

SUMMARY
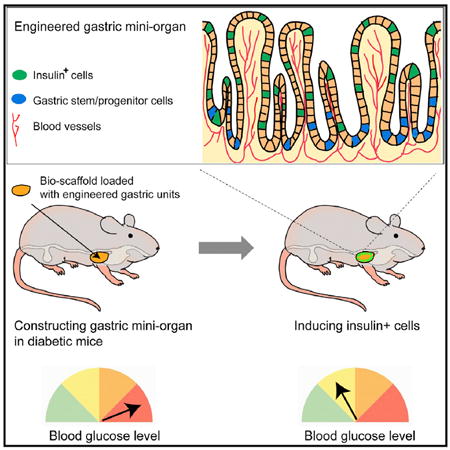
The gastrointestinal (GI) epithelium is a highly regenerative tissue with the potential to provide a renewable source of insulin+ cells after undergoing cellular reprogramming. Here, we show that cells of the antral stomach have a previously unappreciated propensity for conversion into functional insulin-secreting cells. Native antral endocrine cells share a surprising degree of transcriptional similarity with pancreatic β cells, and expression of β cell reprogramming factors in vivo converts antral cells efficiently into insulin+ cells with close molecular and functional similarity to β cells. Induced GI insulin+ cells can suppress hyperglycemia in a diabetic mouse model for at least 6 months and regenerate rapidly after ablation. Reprogramming of antral stomach cells assembled into bioengineered mini-organs in vitro yielded transplantable units that also suppressed hyperglycemia in diabetic mice, highlighting the potential for development of engineered stomach tissues as a renewable source of functional β cells for glycemic control.
Graphical Abstract
INTRODUCTION
Major progress has been made in recent years to produce functional insulin+ cells for cell replacement therapies to treat diabetes. These regenerative technologies include directed differentiation of embryonic stem cells and direct conversion from non-β cells such as liver cells, acinar cells, and others (Hebrok, 2012; Johannesson et al., 2015; Nostro and Keller, 2012; Schiesser and Wells, 2014; Zhou and Melton, 2008). However, because ongoing pathological conditions in diabetes inflict continued damage to native and transplanted β cells (Azzi et al., 2010; Butler et al., 2003; Lakey et al., 2006; Rahier et al., 2008), it is desirable to develop a regenerative system where β cells can be produced in a renewable fashion to counteract β cell loss. The gastrointestinal (GI) tissues are potential sources for such continued generation of β cells. The stomach and intestine are unique among endodermal organs in that they harbor large numbers of adult stem/progenitor cells that constantly produce epithelial cells, including hormone-secreting enteroendocrine cells (Barker et al., 2007, 2010; May and Kaestner, 2010; Schonhoff et al., 2004a). Both organs are developmentally related to the pancreas, arising in adjacent embryonic domains (Offield et al., 1996). Development of gut enteroendocrine and pancreatic endocrine cells also depends on common critical factors, such as Ngn3 (also known as Neurog3) (Gu et al., 2002; Jenny et al., 2002; Lee et al., 2002). Recent studies showed that intestinal cells could be converted into insulin+ cells with either endocrine-specific deletion of FoxO1 or ubiquitous expression of NPM reprogramming factors (Ngn3, Pdx1, and Mafa) (Bouchi et al., 2014; Chen et al., 2014; Talchai et al., 2012a). Although these studies revealed the feasibility of deriving β-like cells from the intestine, critical barriers remain in developing these approaches into future regenerative therapies. FoxO1 plays a critical role in protecting β cells from cellular stress (Kitamura et al., 2005; Talchai et al., 2012b), and deletion or suppression of FoxO1 in pancreatic β cells could result in β cell failure (Talchai et al., 2012b; Talchai and Accili, 2015). Moreover, although NPM factors induce insulin+ cells in the intestine, the induced cells appear to lack certain important β cell genes such as Nkx6.1 and exhibit reduced glucose responsiveness compared with pancreatic β cells (Chen et al., 2014).
We sought to devise improved strategies to derive functional insulin-secreting (insulin+) cells from GI tissues and to harness the regenerative capacity of these tissues as a renewable source of β cells. We report the surprising finding that NPM factors reprogram enteroendocrine cells from the antral stomach more efficiently into functional insulin+ cells compared with enteroendocrine cells from the intestine. Induced antral insulin+ cells also express key β cell factors, including Nkx6.1 and Prohormone convertase 2 (PC2), which intestinal insulin+ cells lack. Our data reveal that native antral enteroendocrine cells share a surprising level of transcriptional similarity with pancreatic β cells. Further, the intestine-specific Cdx2 gene can block efficient β cell reprogramming. Thus, intrinsic molecular differences between antral stomach and intestinal enteroendocrine cells could contribute to the differential reprogramming outcomes. To explore the therapeutic potential of gastric tissue as a source of inducible β cells, we created bioengineered stomach mini-organs; upon transplantation and sphere formation, these structures produced renewable insulin+ cells that reverse hyperglycemia in vivo. Our studies reveal antral stomach tissue as a previously unrecognized source that is highly amenable to reprogramming toward functional insulin+ cells. We also provide proof of principle evidence that bioengineered gastric tissue could serve as a renewable source of β cells for glycemic control.
RESULTS
NPM Factors Efficiently Reprogram GI Enteroendocrine Cells to Insulin+ Cells, with Antral Stomach Showing the Highest Induction Efficiency
Previous studies of reprogramming GI tissues to insulin+ cells have used either deletion of FoxO1 or expression of NPM factors (Ngn3, Pdx1, and Mafa). Surprisingly, no insulin+ cells were reported from stomach with either approach (Chen et al., 2014; Talchai et al., 2012a). To revisit this important question, we performed additional reprogramming experiments in the GI tract. Using adenoviral infection of cultured mouse antral stomach organoids, we observed that the NPM factors are highly effective at inducing insulin expression whereas the other reprogramming factors tested, including Pax4, Insm1, Nkx6.1, and Mafa, are not effective (Figure S1). Based on this observation, we constructed new transgenic mouse lines (TetO-NPMcherry) in which the inducible TetO promoter drives polycistronic expression of NPM factors and the red fluorescent protein Cherry (Figure 1A). Global expression of NPM factors leads to rapid animal death due to hypoglycemia (unpublished observations). To enable long-term observation and comparison of induced insulin+ cells from different GI regions, we targeted NPM factors to the GI enteroendocrine lineage, which shares molecular and developmental similarity with pancreatic endocrine cells (Habib et al., 2012; May and Kaestner, 2010; Schonhoff et al., 2004a), making it an excellent target for β cell conversion. We crossed the TetO-NPMcherry line with the bacterial artificial chromosome (BAC)-transgenic Ngn3-Cre line (Schonhoff et al., 2004b) and the knockin Rosa-floxed-rtTA line (Jackson Laboratory) to derive a triple-transgenic line we call NRT (Figure 1A). The well-described Ngn3-Cre line labels all enteroendocrine cells in the intestine and the majority of antral stomach enteroendocrine cells (Schonhoff et al., 2004b) (Figure S1).
Figure 1. NPM Factors Efficiently Reprogram Gastrointestinal Endocrine Cells to Insulin+ Cells with the Highest Induction Efficiency in Antral Stomach.
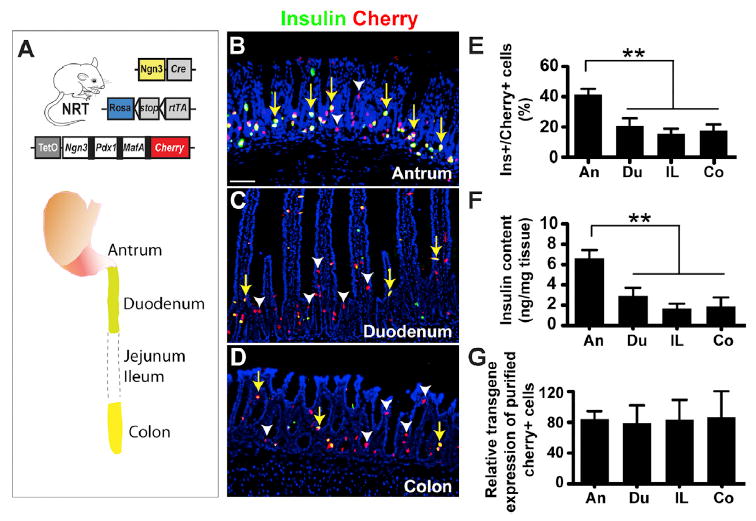
(A) Diagram of the triple-cross transgenic mouse line, referred to as NRT (Ngn3-Cre; Rosa-floxed-rtTA; Teto-NMPcherry). Ngn3-cre is used to target inducible expression of the NPM factors (Ngn3, Pdx1, and Mafa) into the enteroendocrine cells of the antral stomach and the intestine. Black bars in Teto-NPMcherry indicate 2A peptides used to mediate polycistronic expression.
