

Abstract
This review deals with the role of microorganisms in spontaneous regression of a tumour. Spontaneous cancer regression is a phenomenon that has been described for many centuries. One of the most well known methods of inducing spontaneous regression of cancer is the application of Coley’s toxin (heat-killed Streptococcus pyogenes and Serratia marcescens), which has been used for the successful treatment of sarcomas, carcinomas, lymphomas, myelomas and melanomas. In clinical practice, the use of Bacillus Calmette-Guérin vaccine for the treatment of superficial urinary bladder cancer is the most common instance of the application of microorganisms for the treatment of cancer. This review provides further information on other tested bacteria – Clostridium spp., Bifidobacterium spp., Lactobacillus spp. and Salmonella spp. – in this field of study. Among new age methods, bactofection, alternative gene therapy, combination bacteriolytic therapy and bacteria-directed enzyme prodrug therapy are some of the potential cancer treatment modalities that use microorganisms. We have also provided information about the interconnection among microorganisms, immune system response, and the possible mechanisms involved in the spontaneous regression of tumours.
Keywords: Bacillus Calmette-Guérin vaccine, cancer, Clostridium spp., Coley’s toxin, microorganisms, spontaneous regression, treatment
Introduction
Cancer causes 12% of all deaths worldwide and is the most common cause of death in developed countries. Annually, more than 12 million patients are newly diagnosed with cancer and seven million deaths are registered 1,2. It is estimated that this number could increase and reach 15 million by 2020 2.
Substantial progress has been made in the treatment of cancer over the past century. However, some types of tumours are still difficult to treat 3. Conventional methods of carcinoma treatment such as chemotherapy and radiotherapy pose a big burden for the patient because of the wide range of side effects. In addition, the disease relapses in several patients despite these therapies 1. For this reason, efforts are ongoing to establish a treatment that would eliminate these undesirable outcomes 3. New therapies are trying to target only the affected tissue using live, attenuated or genetically modified microorganisms, which could serve as an ideal tool for the stimulation of the immune system 1,3,4.
Spontaneous regression of cancer is not a new phenomenon. Spontaneous healing of cancer patients has been described in the literature over the past several centuries, even millennia 2,5. It is defined as partial or complete disappearance of a malignant tumour or a decrease in proliferation of the cancer in the tissue of a patient that can be demonstrated by microscopic examination. However, to qualify as spontaneous regression, this phenomenon must occur in the absence of any medical treatment and without other obvious causes. Spontaneous regression is seen in the majority of cancers; it is frequently described in the following groups of tumours: embryonal and breast cancer, renal adenocarcinoma, neuroblastoma, melanoma and sarcoma or carcinoma of the urinary bladder 2,6. This phenomenon is often associated with bacterial, fungal, viral or protozoan infection, or vaccination therapy. The most commonly reported symptom wherein spontaneous regression is subsequently registered is an acute febrile state that is evoked by either natural or induced acute infection 6,7.
Historical aspects of spontaneous regression of tumour
As mentioned above, the origin of cancer therapy, associated with spontaneous regression, can be traced back to the time when people did not have any idea about the existence of microorganisms or their potential therapeutic effects in the treatment of tumours.
The first evidence for treatment for cancer comprising microorganisms was seen in the Iberian papyrus (1550 BC). The Egyptian pharaoh Imhotep (2600 BC) used poultice, followed by incision, for the treatment of tumour. This would facilitate the development of infection in the desired location and would cause regression of the tumour. During the 17th and 18th centuries, various forms of immunotherapy in cancer became widespread 2,6,8.
The phenomenon of spontaneous regression is also well-known as St. Peregrine tumour. Peregrine Laziozi was afflicted by cancer of the tibia that required a leg amputation. The tumour progressed until the skin was impaired and the tumour was seriously infected. Subsequently, to the astonishment of the physician, the tumour was no longer present. The relapse of cancer was not observed 2,8.
In the 18th and 19th centuries, septic dressings enclosing ulcerative tumours were used for the treatment of cancer. Surgical wounds were left open to facilitate the development of infection, and purulent sores were created deliberately 9.
In 1813, Vautier reported regression of cancer in patients with gangrene, and in such individuals, the tumour was found to be infected with Clostridium spp. Later, it was shown that the causative agent was the bacterium, Clostridium perfringens 10,11.
Another important mention concerning the interconnection between infectious diseases and spontaneous regression of cancer is Dupuytren’s publication in 1829. It describes the case of a woman with progressive breast cancer who refused surgery. Eighteen months later, the health status of the woman worsened significantly, and she was bedridden, cachectic, and almost moribund. Febrile illness and vomiting followed closely and the tumour was inflamed and gangrenous. Three incisions were made by the physician into the tumour to remove a large amount of viscous fluid. Within 8 days, the cancer had regressed to a third of its original size. Within 4 weeks, no clinical symptom of the tumour was present 9.
Busch in the year 1868 was treating a patient with incurable cancer. After the first cauterization of the tumour on her neck, he assigned the patient the bed next to another patient suffering from an infectious skin disease, erysipelas [causative agent Streptococcus (Str.) pyogenes]. The woman with the tumour became ill with Streptococcus spp. infection, and subsequently rapid tumour regression was observed. The same idea was also proposed by Fehleisen in 1882 4,10.
