

Abstract
Background:
The introduction of antiretroviral therapy has caused a remarkable decrease in the occurrence of diseases and mortality among HIV-positive patients, while this success has not been achieved among injection addicts due to a low adherence to antiretroviral medicine. This study aims at clarifying the important factors affecting adherence to treatment in addicts suffering from HIV.
Materials and Methods:
In this qualitative research, data were gathered through in-depth interviews and field notes, and were interpreted through content analysis in the form of constant comparison. The participants were 16 drug addicts living with HIV/AIDS. Most of them had records of imprisonment and were receiving Highly Active Antiretroviral Therapy (HAART) drug treatments in the AIDS center of Imam Khomeini Hospital complex, affiliated to Tehran University of Medical Sciences. Sampling was started in a purposive method and was continued until data were saturated.
Results:
Four main categories including psychological reactions, contradictory beliefs, perceived support, and individual and environmental barriers were extracted from the data, each having some sub-categories.
Conclusions:
The obtained results indicated that adherence to the treatment of HIV is not constant and mono-dimensional, but is a function of different factors. Hence, an individual having feeble adherence in a specific time and under specific circumstances may show desirable adherence under a different circumstance. Thus, treatment of addicts living with HIV/AIDS requires physical, psychological, and social attention along with drug treatments.
Keywords: Acquired Immunodeficiency Syndrome, adherence medication, drug addicts, drug users, HIV, Iran, treatment adherence
INTRODUCTION
Although AIDS was discovered about three decades ago, it is still considered as a unique issue in comparison with other medical and social issues. Considering medical perspectives, this disease is a fatal and longitudinal disease that destroys the body's immune system and bestows a gradual death to its host.[1] Moreover, regarding social considerations, it is considered as a shame which targets individual's social dignity.[2] Unfortunately, the outbreak of human immunodeficiency virus (HIV) is rapidly expanding in some areas of the world, especially in the developing countries.[3] Based on the data of case registry in Iran, until 21 September 2013, there were 27,041 individuals identified as being infected by the HIV/AIDS virus, of which 89.3% were male and 10.7% were female. So far, 5118 of these identified cases have entered into AIDS stage and 5471 people have died. Also, 45.9% of the infected patients were 25–34 years old when infected by this virus and this was the highest rate among different age groups. The causes of HIV infection among all registered cases in 2013 were respectively: Injecting drug users (52%), sexual intercourse (33.2%), and mother to child transmission (3.4%). In 11.4% of the identified cases during this year, the transmission mode was unknown and no new cases of transmission through blood transfusion were reported.[4]
The most common and known drug regimen is Highly Active Antiretroviral Therapy (HAART), which remarkably decreases the virus spread in the body. Results of clinical trials show that a reduction in viral load can be related to a reduction in infection and an increase in life expectancy.[5] The introduction of antiretroviral therapy has created a remarkable decrease in the occurrence of diseases and fatality caused by HIV; however, this success has not been achieved among injection addicts and the reason is their low adherence to antiretroviral drugs.[6] It should be noted that a desirable result can only be achieved by treatment adherence of over 95%.[7] Evidences show that a feeble level of adherence blocks the treatments and leads to early involvement of the patient with opportunist infections, and thus the life span is decreased.[8]
Adherence to treatment means following the drug regimen daily and regular and accurate use of the medicine doses at the proper time and according to the physician's prescription. Irregular use of the medicine facilitates medical resistance and HIV becomes resistant against the prescribed drug regimen, or even similar drug regimen which the patient has not received yet, and in this way, the treatment fails.[8]
Rate of adherence among Iranian patients living with HIV/AIDS is 65%, and probably, this rate is even less among addicts.[9] This group of patients, besides being addicted, suffer from psychological disorders, unemployment, homelessness, and social instability. So, they are less probable to receive the medical care needed, their treatment is delayed, and they have thin adherence to treatment.[10]
Considering the undeniable effect of adherence to treatment on reaching desirable treatment results, clarifying the important factors on treatment adherence and showing the relationship of these factors and the cultural context of the society is highly essential. Many studies have been carried out all around the world regarding the negative effect of drug abuse on treatment adherence and different results have been obtained. Some of these researches have shown a relation between these two[11] and some others have claimed that there is no relation between drug abuse and treatment adherence.[12] Unfortunately, data about the effective factors on adherence to treatment based on the patients’ experiences is limited. Hence, it is of utmost importance to carry out qualitative research for perceiving the reality of factors influencing adherence to treatment in drug addicts living with HIV/AIDS.[13] Applying a naturalistic approach for reaching a better comprehension of the nature of different phenomena in its specific context, like the real life, is very apt for sensitive and important issues such as HIV/AIDS and can answer the complications of human behavior.[14] Hence, it can enrich our knowledge about the complications and multiple factors of adherence to treatment. The above-mentioned issues emphasize the need of a qualitative research in this field. The qualitative research carried out in other countries has introduced factors such as social support, having related knowledge, observing the positive effects of treatment, medicines’ side effects, and forgetfulness, which influence adherence to treatment,[15,16] and this shows that treatment adherence in HIV/AIDS patients has many complexities and is affected by different social, cultural, psychological, biological, and economic factors. This qualitative research aims at clarifying determinative factors of treatment adherence through talking with HIV addicts.
