

Abstract
Purpose
To test the hypothesis that acute topical dorzolamide (DZ) decreases intraocular pressure (IOP) and increases retinal and choroidal blood flow in the DBA/2J mouse model of glaucoma.
Methods
Retinal and choroidal blood flow were measured in 4- and 9-month-old DBA/2J mice, and 4-month C57BL/6 (control) mice under isoflurane anesthesia using magnetic resonance imaging. Ocular blood flow was measured at baseline, and 1 and 2 hours after topical dorzolamide. Intraocular pressure was measured using a rebound tonometer in a subset of animals at the same time points.
Results
Baseline IOP in the 4-month-old DBA/2J mice and C57BL/6 mice was not significantly different (P > 0.05), and IOP in both groups was less than in the 9-month-old DBA/2J mice (P < 0.05 for both). Compared to baseline, dorzolamide reduced IOP at 1 and 2 hours after dorzolamide in the 4- (P < 0.05) and 9-month-old (P < 0.01) DBA/2J mice, but not in the C57BL/6J mice (P > 0.05). Baseline retinal blood flow was lower in the 4-month and 9-month-old DBA/2J mice compared with the 4-month-old C57BL/6J mice (P < 0.05). Baseline choroidal blood flow in the 9-month-old DBA/2J mice was less than in the C57BL/6J mice (P < 0.05). Compared with baseline, both retinal and choroidal blood flow increased at 1-hour post-dorzolamide and remained elevated 2 hours later in the 9-month-old DBA/2J mice (P < 0.05).
Conclusions
Dorzolamide lowers IOP and raises retinal and choroidal blood flow in older DBA/2J mice, consistent with the study hypothesis.
Keywords: MRI, regional blood flow, glaucomatous optic neuropathy
Animal models often utilize ocular hypertension to study glaucoma pathogenesis, altered homeostatic mechanisms, and pharmacology.1 One widely used model is the DBA/2J mouse.2–6 The mouse DBA/2J has altered expression of two proteins: tyrosinase-related protein 1 associated with iris stromal atrophy, and glycoprotein transmembrane NMB associated with iris pigmentary dispersion, which raises intraocular pressure (IOP) by blocking the trabecular meshwork and reducing outflow facility.7,8 The resultant ocular hypertension is associated with glaucoma-like retinal ganglion cell (RGC) loss with age.
We previously used the “arterial spin labeling” magnetic resonance imaging (ASL-MRI) technique to measure retinal and choroidal blood flow (RBF and ChBF, respectively) in the DBA/2J mouse model.9 We found that RBF and ChBF were reduced in DBA/2J mice compared to C57BL/6 control mice, suggesting a possible ischemic contribution to the optic neuropathy and visual dysfunction that occur in older DBA/2J mice.10–18 Interestingly, there is evidence that lowering the IOP pharmacologically enhances RGC survival in older DBA/2J mice.19,20 It is unknown whether lowering IOP would increase their ocular blood flow, which might contribute to the enhanced RGC survival. Therefore, to further characterize the DBA/2J model, the goal of the present study was to test the hypothesis that lowering IOP increases RBF and ChBF in the DBA/2J mouse at different ages. To lower IOP, topical dorzolamide (DZ) was chosen because it inhibits aqueous humor production21 and it was assumed that an aqueous suppressant would be more effective at lowering IOP than a drug that enhances outflow facility (e.g., pilocarpine) since the ocular hypertension in the DBA/2J model is due to obstruction of the trabecular outflow pathway.
Methods
The protocol was approved by the local Institutional Animal Care and Use Committee in accordance with the Guide for the Care and Use of Laboratory Animals and adhered to the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research.
MRI Measurements of Blood Flow (BF)
Three groups of animals were used for MRI study: male wild-type C57BL/6J mice aged 4 months (n = 8), and male DBA/2J mice aged 4 months (n = 8) and 9 months (n = 6). During imaging, mice spontaneously breathed a mixture of 30% O2/70% N2 with 1.6% isoflurane for anesthesia while the animals were held in a custom-made holder with ear and tooth bars to minimize motion. Respiratory rate was monitored via a force transducer and maintained in a target range of 80 to 120 breaths per minute by slight adjustments to the level of anesthesia. Heart rate and arterial oxygen saturation were also monitored using oximetry (MouseOx; STARR Life Science Corp., Oakmont, PA, USA). Animal temperature was monitored and maintained at 37°C with warm water that circulated through a water pad underneath the mouse throughout the experiment.