One of the most well-known effects of microorganisms on the spontaneous regression of cancer was reported in 1891, when an American surgeon, William B. Coley, inoculated patients having inoperable tumours with Str. pyogenes. Unfortunately, the results were not as effective as expected, and a wide range of side effects were observed 10. Despite this limitation, 51.9% of the patients with inoperable soft-tissue sarcomas showed complete tumour regression and survived for more than 5 years, and 21.2% of the patients had no clinical evidence of tumour at least 20 years after this treatment 5. To eliminate these side effects, Coley developed a toxin that contained heat-killed bacteria, Str. pyogenes and Serratia (Ser.) marcescens. Until 1963, this treatment was used for the treatment of sarcomas 2,10. We have dedicated a whole section of this review to the usage of Coley’s toxin.
The most promising clinical application of microbial agents in the treatment of cancer was discovered in 1976, when Morales, Eidinger and Bruce published on the successful treatment of superficial urinary bladder cancer after inoculation with Bacillus Calmette-Guérin (BCG) vaccine, which is the standard vaccine against tuberculosis. Today, this therapeutic approach has become the method of choice for high-risk urinary bladder tumours 10,12.
Microorganisms and spontaneous regression of tumour
As mentioned above, the role of microorganisms in spontaneous regression of malignancy has been known and studied for a long time. Scientists have tried to define the criteria that allow a microorganism to become an ‘ideal’ tool for cancer therapy.
These criteria are as follows: it should be nontoxic to the host, it should replicate only in the tumour and it should be mobile and capable of spreading the cancer (in hypoxic and necrotic regions). In addition, it should be slowly and completely removable from the macroorganism, it should be nonimmunogenic and it should be capable of lysing tumour cells 13.
Coley’s toxin
More than 100 years ago, in 1891, an American surgeon William B. Coley observed that application of suitable microorganisms could significantly affect subsequent tumour progression 3,14,15. Cancer patients were treated by injection with the so-called Coley’s toxin, which contained heat-killed microorganisms – Str. pyogenes and Ser. marcescens 1,3,5. Coley’s toxin was often used for the successful treatment of sarcomas, carcinomas, lymphomas, melanomas and myelomas. Complete and prolonged regression of advanced stages of malignant disease was documented in many cases. The author has previously reported that in 80% of the cases of malignant tumours, for which no alternate form of treatment was available, survival was longer than 5 years. Even in end-stage cancer patients, notable improvements in health were described 7,16. During treatment with Coley’s toxin, a broad spectrum of side effects of the administered adjuvant occur, owing to which this treatment is not generally accepted among clinicians 3.
Coley set the basic steps for the successful administration of the toxin. After the application, infection with resulting fever should develop. Immunotolerance is induced by a gradual increase in the toxin dose (dependent on the immune response of the patient). Wherever possible, the toxin should be injected directly into the tumour or at the site to which it has metastasized. The injection should be administered daily or every other day for a period of 1–2 months and then once a week for at least 6 months to prevent recurrence of the disease 2,7,8.
An interesting phenomenon that occurred during treatment with Coley’s toxin was that the fever moderated the pain in cancer patients. This finding has been previously described in other studies as well. As a result, some patients could reduce the use of painkillers. This effect was often described immediately after the injection. Hoption Cann 8 has described Lagueux’s observation that the pain always disappeared after the first injection.
Coley emphasized that induction of fever was the most important symptom for inducing spontaneous regression of cancer. In a retrospective study of patients with inoperable sarcoma after treatment with Coley’s toxin, a greater than 5-year survival rate was reported among those who had high fever (38–40°C), compared to those who had no fever or only slightly elevated temperature during the treatment 2.
It is assumed that the main factor responsible for the therapeutic effect of Coley’s toxin was the increased expression of tumour necrosis factor (TNF), interleukins (ILs) and interferons (INFs) in the body of the patient. Antitumour efficacy of TNF has been confirmed in animal models, in which it has been observed to inhibit growth or result in complete regression of the tumour 8,17.
Furthermore, it has also been confirmed that the antitumour effect of Coley’s toxin could be mediated by the production of IL-12, known to extend the function of pre-existing tumour-specific T cells for subsequent induction of signals required for tumour regression. IL-12 receptors are preferentially expressed on activated T-cells, and this explains why the therapy with IL-12 is effective against pre-existing tumours 5.
The last recorded successful application of the toxin was in China in 1980 as a primary therapy for the treatment of terminal liver cancer. The patient received 68 injections of Coley’s toxin during the 34 weeks of therapy. After this procedure, the symptoms disappeared completely 2.
Bacillus Calmette-Guérin
The observation that the presence of bacterial infection results in the stimulation of the immune system has led to the clinical use of BCG (Mycobacterium bovis) in the treatment of superficial urinary bladder cancer 5. It is considered to be the most successful form of immunotherapy, and this method has become the standard for treatment of this type of tumour. The vaccine strain of M. bovis is injected directly into the bladder 3,18.
Many studies have shown a clear correlation between the usage of BCG after surgical removal of the tumour and the subsequent decrease or delay in the risk for cancer recurrence. Almost 60% of the patients showed no signs of tumour recurrence 14,19,20.
The antitumour effect of the vaccine is based on the induction of a local immune response and the production of cytokines such as IL-2, TNF-α and INF-γ. After intravesical administration of the vaccine, IL-1, IL-6, IL-8, IL-10, IL-12, IL-18 and macrophage colony stimulating factor were detected in urine over the course of the disease. Similar to Coley’s toxin, the application of BCG requires long-term administration. The possible influence of BCG on the reduction of colorectal carcinoma has also been studied 5,8,11,12,21.