MATERIALS AND METHODS
This study is a part of a qualitative research, analyzed through qualitative content analysis. Content analysis is a research approach that is used for interpreting hidden semantic units in a written content. In this method, the codes, main categories, and sub-categories are identified through a systematic approach.[17]
Participants in the study were those who had enough and first-hand experience about the topic, and thus were qualified people for taking part in this study. They also had records of drug or alcohol addiction and mostly had records of imprisonment as well. Inclusion criteria were: Patients living with HIV/AIDS as declared by the serological test, receiving treatment with HIV/AIDS antiretroviral drugs, and giving consent to participate in the study. The exclusion criterion was lack of consent to participate in the research and non-prescription of HIV/AIDS antiretroviral medications. The participants were receiving treatment in the AIDS center of Imam Khomeini Hospital affiliated to Tehran University of Medical Sciences. Written consent was obtained from the participants and they were reassured that their conversations would remain confidential.
The participants were invited for the interview through a purposive, convenience sampling method. Decisions about the number of deep, individual interviews were taken based on data saturation, and data collection lasted from August 2013 to July 2014.
Open and semi-structured questions were used in the interviews. The participants were motivated to share their experiences about their disease and addiction and its effects on following their medical treatments. Following questions were posed based on the experiences discussed by the participants, for obtaining some in-depth information and clarifying the topic under investigation. The interview started with these questions: “How is your life with this virus (HIV virus)?” “What therapeutic measures have you taken?” The rest of the questions were formed based on the participants’ answers to these questions. The participants were asked to clarify their viewpoints through concrete instances, and questions like “What do you mean by that?,” “Explain more please!,” and “From what you just said, I get that …, am I right then?” were asked to deepen the interviews. The duration of the interviews varied and ranged between 20 and 70 min, based on the interviewee's concern and interest. In addition to conducting in-depth interview, the researcher's field notes were recorded while the patients were being visited by the infections specialists, received their medicine at the pharmacy, and waited in the waiting room. The objectives of the research were clarified and explained to the participants and their written consent was obtained. The location of this research was the AIDS center and clinic of Tehran's Imam Khomeini Hospital, and the reason for choosing this clinic was it being the main center of the country.
Data analysis was carried out by MAXQDA10 software, using Graneheim and Lundman's suggested analysis method.[14] The analysis was carried out during data collection process, and each interview was implemented and analyzed before the next interview started. To analyze the data, first the content of each interview was read several times. Then the important sections which were related to the research objectives were identified and a constant comparison of the codes to each other and to previous codes was accomplished during the analysis process. In the next step, the basic codes were classified under categories and sub-categories based on similarities and differences; later, the similar sub-categories were merged together and composed the major categories with more abstract concepts. This process was continued till the end of the data collection process. Allocation of enough time and constant interaction with the participants in the research field, and use of observation method, deep interviews, field note taking, and revision of the observers (external checking) were used for validating the data. To prove the reliability of the data, inquiry audit was performed.
Ethical considerations
The protocol of this study has been approved by Tehran University of Medical Sciences.
RESULTS
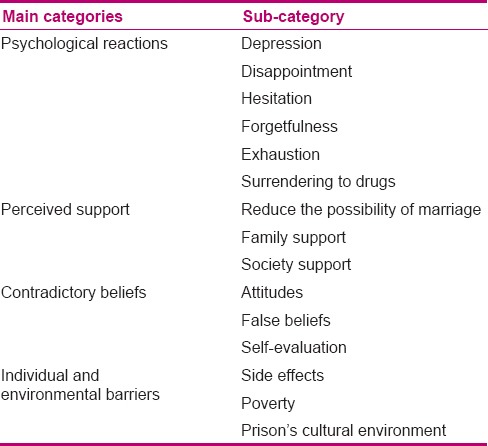
After performing 16 interviews, data codes and categories attained saturation. The demographic specifications of the participants are depicted in Table 1. Four major categories were extracted from the data as effective factors in treatment adherence: 1. psychological reactions, 2. perceived support, 3. contradictory beliefs, and 4. individual and environmental barriers. More details about the categories and sub-categories are presented in Table 2. Each sub-category is extensively discussed below.
