

Abstract
Background:
Waste management is a necessary activity around the world, but involves a variety of health hazards. In a developing country like India, municipal solid waste is collected manually requiring heavy physical activity. Among all occupational health issues, musculoskeletal problems are common among waste collectors in the form of nonfatal injuries because of the presence of such risk factors (lifting, carrying, pulling, and pushing). We have thus conducted this study to evaluate musculoskeletal disorders (MSDs) among municipal solid waste (MSW) workers.
Methodology:
A cross-sectional study using probability proportionate to size sampling, recruited 220 MSW workers from the Chennai Municipal Corporation, India for this study. A pretested validated questionnaire has been used to collect data on demographic and occupational history and information on musculoskeletal pain. Data analysis was performed using R software (3.0.1 version).
Results:
70% of the participants reported that they had been troubled with musculoskeletal pain in one or more of the 9 defined body regions during the last 12 months, whereas 91.8% had pain during the last 7 days. Higher prevalence of symptoms in knees, shoulders, and lower back was found to be 84.5%, 74.5%, and 50.9% respectively. Female illiterate workers with lower socioeconomic status were found to have higher odds for MSDs. Similarly, higher body mass index having no physical activity increases the chance of odds having MSDs.
Conclusion:
The higher percentage of musculoskeletal symptoms among MSW workers could be attributed to the long duration of employment, the low job control, and the nature of their job, which is physically demanding. A workplace of health promotion model integration can minimize the reported high prevalence, and a prospective cohort study could be recommended further.
Keywords: Municipal solid waste, musculoskeletal disorders, risk assessment
Introduction
Solid waste management encompasses a wide range of activities, including collecting garbage, collecting and sorting recyclable materials and collecting and processing of commercial and industrial waste.[1] Risks occur at every step in the process, from the point of the collection at homes, during transportation and at the sites of recycling or disposal.[2] Municipal solid waste (MSW) workers are at risk for a variety of occupational diseases as a result of daily exposure to work-related hazards.[3] In many developing countries, MSW is collected manually, and collection of household waste is also a job which requires repeated heavy physical activity.[4] The socioeconomic status of waste workers is low and their working conditions are unfavorable.[5] For waste collectors, the risk of disease resulting from exposure to various work hazards is high.[6,7,8] as well as the risk of fatal and nonfatal occupational accidents.[9] Musculoskeletal problems are also common among waste collectors[10,11] and in this work group nonfatal injuries are mainly musculoskeletal.[3]
Musculoskeletal disorders (MSDs) are an important public health problem in both developed and developing countries, with substantial impact on the quality of life as well as a substantial economic burden in compensation costs, lost wages, and productivity.[12,13] MSDs contribute to absenteeism, increased work restriction, transfer to other jobs, or disability more than any other group of diseases with a considerable economic toll on the individual, the organization, and the society as a whole.[14,15,16] Moreover, MSDs are the most expensive form of work disability.[17,18] As far as India is concerned, MSD is one of the major occupational health problems. Estimates have shown that MSD contributes to about 40% of all costs toward the treatment of work-related injuries.[19,20] The health of this highly exposed and vulnerable groups is really a huge concern.[21] Workplace activities such as heavy lifting, manual handling, prolonged sitting and standing, bending, and other repetitive tasks are known as risk factors for MSDs.[22] In India, like many developing countries, MSW is collected manually, and a collection of household waste is also a job, which requires repeated heavy physical activity such as lifting, carrying, pulling, and pushing.[4] Although MSDs represent a significant occupational issue for MSW workers worldwide, there is a dearth of evidence found from the literature review. In developing countries like India, there has been little study on the health and incidence of MSDs among solid waste workers. Most of the reviewed studies suffer from limitations related to poor exposure assessment and lack of information on relevant confounders.[23]
Considering this fact and focusing on the Indian context, this study was aimed to determine the prevalence of musculoskeletal symptoms in varied groups of MSW workers and its predictors in Chennai City, India.