It has been previously mentioned that the anti-tumour effect of the BCG vaccine could be due to its effect of decreasing the proliferation of tumour cells, along with production of the cytokines mentioned above 20. Unfortunately, this method of treatment also had significant toxicity and was inefficient in 30–50% of cases 5.
Clostridium spp. and other anaerobic bacteria
Hypoxia is a pathophysiological feature in the majority of solid tumours. Hypoxic areas in poorly vascularized cancers that make the effective distribution of an active drug difficult are the main barriers to successful cancer therapy. The blood vessels in tumours are structurally and functionally abnormal, resulting in heterogeneous blood supply 13,22.
The hypoxic microenvironment in solid cancers is ideal for survival and multiplication of anaerobic bacteria. Healthy tissue, where blood supply is sufficient, is therefore not attacked by the bacteria. It was assumed that their application into the tumour should yield expected therapeutic effect. This assumption was confirmed in the 1960s 22,23.
Over the next 50 years, several strains of facultative and obligate anaerobic bacteria were tested as potential therapeutic agents for the induction of spontaneous regression of tumours. These bacteria were localized to cancer tissue, and lysis of tumours was observed in experimental animal models. These promising data resulted in trial studies initiated in the 1960s that use bacteria of the genus Clostridium. However, the results were not as good as expected and the studies were terminated 5,13,24.
Besides the above-mentioned genus Clostridium, bifidobacteria and lactobacilli were the other microorganisms tested as potential therapeutic agents inducing tumour regression. These bacterial strains were shown to be highly selective and localized primarily within the tumour cells 5,21.
Clostridium spp.
Clostridium spp. was shown to cause tumour regression in a rodent model. However, in subsequent clinical studies in human populations, significant therapeutic effect was not demonstrated. The toxic effects after administration of these bacteria exceeded the beneficial effects 22.
As mentioned above, clostridia have the unique property of proliferating in the necrotic areas of the tumour under hypoxic conditions. Unfortunately, in many animal models, acute toxicity or even mortality of the tested subject was observed.
In 1935, Connell used sterile filtrates from C. histolyticum to treat advanced forms of cancers. The observed tumour regression was attributed to the production of proteolytic enzymes. Mengesha 25 mentioned that the setup with deliberate colonization of tumour-bearing mice with clostridial spores was first used in 1947.
A typical example of this genus is C. novyi, which showed significant antitumour effect during experiments in laboratory animals. Spores of C. novyi were systematically injected into the animal, in which they grew perfectly in the hypoxic tumour environment. Thirty per cent of the mice treated with these spores were cured of their tumours, although the tumour margin remained visible after the germination of the spores. However, the majority of these cases resulted in the death of the animal 21,22,24. For this reason, the attenuated strain C. novyi-NT was developed by genetic modification, with deletion of the gene encoding the lethal toxin. Satisfactory results were obtained; however, toxicity was still present, thus making it unsuitable for tumour therapy 13,24.
To avoid the toxicity, nonpathogenic strains of C. oncolyticum were also used 13. Application of the Clostridium spp. strain M55 resulted in colonization of necrotic areas of the tumour, but cancer regression was not observed 26.
C. perfringens was shown to be capable of colonizing in advanced stages of selective pancreatic cancers and inducing progressive necrosis in the tumours. The possibilities of conventional methods of treatment (radiotherapy and chemotherapy) are limited in this type of cancer and the response to conventional therapy is poor 22.
Bifidobacterium spp.
The genus Bifidobacterium, another promising representative of anaerobic bacteria, is also considered a possible candidate for cancer therapy. Attention is focused mainly on the following three representatives: B. longum, B. infantis and B. adolescentis 10.
B. longum is a nonmotile bacterium that remains, survives and grows under the anaerobic conditions of a tumour. After intravenous administration of B. longum in mice with tumours, no additional visible symptoms were observed. It has been repeatedly proven that the bacteria disappear from normal tissues or organs such as the liver, kidneys, lungs, blood and bone marrow 48–96 h after administration and grow only in the tumour. Within 1 h, 102 CFU/g of bacteria, and by day 7, 106 CFU/g of bacteria were present in the tumour. Unfortunately, there was no antitumour effect 10,21. In another study B. adolescentis was tested, and this bacteria was shown to prevent the occurrence and development of colorectal cancer and induce apoptosis in an animal model 10.
Lactobacillus spp.
Lactobacilli are generally considered as safe microorganisms, and they have been studied for a wide range of possible applications. Experimental studies have shown that oral administration of lactobacilli may contribute to the reduction of recurrence of urinary bladder cancer. It has been proven that lactobacilli on administration inhibit chemically induced carcinogenesis and reduce tumour growth in animal models 27.
Salmonella spp.
Bacteria of the genus Salmonella are facultative anaerobic bacteria and are able to grow in both aerobic and anaerobic environments. S. enterica, serovar Typhimurium has been reported to cause spontaneous regression of cancer after intravenous administration of live attenuated vaccines in mice with growing tumours 23. More than 50 years ago, it was demonstrated that this bacterium can colonize human tumours, and a ratio of microorganisms in the tumour to those in healthy tissue of 103–104 : 1 was mentioned 5,28.