Table 1.
Social and demographic characteristics of the participants
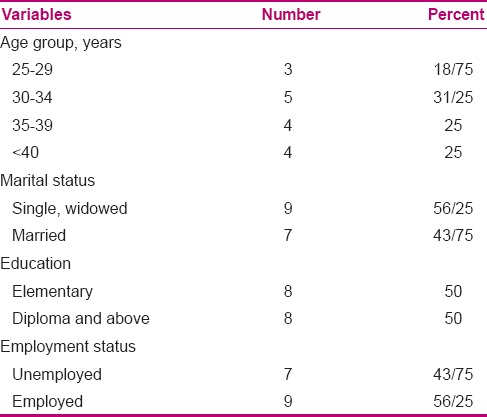
Table 2.
The main categories and sub-categories
Psychological reactions
Psychological reactions are the psychological tactics to cope with HIV/AIDS and taking medications is affected by these reactions.
Main factors affecting the use of antiretroviral drugs, considering the psychological reactions of the participants were depression, disappointment, hesitation, forgetfulness, and exhaustion. All participants emphasized on depression as an important factor.
Depression
Depression is common among positive HIV patients[18] and causes debility among them. The patients’ depression is of high importance as it negatively affects their treatment adherence and, consequently, the desired result of the treatment cannot be achieved.[19,20]
“I, myself, liked to go back and take my drugs, but I took about 30 acetaminophen codeine a day and I was depressed, very depressed, and I used methyl amphetamines as well. Depression caused by methyl amphetamines is so tense; I didn’t take the drugs because I was depressed.” (participant 3)
Disappointment
Some of the participants considered disappointment in life as a reason for not taking their medicine:
“I used to take them, but I no longer take the pills. I have no hope in this life, why should I take them? I have boycotted myself. No one will live forever, I know, why I should get medicine. When I get up in the morning, I am in despair, what am I going to do. Now I am just dependent on heroin.” (participant 10)
Hesitation
Some of the participants talked about their hesitations about choosing between taking medicines and abusing drugs:
“When using these pills, our drug abuse is multiplied. I don’t know! It does not work, we should use much more drugs. We are worried if we use drugs, the pills loss their effectiveness and if we take the pills, the drugs are vanished away. The medicine just ruins the drugs.” (participant 9)
Another participant talked about his hesitation in using alcoholic drinks or antiretroviral medicine, and when asked “What makes you prefer drinking while you know well that it washes away the effects of medicine?” he said:
“I thought that I shouldn’t do that, don’t drink, you won’t die of it, but if you stop taking medicine you will die. But it is a long time I am addicted to drinks, it is true that the doctor says it washes away the medicine, but I used to take medicine for 10 years and drank too and nothing happened. I don’t know, maybe my body is different, maybe the condition of my body is like this, it is 5 years I don’t take medicine and still it is 300 CD4.” (participant 3)
Forgetfulness
Some patients reported that they forget taking their medicine. Forgetting to take the medicine can be due to a damage that this virus causes on the nerve system, or lack of attention, or negligence of the patient. In this regard, one of the participants stated thus:
“I overused methyl amphetamines and made the methyl amphetamines myself. Then there were times I was awake for a week. I said to myself now that I am awake for a week or two, if I take the pills, my body will get weaker. Anyway they were postponed, and finally I forgot that I should take pills.” (participant 3)
Exhaustion
Some of the participants stated that they are fed up with taking medicine and for this reason, they have stopped taking them:
“I knew that I should take them as long as I am alive, it is difficult, I get tired of it. Maybe if I knew it is for 10 years, for example, it could have been much easier.” (participant 2)
“I took my night medicine for 2–3 months, but I am fed up with taking pills and when I take them, I have a deeper hangover.” (participant 9)
To sum up, the results indicated that hesitation, depression, disappointment, forgetfulness, and exhaustion are among the most important psychological reactions of addicts living with AIDS regarding antiretroviral treatment adherence.
Surrendering to drugs
Some of the participants talked about not being able to resist against using drugs.
“When I used drugs, I didn’t think of treatment at all. If I was using drugs, I didn’t come here for receiving treatments. I totally denied my disease and joked about treatment. Now that I have abandoned drugs, I have retrieved a bit of my sanity …. people using drugs sometimes encounter some pressures, and under these pressures, I performed some acts that later I just wondered why did I act like that when I used drugs.” (participant 7)
Perceived support
Perceived support means the perceptions of help received from others. It is known that having a social support in different levels is an important factor in creating a motivation for setting up and continuing treatments. The participants emphasized on losing support of their wife, family, and society as an important factor for not being bound to their treatments.