Blood flow MRI was acquired at baseline (before DZ application). Then a single drop (5 μL) of dorzolamide HCL ophthalmic solution (2%, Bausch and Lomb) was applied on the left eye, and BF MRI was acquired again at 1 and 2 hours after DZ application. The animals were allowed to recover after the scans were completed.
MRI Parameters
Depth-resolved BF MRI was performed at a resolution of 42 × 42 × 400 μm in a magnet with a 150 Gauss/cm gradient (Bruker Biospec 7 Tesla; Bruker Corp., Billerica, MA, USA) using a custom circular eye coil for imaging (diameter = 6 mm) and circular heart coil for ASL (inner diameter = 8 mm).22,23 The blood flow scans were acquired with a gradient-echo, echo-planar imaging sequence with a 6 × 6 mm field of view and 144 × 144 matrix (42 × 42 μm resolution in-plane) zero-filled interpolation to 256 × 256. The blood flow sequence used a single, 400 μm coronal slice, two shots, 2.94-second labeling pulse, 3.0-second repetition time, and a 13 ms echo time. The slice was positioned near the optic nerve and tilted perpendicular to the retina. Blood flow values were calculated from images acquired over a 20-minute period and averaged offline.
Image analysis was performed with custom software (MATLAB; MathWorks, Inc., Natick, MA, USA), and STIMULATE (University of Minnesota, www.cmrr.umn.edu) software packages as described in detail elsewhere.22 A semiautomated process in (MathWorks, Inc.) was used to linearize the retina; align the retina to correct for motion (if any) of the eye during the scan; and conduct an automated profile analysis. Profiles across the retinal thickness were obtained from images by projecting lines perpendicular to the retina with profiles obtained at ×4 spatial interpolation. The blood flow (mL/min/g) was calculated from the signal intensities of labeled and nonlabeled images as: BF = (λ /T1)(SNL-SL)/(SL + [2α-1]SNL)), where λ·(0.9 mL/g) is the tissue-blood partition coefficient for water and is the value ([quantity of water/grams of tissue]/[quantity of water/mL of blood]); T1 is 1.8 seconds at 7 Tesla, SNL is the signal intensity (arbitrary units) of images with non-labeled blood, SL (arbitrary units) is the signal intensity of images with magnetically labeled blood, and α is the arterial spin-labeling efficiency (0.7) for cardiac labeling in mice. Blood flow profiles were averaged along the retina-choroid complex. Two peaks were present in the averaged BF profile, located in the inner retina and choroid. Measurements of retinal and choroidal BF were determined from the corresponding peaks of the average BF profiles for each animal. The arterial spin labeling MRI method to measure retinal and choroid blood flow has been corroborated with the microsphere technique.24
Intraocular Pressure (IOP) Measurements
Measurements of IOP were performed with a rebound tonometer (Icare Tonolab, Helsinki, Finland)25,26 on both eyes of 4-month-old C57BL/6J (n = 3), 4-month-old DBA/2J (n = 3), and 9-month-old DBA/2J (n = 3) male mice. These measurements were taken on a separate occasion than the MRI scans. The animals were anesthetized with 1.6% isoflurane and body temperature was maintained at 37°C using a heating pad. An average of six readings were taken at baseline, and again at 1 and 2 hours post-DZ applications. A single drop (5 μL) of dorzolamide HCL ophthalmic solution (2%, Bausch and Lomb) was applied on each eye. The animals were allowed to recover after the IOP measurements were completed. The same protocol was followed for an additional group of 9-month-old DBA/2J male mice (n = 3) that received topical saline as a control.
Arterial Pressure Measurements
We previously found that arterial pressure in older (age >6 months) C57BL/6 (n = 9) and DBA/2J (n = 9) mice was stable for 1 hour under isoflurane anesthesia.9 To confirm that blood pressure remained stable during the 2-hour period of anesthesia in the present study, femoral arterial pressure was measured in a 6-month-old C57BL/6 mouse and a 9-month-old DBA/2J mouse under 1.6% isoflurane. A femoral artery cutdown was performed and arterial pressure in the femoral artery was measured for >2 hours using a servo-null micropressure system (Model 900A; World Precision Instruments, Sarasota, FL, USA) and a recording system (PowerLab; ADInstruments, Colorado Springs, CO, USA).9 The technique uses glass micropipettes drawn to a 3 to 5 μm diameter tip to cannulate the target blood vessel. The pipette is filled with 2M NaCl that permits an electric circuit to be established between the pipette and a reference electrode placed in the tissue nearby. The resistance across the pipette tip is monitored and a pressure pod with a fast piezoelectric valve applies the necessary pressure to the open end of the pipette to maintain the resistance constant at the tip in the vessel. The applied pressure is taken to be equivalent to the pressure in the vessel. After the experiment, the mice were euthanized without regaining consciousness.