(B–G) Doxycycline treatment of NRT animals yielded many insulin+cherry+ cells from the antral stomach (B), the duodenum (C), and the colon (D), among other GI regions. Quantitation showed a higher induction efficiency of insulin+ cells in antrum compared with duodenum (du), ileum (IL), and colon (Co) (E, n = 3 animals, p = 0.0026). Antrum tissue also has higher insulin content (F, n = 3 animals, p = 0.0046). Using FACS-purified cherry+ cells, the expression level of transgenes in the endocrine population was found to be comparable (G), n = 3 animals). Scale bar, 100 μm. Yellow arrows indicate insulin+cherry+ cells; white arrowheads indicate insulin−cherry+ cells.
See also Figure S1.
After doxycycline (Dox) treatment of NRT animals for 10 days, we observed numerous insulin+ cells in the antral stomach and along the entire length of the intestine (Figures 1B–1D, yellow arrows). The fundus region of the stomach contains relatively few Ngn3+ endocrine cells, and very few of these expressed insulin, suggesting that fundal cells resist NPM-mediated conversion (Figure S1). Quantitative analysis showed significantly higher reprogramming efficiency in the antrum (41.5% ± 8.5%, mean ± SD) than in the proximal (duodenum, 21.4% ± 6.7%), middle (ileum, 14.6% ± 3.3%), or distal (colon, 15.5% ± 3.4%) intestine (Figure 1E). The antral stomach also contains substantially higher levels of insulin protein compared with the intestine (Figure 1F), even though levels of reprogramming factor expression in fluorescence-activated cell sorting (FACS)-purified cherry+ cells from the antrum and different intestinal regions are comparable (Figure 1G).
Enteroendocrine cells in the stomach and intestine include multiple subtypes based on hormone expression (Habib et al., 2012; May and Kaestner, 2010; Schonhoff et al., 2004a). To evaluate whether insulin+ cells are preferentially induced in certain subtypes, we quantified seven major enteroendocrine subtypes before and after induction of insulin+ cells (Figure S1). All endocrine subtypes we examined were reduced upon doxycycline treatment, with the exception of serotonin+ cells, which do not originate from the Ngn3+ lineage (Schonhoff et al., 2004b) (Figure S1). These data indicate that insulin+ cells in both stomach and duodenum arise from multiple endocrine subtypes and/or their common progenitors. We also found the vast majority of induced GI insulin+ cells to be mono-hormonal (Figure S1). These data collectively show that NPM factors can robustly reprogram GI endocrine cells into insulin+ cells, with the highest reprogramming efficiency in the antral stomach.
Induced GI Insulin+ Cells Can Reverse Hyperglycemia Long-Term and Regenerate Rapidly upon Ablation
To test whether the induced GI insulin+ cells can secrete insulin and reverse hyperglycemia, we ablated pancreatic β cells in NRT mice with streptozotocin (STZ), which renders the animals hyperglycemic. Upon Dox treatment and induction of insulin+ cells in the GI tract, hyperglycemia was rapidly reversed and blood glucose levels remained normal for as long as we tracked them (Figure 2A, up to 6 months). In contrast to control animals, which died with hyperglycemia within 8 weeks, nearly every Dox-treated animal was rescued (Figure 2B). Consistent with this effect, intraperitoneal glucose tolerance test (IPGTT) showed substantial improvement after doxycycline induction (Figure 2C) and near-normal blood insulin level in STZ-ablated and Dox-induced animals (Figure 2D).
Figure 2. Induced Insulin+ Cells from the GI Tract Can Reverse Hyperglycemia Long-Term and Regenerate Rapidly.
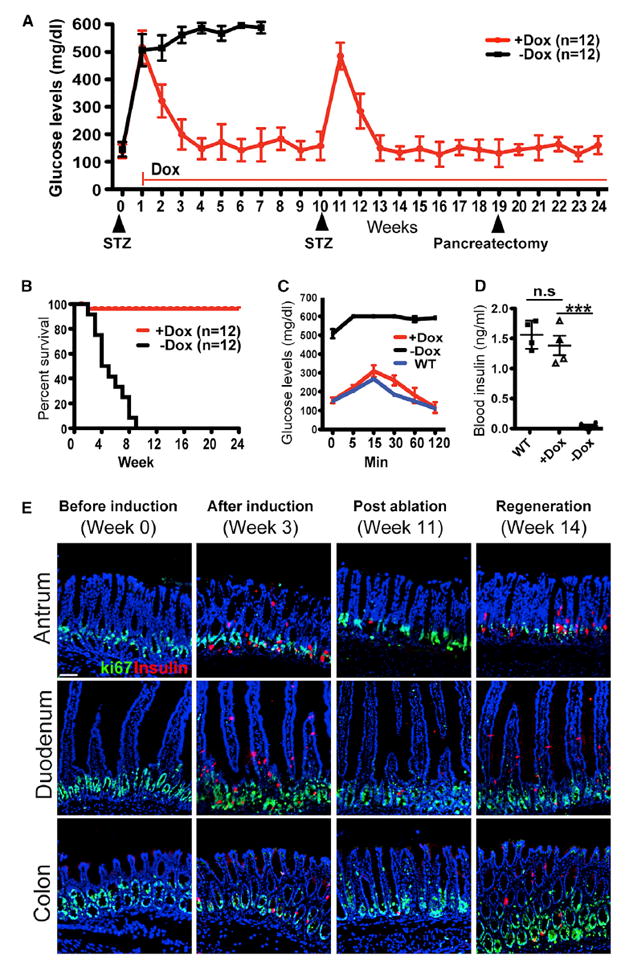
(A) Glucose monitoring of hyperglycemic NRT animals over 6 months. Streptozotocin (STZ) was used to ablate endogenous pancreatic β cells and create hyperglycemia. Doxycycline (Dox) was administered continuously from week 1 onward (red line). Compared with persistent hyperglycemia and death of control animals (–Dox group, black squares), Dox treatment led to long-term suppression of hyperglycemia (+Dox group, red circles). A second round of STZ ablation was conducted at week 10 to evaluate the regenerative capacity of this experimental system. The ensuing hyperglycemia was suppressed again by week 13. Pancreatectomy was performed on week 19 to remove ~80% of the pancreas. No significant effect on blood glucose levels was observed.
(B–D) Dox treatment and induction of insulin+ cells led to significant improvement in the survival of hyperglycemic NRT animals (B, n = 12 animals in each group). Glucose tolerance tests showed near-normal responses for Dox-treated animals (C, n = 4 animals in each group). The blood insulin levels of the induced animals are comparable with that of wild-type animals and significantly higher than non-induced animals (D, n = 4 animals in each group, p < 0.001).
(E) Immunohistochemistry showed before and after induction of insulin+ cells (first and second panel, respectively). STZ treatment was used at week 11 to ablate the induced insulin+ cells from the GI tract (third panel). Insulin+ cells were regenerated rapidly 3 weeks later (last panel). Ki67 staining labels the proliferating stem/progenitor cell compartment at the base of the glands. Scale bar, 100 μm.
All quantitative data presented as mean ± SD. Statistical significance was evaluated with the Student’s t test (***p < 0.001). See also Figures S2 and S3.
To confirm that rescue from hyperglycemia results from induction of insulin+ cells in the GI tract, we surveyed insulin expression in other Ngn3-expressing tissues including the brain, testis, and pancreas. No insulin+ cells were found in the brain or testis (data not shown). In the pancreas of NRT animals, STZ treatment led to near complete ablation of endogenous β cells (Figure S2), but Dox treatment induced insulin in glucagon+ cells, which comprise the majority of islet cells after β cell ablation (Figure S2). These glucagon+insulin+ cells do not, however, express other β cell factors such as Glut2 and Nkx6.1, and their insulin expression level is significantly lower than in native β cells (Figure S2). To assess the possibility that these glucagon+insulin+ cells may nevertheless contribute to reversal of hyperglycemia after Dox induction in NRT animals, we resected ~80% of the pancreas and thus most glucagon+insulin+ cells. No significant changes in blood glucose level followed (Figure 2A). The remnant 20% pancreas showed 0.15 ± 0.03 μg of total insulin (mean ± SD), significantly below the insulin content of antrum (1.89 ± 0.36 μg) or duodenum (1.20 ± 0.63 μg; Figure S4). In comparison, a normal mouse pancreas contains ~10 μg insulin, although only a fraction of the β cell mass is required to maintain normoglycemia (Bonner-Weir, 2000). These data collectively indicate that induced insulin+ cells from the GI tract are the main source of secreted insulin that led to long-term reversal of hyperglycemia.
The GI tract is a highly regenerative organ, with resident glandular stem cells continuously producing new epithelial cells (Barker et al., 2010; Barker et al., 2007). To evaluate the capacity of GI β cell regeneration from the stem cell compartment, we conducted a second round of STZ treatment (Figures 2A and 2E). Similar to pancreatic β cells, induced insulin+ cells from the antrum and intestine were sensitive to the toxin and disappeared, leading to hyperglycemia (Figures 2A and 2E). However, the diabetic state was again rapidly reversed, concomitant with the reappearance of GI insulin+ cells (Figure 2E). These data illustrate the high regenerative capacity of the genetically engineered GI tissues and their ability to sustain injuries and maintain suppression of hyperglycemia.