Reduction of the possibility of marriage
One of the participants talked about getting disappointed from marriage and having a family:
“It is five years I’m not taking medicine, I wanted to marry, but everything was ruined. I loved her, but they just refused. Then I duplicated my drugs and put aside the medicine. At that time, I just used methyl amphetamines for fun, but when I proposed to her and they understood I have AIDS, they did not even answer and just concealed her from me. Then, I thought ok, come on, just let it go.” (participant 3)
“Most of my problems are of loneliness. I am emotionally so irritable. I wanted to marry, but when I talked about my problem, it was all gone. I just wanted to be honest, but it was cancelled and I lost my adherence to treatments.” (participant 7)
Family support
Family is the best place to support patients living with AIDS. Family support can invoke patients’ adherence to treatments and enhance their life quality. Some of the patients mentioned that they have lost their family's support:
“Until last year, I came and got my medicine every month and took them, but now, just to challenge my mom, it is a year since I have not taken any medicine.”
When the researcher asked him why he opposed and challenged his mom and why it caused him to stop taking his medicine, he said:
“My mom ignored me and bothered me at home. Then I said, ‘I won’t take medicine to die and get rid of everything.’” (participant 5)
On the other hand, the patients who were bound to their treatments talked about having their family's support.
“My parents provide anything I want so that I don’t go towards drugs. At home my sister gives me my medicine regularly.” (participant 11)
Society support
Society support is the people's assistance to individuals in crisis and need situations and can be emotional or instrumental. Receiving society support adds on to patient's satisfaction and motivation to continue treatment.
The participants talked about society support and one of them talked about people's behavior toward him:
“Regarding AIDS medicine, sometimes I think of putting them aside and not taking them anymore when I see people who don’t know anything about my disease and willingly or unwillingly assassinate my character. For example, I had a dispute with my brother-in-law. Then his brother told my sister, ‘you better control your brother who has got AIDS because of abusing drugs.’” (participant 6)
When asked why all these cause him not to take his drugs, he said:
“Well, I lose my courage. I am doing the best I can, so that I want to have my dignity. For example, my cousin who is informed about my disease tries to keep herself and her child totally away from me. These are all emotional bumps for me.”
Contradictory beliefs
Beliefs are the viewpoints of individuals regarding the truth and correctness of a phenomenon or an issue, and contradictory beliefs are the ones which do not make sense at the same time.
Contradictory beliefs include three sub-categories: Attitudes, false images of treatment, and self-evaluation. The participants had different beliefs in this regard.
Attitudes
Attitudes are guided beliefs and relatively constant and stable feelings regarding an individual or a situation. Attitudes and mentality of the patients are of high importance regarding patients’ receipt of the treatments. In this view, one of the participants stated thus:
“In the beginning it was hazardous for me. The TV news showed AIDS as something related to the African black people. With bones out, they showed terrible images and this had caused me think of AIDS as a monster and when they told me I am affected, my heart was about to stop. But later I understood that it is not like that.” (participant 2)
False beliefs
Some of the participants had some false beliefs about the treatment and this had stopped their adherence to treatment.
“I believe that each person knows his body better. I know my body better than doctors, sometimes I take medicine and sometimes not. Herbal drugs work better for me in comparison with these chemical medicines, they wash away body infections.” (participant 4)
Self-evaluation
To feel being worthy and having self-respect is another important factor in the constant use of medicine. The participants had different views regarding themselves.
“I am a troubled person and it is not something I wanted and chose. I am a real villain, to be honest. My mother begged me and sent me to take medicine. I told her, ‘just pull them away, I won’t take them, let me just die. I will leave all the happiness and joy for your enemies.’ God knows I cannot remember having experienced happiness, so many troubles I have faced, I have been beaten so much.”
When asked why all these caused the person not to take his medicine, he said:
“I think just let it reach its end, I begged God to press my off button please, is it not enough? 33 years of agony has not compensated my crimes yet? How much more misery I have to carry? I beg just let me die, I don’t want to continue anymore, let the disease grow and destroy me so that I am released of all this pain.” (participant 14)
On the other hand, some participants who were bound to using their medicines had different beliefs:
“I don’t want to be shut-in and homebound one day, or be dependent on others and beg for help. As long as possible, I want to be an effective man and help others. I think I either shouldn’t have started taking medicine or now that I have started, I should take them on time. No one knows how long am I going to live. So, as long as I am alive, I would like to live a healthy life… I abandoned smoking and drinking alcohol, as alcohol intervenes with my medicine. So I thought it will not kill me if I don’t drink. Now that I have this problem, I should bind to my medicines. I should live a good, right and healthy life so that I am not a shame for my family.” (participant 12)
Individual and environmental barriers
There are factors inside and outside the individual which cause adherence to the problem.