Statistical Analysis
The intraocular pressure data for each animal were pooled (i.e., the six measurements in each eye were averaged and then the mean IOP for the two eyes in each animal was averaged to give a single IOP value per animal). All data are reported as mean ± standard error of the mean, with significant differences accepted at P < 0.05. Comparisons within strain by time point were done by 1-way repeated measures ANOVA with Bonferroni post hoc tests. Comparisons between strains by time point were done by 2-way repeated measures ANOVA with Bonferroni post hoc tests (GraphPad Prism, La Jolla, CA, USA).
RESULTS
IOP
Figure 1 shows the IOP measurements at baseline, and 1 and 2 hours after topical DZ application outside the MRI scanner but under otherwise identical conditions as in the MRI experiments. Baseline IOP in the 9-month-old DBA/2J (22.7 ± 0.2 mm Hg) mice was significantly higher than in the C57BL/6J (11.4 ± 0.6 mm Hg, P < 0.001) and 4-month-old DBA/2J (11.0 ± 1.4 mm Hg, P < 0.001) mice. Baseline IOP was not significantly different between C57BL/6J and 4-month DBA/2J (P > 0.05), or between 9-month-old DBA/2J mice that received DZ or saline (21.5 ± 1.5 mm Hg, P > 0.05). One hour after DZ application, the IOP in the 4- DBA/2J (7.5 ± 0.4 mm Hg) and 9-month-old DBA/2J (7.8 ± 0.6 mm Hg) mice was significantly lower than baseline (P < 0.05 and P < 0.01, respectively) and remained significantly reduced (P < 0.05 and P < 0.01, respectively) compared with baseline at 2 hours after DZ (7.5 ± 0.8 and 8.0 ± 0.15 mm Hg, respectively). The intraocular pressure in the C57BL/6J mice was not significantly different (P > 0.05) from baseline at 1 or 2 hours after DZ (8.8 ± 0.2 and 9.1 ± 0.9 mm Hg, respectively). The intraocular pressure also was not significantly different (P > 0.05) from baseline at 1 and 2 hours after saline instead of DZ in 9-month-old DBA/2J mice (22.4 ± 1.4 and 21.72 ± 0.8 mm Hg, respectively).
Figure 1.

Mean IOP measurements for 4-month-old C57BL/6J, 4-month-old DBA/2J, and 9-month-old DBA/2J mice at baseline and at 1 and 2 hours post-DZ as well as 9-month-old DBA/2J mice before and after topical saline. See text for description of statistically significant differences.
MRI of Blood Flow
Figure 2A shows a layer-specific blood flow image from a normal mouse eye. Figure 2B displays an example of RBF and ChBF profiles in one control eye. The choroidal BF is markedly higher than the RBF, and the middle avascular layer has a minimal blood flow signal as expected.
Figure 2.

(A) Layer-specific blood flow map of a C57BL/6J mouse eye at a resolution of 42 × 42 × 400 μm. Blood flow maps detect choroidal and retinal vascular layers with the avascular zone in between. Scale bar: indicates the blood flow range. (B) Retinal and choroidal blood flow profiles (mL/min/g) were calculated from the signal intensities of labeled images such as in Figure 2A.
Retinal BF and ChBF were measured at baseline, and 1 and 2 hours post-DZ application (Fig. 3). Baseline RBF was significantly lower in both the 4- (0.90 ± 0.08 mL/min/g) and 9-month-old (0.78 ± 0.05 mL/min/g) DBA/2J mice compared with the C57BL/6J mice (1.24 ± 0.11 mL/min/g). At 1 hour after DZ, RBF was significantly increased (P < 0.05) in the 9-month-old DBA/2J mice (1.17 ± 0.03 mL/min/g), but not in the C57BL/6J (1.13 ± 0.06 mL/min/g) or the 4-month-old DBA/2J mice (1.06 ± 0.05 mL/min/g). At 2 hours after DZ, RBF in the 9-month-old DBA/2J (1.14 ± 0.07 mL/min/g) remained elevated above baseline (P < 0.05). Although trending lower, RBF in the C57BL/6J (1.06 ± 0.05 mL/min/g) and 4-month DBA/2J (0.95 ± 0.07 mL/min/g) mice remained unchanged from baseline at 2 hours after DZ.