The Salmonella spp. strain VNP20009 was successfully developed for use in anticancer therapy. Deletion of MsbB and purL genes resulted in complete attenuation and elimination of potential adverse effects after its application. Some strains of this genus induce clinical conditions associated with septic shock. This vector showed a long lasting efficacy against a broad spectrum of carcinomas, and it targeted the metastatic lesions as well 5,24. The Salmonella strain VPN20009 was used in the USA in phase I of testing for the treatment of metastatic melanoma and renal cancer. The minimum tolerated dose in relation to the toxicity was determined to be 3×108/body surface (m2), and the presence of Salmonella was detected by biopsy of tissue. Regression of cancer was not observed in any patient, and only in three patients was the presence of bacteria demonstrated by biopsy. In four patients, symptoms associated with the presence of bacterial infection were described. However, no bacteria were found in the biopsy samples. Their identification was confirmed by excision of whole tumour tissues 21. Overall, it could be concluded that the results of application of this bacterial strain were not satisfactory. Only high doses and repeated administration of these bacteria led to colonization of the tumour, but the therapeutic effect was unremarkable 29.
S. typhimurium strain A1 proliferates in tumour xenografts but not in normal tissue. It is auxotrophic (leu/arg-dependent) and only grows locally. Reisolated S. typhimurium A1 strain (from A1-targeted tumour), named A1-R, inhibited, and in some cases even eradicated, primary and metastatic tumours. In vivo, these bacteria caused human prostatic cancer cell inhibition and subsequent regression of subcutaneous xenografts 30,31.
Strain A1-R administered intravenously induced human breast cancer regression and cured cancer in nude mouse models 32,33. Furthermore, breast-cancer brain metastases were significantly inhibited by this bacterial strain in mouse models 34. Uchogonova et al. 35 and Liu et al. 36 reported that the A1-R strain was highly effective against lung carcinoma, especially against metastases in nude mice.
S. typhimurium A1-R has a promising effect on disseminated ovarian cancer, especially after intraperitoneal administration in nude mouse models. Clinical application of S. typhimurium A1-R was suggested for ovarian cancer, a highly treatment-resistant disease 37,38. Potential therapeutic usage of these bacteria in cervical carcinoma has also been mentioned 39.
A significant effect of the A1-R strain against pancreatic cancer has been described in different mouse models [nude, C57BL/6 and C57BL/6 CD8−/− (B6.129S2-CD8atm1Mak/J mice)], and the clinical implications have been described 40–45. For sarcoma and glioma treatment, a potential therapeutic effect of the A1-R strain has been suggested as well 46–51.
The antitumour activity of Salmonella spp. has been previously described. The production of a wide spectrum of enzymes by bacterial species could be one of the mechanisms that lead to the apoptosis of tumour cells. It has been reported that induction of apoptosis in cancer correlated with the accumulation of Salmonella spp. in tumours. Autophagy could also be another mechanism of tumour cell apoptosis. Inhibition of apoptosis of the infected cancer leads to an increase in autophagy 28.
Other tested microorganisms
The following microbial agents have been tested as potential anticancer agents or for the production of vaccines: S. cholerae suis, Vibrio cholerae, Listeria monocytogenes and Escherichia coli 24.
Spontaneous regression has also been associated with other bacterial infections such as diphtheria, gonorrhoea, syphilis and tuberculosis; viral diseases like hepatitis, influenza, rubella and smallpox; and other purulent or nonpurulent diseases 2.
Bacteria and viruses are not the only agents that can induce tumour regression in an infected host. Protozoans such as Toxoplasma gondii and Besnoitia jellisoni can also activate macrophages and induce tumour regression 23.
Anticancer methods using microorganisms
Commonly used anticancer methods using microorganisms comprise bactofection, alternative gene therapy, combined bacteriolytic therapy and bacteria-directed enzyme prodrug therapy. For more details, see Table 1. Special categories of cancer treatment using microbial peptides have been described in Table 2.
Table 1.
Commonly used methods of application of microorganisms in anticancer therapy

Table 2.
Microbial peptides used in the application of microorganisms in anticancer therapy

Role of the immune system in spontaneous regression of cancer
As mentioned above, spontaneous regression of tumours is associated with bacterial, viral, fungal or protozoan infections.
The duality of the immune system
An important factor that applies to the regression of cancer is the duality of the immune system. In the defensive mode, there is regression of the tumour and cells of the immune system are produced. Conversely, in the reparative mode, progression is facilitated and invasiveness is increased by the production of immunosuppressive cytokines, growth factors, angiogenic factors and matrix metalloproteinases. The defensive mode is active during an ongoing infectious disease 8,12. A considerable number of studies confirm that tumour infiltrating leucocytes are not successful in inhibiting the growth of tumours; however, they are actively involved in the progression of cancer through their reparative functions 57.
The immune system versus bacteria versus spontaneous regression of cancer
Infection of tumours leads to infiltration by lymphocytes and antigen-presenting cells such as macrophages and dendritic cells (DCs). Binding of pathogen-associated molecular patterns to toll-like receptors on antigen-presenting cells induces activation and antigen presentation. Induction leads to the production of important costimulatory molecules such as B7 and IL-12, resulting in the activation of the immune system 12. DCs can be stimulated primarily by lipopolysaccharides of Gram-negative bacteria or by other bacterial or viral products. The present bacterial infection has a three-fold effect on their stimulation. Large numbers of bacteria possessing lipopolysaccharides induce the production of cytokines; the production of thymocytes and cytotoxic T lymphocytes (CTL) increases in vitro during the rise of temperature. Cancer cells can be more sensitive to heat than normal cells; infections that cause haemorrhagic necrosis could trigger collapse of the vasculature of the tumour because of fever 7,58. Febrile illness could play a role in remission of cancer because fever can lead to the release of a cascade of proinflammatory factors capable of stimulating DCs and resulting in T-cell activation 7.