Participants demonstrated that there were many barriers to achieve effective adherence. These ranged from physiological aspects to cultural and economic concerns including side effects, poverty, and prison's cultural environment.
Side effects
Living with the side effects of medicine was one of the other factors mentioned by the participants.
“These pills have some side effects as well. They wash away all your stamina and leave you bloodless. When I use them, my stomach aches, my head is not mine any more, then I do things without really knowing what I am doing. I am out of me, my behaviour and character changes, it is all unconscious, so everybody thinks that I have used methyl amphetamines.” (participant 9)
Poverty
Poverty is inability to meet human needs. A person who has insufficient economic power and cannot meet her/his health requirements is said to be stricken by poverty. So, another important factor that was repeatedly emphasized by the participants was poverty.
One of the participants who was desperate and frustrated under the pressures of economic problems said:
“When I even don’t have some bread to eat, how can I think about my medicine? Landlord wants to vent my furniture, how can I take medicine? I don’t even have 1000 tomans to pay for medicine; I have to spend 5000 monthly just to come here. When I don’t have these provisions, everything is just a mishmash. So, my medicine program is abandoned too; one day I take the medicine and one day not.” (participant 9)
Prison's cultural environment
Another issue that was mentioned by the participants having records of imprisonment was the prison's cultural environment for taking medicine.
“Once I was imprisoned for 20 days, I didn’t take my medicine there, I was ashamed of taking them, didn’t want others to change their opinions about me. It was a shame to take pills, I was afraid they call it foppery and think of me as a weak and sick person. When in prison, you should either have lots of money or be powerful and mighty to have a comfortable life…. I didn’t want to take medicine so that they would say he is about to die and needs medicine.” (participant 8)
DISCUSSION
The present study is a qualitative research about drug addicts with HIV/AIDS in Iran, and explored details of adherence to antiretroviral treatments from the participants’ expressions. Four major categories were extracted from the obtained data: Psychological reactions, contradictory beliefs, perceived support, and individual and environmental barriers.
Psychological reactions with sub-categories such as depression, disappointment, hesitation, forgetfulness, and exhaustion due to drug abuse and AIDS disease negatively affected the patients’ adherence to treatment. Depression was the most common secondary complication of HIV infection and is the most common psychological disorder among people with positive HIV.[21] Some of the patients claimed that their depression started with the use of drugs or alcoholic drinks. This is compatible with the results obtained by Jaquet et al. The result of their study indicated that more than 70% of participants with HIV who had drug abuse suffered from depression.[22] The participants also indicated that due to depression, their adherence to treatment has decreased and has caused them to totally stop taking the prescribed medicine. The medical science and previous research also confirms these claims. As Capaldini and Harison state, depression causes drug and alcoholic drink abuse and disturbs adherence to antiviral treatments.[23] It seems that emphasis on treatment of depression along with using anti-HIV medicine can enhance the motivation and adherence to treatment in this group of patients.[24] Since the drug addicts living with AIDS are mostly homeless and boycotted by the society, they usually do not have access to sanitary and remedial services including mental health services. Hence, there should be some solutions, so that these patients can use therapeutic care as much as possible. Peer support can be a suitable solution for gathering these patients together and holding consultation meetings and group therapy. As evidences show, group therapy can be an effective method for decreasing depression. Due to sharing experiences among the members of this group and the patient's attention to the fact that other members of the group suffer from the same problems, and through interaction with peers and being accepted by them, the patient shows his suppressed emotions and his depression and disappointment will decrease through the support and compassion he receives from the other group members and his adherence to treatment will be enhanced.[25]
Psychological reactions such as forgetfulness, hesitation, and exhaustion caused due to taking drugs create a great challenge for the participants’ adherence to treatments. Their hesitation for taking drugs is due to the interference of anti-AIDS medicine with drugs and it seems to reduce the joy they receive from using drugs and alcohol. A research carried out by Remien et al. on homosexual and injection addicted men and women certifies the results of this study.[16] On the other hand, memory problems, lack of attention, and feeble motivation are important factors interfering with adherence to medical treatments.[26]
Society considers addicted people as criminals, but in this case, addiction is considered as a disease and addicts are treated like sick people, not as criminals. Judiciary and security systems change their policies and follow and execute their anti-drug campaigns for controlling drug use. It is probable that people in the society show more flexibility with these patients so that their motivation for treating their addiction and AIDS is enhanced.