Methodology
The present cross-sectional study was carried out among MSW workers of Chennai, which is capital city of the Tamil Nadu, a Southern Indian State. Chennai is the fifth largest city and fourth most populous metropolitan area in the country and 31st largest urban area in the world having a population of 4.7 million.[24] Every day, 4500 MT of garbage is collected and removed from the city, with a per capita generation per day of about 700 g. Door to door collection of garbage is prescribed in all zones.[25] More than 10,000 workers are engaged in this solid waste management in this city. The sample for this study was selected randomly from the employee roster of the municipal registry, Chennai City. Using probability proportionate to sample, three zones of Chennai were identified for the desired sample size of 220 workers (collectors, transporters, segregators and disposers, and rag pickers), for the study purpose. Permission was obtained from the project manager of private companies handling solid waste operations in Chennai City under the Chennai Municipal Corporation. A pretested validated questionnaire through pilot testing has been used to collect the data on demographic and occupational history. Anthropometric measurements were done using the standardized scale, for assessing the physical status. A globally validated tool called Nordic Musculoskeletal Questionnaire[26] used to collect the information on musculoskeletal pain.
The study proposal was approved by the University Institutional Ethics Committee (Reference: CSP/13/Jan/26/17 of Sri Ramachandra University, Chennai, India) prior to the data collection. The study participants were informed about the study, its objective, and benefits. A written informed consent was obtained from all of the participants who were willing to be involved in the study, before administering the questionnaire.
The descriptive analysis in the form of the mean with standard deviation or percentage was conducted for demographic variables and occupational information. Test of significance such as independent “t-test” and Chi-square tests were used for comparison and are shown with P values, considering the level of significance at P < 0.05. Data analysis was performed using R software (3.0.1 version, University of Auckland, New Zealand).[27]
Results
The mean age, height, weight, and body mass index (BMI) of all MSWs were 36.9 ± 10.1 years, 160 ± 9.7 cm, 57.1 ± 11.7 kg, and 22.2 ± 3.8, respectively. The total years of work experience was found to be 12.1 ± 7.5 years, and all were working for 8 h in a single shift.
This study population contains 59.5% male and 40.56% female with 105 (48%) being young adults (<35 years). More than one-third (39%) of the sample have no formal education, whereas only 14% went to high school or more. Approximately 65% of waste workers had <5 years of experience, whereas 75% were found to be unskilled in waste management. It has been found that, 24.5% participants were smokers and 20.5% were alcoholics in this study. But around 40% of waste workers were habituated to paan, or gutka, or any form of tobacco chewing The anthropometric measurement indicates that 63% workers had normal BMI (18.5–24.9 kg/m2), whereas only 21% were obese or overweight. Of all workers, 70% reported one body part as having musculoskeletal pain during the last year. The details of workers with sub-categories are shown in Table 1. It describes the differences between the “subgroups of MSWs” for all demographic and occupational history variables. Except for personal habits, employment duration, and MSD pain, all other variables found to be statistically significant among sub groups.
Table 1.