We also evaluated the lifespan of antral and intestinal insulin+ cells and their relative contributions toward glycemic control (Figure S3). In a pulse-chase experiment, GI insulin+ cells were first induced by Dox treatment, followed by Dox withdrawal. Intestinal insulin+ cells disappeared within 7 days, whereas stomach insulin+ cells persisted for more than 20 days, consistent with estimated turnover rates of the native intestinal and antral epithelia (Karam and Leblond, 1993; Lehy and Willems, 1976; Messier and Leblond, 1960; Thompson et al., 1990). Antral insulin+ cells continued to suppress hyperglycemia after intestinal insulin+ cells had disappeared (Figure S3). Thus, antral insulin+ cells have a longer lifespan than their intestinal counterparts and can suppress hyperglycemia independently.
Antral Insulin+ Cells Bear Close Molecular and Functional Resemblance to Pancreatic β Cells
Immunohistochemistry revealed that induced insulin+ cells from the antral stomach and the proximal and distal intestine all express β cell factors such as c-peptide, glucose transporter 2 (Glut2, or Slc2a2), prohormone convertase 1/3 (PC1/3), and Pax6 (Figure 3A, quantification shown in Figure S4). However, other key β cell genes, including Nkx6.1, Nkx2.2, and prohormone convertase 2 (PC2), are expressed exclusively or predominantly in antral insulin+ cells (Figure 3A, quantitation shown in Figure S4). qPCR analysis further confirmed that many β cell factors are expressed at substantially higher levels in antral insulin+ cells than in duodenal or colonic insulin+ cells (Figure S4). Endogenous Pdx1, but not endogenous Mafa, is expressed in the native duodenum and antrum (Figure S4), as previously reported (Habib et al., 2012; Offield et al., 1996). Endogenous Mafa is activated strongly in antral insulin+ cells, but only weakly in duodenal and colonic insulin+ cells (Figure S4), whereas endogenous Pdx1 is induced in both antral and intestinal insulin+ cells (Figure S4). In contrast, endogenous Ngn3 is not induced (Figure S4). We observed continued expression of FoxO1 expression in both antral and intestinal insulin+ cells (Figure S4).
Figure 3. Induced Insulin+ Cells from the Antral Stomach More Closely Resemble β Cells Molecularly and Functionally.
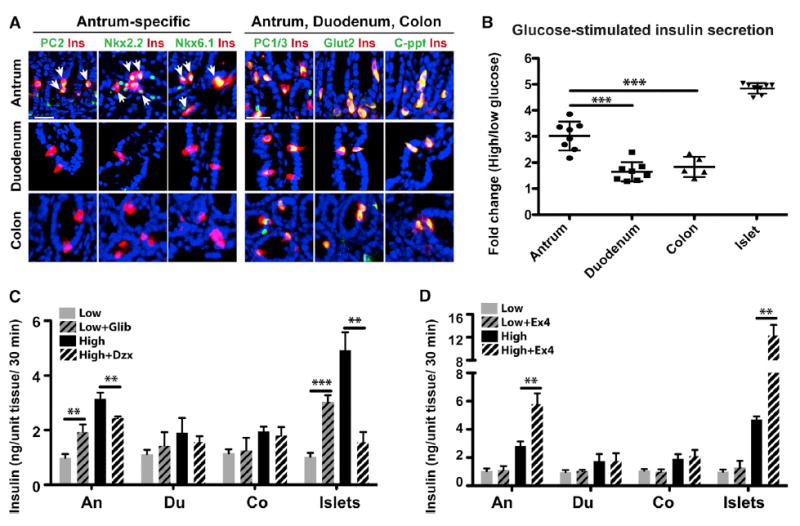
(A) Immunohistochemistry showed that induced insulin+ cells from the antrum express β cell genes Nkx6.1, Nkx2.2, and Prohormone convertase 2 (PC2), which are largely absent from duodenum and colon insulin+ cells. In contrast, Prohormone convertase 1/3 (PC1/3), glucose transporter 2 (Glut2), and c-peptide (c-ppt) are expressed commonly in antral, duodenal, and colonic insulin+ cells. Arrows indicate antral insulin+ that are PC2+, Nkx2.2+, and Nkx6.1+. Scale bar, 50 μm.
(B) Glucose stimulated insulin secretion (GSIS) in vitro. Antral tissues have significantly higher glucose responsiveness, defined as fold increase of insulin release at high versus low glucose conditions, compared with duodenal and colonic tissues (n = 8, p < 0.001).
(C and D) The antidiabetic drug Glibenclamide (Glib) stimulated insulin release from the antral insulin+ cells whereas Diazoxide (Dzx), a suppressor of insulin release, reduced antral insulin secretion (C, n = 4). In contrast, duodenal and colonic insulin+ cells do not respond to Glib or Dzx (C). Antral insulin+ cells also respond to Exendin-4 (Ex4) with enhanced insulin secretion at high glucose levels whereas duodenal and colonic cells do not respond to Exendin (D, n = 4).
All quantitative data presented as mean ± SD. Statistical significance was evaluated with the Student’s t test (*p < 0.05, **p < 0.01, and ***p < 0.001). See also Figure S4.
To assess functional properties of induced insulin+ cells from the stomach and the intestine, we harvested whole epithelial tissues from the antrum, duodenum, and colon of NRT animals after 10 days of Dox treatment. In vitro glucose-stimulated insulin secretion assays were performed with each sample at low-glucose (1.7 mM) and high-glucose (20.2 mM) conditions. Our data showed that although all GI insulin+ cells can respond to high glucose (Figure 3B), the responsiveness of antral insulin+ cells is significantly higher than that of duodenal and colonic insulin+ cells (Figure 3B; data standardized as high-glucose versus low-glucose response ratio: 3.02 ± 0.55 for antrum, 1.65 ± 0.37 for duodenum, and 1.61 ± 0.46 for colon).
To further evaluate the function of induced GI insulin+ cells, we tested their physiological response to glibenclamide (Glib), an anti-diabetic drug that binds to Sur1 and inhibits the ATP-sensitive potassium channel in β cells. Glib treatment led to insulin release from antral, but not from duodenal or colonic, insulin+ cells (Figure 3C). Conversely, treatment with Diazoxide (Dzx), a potassium channel activator, suppressed insulin release from antral insulin+ cells, whereas duodenal and colonic cells showed no response (Figure 3C). Moreover, antral insulin+ cells responded to exendin-4, an antidiabetic drug that activates glucagon-like-peptide receptor (Glp1R), leading to increased insulin release at high glucose concentrations (Figure 3D), whereas duodenal and colonic insulin+ did not respond (Figure 3D). Consistent with these physiological data, antral insulin+ cells express significantly higher levels of Sur1 and Glp1R, compared with duodenal and colonic insulin+ cells (Figure S4).
Thus, molecular and physiological studies together indicate that antral endocrine cells can be reprogrammed efficiently into insulin+ cells that resemble pancreatic β cells, whereas conversion from intestinal endocrine cells is comparatively incomplete.
Native Antral Endocrine Cells Share Substantial Transcriptional Similarity with Pancreatic β Cells
What mechanisms might underlie the significant difference? One long-standing hypothesis postulates that the more transcriptional and epigenetic similarities two cells share, the easier it is to interconvert them (Graf and Enver, 2009; Gurdon and Melton, 2008). Transcriptional studies of specific intestinal endocrine populations have been reported (Egerod et al., 2012; Habib et al., 2012), but transcriptomes of antral endocrine cells remain uncharacterized. We therefore profiled the transcriptomes of enteroendocrine cells from the antrum, duodenum, and colon and assessed their similarity to pancreatic β cells. We used Ngn3-GFP reporter mice to isolate enteroendocrine cells from the different GI regions (Lee et al., 2002); Ngn3 expression in the gut is transient and restricted to endocrine progenitors (Jenny et al., 2002; Lee et al., 2002). Ngn3-GFP labels a mixture of chromogranin− (Chga−) and chromogranin+ (Chga+) cells, representing immature and mature endocrine cells, respectively (Lee et al., 2002) (Figure 4A). Our quantitation showed that the relative proportions of GFP+Chga− and GFP+Chga+ cells are comparable in antral stomach, duodenum, and colon (Figure S5). GFP+ cells purified by FACS from the different GI regions (Figure 4B) constitute ~1%–2% of the total cell population (Figure 4B), consistent with the estimated prevalence of gut endocrine cells (Schonhoff et al., 2004a).
Figure 4. Enteroendocrine Cells of the Antral Stomach Share Substantial Transcriptional Similarity with Pancreatic β Cells.