The participants talked about support and its important role in following the treatments. They indicated that receiving emotional and instrumental supports like having a love relation with the opposite gender, reminding the time of taking the medicine by family members, or the spouse bringing the medicine for them will enhance their adherence to treatments, while lack of this support is a challenge for the patient and results in a decrease in adherence to treatment. Similar researches certify these findings.[27] HIV is not just a medical issue, but a social problem,[28] and due to the undeniable effect of social support in the patients following their treatments, there is a great need for adopting a policy by which along with informing the people about the ways through which this disease can be transferred, these patients can be treated like normal people in the society and are accepted by others. This way, families and society will not deprive them from their support. The motivation for living and, as a result, following treatment programs can be enhanced by creating and strengthening social networks for this group of patients.
Individuals’ contradictory beliefs are another important and effective factor that was extracted from the obtained results. False beliefs and images of treatment and self-evaluation are among the important concepts in this regard. Some of the patients believed that AIDS is not a serious disease and they can control it by taking medicine. They believed that normal people should be informed about this reality. Others stated that they think of AIDS as a monster that causes their death and this false belief, which is due to lack of enough knowledge about this disease, delays the treatment since they feel they are very close to death, but gradually they get some information and during interaction with peers, they conclude that they can extend their life span by using medicine. The results of other researches also confirm and emphasize the role of lack of knowledge and false beliefs in treatment adherence.[29] One of the facilitators of treatment adherence is individual's belief to the medicine's effectiveness for survival and enhancement of their health, while lack of this positive belief is an obstacle to treatment adherence.[22]
The present study also indicated that lack of adherence to treatments in some patients is due to their belief in traditional treatments and false beliefs about chemical treatments. On the other hand, appreciating one's health and believing in treatments as the correct way of living and the individual's will and determination for having a longer and healthier life have a great impact on some of the participants’ adherence to treatment and this is in line with the results of a study by Sidat et al.[30]
Individual and environmental barriers such as side effects of the medicines, poverty, and cultural environment of the prisons are among the existing obstacles for continuous use of the medicine and these were all emphasized in previous studies as well.[31,32,33] Nearly all the participants stated that experiencing the side effects of the medicine was one of the first reasons for stopping the use of medicines. Nausea, vomiting, stomach ache, delusion, dizziness, and headache are some of the side effects mentioned by the participants and this is also in line with previous researches.
Limitations
One of the limitations of this study was the fact that most of the HIV/AIDS patients were unwilling to take part in the interviews due to a fear of their disease being revealed and its consequences like stigma and being boycotted due to the country's cultural and religious environment. However, when the participants were assured that their data would be kept confidential in all stages of this research and that they were free to withdraw from the interviews whenever they decided not to continue, this limitation was resolved to some extent.
CONCLUSION
The results of this study indicated that adherence to treatment is not a one-dimensional and constant phenomenon, but a dynamic concept and is influenced by different variables. Hence, an individual who has a low adherence in a specific time and situation can show a desirable adherence in another time and under different circumstances. The results showed that adherence to HIV treatment in drug abusers is a function of different factors which can be precisely identified through digging the experiences of addicts under treatment for HIV. Drug abuse has a negative effect on the treatment of AIDS and usually the adherence to medical treatment is low among drug abusers. Use of the drugs disorganizes life and does not allow the users to have regular behaviors like using the medicine daily. Being affected by HIV infection, drug and drink abuse are chronic diseases which need a comprehensive and multidimensional approach for treatment. The constant adherence of the addicted HIV-positive patients to medical treatment is a complicated and multidimensional phenomenon, and a successful treatment, as the results of this study indicated, needs medical treatments along with physical, psychological, and social attention. First, because of the fact that addiction causes people not to care enough about their health, and second, because some addicts who are also living with HIV lose the family and society's support and this deprives them from the necessary assistance they need for caring and curing their HIV. Third, even when the treatment for HIV is presented free of charge, adherence to treatment involves others charges such as transportation, a better nutrition, doing tests and examinations, receiving extra treatments for their addiction, tuberculosis, hepatitis, and other costs, the provision of which is usually difficult for the addicted people. Merging different services as health and care services like methadone therapy, emotional health services, along with AIDS diet therapy can alleviate these problems and cause better therapeutic results. The participants of this study were addicted people referring to AIDS clinic for receiving treatment. It should be noted that HIV-positive addicts who can get medical treatments, but had not referred to therapeutic centers, were not included in the research due to lack of availability. No doubt, their reasons for not following treatments could enrich the findings of the present study; hence, it is recommended that in future studies, this group of patients is included in the research population.
Financial support and sponsorship
Tehran University of Medical Science.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The researcher would like to thank Tehran University of Medical Science for the financial support. The researcher also likes to acknowledge with gratitude the staffs of the Positive Fellowship Club and HIV patients.