Descriptive statistics of MSWs with groups
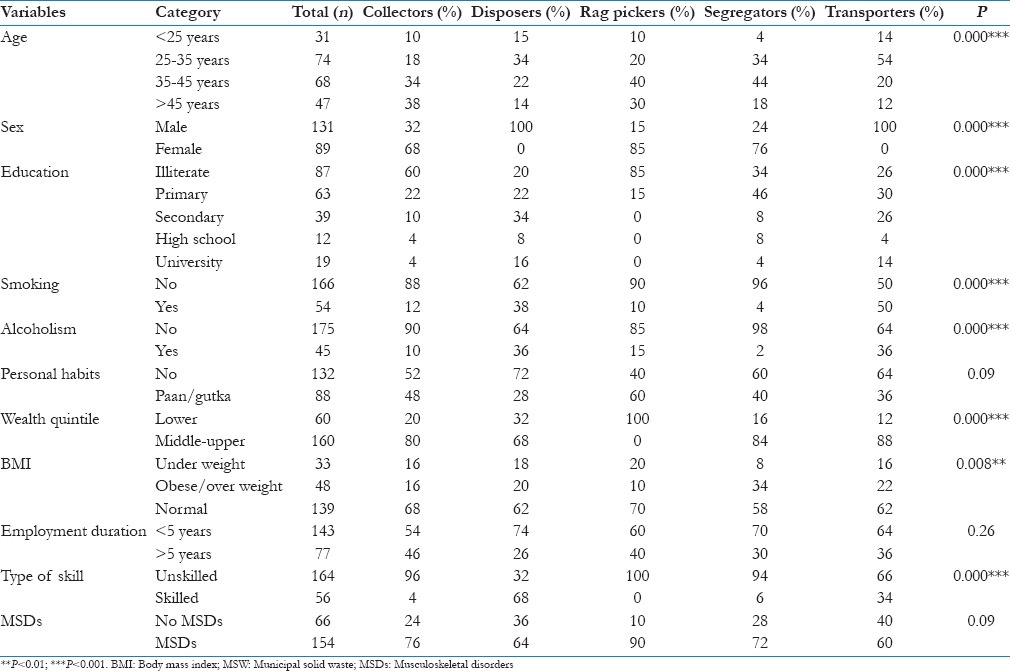
Figure 1 demonstrates the prevalence of musculoskeletal pain among all theMSW workers. Their period prevalence was asked for the past year, and the point prevalence was asked for the last 7 days concerning pain in any body part, which was self-reported by the participants. The period prevalence, that is, last 12 months, any body region pain was reported as 70%, whereas point prevalence, that is, last 7 days any body region found to be 91.8%.Among all the body parts, knee pain was found to be the highest (point = 84.5%, period = 60%) followed by shoulder joint (point = 74.5%, period = 38.6%). Low back pain and wrist joint were next to above as the manual handling involves these two majorly. Other peripheral joints such as elbow, hip, and ankle were in negligible proportion.
Figure 1.
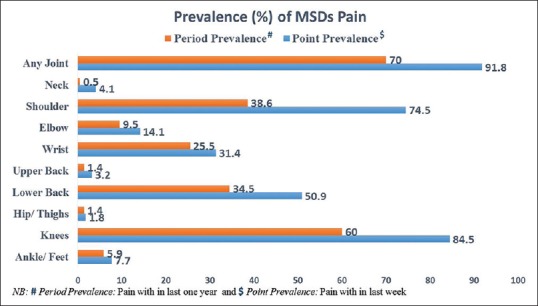
Prevalence of musculoskeletal disorders among municipal solid wastes
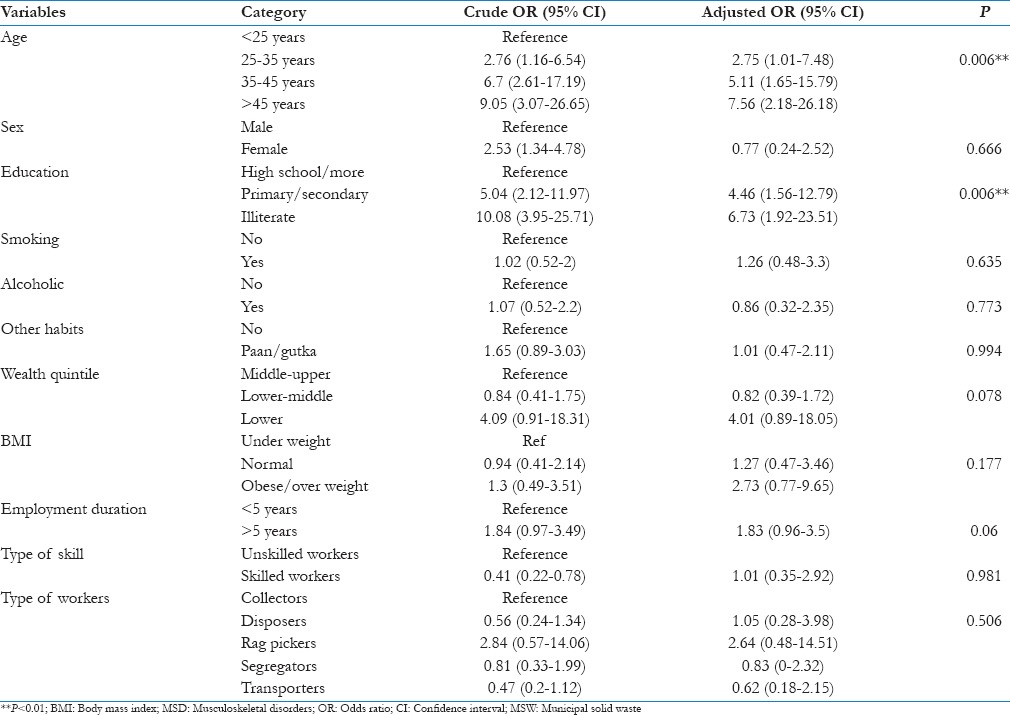
The logistic regression model as shown in Table 2, that age increases the chance of getting MSDs as odds increases from odds ratio (OR) =2.75 (25–35 years) to OR = 7.56 (>45 years). The odds of females having MSDs is 2.53 times that of males, within the study population. However, it loses its significance in the model as adjusted OR is found to be 0.77. It is obvious that those who have less education[5] (OR = 6.73) and lower wealth quintile (OR = 4.01) are at greater chance for MSDs as they are mostly poor; and lack knowledge of using an ideal posture while working. Personal habits such as smoking (OR = 1.26) or tobacco chewing (OR = 1.01) were found to have some effect of MSDs development. We suspect that obese