Figure 3.

Retinal (A) and choroidal BF (B) at baseline, and 1 and 2 hours after topical dorzolamide in 4-month-old C57BL/6J, 4-month-old DBA/2J, and 9-month-old DBA/2J mice. See text for description of statistically significant differences.
Baseline ChBF was significantly lower in the 9-month-old DBA/2J mice (3.42 ± 0.27 mL/min/g) compared with the C57BL/6J mice (6.61 ± 0.62 mL/min/g) and the 4-month-old DBA/2J mice (4.84 ± 0.43 mL/min/g). At 1 hour after DZ, ChBF significantly increased (P < 0.05) in the 9-month-old DBA/2J mice (4.38 ± 0.39 mL/min/g), but not in the C57BL/6J (7.09 ± 0.62 mL/min/g) and the 4-month-old DBA/2J (5.19 ± 0.61 mL/min/g) compared with baseline. At 2 hours after DZ, ChBF remained above baseline (P < 0.05) in the 9-month-old DBA/2J mice (4.31 ± 0.40 mL/min/g); however, ChBF in the C57BL/2J (6.24 ± 0.45 mL/min/g) and the 4-month-old DBA/2J (3.92 ± 0.41 mL/min/g) mice were not significantly different from baseline, although both decreased significantly (P < 0.05) from their 1 hour values. Choroidal BF in the 9-month-old DBA/2J mice was lower than in the C57BL/6J mice at all time points (P < 0.05).
Blood Pressure Measurements
Systemic blood pressure in a 6-month-old C57BL/6J and a 9-month-old DBA/2J mouse were measured outside the MRI scanner over a similar 2-hour period as the MRI experiments (Fig. 4). The blood pressure was relatively stable in both animals, averaging (mean ± SD) 79 ± 5 mm Hg in the C57BL/6J mouse and 60 ± 5 mm Hg in the DBA/2J mouse, consistent with our previous experience with these mouse strains for 1 hour under anesthesia.9
Figure 4.
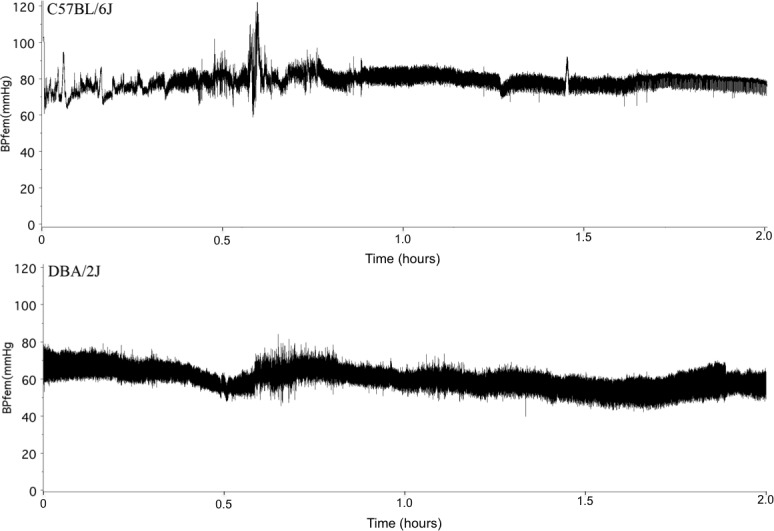
Arterial pressure traces from a 6-month-old C57BL/6J mouse (top) and a 9-month-old DBA/2J mouse (bottom) over a 2-hour period of anesthesia similar to that used in the MRI experiments table.
Discussion
Ocular hypertension and the consequent diminished perfusion pressure available to drive blood through the ocular circulations is the basis for the longstanding ischemic hypothesis of glaucoma. The present study and other investigations of the DBA/2J model support this hypothesis since it develops age-related ocular hypertension, reduced ocular blood flow and the RGC loss and decreased optic nerve axon density seen in human glaucoma. The present study adds to the existing literature by showing that acute pharmacologic IOP reduction with topical dorzolamide in the older DBA/2J mouse is associated with increased retinal and choroidal blood flow.