REFERENCES
- 1.Cokerham W. Health as a social problem. In: Ritzer GO, editor. Handbook of Social Problem: A Comprehensive International Perspective. 1st ed. Thousand Oaks, CA: Sage Publication; 2004. pp. 271–315. [Google Scholar]
- 2.Weits R. Life with AIDS. In: Brown PH, editor. Perspective in Medical Sociology. 4th ed. Long Grove, Illinois: Waveland Press Inc; 2007. pp. 242–55. [Google Scholar]
- 3.WHO. Regional Office for the Eastern Mediterranean: HIV Surveillance in the WHO Eastern Mediterranean Region Regional Update 2012. [Last accessed on 2013 Dec 29]. Available from: http://www.applications.emro.who.int/dsaf/EMROPUB_2013_EN_1588 .
- 4.Ministry of Health and Medical Education, National AIDS Committee Secretariat, Islamic Republic of Iran. AIDS Progress Report, On Monitoring of the United Nations General Assembly Special Session on HIV and AIDS. March 2014. [Last accessed on 2014 Oct 05]. Available from: http://www.unaids.org/sites/defaulty/files/en/dataanalysis/knowyourresponse/countryprogressrepor .
- 5.Mills EJ, Bakanda C, Birungi J, Chan K, Ford N, Cooper CL, et al. Life expectancy of persons receiving combination antiretroviral therapy in low-income countries: A cohort analysis from Uganda. Ann Intern Med. 2011;155:209–16. doi: 10.7326/0003-4819-155-4-201108160-00358. [DOI] [PubMed] [Google Scholar]
- 6.Mills EJ, Nachega JB, Buchan I, Orbinski J, Attaran A, Singh S, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: A meta-analysis. JAMA. 2006;296:679–90. doi: 10.1001/jama.296.6.679. [DOI] [PubMed] [Google Scholar]
- 7.Nabukeera-Barungi N, Kalyesubula I, Kekitiinwa A, Byakika-Tusiime J, Musoke P. Adherence to antiretroviral therapy in children attending Mulago Hospital, Kampala. Ann Trop Paediatr. 2007;27:123–31. doi: 10.1179/146532807X192499. [DOI] [PubMed] [Google Scholar]
- 8.Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected adults and adolescents. Washington, DC: [Last accessed on 2014 Oct 15]. Department of Health and Human Services. Available from: http://aidsinfo.nih.gov/guideline.August 2012 . [Google Scholar]
- 9.Yalda A, Seyyed Alinaghi S A, Hajiabdolbaghi M. Adherence to antiretroviral therapy and its determinants in AIDS patients: Review article. Tehran Univ Med J. 2008;66:447–5. [Google Scholar]
- 10.Nijhawan A, Kim S, Rich JD. Management of HIV infection in patients with substance use problems. Curr Infect Dis Rep. 2008;10:432–8. doi: 10.1007/s11908-008-0068-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hinkin CH, Barclay TR, Castellon SA, Levine AJ, Durvasula RS, Marion SD, et al. Drug use and medication adherence among HIV-1 infected individuals. AIDS Behav. 2007;11:185–94. doi: 10.1007/s10461-006-9152-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Crisp BR, Williams M, Timpson S, Ross MW. Medication compliance and satisfaction with treatment for HIV disease in a sample of African-American crack cocaine smokers. AIDS Behav. 2004;8:199–206. doi: 10.1023/B:AIBE.0000030250.33931.af. [DOI] [PubMed] [Google Scholar]
- 13.Golafshani N. Understanding reliability and validity in qualitative research. Qual Rep. 2003;8:597–607. [Google Scholar]
- 14.UNESCO. Akpaka O: Qualitative research on Education and HIV/AIDS, Module. [Last accessed on 2015 Nov 18]. Available from: http://www.iiep.unesco.org/fileadmin/user_upload/cap_dev-training/
- 15.Curioso WH, Kepka D, Cabello R, Segura P, Kurth AE. Understanding the facilitators and barriers of antiretroviral adherence in Peru: A qualitative study. BMC Public Health. 2010;10:13. doi: 10.1186/1471-2458-10-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Remien RH, Hirky AE, Johnson MO, Weinhardt LS, Whittier D, Le GM. Adherence to medication treatment: A qualitative study of facilitators and barriers among a diverse sample of HIV+men and women in four U.S. cities. AIDS Behav. 2003;7:61–72. doi: 10.1023/a:1022513507669. [DOI] [PubMed] [Google Scholar]