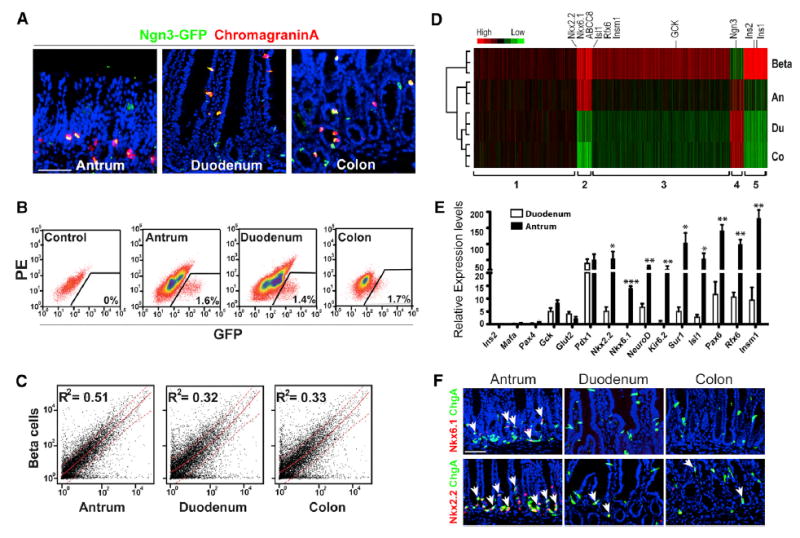
(A) Immunohistochemistry showing distribution of GFP+ in the GI tract of the Ngn3-GFP mouse line. The GFP+ cells include both relatively immature (GFP+Chromogranin−) and more mature enteroendocrine cells (GFP+Chromogranin+). Scale bar, 50 μm.
(B and C) Ngn3-GFP+ cells were purified by FACS from antrum, duodenum, and colon (B). Scatterplots of transcriptome comparisons between pancreatic β cells and the GI enteroendocrine populations (C). Antral enteroendocrine cells show a greater similarity with β cells.
(D and E) Analysis of 2,398 β cell-enriched genes showed a general trend of elevated expression in antral enteroendocrine cells compared with duodenal and colonic enteroendocrine cells (D). In particular, antral enteroendocrine cells share a group of genes (group 2) with β cells (D) that are enriched for factors important in β cell development and function (E). Quantitative data presented as mean ± SD. Statistical significance was evaluated with the Student’s t test (*p < 0.05, **p < 0.01, and ***p < 0.001).
(F) Immunohistochemistry showed that Nkx6.1 is present in a population of Chga+ enteroendocrine cells in the antrum, but not expressed in duodenum or colon (top, arrows). Nkx2.2 is expressed in a majority of Chga+ enteroendocrine cells in the antrum and a minority of Chga+ cells in the duodenum and colon (F, bottom, arrows). Scale bar, 50 μm.
See also Figure S5.
We generated global transcriptome data from the purified cells with Illumina arrays. Comparative analyses showed that endocrine cells from the proximal and distal intestine are more similar to each other and less similar to antral endocrine cells (Figure S5, Spearman correlation coefficients: 0.91 [duodenum versus colon], 0.82 [antrum versus duodenum], and 0.80 [antrum versus colon]). The overall similarity of proximal and distal intestine endocrine cells is high and consistent with published studies (Egerod et al., 2012; Habib et al., 2012) (1,470 differentially expressed genes listed in Table S3). We performed pairwise comparison of the three GI endocrine populations with our published transcriptome data of β cells, which was obtained by FACS purification from the islets of MIP-GFP animals (Li et al., 2014b). This analysis showed overall higher transcriptional similarity between antral and β cells than between intestinal and β cells (Figures 4C and S5, Spearman correlation coefficients: 0.72 [antrum versus β], 0.57 [duodenum versus β], and 0.57 [colon versus β]; Steiger’s Z-test for dependent correlations: p = 6.5 × 10−185). Thus, although enteroendocrine cells from the antrum, duodenum, and colon are more similar to each other than they are to pancreatic β cells, β cells appear to share more transcriptional similarity with antral enteroendocrine cells than intestinal enteroendocrine cells.
To evaluate the expression of β cell-enriched genes in GI enteroendocrine cells, we focused analysis on a collection of 2,398 genes that show higher expression in β cells than in acinar cells (Li et al., 2014b). Antral enteroendocrine cells showed higher expression of many β cell-enriched genes (Figure 4D, group 2 and 3 genes; Table S2) compared with intestinal enteroendocrine cells. In particular, many genes critical for β cell development and function, such as Nkx6.1, Nkx2.2, NeuroD1, Isl1, Rfx6, Insm1, Sur1 (ABCC8), and Glucokinase (GCK), are enriched in antral, compared with duodenal or colonic, enteroendocrine cells (Figures 4E and S5). Immunohistochemistry showed Nkx6.1 expression in a subset of antral GFP+ cells (24.9% ± 3.5%, mean ± SD), but not in the duodenum or colon (Figure 4F). The vast majority of antral Nkx6.1+ cells also express Chga (94.7% ± 3.1%) (Figures 4F and S5). Nkx2.2 is expressed in a majority of GFP+ cells in the antrum (57.2% ± 4.7%), but only in a minority of duodenal (18.7% ± 2.7%) or colonic (23.4% ± 4.3%) Chga+ cells (Figure 4F). Most Nkx2.2+ cells express Chga (69.4% ± 3.4%, 64.0% ± 5.1%, and 65.5% ± 8.3% in antrum, duodenum, and colon, respectively) (Figure 4F; Figure S5). Gene Ontology analyses show that whereas enteroendocrine cells from all GI regions are enriched for pathways involved in regulation of hormone secretion, G-protein-coupled receptor signaling, and vesicle-mediated transport, antral enteroendocrine cells are enriched specifically for the “glucose homeostasis” module (Figure S5; Table S2). Together, these studies reveal a surprising intrinsic difference between endocrine cell populations from the antral stomach and intestine, which likely contributes to their differential capacity for β cell reprogramming.
The Intestine-Specific Gene Cdx2 Can Inhibit β Cell Conversion
In a prior study of acinar to β cell conversion, we showed that persistent expression of acinar cell fate regulators Ptf1a and Nr5a2 blocks acquisition of β cell fate (Li et al., 2014c). Cdx2 is an intestine-specific master regulator gene (Gao et al., 2009), and its persistent expression in intestinal insulin+ cells (Figure 5A) raises the question of whether Cdx2 might block intestinal cells from adopting more complete β cell features. To test this hypothesis, we generated epithelial organoids from the antrum and duodenum of double transgenic Rosa-rtTA;TetO-NPMcherry (Rosa-NPM) animals and treated them with Dox in culture. Similar to our observations in vivo, antral organoids produced more C-peptide+ cells with higher levels of β cell factors compared with intestinal organoids (Figure S6). Next, we expressed either the control cherry gene or Cdx2 using adenoviral infection in the double-transgenic antral organoids (Figures 5B and 5C), followed by treatment with Dox to activate β cell conversion. Cdx2 significantly suppressed expression of multiple β cell genes, including NeuroD1, Nkx2.2, and Nkx6.1 (Figure 5D).
Figure 5. The Intestine-Specific Cell Fate Regulator Cdx2 Can Inhibit β Cell Conversion.
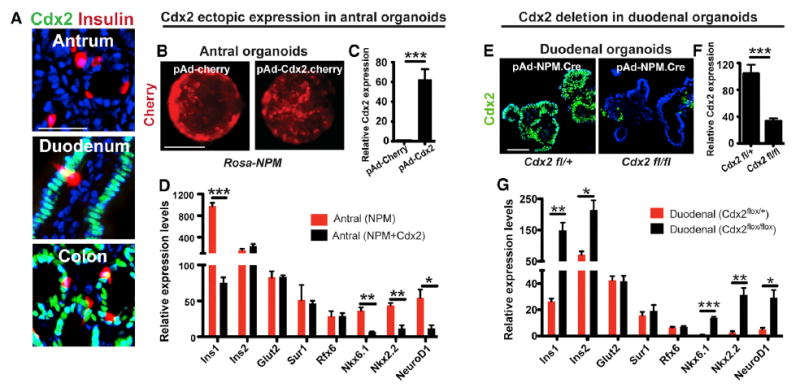
(A) Duodenal and colonic insulin+ cells express Cdx2, the master regulator of intestine cell fate whereas antral stomach cells do not express Cdx2 before or after induction in NRT animals. Scale bar, 50 μm.
(B–D) Epithelial organoids were established from antral tissues of double-transgenic Rosa-rtTA;Teto-NPMcherry (Rosa-NPM) animals and infected with either control adenovirus expressing Cherry (pAd-cherry) or adenovirus expressing Cdx2 and Cherry (pAd-Cdx2.cherry) (B and C). Dox treatment was subsequently used to induce β cell conversion in these antral organoids. qPCR analysis showed that ectopic Cdx2 suppressed the expression of multiple β cell genes (D, n = 3). Scale bar, 100 μm.
(E–G) Duodenal organoids were established from Cdx2fl/+ and Cdx2fl/fl animals (E, left and right, respectively). Infection with an adenovirus co-expressing both NPM factors and the Cre recombinase led to simultaneous deletion of floxed Cdx2 allele and expression of NPM factors (E). Complete removal of Cdx2 was observed in majority of Cdx2fl/fl duodenal cells by immunohistochemistry and qPCR analysis (E and F) and led to enhanced expression of multiple β cell genes from the duodenal organoids (G, n = 3). Scale bar, 100 μm.