or overweight people would have a greater chance of MSDs as the level of physical activity decreases among them. This study found that as the BMI increases (OR = 2.73), the occurrence of MSDs also increases from 1.27 to 2.73 times. Among all sub-categories, the rag pickers (OR = 2.64) were found to be the most vulnerable group to develop MSDs, followed by disposers (OR = 1.05).
Table 2.
Regression model for predictors of MSDs among MSWs
Discussion
This study has generated the baseline MSD profile of the MSW workers working under the private agencies in Chennai City. This study has presented a 100% of response rate, and this is superior to previous questionnaire studies on this topic such as 70% in Hussain[28] and 80% in Smith et al.[29] In this group of MSW workers, most of them reported knee complaint in one or more parts of the body in the last 12 months. Previous studies using the Nordic Questionnaire in a variety of jobs have reported 1 year prevalence rates of musculoskeletal symptoms.[16]
The results of the present study showed that a high percentage of musculoskeletal complaints (90.8%) were detected among MSW collectors, and the knee (84.5%) was the most frequently affected body region. High prevalence of MSDs among waste collectors was reported also in studies of Brazil,[30] Denmark,[31] Taiwan,[4] USA,[32] and The Netherlands.[33] The independent risk factors for musculoskeletal symptoms among MSW collectors were the duration of employment; lifting, pulling; pushing/carrying loads >20/kg, and walking for long periods of time. The differences in the distribution of musculoskeletal complaints in between different types of MSW collectors were statistically not significant but shown higher in the rag pickers group.