- 17.Graneheim UH, Lundman B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105–12. doi: 10.1016/j.nedt.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 18.Tate D, Paul RH, Flanigan TP, Tashima K, Nash J, Adair C, et al. The impact of apathy and depression on quality of life in patients infected with HIV. AIDS Patient Care STDS. 2003;17:115–20. doi: 10.1089/108729103763807936. [DOI] [PubMed] [Google Scholar]
- 19.Rao D, Chen WT, Pearson CR, Simoni JM, Fredriksen-Goldsen K, Nelson K, et al. Social support mediates the relationship between HIV stigma and depression/quality of life among people living with HIV in Beijing, China. Int J STD AIDS. 2012;23:481–4. doi: 10.1258/ijsa.2009.009428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Safren SA, O’Cleirigh CM, Bullis JR, Otto MW, Stein MD, Pollack MH. Cognitive behavioral therapy for adherence and depression (CBT-AD) in HIV-infected injection drug users: A randomized controlled trial. J Consult Clin Psychol. 2012;80:404–15. doi: 10.1037/a0028208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Valent SM. Depression and HIV Disease. J Assoc Nurses AIDS Care. 2003;14:41–51. doi: 10.1177/1055329002250993. [DOI] [PubMed] [Google Scholar]
- 22.Jaquet A, Ekouevi DK, Bashi J, Aboubakrine M, Messou E, Maiga M, et al. Alcohol use and non-adherence to antiretroviral therapy in HIV-infected patients in West Africa. Addiction. 2010;105:1416–21. doi: 10.1111/j.1360-0443.2010.02978.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Capaldini L, Harison G. Overcoming depression. BETA. 2004;16:18–25. [PubMed] [Google Scholar]
- 24.Hardling R, Molloy T, Easterbrook P, Frame K, Higginson L. Is antiretroviral therapy associated with symptom prevalence and burden? Int J STD AIDS. 2006;17:400–5. doi: 10.1258/095646206777323409. [DOI] [PubMed] [Google Scholar]
- 25.Salgi Z, Hashemiyan K, Saeidi Poor B. The effect of group cognitive therapy to reduce depression in HIV positive patients. Psych Stud J. 2007;3:105–22. [Google Scholar]
- 26.Catalan J, Harding R, Sibley E, Clucas C, Croome N, Sherr L. HIV infection and mental health: Suicidal behaviour--systematic review. Psychol Health Med. 2011;16:588–611. doi: 10.1080/13548506.2011.582125. [DOI] [PubMed] [Google Scholar]
- 27.Woodward EN, Pantalone DW. The role of social support and negative affect in medication adherence for HIV-infected men who have sex with men. J Assoc Nurses AIDS Care. 2012;23:388–96. doi: 10.1016/j.jana.2011.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mawar N, Saha S, Pandit A, Mahajan U. The third phase of HIV pandemic: Social consequences of HIV/AIDS stigma and discrimination and future needs. Indian J Med Res. 2005;122:471–84. [PubMed] [Google Scholar]
- 29.Murphy DA, Belzer M, Durako SJ, Sarr M, Wilson CM, Muenz LR Adolescent Medicine HIV/AIDS Research Network. Longitudinal antiretroviral adherence among adolescents infected with human immunodeficiency virus. Arch Pediatr Adolesc Med. 2005;159:764–70. doi: 10.1001/archpedi.159.8.764. [DOI] [PubMed] [Google Scholar]
- 30.Sidat M, Fairley C, Grierson J. Experiences and perceptions of patients with 100% adherence to highly active antiretroviral therapy: A Qualitative study. AIDS Patient Care STDS. 2007;21:509–20. doi: 10.1089/apc.2006.0201. [DOI] [PubMed] [Google Scholar]
- 31.Eholié SP, Tanon A, Polneau S, Ouiminga M, Djadji A, Kangah- Koffi C, et al. Field adherence to highly active antiretroviral therapy in HIV-infected adults in Abidjan, Côte d’Ivoire. J Acquir Immune Defic Syndr. 2007;45:355–8. doi: 10.1097/QAI.0b013e31805d8ad0. [DOI] [PubMed] [Google Scholar]
- 32.Palepu A, Tyndall MW, Chan K, Wood E, Montaner JS, Hogg RS. Initiating highly active antiretroviral therapy and continuity of HIV care: The impact of incarceration and prison release on adherence and HIV treatment outcomes. Antivir Ther. 2004;9:713–9. [PubMed] [Google Scholar]
- 33.Yuan Y, L’italien G, Mukherjee J, IIoeje UH. Determinants of discontinuation of initial highly active antiretroviral therapy regimens in a US HIV-infected patient cohort. HIV Med. 2006;7:156–62. doi: 10.1111/j.1468-1293.2006.00355.x. [DOI] [PubMed] [Google Scholar]