It has been suggested that regression is related to cellular rather than humoral immunity. In Coley’s experiments, it has been described that tumour regression occurred several hours after injection of the toxin, and discontinuation of therapy for even a day resulted in reappearance of the tumour from its residual tissue. Antitumour immunity was mediated by innate and nonspecific immune responses rather than by the slower adaptive immunity. For this reason, Coley had recommended daily injection of the toxin 8,23.
T lymphocytes are responsible for cell-mediated immunity, and B cells for humoral immunity. B-cells play a role in the destruction of tumours by lysis mediated by complement activation and facilitate antibody-dependent cell-mediated cytotoxicity. CTL and natural killer (NK) cells are important in inducing tumour lysis. CTL cells recognize major histocompatibility complex antigens on the cell membrane and NK cells seek out and kill the tumour cells, thus playing an important role in the prevention of metastases 6.
Oikonomopoulou and colleagues reported that some pathogens express antigens that cross-react with tumour-associated antigens. Thomsen-Friedenreich (T) and Tn parasitic antigens were detected in more than 80% of cancer patients, and appear to be potential markers for clinical use. In addition, in sera obtained from patients with parasitic infections (Echinococcus), cross-reactivity is often observed with sera gained from patients with carcinoma. Interestingly, these sera are frequently present in patients with less-extensive tumours. Antibodies against these shared antigens can potentially target the tumour cells to be destroyed or increase the presentation of antigens to T cells and thus induce an antitumour response 59.
Another interesting finding was that, in mice bearing melanoma infected with T. gondii tumour, regression was observed without current activation of CTLs and NK cells, production of NO by macrophages and IL-12 or TNF release. The authors found that the tissues infected by T. gondii produced some factors that prevent the formation of blood vessels in tumour tissue. As a result, hypoxia occurs and therefore causes necrosis and subsequent cell death. The authors consider that inhibition of angiogenesis during infection could be caused by synthesis of soluble antiangiogenic factors by infected tissues, which could serve as a potential therapeutic agent like endostatin (endogenous angiogenesis inhibitor) 23,59.
Factors related to microorganisms and macroorganism versus spontaneous regression of tumour
Factors related to microorganisms comprise microbial products and pathogen-associated molecular patterns (extracellular and intracellular microorganisms) and subsequent activation of an appropriate immune response. For more information, see Fig. 1. Figure 2 informs the readers about the factors related to macroorganism with regard to subsequent possible spontaneous regression of tumours (immune system, receptors, mediators, cells, etc.)
Fig. 1.
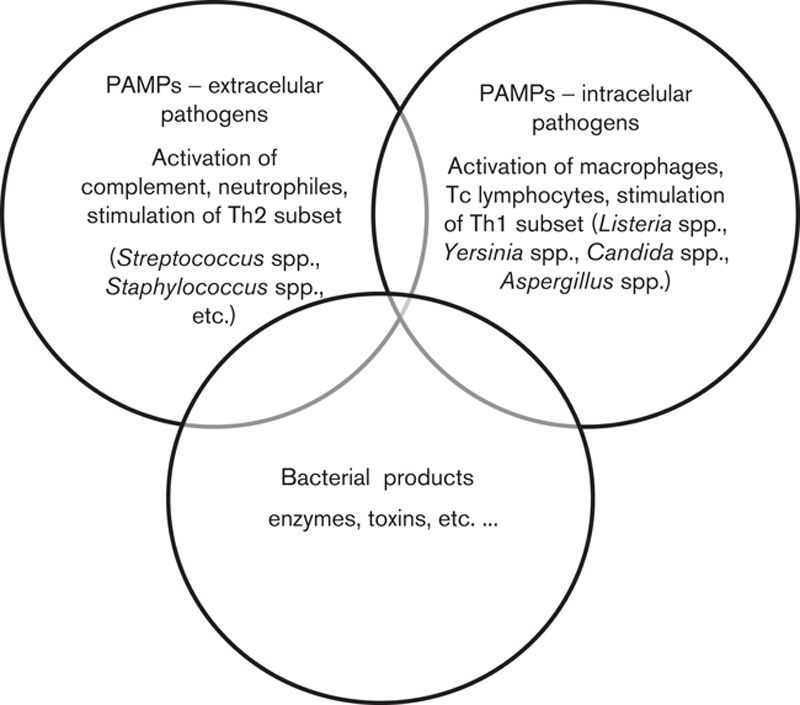
Factors related to microorganisms.
Fig. 2.

Factors related to macroorganisms. CLR, C-type lectin receptors; DC, dendritic cell; IL, interleukin; INF, interferon; MF, macrophages; NLR, NOD-like receptors; RLR, RIG-I-like receptors; TIL, tumour-infiltrating lymphocytes; TLR, Toll-like receptors; TNF, tumour necrosis factor.