Dorzolamide is a carbonic anhydrase inhibitor commonly used in glaucoma treatment to lower IOP.27 Its hypotensive effect is mediated by inhibition of aqueous humor production.21 In addition to its hypotensive effect, dorzolamide dilates isolated retinal arterioles28,29 and so it may have a direct vasodilatory effect in vivo. However, although topical dorzolamide reaches the back of the eye,30,31 its ability to increase blood flow in the retina, choroid and optic nerve has not been shown consistently. In rabbits, acute dorzolamide had no effect on choroidal perfusion,32 but chronic dosing increased optic nerve head perfusion in one study33 and had no effect in another.34 For humans, some studies reported no change in retinal blood flow35–37 while others reported an increase.38–41 Similarly, for human optic nerve head blood flow, dorzolamide was reported to have no effect42 or to increase perfusion43 and to flatten the pressure-flow relationship.44 For human choroidal blood flow, modest increases in perfusion indexes were reported.43,45 The discrepancies in the literature are likely due to differences in dosing protocols, and also the inherent ambiguities in the methods used to measure blood flow in the human ocular circulations. However, on balance, it does not appear that dorzolamide has a dramatic hyperemic effect on human retinal or choroidal blood flow.
What then accounts for the blood flow responses in the present study? As ocular blood flow could be affected by instability of systemic blood pressure over the course of the 2-hour MRI experiments, we monitored arterial blood pressure over the same period outside the MRI scanner. We found the arterial blood pressure to be stable over 2 hours under isoflurane anesthesia, consistent with our previous results in larger cohorts of DBA/2J and C57BL/6J (n = 9 each) during 1 hour of isoflurane anesthesia.9 Thus, the changes in ocular blood flow after DZ do not seem to be due to systemic blood pressure instability. By contrast, IOP in the older DBA/2J group was markedly elevated at baseline and declined markedly after dorzolamide. The perfusion pressure ranges for retinal and choroidal pressure-flow autoregulation in the DBA/2J mouse are unknown; however, the perfusion pressure below which retinal and choroidal blood flow respond linearly to perfusion pressure changes is approximately 40 mm Hg in several species.46 Assuming the perfusion pressure was below the autoregulatory cut-off pressure in the older DBA/2J mice at baseline, it is plausible that the increase in perfusion pressure when IOP decreased after DZ would cause the observed increases in retinal and choroidal blood flow.
For the younger DBA/2J group and the C57BL/6J group, the interpretation of the retinal and choroidal blood flow response pattern is less clear. At baseline, their IOPs were similar and relatively low, and did not fall markedly after dorzolamide. Thus, IOP does not explain the reduced baseline retinal blood flow and marginally reduced (P = 0.07 by unpaired t-test) choroidal blood flow in the younger DBA/2J group, nor does IOP explain the fall in choroidal blood flow in the second hour after dorzolamide. The differences in baseline retinal and choroidal blood flows may be due to arterial pressure. Arterial pressures in conscious C57BL/6J and DBA/2J mice are similar and around 100 mm Hg.47,48 Under isoflurane anesthesia, arterial pressure may fall lower in DBA/2J mice than C57BL/6J mice, as suggested by the two animals we tested (Fig. 4); higher IOP and low arterial pressure would obviously contribute to the even lower baseline retinal and choroidal blood flows in the older DBA/2J mice. However, the fall in choroidal blood flow in the DBA/2J and C57BL/6J during the second hour after dorzolamide cannot be explained by perfusion pressure. A possible explanation is washout of an endogenous vasodilator during the first hour hyperemia, but this is speculative.
Conclusions
This study investigated the effects of acute topical application of dorzolamide on IOP and retinal and choroidal blood flow in an animal model of glaucoma. The results support the hypothesis that acute topical dorzolamide decreases intraocular pressure and increases retinal and choroidal blood flow in the older DBA/2J mouse model of glaucoma. Future studies will investigate the effects of chronic dorzolamide treatment on retinal and choroidal blood flow in young and old DBA/2J mice.
Acknowledgments
Supported by the NIH (EY021173); a MERIT award from the Department of Veterans Affairs, a Translational Resource Technology grant and a Pilot grant from the Clinical Translational Science Award (CTSA, parent grant UL1RR025767); and the van Heuven endowment.