Quantitative data presented as mean ± SD. Statistical significance was evaluated with the Student’s t test (*p < 0.05, **p < 0.01, and ***p < 0.001). See also Figure S6.
To further evaluate the role of Cdx2 in intestine reprogramming, we deleted Cdx2 from duodenal organoids. We established duodenal organoids from animals where a single allele or both alleles of the Cdx2 gene are floxed (Figure 5E, Cdx2fl/+ and Cdx2fl/fl). Infection with an polycistronic adenovirus expressing NPM factors and the Cre recombinase (pAd-NPM.Cre) led to simultaneous removal of the floxed Cdx2 allele(s) and expression of NPM factors (Figure 5E). Immunohistochemistry and qPCR confirmed complete removal of Cdx2 from the majority of Cdx2fl/fl duodenal cells (Figures 5E and 5F). Cdx2 deletion significantly enhanced expression of several β cells genes, including Insulin1, insulin2, Nkx6.1, and NeuroD. These data together suggest that Cdx2 acts as a molecular barrier to β cell conversion; thus, failure to downregulate Cdx2 in intestinal insulin+ cells likely contributes to their incomplete acquisition of β cell properties.
Constructing Bioengineered Stomach and Intestine Mini-organs to Produce Insulin+ Cells
Among GI tissues, antral stomach is a superior source of functional β cells by NPM-mediated conversion, and antral insulin+ cells are rapidly replenished from the native stem cell compartment. However, inducing β cells from the native GI tract in situ may have limitations in therapy, because the native endocrine populations regulate many physiologic processes (Field et al., 2010; May and Kaestner, 2010; Schonhoff et al., 2004a), and diverting them into β cells may disrupt normal endocrine homeostasis. Moreover, induced β cells positioned along the native GI epithelium may inadvertently respond to dietary as well as blood glucose. To circumvent these potential barriers to therapeutic application, we studied the feasibility of constructing “stomach mini-organs” that contain genetically engineered antral tissues as a reservoir of new β cells.
Following published protocols on bioengineering stomach (Maemura et al., 2004; Speer et al., 2011), we embedded gastric gland units from the antrum of CAGrtTA∷TetO-NPMcherry (CAG-NPM) animals in Matrigel, loaded them onto poly(glycolic acid) (PGA) scaffolds, and transplanted the material into the omental flap of immunodeficient NSG recipient animals (Figures 6A–6C). Four weeks later, bioengineered stomach spheres measuring 0.5 to 1 cm in diameter formed outside the native gut (Figure 6D). By histology, 5 out of 15 such spheres showed robust epithelial reconstitution, while the others showed little or no epithelium (Figure S7). Antral glands in the native stomach are composed largely of mucous and endocrine cells and lack acid-secreting parietal cells. The engineered stomachs also showed a simple organization, with one or several layers of Ecadherin+ cells surrounded by connective tissue (Figure S7). The epithelial component contained Sox9+ stem/progenitor cells (Furuyama et al., 2011), Mucin5+ secretory cells, and Chga+ endocrine cells (Figure S7). In parallel, we used a similar bioengineering approach to construct “intestine mini-organs” using duodenal gland units. The success rate for epithelial reconstitution was lower in intestinal spheres (3 out of 15), which contained Muc2+ secretory cells and Chga+ endocrine cells, similar to the native duodenal epithelium. Our observations are consistent with other published studies on bioengineered stomach and intestine (Maemura et al., 2004; Speer et al., 2011).
Figure 6. Construction of Bioengineered Stomach and Intestine Mini-organs to Produce Insulin+ Cells.
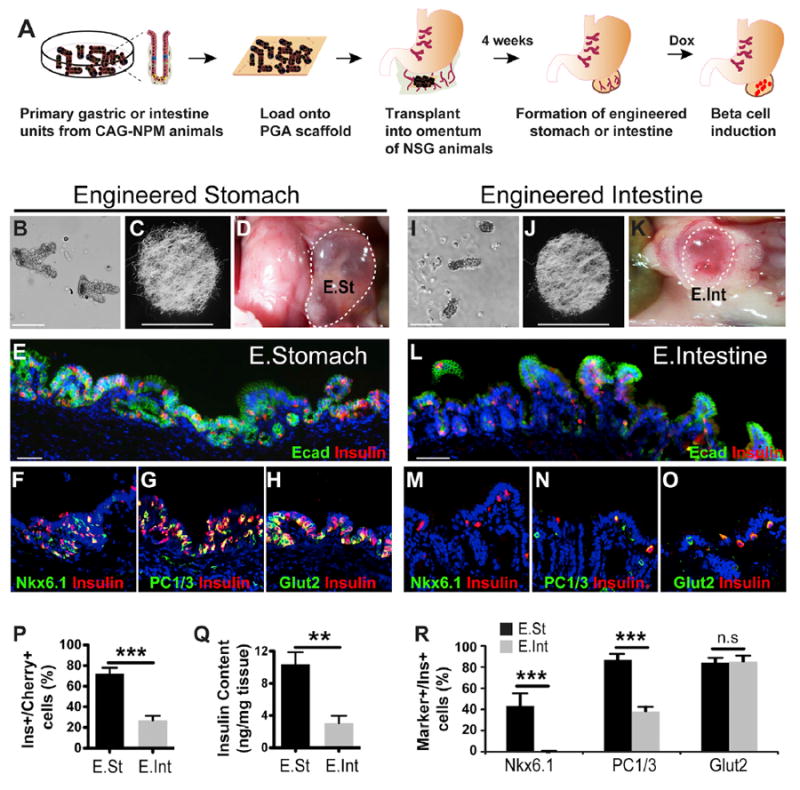
(A–K) Schematic diagram of engineering stomach and intestine mini-organs (A). Gastric or intestinal units were isolated from the antrum or duodenum of CAG-NPM (Cag-rtTA∷TetO-NPMcherry) animals (B and I) and loaded onto polyglycolic acid scaffolds (C and J). The scaffolds were placed inside the omental flap of recipient immune-deficient NSG animals. 4 weeks later, an engineered stomach (E. St) or intestine (E. Int) sphere formed (D and K, circled tissue). Scale bars represent 400 μm (B and I) and 6 μm (C and J).
(E–R) In engineered stomach and intestine spheres where reconstitution of epithelium was successful, Dox treatment led to induction of many insulin+ cells (E and L). The induction efficiency is higher for stomach tissues (P, n = 3). Stomach tissues also have higher insulin content (Q, n = 3). The majority of insulin+ cells from engineered stomach express Nkx6.1, PC1/3, and Glut2 (F, G, H, and R) whereas insulin+ cells from engineered intestine lack Nkx6.1 and have reduced PC1/3 expression (M, N, O, and R). Quantitation presented as mean ± SD. Statistical significance was evaluated with the Student’s t test (**p < 0.01 and ***p < 0.001).
See also Figure S7.
To evaluate induction of insulin+ cell in the engineered stomach and intestine spheres, we administered Dox for 2 weeks. Many insulin+ cells appeared in the epithelial layer of stomach as well as intestinal spheres. The stomach spheres had significantly more insulin+ cells, higher reprogramming efficiency, and higher insulin content per milligram of tissue (Figures 6E, 6L, 6P, and 6Q). The majority of stomach insulin+ cells express Nkx6.1, Glut2, and PC1/3, whereas intestine insulin+ cells lack Nkx6.1 and have reduced PC1/3 expression (Figures 6F–6H, 6M–6O, and 6R).
Transplanted Stomach Mini-organs Can Control Hyperglycemia in Diabetic Mice
To assess if β cells induced in the engineered stomachs could release functional insulin, we ablated pancreatic β cells in transplanted animals using STZ and then induced insulin+ cells in the engineered stomach spheres by administering Dox (Figure 7A). Of the 22 treated animals, 5 showed sustained decreases in blood glucose levels after Dox treatment (group 1), whereas the others remained hyperglycemic (group 2) (Figure 7B). We monitored animals for 6 weeks and subsequently removed the grafted stomach spheres from G1 mice, which restored hyperglycemia (Figure 7B). Engineered stomach spheres from G1 animals showed good epithelial structures containing many insulin+ cells (Figure S7), whereas spheres from the G2 groups showed limited epithelial structures with few insulin+ cells (Figure S7). Consistent with the glucose monitoring data and histology, G1 animals showed improved responses to intraperitoneal glucose challenge (Figure 7C). Blood insulin levels in G1 animals also were substantially higher than in G2 animals (Figure 7D).
Figure 7. Transplanted Stomach Mini-organs Can Reverse Hyperglycemia in Diabetic Mice.