Other mechanisms
Mager mentions an interesting study on the mechanism that could potentially contribute to the spontaneous regression of cancer. The tumour regression observed after the administration of Coley’s toxin was caused by activation of plasminogen. In that case, the bacterial enzyme streptokinase (product of bacteria Str. pyogenes) acts on the plasminogen of the host, resulting in the release of plasmin. Plasmin triggers a cascade of proteases that degrade the plasma and extracellular matrix proteins. These mechanisms are fatal for tumour cells as they disrupt the extracellular matrix of the tumour, suspend its subsequent growth and reduce the risk for metastases 7.
Conclusion
Spontaneous regression of cancer associated with the presence of microbial agents is a very important treatment option for cancer. These new therapeutic approaches, aimed at application of killed or genetically modified microorganisms as vaccines, could significantly reduce the side effects of other more commonly used methods of cancer therapy like chemotherapy and radiotherapy. The phenomenon of spontaneous regression of cancer is also one of the key areas of research in our laboratory, because of the spontaneous regression of hereditary melanoma observed in the Melanoma-bearing Libechov Minipig (MeLiM). Bacterial strains of Staphylococcus spp. [Staphylococcus (St.) hyicus, St. epidermidis, St. lentis, St. hyicus, etc.], Streptococcus spp. (Str. uberis, Str. equi, Str. Dysgalactiae, etc.), and Enterobacteriaceae (E. coli, Klebsiella pneumoniae), as well as yeast (Candida lipolytica) have been cultivated from cutaneous and melanoma smears from the minipigs in our laboratory. It could be hypothesized that the production of specific enzymes by these microorganisms could induce immune mechanisms leading to spontaneous regression of malignant melanoma in the MeLiM model. Until now, we have failed to identify the exact mechanisms of melanoma regression. The presence of specific strains of microorganisms in the tumours of our minipigs could provide us with a vital clue that connects spontaneous regression with microorganisms.
Acknowledgements
This study was funded by grant project OP VaVpI-CZ.1.05/2.1.00/03.0124 – ‘ExAM – Experimental Animal Models’.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Bunting A. Genetically engineered bacteria as cancer fighting agents. Univ Ottawa J Med 2013; 3:26–33. [Google Scholar]
- 2.Jessy T. Immunity over inability: the spontaneous regression of cancer. J Nat Sci Biol Med 2011; 2:43–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Baird JR, Byrne KT, Lizotte PH, Toraya-Brown S, Scarlett UK, Alexander MP, et al. Immune-mediated regression of established B16F10 melanoma by intratumoral injection of attenuated Toxoplasma gondii protects against rechallenge. J Immunol 2013; 190:469–478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Abdulamir AS, Hafidh RR, Abu Bakar F. The tumoricidal activity of Salmonella and its role in treating cancers. Cancer Ther 2013; 8:10–23. [Google Scholar]
- 5.Sengupta N, MacFie TS, MacDonald TT, Pennington D, Silver AR. Cancer immunoediting and ‘‘spontaneous’’ tumor regression. Pathol Res Pract 2010; 206:1–8. [DOI] [PubMed] [Google Scholar]
- 6.Thomas JA, Badini M. The role of innate immunity in spontaneous regression of cancer. Indian J Cancer 2011; 48:246–251. [DOI] [PubMed] [Google Scholar]
- 7.Mager DL. Bacteria and cancer: cause, coincidence or cure? A review. J Transl Med 2006; 4:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hoption Cann SA, van Netten JP, van Netten C. Dr William Coley and tumour regression: a place in history or in the future. Postgrad Med J 2003; 79:672–680. [PMC free article] [PubMed] [Google Scholar]
- 9.Hoption Cann SA, van Netten JP, van Netten C. Acute infections as a means of cancer prevention: Opposing effects to chronic infections? Cancer Detect Prev 2006; 30:83–93. [DOI] [PubMed] [Google Scholar]
- 10.Wei MQ, Mengesha A, Good D, Anné J. Bacterial targeted tumour therapy – dawn of a new era. Cancer Lett 2008; 259:16–27. [DOI] [PubMed] [Google Scholar]
- 11.Paton AW, Morona R, Paton JC. Bioengineered microbes in disease therapy. Trends Mol Med 2012; 18:417–425. [DOI] [PubMed] [Google Scholar]
- 12.Kok-Ho H. Spontaneous regression of cancer: a therapeutic role for pyrogenic infections? AMSJ 2012; 3:30–33. [Google Scholar]
- 13.Jain RK, Forbes NS. Can engineered bacteria help control cancer? Proc Natl Acad Sci USA 2001; 98:14748–14750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chakrabarty AM. Microorganisms and cancer: quest for a therapy. J Bacteriol 2003; 185:2683–2686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ramasamy S, Nattarayan V, Jayaraj GG, Arulanandh MD, Jaiswal A. Bacterial infection-mediated anticancer activity (BIMAc) – revisiting the molecular mechanisms. J Med Hypotheses Ideas 2012; 6:19–22. [Google Scholar]
- 16.Kim CJ, Dessureault S, Gabrilovich D, Reintgen DS, Slingluff CL., Jr Immunotherapy for melanoma. Cancer Control 2002; 9:22–30. [DOI] [PubMed] [Google Scholar]