Disclosure: S. Chandra, None; E.R. Muir, None; K. Deo, None; J.W. Kiel, None; T.Q. Duong, None
References
- 1. Johnson TV,, Tomarev SI. Rodent models of glaucoma. Brain Res Bull. 2010; 81: 349–358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. John SW,, Smith RS,, Savinova OV,, et al. Essential iris atrophy, pigment dispersion, and glaucoma in DBA/2J mice. Invest Ophthalmol Vis Sci. 1998; 39: 951–962. [PubMed] [Google Scholar]
- 3. Libby RT,, Anderson MG,, Pang IH,, et al. Inherited glaucoma in DBA/2J mice: pertinent disease features for studying the neurodegeneration. Vis Neurosci. 2005; 22: 637–648. [DOI] [PubMed] [Google Scholar]
- 4. Inman DM,, Sappington RM,, Horner PJ,, Calkins DJ. Quantitative correlation of optic nerve pathology with ocular pressure and corneal thickness in the DBA/2 mouse model of glaucoma. Invest Ophthalmol Vis Sci. 2006; 47: 986–996. [DOI] [PubMed] [Google Scholar]
- 5. Scholz M,, Buder T,, Seeber S,, Adamek E,, Becker CM,, Lutjen-Drecoll E. Dependency of intraocular pressure elevation and glaucomatous changes in DBA/2J and DBA/2J-Rj mice. Invest Ophthalmol Vis Sci. 2008; 49: 613–621. [DOI] [PubMed] [Google Scholar]
- 6. McKinnon SJ,, Schlamp CL,, Nickells RW. Mouse models of retinal ganglion cell death and glaucoma. Exp Eye Res. 2009; 88: 816–824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Anderson MG,, Smith RS,, Hawes NL,, et al. Mutations in genes encoding melanosomal proteins cause pigmentary glaucoma in DBA/2J mice. Nat Genet. 2002; 30: 81–85. [DOI] [PubMed] [Google Scholar]
- 8. Chang B,, Smith RS,, Hawes NL,, et al. Interacting loci cause severe iris atrophy and glaucoma in DBA/2J mice. Nat Genet. 1999; 21: 405–409. [DOI] [PubMed] [Google Scholar]
- 9. Lavery WJ,, Muir ER,, Kiel JW,, Duong TQ. Magnetic resonance imaging indicates decreased choroidal and retinal blood flow in the DBA/2J mouse model of glaucoma. Invest Ophthalmol Vis Sci. 2012; 53: 560–564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Perez de Lara MJ,, Santano C,, Guzman-Aranguez A,, et al. Assessment of inner retina dysfunction and progressive ganglion cell loss in a mouse model of glaucoma. Exp Eye Res. 2014; 122: 40–49. [DOI] [PubMed] [Google Scholar]
- 11. Soto I,, Pease ME,, Son JL,, Shi X,, Quigley HA,, Marsh-Armstrong N. Retinal ganglion cell loss in a rat ocular hypertension model is sectorial and involves early optic nerve axon loss. Invest Ophthalmol Vis Sci. 2011; 52: 434–441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Williams PA,, Howell GR,, Barbay JM,, et al. Retinal ganglion cell dendritic atrophy in DBA/2J glaucoma. PLoS One. 2013; 8: e72282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Nguyen JV,, Soto I,, Kim KY,, et al. Myelination transition zone astrocytes are constitutively phagocytic and have synuclein dependent reactivity in glaucoma. Proc Natl Acad Sci U S A. 2011; 108: 1176–1181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Baltan S,, Inman DM,, Danilov CA,, Morrison RS,, Calkins DJ,, Horner PJ. Metabolic vulnerability disposes retinal ganglion cell axons to dysfunction in a model of glaucomatous degeneration. J Neurosci. 2010; 30: 5644–5652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Burroughs SL,, Kaja S,, Koulen P. Quantification of deficits in spatial visual function of mouse models for glaucoma. Invest Ophthalmol Vis Sci. 2011; 52: 3654–3659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Rangarajan KV,, Lawhn-Heath C,, Feng L,, Kim TS,, Cang J,, Liu X. Detection of visual deficits in aging DBA/2J mice by two behavioral assays. Curr Eye Res. 2011; 36: 481–491. [DOI] [PubMed] [Google Scholar]