In Egypt, collectors suffer from MSDs because of the large volume of waste they have to pack manually. Ergonomic risk factors might be a contributing factor. The illiterate collectors may be unaware of the proper safety techniques during waste collection. In Palestine, 45.7% of surveyed waste collectors have suffered from backache, 34.1% of waste collectors have suffered from twisted ankle, 22.1% have suffered from muscle tear, and 8.7% have suffered from joint pain.[34] These findings differ from the current study; as in India several municipalities are transforming waste collection management services from a public-private partnerships model and they engage temporary workers informally;[35] as in the current study larger population have <5 years of work experience. In Nigeria, 171 workers representing 61.3% of the sampled solid waste collectors had suffered from musculoskeletal injuries on the job. Solid waste collectors in Port Harcourt municipality suffered from musculoskeletal injuries because of the large volume of waste they have to pack manually in contrast to the use of hydraulic lifts.[36] In Iran, the prevalence of musculoskeletal symptoms, among MSW workers in Tehran, in low back, knees, shoulders, upper back, and neck were 45%, 29%, 24%, 23%, and 22%, respectively. The study found that solid waste workers had more MSDs than the general population. The risk of disease increased with increasing years of work as a solid waste worker and smoking. There was no relationship between MSDs and education or marriage status of workers.[5] Whereas the current study indicates that illiterate, adult female workers have higher odds for development of MSDs. Habits such as smoking or alcoholic have less influence on MSDs status; on the other hand, a local tobacco chewing, that is, paan/gutka was found to be a contributing factor for MSD pain.[5] Lower wealth quintiles population of MSWs were found to exhibit higher odds for the MSDs (OR = 4.01).
In many developing countries, MSW is collected manually and collection of household waste is also a job, which requires repeated heavy physical activity such as lifting, carrying, pulling, and pushing.[4] This study also suggests that MSW workers were mostly engaged in manual handling tasks for waste collection. Though the workers were found to be highly experienced, they have little knowledge about health hazards at their workplace; an integrated screening of workplace hazards[37] and awareness might help to prevent further development of MSDs among this high risk group.
Limitations
The study failed to evaluate non-occupational risk factors for musculoskeletal pains. The nonwork-related risk factors have not been studied explored extensively in this study as well as the musculoskeletal pain was self-reported not the medical diagnosis or confirmatory MSDs. This is a single-center study that included a small number of MSW collectors; Because of which, the results cannot be generalized to the total population of MSW collectors.
Conclusion
MSW collectors are among the most highly exposed occupational groups with respect to MSDs. The higher percentage of musculoskeletal symptoms among MSW workers could be attributed to the long duration of employment, the low job control, and the nature of their job, which is physically demanding and involves lifting, pulling, pushing heavy loads, and frequent bending and twisting activities, and walking for long distances in their task profile. Also the less educated (illiterate or having less than primary education) collectors seem to be less aware of the potential hazards and health impacts related to the collection methods. The unfavorable working conditions of MSW collectors could be ameliorated through engineering, medical, and legislative measures as well as a proper workplace health promotion model intervention. As education was found to be highly significant in contributing a factor of MSDs, an integrated health education consisting of ergonomics and healthy work habits needs to be incorporated in a prehealth screening program. In addition, a routine workplace health promotion model needs to be activated for the welfare of these undermarginalized population.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We are thankful to the participants of the study who gave us unconditional support and NMQ team to permit us for using the scale in this study.