- 17.Karpiński TM, Szkaradkiewicz AK. Anticancer peptides from bacteria. Bangladesh J Pharmacol 2013; 8:343–348. [Google Scholar]
- 18.Chorobik P, Czaplicki D, Ossysek K, Bereta J. Salmonella and cancer: from pathogens to therapeutics. Acta Biochim Pol 2013; 60:285–297. [PubMed] [Google Scholar]
- 19.Paterson Y, Guirnalda PD, Wood LM. Listeria and Salmonella bacterial vectors of tumor-associated antigens for cancer immunotherapy. Semin Immunol 2010; 22:183–189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mukaratirwa S, Chitanga S, Chimatira T, Makuleke C, Sayi ST, Bhebhe E. Combination therapy using intratumoral bacillus Calmette-Guerin (BCG) and vincristine in dogs with transmissible venereal tumours: therapeutic efficacy and histological changes. J S Afr Vet Assoc 2009; 80:92–96. [DOI] [PubMed] [Google Scholar]
- 21.Taniguchi S, Fujimori M, Sasaki T, Tsutsui H, Shimatani Y, Seki K, et al. Targeting solid tumors with non-pathogenic obligate anaerobic bacteria. Cancer Sci 2010; 101:1925–1932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Li Z, Fallon J, Mandeli J, Wetmur J, Woo SL. A genetically enhanced anaerobic bacterium for oncopathic therapy of pancreatic cancer. J Natl Cancer Inst 2008; 100:1389–1400. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 23.Yamada T, Goto M, Punj V, Zaborina O, Chen ML, Kimbara K, et al. Bacterial redox protein azurin, tumor suppressor protein p53, and regression of cancer. Proc Natl Acad Sci USA 2002; 99:14098–14103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Patyar S, Joshi R, Byrav DS, Prakash A, Medhi B, Das BK. Bacteria in cancer therapy: a novel experimental strategy. J Biomed Sci 2010; 17:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Mangesha A. Use of non-pathogenic bacteria as vectors for targeted gene expression in cancer gene therapy [dissertation]. the NetherlandsMaastricht University, 2009.
- 26.Sen PP, Gautham A, Manavalan M, Najeeb MA. Bacteria in cancer therapy: an emerging robust therapy. Int Res J Pharm 2013; 4:1–4. [Google Scholar]
- 27.Seow SW, Cai S, Rahmat JN, Bay BH, Lee YK, Chan YH, et al. Lactobacillus rhamnosus GG induces tumor regression in mice bearing orthotopic bladder tumors. Cancer Sci 2010; 101:751–758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Chang WW, Lee CH. Salmonella as an innovative therapeutic antitumor agent. Int J Mol Sci 2014; 15:14546–14554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Leschner S, Westphal K, Dietrich N, Viegas N, Jablonska J, Lyszkiewicz M, et al. Tumor invasion of Salmonella enterica serovar Typhimurium is accompanied by strong hemorrhage promoted by TNF-a. PLoS One 2009; 4:e6692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Zhao M, Yang M, Li XM, Jiang P, Baranov E, Li S, et al. Tumor targeting bacterial therapy with amino acid auxotrophs of GFP-expressing Salmonella typhimurium. Proc Natl Acad Sci USA 2005; 102:755–760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zhao M, Geller J, Ma H, Yang M, Penman S, Hoffman RM. Monotherapy with a tumor-targeting mutant of Salmonella typhimurium cures orthotopic metastatic mouse models of human prostate cancer. Proc Natl Acad Sci USA 2007; 104:10170–10174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Zhao M, Yang M, Ma H, Li X, Tan X, Li S, et al. Targeted therapy with a Salmonella typhimurium leucine arginine auxotroph cures orthotopic human breast tumors in nude mice. Cancer Res 2006; 66:7647–7652. [DOI] [PubMed] [Google Scholar]
- 33.Zhang Y, Tome Y, Suetsugu A, Zhang L, Zhang N, Hoffman RM, et al. Determination of the optimal route of administration of Salmonella typhimurium A1 R to target breast cancer in nude mice. Anticancer Res 2012; 32:2501–2508. [PubMed] [Google Scholar]
- 34.Zhang Y, Miwa S, Zhang N, Hoffman RM, Zhao M. Tumor-targeting Salmonella typhimurium A1-R arrests growth of breast-cancer brain metastasis. Oncotarget 2015; 6:2615–2622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Uchugonova A, Zhao M, Zhang Y, Weinigel M, König K, Hoffman RM. Cancer-cell killing by engineered Salmonella imaged by multiphoton tomography in live mice. Anticancer Res 2012; 32:4331–4337. [PubMed] [Google Scholar]
- 36.Liu F, Zhang L, Hoffman RM, Zhao M. Vessel destruction by tumor targeting Salmonella typhimurium A1-R is enhanced by high tumor vascularity. Cell Cycle 2010; 9:4518–4524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Matsumoto Y, Miwa S, Zhang Y, Hiroshima Y, Yano S, Uehara F, et al. Efficacy of tumor-targeting Salmonella typhimurium A1 R on nude mouse models of metastatic and disseminated human ovarian cancer. J Cell Biochem 2014; 115:1996–2003. [DOI] [PubMed] [Google Scholar]
