central American countries such as Guatemala, Honduras, and Costa Rica. Pharmacists can play a vital role on short-term medical mission trips and enable the provision of quality health care and pharmacy services.30 Europe had the lowest average percent of rotations classified as interprofessional (44.8%). This could be attributed to European countries having a stronger emphasis on research and pharmaceutical sciences within the curriculum. Future research could examine why Europe has the lowest average percent of rotations classified as interprofessional.
In the classroom, student pharmacists were exposed to the concepts of globalization and global health, with almost half of US schools offering some sort of globally focused course. This is slightly higher than the 2011 survey by Arif indicating that 42.6% of schools offered a global health course.19 Globally focused didactic opportunities could help prepare students for international APPE rotations regardless of location. However, there is a lack of information in the literature on what didactic opportunities exist. Several of the didactic course offerings were part of a structured global health program. Many schools also noted that their global didactic offerings included an experiential component as part of the course such as a medical mission trip or a service learning experience. There is a need to further understand why schools offer particular globally focused courses and the competencies that these courses are developing. Schools looking to develop courses focused on global health should consider looking at the competency frameworks being developed in medicine and public health.8 In addition to globally focused courses, schools can incorporate preparatory activities such as global health journal clubs, seminars, and service projects with locally underserved populations.14 Future research could examine what types of global activities students prefer on how these activities can influence their professional development.
Participation in global pharmacy education opportunities seemed to lag behind participation in such opportunities in other disciplines such as medicine. The rate of 6.1% of student pharmacists participating in an international experience was behind the 29% of medical students who did so in 2014 and was comparable to the 5.9% of medical students who completed an international experience in 1978.15Although participation in globally focused didactic courses was more than twice of that for international APPE rotations, demand was substantially greater for international APPE rotations indicating that financial and logistical barriers may preclude students from participating in such opportunities. While overall student demand did not outweigh supply, there was higher student demand than supply for international APPE rotations at schools that offered at least one international rotation, indicating that awareness of such opportunities could facilitate interest.
A limitation to the study is that the definition of interprofessional was not defined in the e-mail sent to school contacts. The investigators defined interprofessional according to the WHO definition: “when students from two or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes.”31 Some participants also were confused regarding the term “globally focused course.” When asked, the investigators stated that it was a course where a majority of the content pertained to the world. Globally focused was used as opposed to global health in order to have a more comprehensive understanding of global education offerings, although most courses seem to be focused on global health. The lack of clarity around these definitions could have led to participants misclassifying rotations or courses as interprofessional and courses as global.
A strength of the study was the 2-stage web-based review, which allowed for the confirmation and clarification of information found from the website review in stage one. As mentioned, much of the information on rotations and courses was identified during stage two and without this additional step, the data would not be accurate or representative. While just a stage two survey could have been conducted, stage one allowed the investigators to present school-specific findings, which may have led to a higher response rate. However, a limitation to the e-mail correspondence in stage two was that some e-mail responses by school contacts were vague and required further clarification.
CONCLUSION
Schools of pharmacy in the United States are continuing to develop and provide global education opportunities for students in the classroom and throughout the world. Pharmacy schools can work on collaborating further with each other and with other health disciplines in developing more global curricular options and experiences. To enable global education opportunities, schools also may need to identify and address barriers such as faculty development, administrative support, resource allocation, and capacity building among others. As the role of the pharmacist in global health becomes more clearly defined, schools have the opportunity to use these experiences to prepare the next generation of globally minded pharmacists.
REFERENCES
- 1.Pfeiffer J, Beschta J, Hohl S, Gloyd S, Hagopian A, Wasserheit J. Competency-based curricula to transform global health: redesign with the end in mind. Acad Med. 2013;88(1):131–136. doi: 10.1097/ACM.0b013e318276bdf4. [DOI] [PubMed] [Google Scholar]
- 2.Battat R, Seidman G, Chadi N, et al. Global health competencies and approaches in medical education: a literature review. BMC Med Educ. 2010;10(1):94. doi: 10.1186/1472-6920-10-94. http://www.biomedcentral.com/1472-6920/10/94 . Accessed November 10, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rassiwala J, Vaduganathan M, Kupershtok M, Castillo FM, Evert J. Global health educational engagement – a tale of two models. Acad Med. 2013;88(11):1651–1657. doi: 10.1097/ACM.0b013e3182a6d0b0. [DOI] [PubMed] [Google Scholar]
- 4.Francis ER, Goodsmith N, Michelow M, et al. The global health curriculum of Weill Cornell Medical College: how one school developed a global health program. Acad Med. 2012;87(9):1296–1302. doi: 10.1097/ACM.0b013e3182628edb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Merson MH. University engagement in global health. N Engl J Med. 2014;370(18):1676–1678. doi: 10.1056/NEJMp1401124. [DOI] [PubMed] [Google Scholar]
- 6.Peluso ML, Forrestel AK, Hafler JP, Rohrbaugh RM. Structured global health programs in US medical schools: a web-based review of certificates, tracks, and concentrations. Acad Med. 2013;88(1):124–130. doi: 10.1097/ACM.0b013e3182765768. [DOI] [PubMed] [Google Scholar]
- 7.Medical school graduation questionnaire. 2014. all schools summary report. Association of American Medical Colleges. https://www.aamc.org/download/397432/data/2014gqallschoolssummaryreport.pdf. Accessed November 1, 2014.