References
- 1.Cointreau-Levine S, Listorti J, Furedy C. Solid waste. In: Herzstein JA, Bunn WB, Fleming LE, Harrington JM, Jeyaratnam J, Gardner IR, editors. International Occupational and Environmental Medicine. 1st ed. St. Louis: Mosby; 1998. p. 62032. [Google Scholar]
- 2.Cointreau-Levine S. Washington DC: World Bank Group, Urban Sector Board; 2006. [Last cited on 2012 Aug 01]. Occupational and Environmental Health Issues of Solid Waste Management. Special Emphasis on Middleand LowerIncome Countries Urban Papers. Available from: http://www worldbank.org/INTUSWM/Resources/up2.pdf . [Google Scholar]
- 3.Dorevitch S, Marder D. Occupational hazards of municipal solid waste workers. Occup Med. 2001;16:125–33. [PubMed] [Google Scholar]
- 4.Yang CY, Chang WT, Chuang HY, Tsai SS, Wu TN, Sung FC. Adverse health effects among household waste collectors in Taiwan. Environ Res. 2001;85:195–9. doi: 10.1006/enrs.2000.4235. [DOI] [PubMed] [Google Scholar]
- 5.Mehrdad R, Majlessi-Nasr M, Aminian O, Sharifian SA, Malekahmadi F. Musculoskeletal disorders among municipal solid waste workers. Acta Med Iran. 2008;46:233–8. [Google Scholar]
- 6.Kuijer P, Frings-Dresen M, de Looze M, Visserb B, Beeka AV. Work situation and physical workload of refuse collectors in three different time periods. Int J Ind Ergon. 2000;26:509–19. [Google Scholar]
- 7.Schibye B, Søgaard K, Martinsen D, Klausen K. Mechanical load on the low back and shoulders during pushing and pulling of two-wheeled waste containers compared with lifting and carrying of bags and bins. Clin Biomech (Bristol, Avon) 2001;16:549–59. doi: 10.1016/s0268-0033(01)00039-0. [DOI] [PubMed] [Google Scholar]
- 8.Wouters IM, Hilhorst SK, Kleppe P, Doekes G, Douwes J, Peretz C, et al. Upper airway inflammation and respiratory symptoms in domestic waste collectors. Occup Environ Med. 2002;59:106–12. doi: 10.1136/oem.59.2.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kuijer PP, Frings-Dresen MH. World at work: Refuse collectors. Occup Environ Med. 2004;61:282–6. doi: 10.1136/oem.2002.001172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rogers B. Municipal healthcare workers: Work-related health hazards. Occup Med. 2001;16:143–61. [PubMed] [Google Scholar]
- 11.Poulsen OM, Breum NO, Ebbehøj N, Hansen AM, Ivens UI, van Lelieveld D, et al. Collection of domestic waste. Review of occupational health problems and their possible causes. Sci Total Environ. 1995;170:1–19. doi: 10.1016/0048-9697(95)04524-5. [DOI] [PubMed] [Google Scholar]
- 12.Yelin EH, Felts WR. A summary of the impact of musculoskeletal conditions in the United States. Arthritis Rheum. 1990;33:750–5. doi: 10.1002/art.1780330520. [DOI] [PubMed] [Google Scholar]
- 13.Karwowski W, Marras WS. Florida: CRC Press; 2003. Occupational Ergonomics: Principles of Work Design. [Google Scholar]
- 14.Badley EM, Rasooly I, Webster GK. Relative importance of musculoskeletal disorders as a cause of chronic health problems, disability, and health care utilization: Findings from the 1990 Ontario Health Survey. J Rheumatol. 1994;21:505–14. [PubMed] [Google Scholar]
- 15.Riihimäki H. Hands up or back to work – Future challenges in epidemiologic research on musculoskeletal diseases. Scand J Work Environ Health. 1995;21:401–3. doi: 10.5271/sjweh.54. [DOI] [PubMed] [Google Scholar]
- 16.Leijon M, Hensing G, Alexanderson K. Gender trends in sick-listing with musculoskeletal symptoms in a Swedish county during a period of rapid increase in sickness absence. Scand J Soc Med. 1998;26:204–13. doi: 10.1177/14034948980260031101. [DOI] [PubMed] [Google Scholar]
- 17.European Agency for Safety and Health at Work. Work-related Neck and Upper Limb Musculoskeletal Disorders, 1999. National Research Council. Musculoskeletal Disorders and the Workplace. 2001 [Google Scholar]
- 18.Occupational Health and Safety Act. [Last assessed on 2012 Dec 12]. Available from: http://www.elaws.gov.on.ca/html/statutes/english/elaws_statutes_90o01_e.htm .
- 19.European Agency for Safety and Health at Work Fact Sheet. [Last assessed on 2012 Dec 12]. Available from: http://osha.europa.eu .