- 38.Matsumoto Y, Miwa S, Zhang Y, Zhao M, Yano S, Uehara F, et al. Intraperitoneal administration of tumor-targeting Salmonella typhimurium A1-R inhibits disseminated human ovarian cancer and extends survival in nude mice. Oncotarget 2015; 6:11369–11377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hiroshima Y, Zhang Y, Zhang N, Maawy A, Mii S, Yamamoto M, et al. Establishment of a patient-derived orthotopic xenograft (PDOX) model of HER-2-positive cervical cancer expressing the clinical metastatic pattern. PLoS One 2015; 10:e0117417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Nagakura C, Hayashi K, Zhao M, Yamauchi K, Yamamoto N, Tsuchiya H, et al. Efficacy of a genetically-modified Salmonella typhimurium in an orthotopic human pancreatic cancer in nude mice. Anticancer Res 2009; 29:1873–1878. [PubMed] [Google Scholar]
- 41.Yam C, Zhao M, Hayashi K, Ma H, Kishimoto H, McElroy M, et al. Monotherapy with a tumor-targeting mutant of S. typhimurium inhibits liver metastasis in a mouse model of pancreatic cancer. J Surg Res 2010; 164:248–255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hiroshima Y, Zhao M, Zhang Y, Maawy A, Hassanein MK, Uehara F, et al. Comparison of efficacy of Salmonella typhimurium A1-R and chemotherapy on stem-like and non-stem human pancreatic cancer cells. Cell Cycle 2013; 12:2774–2780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Binder DC, Engels B, Arina A, Yu P, Slauch JM, Fu YX, et al. Antigen-specific bacterial vaccine combined with anti-PD-L1 rescues dysfunctional endogenous T cells to reject long-established cancer. Cancer Immunol Res 2013; 1:123–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hiroshima Y, Zhao M, Maawy A, Zhang Y, Katz MH, Fleming JB, et al. Efficacy of Salmonella typhimurium A1-R versus chemotherapy on a pancreatic cancer patient-derived orthotopic xenografts (PDOX). J Cell Biochem 2014; 115:1254–1261. [DOI] [PubMed] [Google Scholar]
- 45.Hiroshima Y, Zhang Y, Murakami T, Maawy A, Miwa S, Yamamoto M, et al. Efficacy of tumor-targeting Salmonella typhimurium A1-R in combination with anti-angiogenesis therapy on a pancreatic cancer patient-derived orthotopic xenografts (PDOX) and cell-line mouse models. Oncotarget 2014; 5:12346–12357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hayashi K, Zhao M, Yamauchi K, Yamamoto N, Tsuchiya H, Tomita K, et al. Systemic targeting of primary bone tumor and lung metastasis of high-grade osteosarcoma in nude mice with a tumor-selective strain of Salmonella typhimurium. Cell Cycle 2009; 8:870–875. [DOI] [PubMed] [Google Scholar]
- 47.Hayashi K, Zhao M, Yamauchi K, Yamamoto N, Tsuchiya H, Tomita K, et al. Cancer metastasis directly eradicated by targeted therapy with a modified Salmonella typhimurium. J Cell Biochem 2009; 106:992–998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Miwa S, Zhang Y, Baek KE, Uehara F, Yano S, Yamamoto M, et al. Inhibition of spontaneous and experimental lung metastasis of soft-tissue sarcoma by tumor-targeting Salmonella typhimurium A1-R. Oncotarget 2014; 5:12849–12861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hiroshima Y, Zhao M, Zhang Y, Zhang N, Maawy A, Murakami T, et al. Tumor-targeting Salmonella typhimurium A1-R arrests a chemo-resistant patient soft-tissue sarcoma in nude mice. PLoS One 2015; 10:e0134324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Kimura H, Zhang L, Zhao M, Hayashi K, Tsuchiya H, Tomita K, et al. Targeted therapy of spinal cord glioma with a genetically modified Salmonella typhimurium. Cell Prolif 2010; 43:41–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Momiyama M, Zhao M, Kimura H, Tran B, Chishima T, Bouvet M, et al. Inhibition and eradication of human glioma with tumor-targeting Salmonella typhimurium in an orthotopic nude-mouse model. Cell Cycle 2012; 11:628–632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Lehouritis P, Springer C, Tangney M. Bacterial-directed enzyme prodrug therapy. J Control Release 2013; 170:120–131. [DOI] [PubMed] [Google Scholar]
- 53.Bizzarri AR, Santini S, Coppari E, Bucciantini M, Di Agostino S, Yamada T, et al. Interaction of an anticancer peptide fragment of azurin with p53 and its isolated domains studied by atomic force spectroscopy. Int J Nanomed 2011; 6:3011–3019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Wolf P, Elsasser-Beile U. Pseudomonas exotoxin A: from virulence factor to anti-cancer agent. Int J Med Microbiol 2009; 299:161–176. [DOI] [PubMed] [Google Scholar]
- 55.Zhang Y, Schulte W, Pink D, Phipps K, Zijlstra A, Lewis JD, et al. Sensitivity of cancer cells to truncated diphtheria toxin. PLoS One 2010; 5:e10498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Lee DG, Hahm KS, Park Y, Kim HY, Lee W, Lim SC, et al. Functional and structural characteristics of anticancer peptide Pep27 analogues. Cancer Cell Int 2005; 5:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Hoption Cann SA, van Netten JP, van Netten C, Glover DW. Spontaneous regression: a hidden treasure buried in time. Med Hypotheses 2002; 58:115–119. [DOI] [PubMed] [Google Scholar]
- 58.Hobohm U. Fever and cancer in perspective. Cancer Immunol Immunother 2001; 50:391–396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Oikonomopoulou K, Brinc D, Kyriacou K, Diamandis EP. Infection and cancer: revaluation of the hygiene hypothesis. Clin Cancer Res 2013; 9:2834–2841. [DOI] [PubMed] [Google Scholar]