- 8.Ablah E, Biberman DA, Weist EM, et al. Improving global health education: development of a global health competency model. Am J Trop Med Hyg. 2014;90(3):560–565. doi: 10.4269/ajtmh.13-0537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Sagraves R. Survey of current global affiliations of US colleges and schools of pharmacy [unpublished raw data]. Alexandria, VA: American Association of Colleges of Pharmacy. 2010.
- 10.Audus KL, Moreton JE, Normann SA, et al. Going global: the report of the 2009-2010 Research and Graduate Affairs Committee. Am J Pharm Educ. 2010;74(10):Article S8. doi: 10.5688/aj7410s8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Koplan JP, Bond TC, Merson MH, et al. Towards a common definition of global health. Lancet. 2009;373(9679):1993–1995. doi: 10.1016/S0140-6736(09)60332-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Global pharmacy education special interest group of the American Association of Colleges of pharmacy bylaws. American Association of Colleges of Pharmacy. http://www.aacp.org/governance/SIGS/global/Documents/GlobalPharmEdSIGBylaws7-09.pdf. Accessed November 6, 2014.
- 13.Alsharif N. Globalization of pharmacy education: what is needed? Am J Pharm Educ. 2012;76(5):Article 77. doi: 10.5688/ajpe76577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Drain PK, Holmes KK, Skeff KM, Hall TL, Gardner P. Global health training and international clinical rotations during residency: current status, needs, and opportunities. Acad Med. 2009;84(3):320–325. doi: 10.1097/ACM.0b013e3181970a37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Drain PK, Primack A, Hunt DD, Fawzi WW, Holmes KK, Gardner P. Global health in medical education: a call for more training and opportunities. Acad Med. 2007;82(3):226–230. doi: 10.1097/ACM.0b013e3180305cf9. [DOI] [PubMed] [Google Scholar]
- 16.Gourley DR, Vaidya VA, Hufstader MA, Ray MD, Chisholm-Burns MA. An international capstone experience for pharmacy students. Am J Pharm Educ. 2013;77(3):Article 50. doi: 10.5688/ajpe77350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Owen C, Breheny P, Ingram R, Pfeifle W, Cain J, Ryan M. Factors associated with pharmacy student interest in international study. Am J Pharm Educ. 2013;77(3):Article 54. doi: 10.5688/ajpe77354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Thompson MJ, Huntington MK, Hunt DD, Pinsky LE, Brodie JJ. Educational effects of international health electives on US and Canadian medical students and residents: a literature review. Acad Med. 2003;78(3):342–347. doi: 10.1097/00001888-200303000-00023. [DOI] [PubMed] [Google Scholar]
- 19.Arif SA, Gill TK, Reutzel TJ. Barriers to offering international experiences to pharmacy students by U.S. colleges of pharmacy. Curr Pharm Teach Learn. 2013;5(5):387–393. [Google Scholar]
- 20.Nelson BD, Lee AC, Newby PK, Chamberlin MR, Huang CC. Global health training in pediatric residency programs. Pediatrics. 2008;122(1):28–33. doi: 10.1542/peds.2007-2178. [DOI] [PubMed] [Google Scholar]
- 21.Cisneros RM, Jawaid SP, Kendall DA, et al. International practice experiences in pharmacy education. Am J Pharm Educ. 2013;77(9):Article 188. doi: 10.5688/ajpe779188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kerry VB, Ndung’u T, Walensky RP, Lee PT, Kayanja VF, Bangsberg DR. Managing the demand for global health education. PLoS Med. 2011;8(11):e1001118. doi: 10.1371/journal.pmed.1001118. http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.1001118 Accessed November 10, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Khan T, Anwar M, Mueen Ahmed K. A perspective for clinical pharmacy curriculum development and validation in Asian developing nations. J Young Pharm. 2011;3(2):151–154. doi: 10.4103/0975-1483.80304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ryan M, Shao H, Yang L, Nie X, et al. Clinical pharmacy education in China. Am J Pharm Educ. 2008;72(6):Article 129. doi: 10.5688/aj7206129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Directory of Certified Programs. Accreditation Council for Pharmacy Education. https://www.acpe-accredit.org/pdf/DirectoryofCertifiedPrograms.pdf. Accessed November 15, 2014.
- 26.Country and lending groups. The World Bank. http://data.worldbank.org/about/country-and-lending-groups. Accessed November 10, 2014.
- 27.Bruno A, Bates I, Brock T, Anderson C. Towards a global competency framework. Am J Pharm Educ. 2010;74(3):Article 56. doi: 10.5688/aj740356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Steeb DR, Joyner PU, Thakker DR. Exploring the role of the pharmacist in global health. J Am Pharm Assoc. 2014;54(5):552–555. doi: 10.1331/JAPhA.2014.13251. [DOI] [PubMed] [Google Scholar]
- 29.Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes (update) Cochrane Database Syst Rev. 2013;3:CD002213. doi: 10.1002/14651858.CD002213.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Johnson CA, Stieglitz N, Schroeder ME. Opportunities and responsibilities for pharmacists on short-term medical mission teams. J Am Pharm Assoc. 2009;49(6):801–807. doi: 10.1331/JAPhA.2009.08172. [DOI] [PubMed] [Google Scholar]
- 31.Framework for action on interprofessional education and collaborative practice. World Health Organization. http://www.who.int/hrh/resources/framework_action/en/index.html. Accessed November 1, 2014. [PubMed]