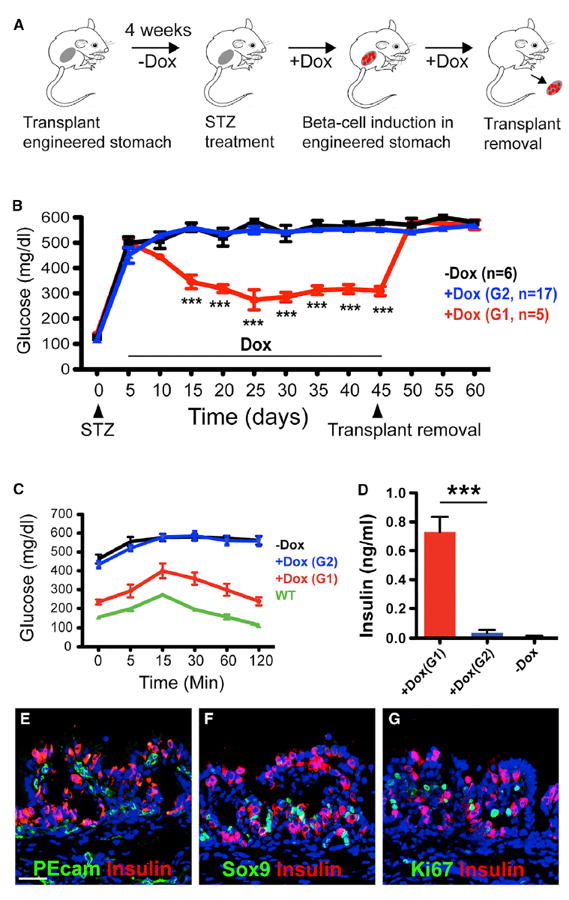
(A) Diagram of the experimental design. STZ treatment was used to ablate endogenous β cells in NSG animals transplanted with 4-week-old stomach spheres, followed by continuous Dox treatment of induce insulin+ cells. At the end of the experiment, the engineered stomachs were removed surgically.
(B–D) STZ treatment led to rapid hyperglycemia that persists in the absence of treatment (−Dox group, n = 6, black squares) (B). After Dox treatment, a group of five animals showed prolonged suppression of hyperglycemia (G1 animals, n = 5, red squares), whereas another group of animals remained hyperglycemic (G2 animals, n = 17, blue squares) (B). After 6 weeks, the engineered stomach spheres were removed from the G1 animals, which led to their reversal back to hyperglycemia (B). G1 animals showed improved response in glucose tolerance test (C, n = 4) and substantially higher blood insulin levels (D, n = 4) compared with G2 animals or control STZ-treated animals without Dox induction. Wilde-type control animals in (C) (green squares) are non-STZ-treated animals with intact pancreatic β cell mass. Quantitative data presented as mean ± SEM. Statistical significance was evaluated with the Student’s t test (***p < 0.001).
(E–G) Sox9+ and Ki67+ cells are present in the engineered stomach after 4-week Dox treatment (E and F), indicating persistence of stem/progenitor cells. PEcam+ blood vessels are closely associated with insulin+ cells inside the engineered stomach sphere (G). Scale bars, 100 μm. Blue channel, DAPI.
See also Figure S7.
Immunohistochemistry revealed PEcam+ blood vessels closely associated with insulin+ cells in engineered stomach spheres (Figure 7E), consistent with previous observations that induced β cells, similar to endogenous β cells, can secrete VEGF and remodel local vasculature (Zhou et al., 2008). Moreover, large numbers of Sox9+ stem/progenitor cells and Ki67+ proliferating epithelial cells are present in the engineered stomach spheres before and after Dox treatment, indicating persistence of a stem/progenitor compartment (Figures 7F and 7G). These studies collectively indicate that induced insulin+ cells from the bioengineered stomach spheres can release insulin into the circulation and regulate blood glucose levels.
DISCUSSION
The GI tract is a highly regenerative endodermal organ. We sought to harness this regenerative capacity to create a renewable source of functional insulin+ cells by NPM-mediated reprogramming. Our data show that antral stomach enteroendocrine cells are converted to insulin+ cells more efficiently than intestinal enteroendocrine cells and possess molecular and functional hallmarks of pancreatic β cells. Thus, the antral stomach is a surprisingly good source for reprogrammed insulin+ cells, and we demonstrate the application of bioengineered stomach spheres to control blood glucose levels.
Expression of NPM factors previously led to formation of insulin+ cells in the intestine (Chen et al., 2014). Our experimental system is similar to this previous report and confirms induction of insulin+ cells in the intestine with incomplete β cell conversion. In contrast, antral stomach endocrine cells are more fully reprogrammed, with robust expression of key β cell genes and substantially improved glucose responsiveness. Our studies suggest that the difference can be attributed, at least in part, to intrinsic molecular differences between antral and intestinal enteroendocrine cells. Higher levels of β cell fate regulators in antral enteroendocrine cells may facilitate their conversion, whereas Cdx2, which is specifically expressed in all intestinal, but not stomach, cells inhibits conversion. It is notable that Cdx2 expression persists in induced insulin+ intestinal cells. Prior studies have shown that ectopic Cdx2 expression in stomach promotes an intestine fate (Silberg et al., 2002; Verzi et al., 2013), whereas Cdx2 loss in cultured intestinal organoids activates antral differentiation (Simmini et al., 2014). Continued expression of Cdx2 in intestinal insulin+ cells may thus present a molecular barrier for complete reprogramming.
Compared with the gastric antrum, the gastric corpus contains few Ngn3-derived enteroendocrine cells, and few such cells expressed insulin after NPM induction. Global expression of NPM factors also induced few insulin+ cells in the fundus (Figure S1). Thus, gastric corpus endocrine cells, which are distinct from those in the antrum or intestine (Choi et al., 2014; Li et al., 2014a) and mainly derive from Ngn3-independent lineages (Li et al., 2014a; Schonhoff et al., 2004b), are not amenable to NPM-mediated β cell conversion. What might account for this resistance? The antral stomach shares a close developmental origin with the pancreas, with both organs arising from a common Pdx1+ endodermal domain during embryogenesis (Wells and Melton, 1999). Therefore, we speculate that the epigenetic landscape of endocrine cells from the fundus is more distinct than those from the antrum, making them harder to convert into β cells. Future studies will be necessary to understand these regional distinctions.
FoxO1 deletion also leads to formation of insulin+ cells in the intestine, suggesting a therapeutic path toward inducing insulin+ cells in situ (Bouchi et al., 2014; Talchai et al., 2012a). Our approach offers several advantages. First, with our method, induced insulin+ cells preserve FoxO1 function, which is known to protect β cells from physiologic stress (Kitamura et al., 2005; Talchai et al., 2012b). Second, with bioengineered stomach spheres, native endocrine cell populations in the gut remain undisturbed, and their functions in physiology are preserved. Third, by separating engineered stomachs from the native organ, induced β cells can be positioned to respond only to changes in blood and not luminal glucose levels.
In summary, our study offers a new approach to harness the intrinsic regenerative capacity of the stomach epithelium to replenishing β cell mass in vivo. Given ongoing pathological insults that continuously erode native or transplanted β cells in diabetes, long-term treatment may require repeated transplants. The regenerative system we propose could eliminate that need, and the number and size of transplanted stomach spheres could be manipulated to control β cell numbers. Coupled with recent progress in genome engineering and the ready access to human gastric epithelium from biopsies and differentiated induced pluripotent stem cells or embryonic stem cells (McCracken et al., 2014), the therapeutic applications of this approach are considerable.
EXPERIMENTAL PROCEDURES
Mouse Strains
R26-floxed-rtTA, R26-floxed-GFP, R26-rtTA, CAG-rtTA, Ngn3-Cre, and NSG mouse strains were obtained from The Jackson Laboratory. Ngn3-GFP (Gu et al., 2002; Jenny et al., 2002; Lee et al., 2002) and Cdx2fl/fl (Silberg et al., 2002; Verzi et al., 2013) mice have been described previously. The TetO-NPMcherry mouse lines were made by standard pronuclear injection at the Harvard Genomic Modification Facility (Cambridge, MA). All animal experiments are approved by the Harvard Institutional Animal Care and Use Committee.
Antibodies and Immunofluorescence
Tissues were processed as previously described (Li et al., 2014b). Primary antibodies are listed in Supplemental Experimental Procedures. Pictures were taken with a Zeiss LSM 510 META confocal microscope. For quantification of marker+ cells such as insulin+ cells, a total of at least 1,000 Marker+ were analyzed from tissues harvested from three different animals. Typically, at least ten randomly selected sections were counted per animal.
FACS Isolation of GFP+ Cells and Gene Profiling
To dissociate tissues into single cells for FACS purification, we modified published protocols (Habib et al., 2012; Reimann et al., 2008; Talchai et al., 2012a). See Supplemental Experimental Procedures for details. GFP+ cells were isolated by FACS with FACSaria (BD Bioscience). Transcriptome data were generated with Illumina microarrays (Sentrix BeadChip MouseRef-8 v2 Arrays) that contain probes for ~19,000 genes. Data analysis, including statistical methods used, is described in Supplemental Experimental Procedures.