- 17. Saleh M,, Nagaraju M,, Porciatti V. Longitudinal evaluation of retinal ganglion cell function and IOP in the DBA/2J mouse model of glaucoma. Invest Ophthalmol Vis Sci. 2007; 48: 4564–4572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Calkins DJ,, Horner PJ,, Roberts R,, Gradianu M,, Berkowitz BA. Manganese-enhanced MRI of the DBA/2J mouse model of hereditary glaucoma. Invest Ophthalmol Vis Sci. 2008; 49: 5083–5088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Schuettauf F,, Quinto K,, Naskar R,, Zurakowski D. Effects of anti-glaucoma medications on ganglion cell survival: the DBA/2J mouse model. Vision Res. 2002; 42: 2333–2337. [DOI] [PubMed] [Google Scholar]
- 20. Wong AA,, Brown RE. A neurobehavioral analysis of the prevention of visual impairment in the DBA/2J mouse model of glaucoma. Invest Ophthalmol Vis Sci. 2012; 53: 5956–5966. [DOI] [PubMed] [Google Scholar]
- 21. Sugrue MF. Pharmacological and ocular hypotensive properties of topical carbonic anhydrase inhibitors. Prog Retin Eye Res. 2000; 19: 87–112. [DOI] [PubMed] [Google Scholar]
- 22. Muir ER,, Duong TQ. MRI of retinal and choroidal blood flow with laminar resolution. NMR Biomed. 2011; 24: 216–223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Duong TQ. Magnetic resonance imaging of the retina: from mice to men. Magn Reson Med. 2014; 71: 1526–1530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Shih YY,, Wang L,, De La Garza BH,, et al. Quantitative retinal and choroidal blood flow during light, dark adaptation and flicker light stimulation in rats using fluorescent microspheres. Curr Eye Res. 2013; 38: 292–298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Pease ME,, Cone FE,, Gelman S,, Son JL,, Quigley HA. Calibration of the TonoLab tonometer in mice with spontaneous or experimental glaucoma. Invest Ophthalmol Vis Sci. 2011; 52: 858–864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Wang WH,, Millar JC,, Pang IH,, Wax MB,, Clark AF. Noninvasive measurement of rodent intraocular pressure with a rebound tonometer. Invest Ophthalmol Vis Sci. 2005; 46: 4617–4621. [DOI] [PubMed] [Google Scholar]
- 27. Strahlman E,, Tipping R,, Vogel R. A double-masked randomized 1-year study comparing dorzolamide (Trusopt), timolol, and betaxolol. International Dorzolamide Study Group. Arch Ophthalmol. 1995; 113: 1009–1016. [DOI] [PubMed] [Google Scholar]
- 28. Josefsson A,, Sigurdsson SB,, Bang K,, Eysteinsson T. Dorzolamide induces vasodilatation in isolated pre-contracted bovine retinal arteries. Exp Eye Res. 2004; 78: 215–221. [DOI] [PubMed] [Google Scholar]
- 29. Kehler AK,, Holmgaard K,, Hessellund A,, Aalkjaer C,, Bek T. Variable involvement of the perivascular retinal tissue in carbonic anhydrase inhibitor induced relaxation of porcine retinal arterioles in vitro. Invest Ophthalmol Vis Sci. 2007; 48: 4688–4693. [DOI] [PubMed] [Google Scholar]
- 30. Kadam RS,, Jadhav G,, Ogidigben M,, Kompella UB. Ocular pharmacokinetics of dorzolamide and brinzolamide after single and multiple topical dosing: implications for effects on ocular blood flow. Drug Metab Dispos. 2011; 39: 1529–1537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Inoue J,, Oka M,, Aoyama Y,, et al. Effects of dorzolamide hydrochloride on ocular tissues. J Ocul Pharmacol Ther. 2004; 20: 1–13. [DOI] [PubMed] [Google Scholar]
- 32. Reitsamer HA,, Bogner B,, Tockner B,, Kiel JW. Effects of dorzolamide on choroidal blood flow ciliary blood flow, and aqueous production in rabbits. Invest Ophthalmol Vis Sci. 2009; 50: 2301–2307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Barnes GE,, Li B,, Dean T,, Chandler ML. Increased optic nerve head blood flow after 1 week of twice daily topical brinzolamide treatment in Dutch-belted rabbits. Surv Ophthalmol. 2000; 44 (suppl 2): S131–140. [DOI] [PubMed] [Google Scholar]