- 20.Yasobant S, Rajkumar P. Health of the healthcare professionals: A risk assessment study on work-related musculoskeletal disorders in a tertiary hospital, Chennai, India. Int J Med Public Health. 2015;5:189–95. [Google Scholar]
- 21.Sigsgaard T. Health hazards to waste management workers in Denmark. Schriftenr Ver Wasser Boden Lufthyg. 1999;104:563–8. [PubMed] [Google Scholar]
- 22.Yasobant S, Rajkumar P. Work-related musculoskeletal disorders among health care professionals: A cross-sectional assessment of risk factors in a tertiary hospital, India. Indian J Occup Environ Med. 2014;18:75–81. doi: 10.4103/0019-5278.146896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Porta D, Milani S, Lazzarino AI, Perucci CA, Forastiere F. Systematic review of epidemiological studies on health effects associated with management of solid waste. [Last cited on 2012 Aug 20];Environ Health. 2009 8:60. doi: 10.1186/1476-069X-8-60. Available from: http://www.ehjournal.net/content/8/1/60 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Registrar General India. Government of India Census. [Last accessed on 2012 Dec 12]. Available from: http://www.census2011.co.in/census/district/21-chennai.html .
- 25.Corporation of Chennai. Department of Solid Waste Management. [Last accessed on 2012 Dec 12]. Available from: http://www.chennaicorporation.gov.in/departments/solid-waste-management/index.htm .
- 26.Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardized Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18:233–7. doi: 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- 27.R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. Vienna, Austria. 2013. [Last accessed on 2011 Sep 10]. Available from: http://www.R.project.org/
- 28.Hussain T. Musculoskeletal symptoms among truck assembly workers. Occup Med (Lond) 2004;54:506–12. doi: 10.1093/occmed/kqh087. [DOI] [PubMed] [Google Scholar]
- 29.Smith DR, Sato M, Miyajima T, Mizutani T, Yamagata Z. Musculoskeletal disorders self-reported by female nursing students in central Japan: A complete cross-sectional survey. Int J Nurs Stud. 2003;40:725–9. doi: 10.1016/s0020-7489(03)00012-9. [DOI] [PubMed] [Google Scholar]
- 30.Robazzi ML, Moriya TM, Favero M, Lavrador MA, Luis MA. Garbage collectors: Occupational accidents and coefficients of frequency and severity per accident. Ann Agric Environ Med. 1997;4:91–6. [Google Scholar]
- 31.Ivens UI, Lassen JH, Kaltoft BS, Skov T. Injuries among domestic waste collectors. Am J Ind Med. 1998;33:182–9. doi: 10.1002/(sici)1097-0274(199802)33:2<182::aid-ajim10>3.0.co;2-x. [DOI] [PubMed] [Google Scholar]
- 32.An H, Englehardt J, Fleming L, Bean J. Occupational health and safety amongst municipal solid waste workers in Florida. Waste Manag Res. 1999;17:369–77. [Google Scholar]
- 33.Kuijer PP, Frings-Dresen MH. World at work: Refuse collectors. Occup Environ Med. 2004;61:282–6. doi: 10.1136/oem.2002.001172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Milhem A. Investigation of Occupational Health and Safety Hazards Among Domestic Waste Collectors in Bethlehem and Hebron Districts. MSc Thesis, Environmental Science, Faculty of Graduate Studies, at An-Najah National University, Nablus, Palestine. 2004 [Google Scholar]
- 35.Department of Economic Affairs Ministry of Finance Government of India. Position Paper on the Solid Waste Management Sector in India, November. 2009. [Last accessed on 2012 Sep 11]. Available from: http://www.pppinindia.com/pdf/ppp_position_paper_solid_waste_mgmt_112k9.pdf .
- 36.Inyang M. Health and Safety Risks Amongst the Municipal Solid Waste Collectors in Port Harcourt Metropolis of the Niger Delta Region of Nigeria. International Conference “Waste Management, Environmental Geotechnology and Global Sustainable Development (Icwmeggsd’07-Gzo’07)” Ljubljana, Slovenia, August 28-30. 2007 [Google Scholar]
- 37.Yasobant S. Ergo-HIRA: A conceptual model for fitness to work. Indian J Res. 2014;3:148–9. [Google Scholar]