Glucose Stimulated Insulin Secretion Assay and Drug Treatments
Isolation of gastrointestinal epithelial cells was carried out as previously described with slight modifications (Habib et al., 2012; Reimann et al., 2008; Talchai et al., 2012a). Briefly, antrum tissue was cut into small pieces and incubated in 10 mM EDTA for 30 min, followed by mechanical dissociation to extract cell clusters. To collect duodenal samples, the duodenum tissue was first cut into small pieces, incubated in 10 mM EDTA for 5 min, and mechanically stripped to release the villi. Each cell fraction was incubated with Krebs Ringer buffer supplemented with 1.7 mM or 20.2 mM glucose, glibenclamide (10 nM; Tocris), diazoxide (0.5 mM; Sigma), or exendin-4 (100 nM; Sigma). Released insulin amounts were determined by ELISA (Alpco) at the Joslin Specialized Assay core (Joslin Diabetes Center, Boston). Data from different tissue sources were standardized according to basal insulin release level. Each standardized sample is equivalent to 1/15 of antrum or 5 mm of duodenum, or 10 mm of colon in a single animal.
Physiological Studies
Diabetic animals were produced with intraperitoneal injection of STZ (150–170 mg/kg) in 6- to 8-week-old animals. Animals that displayed >400 mg dl−1 blood glucose levels for 2 consecutive days after STZ administration were used for experiments. Blood glucose was measured with an Ascensia Elite glucometer (Bayer). For blood glucose monitoring, a short 2-hr fasting precedes glucose measurements. Glucose tolerance test was performed with intraperitoneal injection of 1 mg/g body weight of glucose, preceded by 4-hr fasting. Blood insulin was collected from tail vein blood sampling and measured by ELISA. Tissue insulin was extracted with acid-ethanol solutions and measured by ELISA.
Organoid Culture and Adenoviral Infection
Antral stomach and duodenal organoids were derived from young adult mice (1–2 months) and cultured using standard growth media, essentially as described (Barker et al., 2010). To test β cell reprogramming factors, 4- to 7-day cultures of antral or duodenal organoids were recovered from the Matrigel with the recover solution (Corning), infected with purified adenovirus at 4 ×107 plaque-forming units (PFU) in 100 μl medium for 1 hr at 37°C and re-embedded in Matrigel. qPCR analysis was performed 6–8 days after infection.
Generation of Bioengineered Stomach and Intestine
Generation of bioengineered stomach and stomach spheres was performed essentially as described previously (Maemura et al., 2004; Speer et al., 2011). See Supplemental Experimental Procedures for further details.
Supplementary Material
Highlights.
Antral stomach cells reprogram effectively to insulin+ pancreatic β-like cells
Antral endocrine cells are transcriptionally related to pancreatic β cells
Induced insulin+ cells reverse hypoglycemia after transplantation in diabetic mice
Reprogrammed cells in bioengineered mini-organs give functional rescue in vivo
Acknowledgments
We thank Boston Children’s Hospital core facility for Illumina array; Joslin Specialized Assay Core for insulin measurement; Juliana Brown for expert help with pancreatectomy; members of the Zhou lab for advice and feedback; and Gordon Weir, Susan Bonner-Weir, Andrew Leiter, Konrad Hochedlinger, and Jay Rajagopal for discussion and reading of the manuscript. This study was supported by awards from the National Institute of Health and the Harvard Stem Cell Institute (U01 DK089536 and DP-0144-14-00) to Q.Z., awards (R01DK084056, the Timothy Murphy Fund, the IDDRC P30HD18655, and the HDDC P30DK034854) to D.T.B., and R01DK082889 to R.A.S. C.A. is a recipient of HSCI-Sternlicht Fellowship.
Footnotes
AUTHOR CONTRIBUTIONS
C.A. and Q.Z. conceived and designed the experiments and analyzed the results; C.A. performed most of the experiments; A.T., J.L., M.S.S., C.A.R., and D.T.B. helped design and perform the organoid experiments; G.X. and S.M. analyzed the microarray data and performed statistical analysis; C.V. and D.M. helped design and perform the bioengineered stomach experiments; R.A.S helped design the Cdx2 experiments; D.A.M., B.Z.S., D.M., R.A.S, Q.X, and D.T.B. contributed reagents/materials/analysis; and Q.Z. and C.A. wrote the paper. All authors discussed the manuscript.
ACCESSION NUMBERS
The accession number for the microarray data reported in this paper is GEO: GSE76686.
SUPPLEMENTAL INFORMATION
Supplemental Information includes Supplemental Experimental Procedures, seven figures, and four tables and can be found with this article online at http://dx.doi.org/10.1016/j.stem.2016.01.003.
References
- Azzi J, Geara AS, El-Sayegh S, Abdi R. Immunological aspects of pancreatic islet cell transplantation. Expert Rev Clin Immunol. 2010;6:111–124. doi: 10.1586/eci.09.67. [DOI] [PubMed] [Google Scholar]
- Barker N, van Es JH, Kuipers J, Kujala P, van den Born M, Cozijnsen M, Haegebarth A, Korving J, Begthel H, Peters PJ, Clevers H. Identification of stem cells in small intestine and colon by marker gene Lgr5. Nature. 2007;449:1003–1007. doi: 10.1038/nature06196. [DOI] [PubMed] [Google Scholar]
- Barker N, Huch M, Kujala P, van de Wetering M, Snippert HJ, van Es JH, Sato T, Stange DE, Begthel H, van den Born M, et al. Lgr5(+ve) stem cells drive self-renewal in the stomach and build long-lived gastric units in vitro. Cell Stem Cell. 2010;6:25–36. doi: 10.1016/j.stem.2009.11.013. [DOI] [PubMed] [Google Scholar]
- Bonner-Weir S. Life and death of the pancreatic beta cells. Trends Endocrinol Metab. 2000;11:375–378. doi: 10.1016/s1043-2760(00)00305-2. [DOI] [PubMed] [Google Scholar]
- Bouchi R, Foo KS, Hua H, Tsuchiya K, Ohmura Y, Sandoval PR, Ratner LE, Egli D, Leibel RL, Accili D. FOXO1 inhibition yields functional insulin-producing cells in human gut organoid cultures. Nat Commun. 2014;5:4242. doi: 10.1038/ncomms5242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler AE, Janson J, Bonner-Weir S, Ritzel R, Rizza RA, Butler PC. Beta-cell deficit and increased beta-cell apoptosis in humans with type 2 diabetes. Diabetes. 2003;52:102–110. doi: 10.2337/diabetes.52.1.102. [DOI] [PubMed] [Google Scholar]
- Chen YJ, Finkbeiner SR, Weinblatt D, Emmett MJ, Tameire F, Yousefi M, Yang C, Maehr R, Zhou Q, Shemer R, et al. De novo formation of insulin-producing “neo-β cell islets” from intestinal crypts. Cell Rep. 2014;6:1046–1058. doi: 10.1016/j.celrep.2014.02.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choi E, Roland JT, Barlow BJ, O’Neal R, Rich AE, Nam KT, Shi C, Goldenring JR. Cell lineage distribution atlas of the human stomach reveals heterogeneous gland populations in the gastric antrum. Gut. 2014;63:1711–1720. doi: 10.1136/gutjnl-2013-305964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Egerod KL, Engelstoft MS, Grunddal KV, Nøhr MK, Secher A, Sakata I, Pedersen J, Windeløv JA, Füchtbauer EM, Olsen J, et al. A major lineage of enteroendocrine cells coexpress CCK, secretin, GIP, GLP-1, PYY, and neurotensin but not somatostatin. Endocrinology. 2012;153:5782–5795. doi: 10.1210/en.2012-1595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Field BC, Chaudhri OB, Bloom SR. Bowels control brain: gut hormones and obesity. Nat Rev Endocrinol. 2010;6:444–453. doi: 10.1038/nrendo.2010.93. [DOI] [PubMed] [Google Scholar]
- Furuyama K, Kawaguchi Y, Akiyama H, Horiguchi M, Kodama S, Kuhara T, Hosokawa S, Elbahrawy A, Soeda T, Koizumi M, et al. Continuous cell supply from a Sox9-expressing progenitor zone in adult liver, exocrine pancreas and intestine. Nat Genet. 2011;43:34–41. doi: 10.1038/ng.722. [DOI] [PubMed] [Google Scholar]
- Gao N, White P, Kaestner KH. Establishment of intestinal identity and epithelial-mesenchymal signaling by Cdx2. Dev Cell. 2009;16:588–599. doi: 10.1016/j.devcel.2009.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graf T, Enver T. Forcing cells to change lineages. Nature. 2009;462:587–594. doi: 10.1038/nature08533. [DOI] [PubMed] [Google Scholar]
- Gu G, Dubauskaite J, Melton DA. Direct evidence for the pancreatic lineage: NGN3+ cells are islet progenitors and are distinct from duct progenitors. Development. 2002;129:2447–2457. doi: 10.1242/dev.129.10.2447. [DOI] [PubMed] [Google Scholar]
- Gurdon JB, Melton DA. Nuclear reprogramming in cells. Science. 2008;322:1811–1815. doi: 10.1126/science.1160810. [DOI] [PubMed] [Google Scholar]