- 34. Tamaki Y,, Araie M,, Muta K. Effect of topical dorzolamide on tissue circulation in the rabbit optic nerve head. Jpn J Ophthalmol. 1999; 43: 386–391. [DOI] [PubMed] [Google Scholar]
- 35. Grunwald J,, Mathur S,, DuPont J. Effects of dorzolamide hydrochloride 2% on the retinal circulation. Acta Ophthalmol Scand. 1997; 75: 236–238. [DOI] [PubMed] [Google Scholar]
- 36. Bergstrand IC,, Heijl A,, Harris A. Dorzolamide and ocular blood flow in previously untreated glaucoma patients: a controlled double-masked study. Acta Ophthalmol Scand. 2002; 80: 176–182. [DOI] [PubMed] [Google Scholar]
- 37. Harris A,, Ciulla TA,, Pratt LM,, et al. The effects of dorzolamide on choroidal and retinal perfusion in non-exudative age related macular degeneration. Br J Ophthalmol. 2003; 87: 753–757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Martinez A,, Gonzalez F,, Capeans C,, Perez R,, Sanchez-Salorio M. Dorzolamide effect on ocular blood flow. Invest Ophthalmol Vis Sci. 1999; 40: 1270–1275. [PubMed] [Google Scholar]
- 39. Arend O,, Harris A,, Wolter P,, Remky A. Evaluation of retinal haemodynamics and retinal function after application of dorzolamide, timolol and latanoprost in newly diagnosed open-angle glaucoma patients. Acta Ophthalmol Scand. 2003; 81: 474–479. [DOI] [PubMed] [Google Scholar]
- 40. Pedersen DB., Koch Jensen P,, la Cour M,, et al. Carbonic anhydrase inhibition increases retinal oxygen tension and dilates retinal vessels. Graefes Arch Clin Exp Ophthalmol. 2005; 243: 163–168. [DOI] [PubMed] [Google Scholar]
- 41. Simsek T,, Yanik B,, Conkbayir I,, Zilelioglu O. Comparative analysis of the effects of brimonidine and dorzolamide on ocular blood flow velocity in patients with newly diagnosed primary open-angle glaucoma. J Ocul Pharmacol Ther. 2006; 22: 79–85. [DOI] [PubMed] [Google Scholar]
- 42. Pillunat LE,, Bohm AG,, Koller AU,, Schmidt KG,, Klemm M,, Richard G. Effect of topical dorzolamide on optic nerve head blood flow. Graefes Arch Clin Exp Ophthalmol. 1999; 237: 495–500. [DOI] [PubMed] [Google Scholar]
- 43. Fuchsjager-Mayrl G,, Wally B,, Rainer G,, et al. Effect of dorzolamide and timolol on ocular blood flow in patients with primary open angle glaucoma and ocular hypertension. Br J Ophthalmol. 2005; 89: 1293–1297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Fuchsjager-Mayrl G,, Georgopoulos M,, Hommer A,, et al. Effect of dorzolamide and timolol on ocular pressure: blood flow relationship in patients with primary open-angle glaucoma and ocular hypertension. Invest Ophthalmol Vis Sci. 2010; 51: 1289–1296. [DOI] [PubMed] [Google Scholar]
- 45. Zeitz O,, Matthiessen ET,, Reuss J,, et al. Effects of glaucoma drugs on ocular hemodynamics in normal tension glaucoma: a randomized trial comparing bimatoprost and latanoprost with dorzolamide [ISRCTN18873428]. BMC Ophthalmol. 2005; 5: 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Kiel J. Local determinants of ocular blood flow. : Schmetterer L,, Kiel J, Ocular Blood Flow. Berlin: Springer; 2012. [Google Scholar]
- 47. Campen MJ,, Tagaito Y,, Jenkins TP,, Smith PL,, Schwartz AR,, O'Donnell CP. Phenotypic differences in the hemodynamic response during REM sleep in six strains of inbred mice. Physiol Genomics. 2002; 11: 227–234. [DOI] [PubMed] [Google Scholar]
- 48. Campen MJ,, Tagaito Y,, Jenkins TP,, Balbir A,, O'Donnell CP. Heart rate variability responses to hypoxic and hypercapnic exposures in different mouse strains. J Appl Physiol (1985). 2005; 99: 807–813. [DOI] [PubMed] [Google Scholar]