- Habib AM, Richards P, Cairns LS, Rogers GJ, Bannon CA, Parker HE, Morley TC, Yeo GS, Reimann F, Gribble FM. Overlap of endocrine hormone expression in the mouse intestine revealed by transcriptional profiling and flow cytometry. Endocrinology. 2012;153:3054–3065. doi: 10.1210/en.2011-2170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hebrok M. Generating β cells from stem cells-the story so far. Cold Spring Harb Perspect Med. 2012;2:a007674. doi: 10.1101/cshperspect.a007674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jenny M, Uhl C, Roche C, Duluc I, Guillermin V, Guillemot F, Jensen J, Kedinger M, Gradwohl G. Neurogenin3 is differentially required for endocrine cell fate specification in the intestinal and gastric epithelium. EMBO J. 2002;21:6338–6347. doi: 10.1093/emboj/cdf649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johannesson B, Sui L, Freytes DO, Creusot RJ, Egli D. Toward beta cell replacement for diabetes. EMBO J. 2015;34:841–855. doi: 10.15252/embj.201490685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karam SM, Leblond CP. Dynamics of epithelial cells in the corpus of the mouse stomach. V. Behavior of enteroendocrine and caveolated cells: general conclusions on cell kinetics in the oxyntic epithelium. Anat Rec. 1993;236:333–340. doi: 10.1002/ar.1092360206. [DOI] [PubMed] [Google Scholar]
- Kitamura YI, Kitamura T, Kruse JP, Raum JC, Stein R, Gu W, Accili D. FoxO1 protects against pancreatic beta cell failure through NeuroD and MafA induction. Cell Metab. 2005;2:153–163. doi: 10.1016/j.cmet.2005.08.004. [DOI] [PubMed] [Google Scholar]
- Lakey JR, Mirbolooki M, Shapiro AM. Current status of clinical islet cell transplantation. Methods Mol Biol. 2006;333:47–104. doi: 10.1385/1-59745-049-9:47. [DOI] [PubMed] [Google Scholar]
- Lee CS, Perreault N, Brestelli JE, Kaestner KH. Neurogenin 3 is essential for the proper specification of gastric enteroendocrine cells and the maintenance of gastric epithelial cell identity. Genes Dev. 2002;16:1488–1497. doi: 10.1101/gad.985002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lehy T, Willems G. Population kinetics of antral gastrin cells in the mouse. Gastroenterology. 1976;71:614–619. [PubMed] [Google Scholar]
- Li HJ, Johnston B, Aiello D, Caffrey DR, Giel-Moloney M, Rindi G, Leiter AB. Distinct cellular origins for serotonin-expressing and enterochromaffin-like cells in the gastric corpus. Gastroenterology. 2014a;146:754–764. doi: 10.1053/j.gastro.2013.11.048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li W, Cavelti-Weder C, Zhang Y, Clement K, Donovan S, Gonzalez G, Zhu J, Stemann M, Xu K, Hashimoto T, et al. Long-term persistence and development of induced pancreatic beta cells generated by lineage conversion of acinar cells. Nat Biotechnol. 2014b;32:1223–1230. doi: 10.1038/nbt.3082. [DOI] [PubMed] [Google Scholar]
- Li W, Nakanishi M, Zumsteg A, Shear M, Wright C, Melton DA, Zhou Q. In vivo reprogramming of pancreatic acinar cells to three islet endocrine subtypes. eLife. 2014c;3:e01846. doi: 10.7554/eLife.01846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maemura T, Ogawa K, Shin M, Mochizuki H, Vacanti JP. Assessment of tissue-engineered stomach derived from isolated epithelium organoid units. Transplant Proc. 2004;36:1595–1599. doi: 10.1016/j.transproceed.2004.05.020. [DOI] [PubMed] [Google Scholar]
- May CL, Kaestner KH. Gut endocrine cell development. Mol Cell Endocrinol. 2010;323:70–75. doi: 10.1016/j.mce.2009.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCracken KW, Catá EM, Crawford CM, Sinagoga KL, Schumacher M, Rockich BE, Tsai YH, Mayhew CN, Spence JR, Zavros Y, Wells JM. Modelling human development and disease in pluripotent stem-cell-derived gastric organoids. Nature. 2014;516:400–404. doi: 10.1038/nature13863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Messier B, Leblond CP. Cell proliferation and migration as revealed by radioautography after injection of thymidine-H3 into male rats and mice. Am J Anat. 1960;106:247–285. doi: 10.1002/aja.1001060305. [DOI] [PubMed] [Google Scholar]
- Nostro MC, Keller G. Generation of beta cells from human pluripotent stem cells: Potential for regenerative medicine. Semin Cell Dev Biol. 2012;23:701–710. doi: 10.1016/j.semcdb.2012.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Offield MF, Jetton TL, Labosky PA, Ray M, Stein RW, Magnuson MA, Hogan BL, Wright CV. PDX-1 is required for pancreatic outgrowth and differentiation of the rostral duodenum. Development. 1996;122:983–995. doi: 10.1242/dev.122.3.983. [DOI] [PubMed] [Google Scholar]
- Rahier J, Guiot Y, Goebbels RM, Sempoux C, Henquin JC. Pancreatic beta-cell mass in European subjects with type 2 diabetes. Diabetes Obes Metab. 2008;10(suppl 4):32–42. doi: 10.1111/j.1463-1326.2008.00969.x. [DOI] [PubMed] [Google Scholar]
- Reimann F, Habib AM, Tolhurst G, Parker HE, Rogers GJ, Gribble FM. Glucose sensing in L cells: a primary cell study. Cell Metab. 2008;8:532–539. doi: 10.1016/j.cmet.2008.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schiesser JV, Wells JM. Generation of β cells from human pluripotent stem cells: are we there yet? Ann N Y Acad Sci. 2014;1311:124–137. doi: 10.1111/nyas.12369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schonhoff SE, Giel-Moloney M, Leiter AB. Minireview: Development and differentiation of gut endocrine cells. Endocrinology. 2004a;145:2639–2644. doi: 10.1210/en.2004-0051. [DOI] [PubMed] [Google Scholar]
- Schonhoff SE, Giel-Moloney M, Leiter AB. Neurogenin 3-expressing progenitor cells in the gastrointestinal tract differentiate into both endocrine and non-endocrine cell types. Dev Biol. 2004b;270:443–454. doi: 10.1016/j.ydbio.2004.03.013. [DOI] [PubMed] [Google Scholar]
- Silberg DG, Sullivan J, Kang E, Swain GP, Moffett J, Sund NJ, Sackett SD, Kaestner KH. Cdx2 ectopic expression induces gastric intestinal metaplasia in transgenic mice. Gastroenterology. 2002;122:689–696. doi: 10.1053/gast.2002.31902. [DOI] [PubMed] [Google Scholar]
- Simmini S, Bialecka M, Huch M, Kester L, van de Wetering M, Sato T, Beck F, van Oudenaarden A, Clevers H, Deschamps J. Transformation of intestinal stem cells into gastric stem cells on loss of transcription factor Cdx2. Nat Commun. 2014;5:5728. doi: 10.1038/ncomms6728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Speer AL, Sala FG, Matthews JA, Grikscheit TC. Murine tissue-engineered stomach demonstrates epithelial differentiation. J Surg Res. 2011;171:6–14. doi: 10.1016/j.jss.2011.03.062. [DOI] [PubMed] [Google Scholar]
- Talchai SC, Accili D. Legacy Effect of Foxo1 in Pancreatic Endocrine Progenitors on Adult β-Cell Mass and Function. Diabetes. 2015;64:2868–2879. doi: 10.2337/db14-1696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Talchai C, Xuan S, Kitamura T, DePinho RA, Accili D. Generation of functional insulin-producing cells in the gut by Foxo1 ablation. Nat Genet. 2012a;44:406–412. doi: 10.1038/ng.2215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Talchai C, Xuan S, Lin HV, Sussel L, Accili D. Pancreatic β cell dedifferentiation as a mechanism of diabetic β cell failure. Cell. 2012b;150:1223–1234. doi: 10.1016/j.cell.2012.07.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson EM, Price YE, Wright NA. Kinetics of enteroendocrine cells with implications for their origin: a study of the cholecystokinin and gastrin subpopulations combining tritiated thymidine labelling with immunocytochemistry in the mouse. Gut. 1990;31:406–411. doi: 10.1136/gut.31.4.406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verzi MP, Shin H, San Roman AK, Liu XS, Shivdasani RA. Intestinal master transcription factor CDX2 controls chromatin access for partner transcription factor binding. Mol Cell Biol. 2013;33:281–292. doi: 10.1128/MCB.01185-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wells JM, Melton DA. Vertebrate endoderm development. Annu Rev Cell Dev Biol. 1999;15:393–410. doi: 10.1146/annurev.cellbio.15.1.393. [DOI] [PubMed] [Google Scholar]
- Zhou Q, Melton DA. Pathways to new beta cells. Cold Spring Harb Symp Quant Biol. 2008;73:175–181. doi: 10.1101/sqb.2008.73.002. [DOI] [PubMed] [Google Scholar]
- Zhou Q, Brown J, Kanarek A, Rajagopal J, Melton DA. In vivo reprogramming of adult pancreatic exocrine cells to beta-cells. Nature. 2008;455:627–632. doi: 10.1038/nature07314. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.