

Abstract
Follicular variant papillary thyroid cancer (FVPTC) is the second most common subtype after conventional PTC. We compared ultrasonographic (US) features of FVPTC to those of conventional PTC according to tumor size. We reviewed US findings, pathologic reports, and medical charts of 249 PTC patients with surgically proven disease (83 FVPTCs, 166 conventional PTCs) at our institution from January 2007 to December 2012. FVPTCs were divided into PTC-like and follicular neoplasm (FN)-like based on sonographic characteristics. PTC-like features were defined as having at least one malignant feature (taller-than-wide shape, infiltrative margin, marked hypoechogenicity, and micro-calcifications), whereas FN-like cancers showed oval solid features without malignant features. FVPTCs showed a higher rate of FN-like features than conventional PTCs. Of 166 conventional PTCs, 13 (7.8%) had FN-like features and 153 (92.2%) had PTC-like features, whereas of the 83 FVPTCs, 31 (37.3%) had FN-like features and 52 (62.7%) had PTC-like features. Macro-FVPTCs showed a higher rate of FN-like features than micro-FVPTCs (P < 0.001). Of 21 macro-FVPTCs, 18 (85.7%) had FN-like features and 3 (14.3%) had PTC-like features, whereas of the 62 micro-FVPTCs, 13 (21%) had FN-like features and 49 (79%) had PTC-like features. There were no differences in multifocality, extrathyroidal invasion, and lymph node metastasis between PTC-like FVPTCs and FN-like FVPTCs. FVPTCs showed fewer sonographic malignant features than conventional PTCs. In particular, FVPTCs larger than 1 cm had a more frequent benign sonographic appearance. Therefore, if fine-needle aspiration result is suspicious for PTC in a nodule larger than 1 cm with no suspicious US features, the possibility of FVPTC might be considered.
Keywords: Follicular Variant, Papillary, Thyroid Neoplasms
Graphical Abstract
INTRODUCTION
Thyroid nodules are a common clinical problem, and differentiated thyroid cancer is becoming increasingly prevalent (1). Approximately 90% of thyroid cancer cases are well differentiated, and are usually classified as papillary thyroid carcinoma (PTC) or follicular thyroid carcinoma based on the predominant histology (2). Many variants of PTC have been described, including oncocytic, tall-cell, columnar-cell, diffuse-sclerosing, encapsulated, and follicular variants (3). Follicular variant PTC (FVPTC) is the second most common variant of PTC and variably accounts for 9% to 50% of all PTCs following conventional PTC, which is the most common type of thyroid cancer (4,5,6). FVPTC is composed predominantly of follicular architecture, which is lined by cells with nuclear features of PTC (7). Nevertheless, because it behaves clinically like PTC, it is classified as a subtype of PTC in the International Histological Classification of Tumors by the World Health Organization (8).
With the increasing incidence of thyroid cancer, FVPTC has been increasingly diagnosed in recent years. This increase in incidence may be due largely to increased detection of small nonpalpable nodules by thyroid US or other imaging modalities. Therefore, the incidence of papillary thyroid microcarcinoma (PTMC), defined as a PTC with a maximum diameter of 1 cm or less, has increased rapidly and a similar increase in micro-FVPTC is expected. However, the clinical behavior and outcomes of FVPTC remain controversial (4,6,9,10,11,12,13,14). In addition, cytologic diagnosis of FVPTC using fine-needle aspiration (FNA) can be difficult owing to the paucity of nuclear changes of PTC and overlapping features with other follicular-derived lesions (15).
Many clinical studies have reported relatively consistent sonographic findings of thyroid malignancy, especially for PTCs (16,17,18); however, the sonographic features of FVPTC are not established. Some studies reported that FVPTC has a relatively benign appearance and is more similar to a follicular neoplasm than PTC on ultrasonography (US) (19,20,21). To date, there are few studies of US features of FVPTC according to tumor size.
Therefore, in this study, we compared US features of FVPTC to those of conventional PTC according to tumor size.
MATERIALS AND METHODS
Subjects
All patients who underwent thyroidectomy and were finally diagnosed with PTC at our hospital between January 2007 and December 2012 were searched and a total of 249 cases (83 FVPTCs, 166 conventional PTCs) were included in statistical analysis for this study. A propensity score matching method was used for matching with age and sex as confounding variables, and logit was used to indicate the maximum width of the caliper for which matching should be done. The caliper size was 0.145 and the matching ratio was 1:2.
Thyroid ultrasonography
The sonographic findings of these thyroid nodules were retrospectively reviewed and clinical information was obtained from the medical records. The US images were analyzed retrospectively in a review by one endocrinologist (J.E.D.) with 10 years of experience in evaluating thyroid nodules. Ultrasound examinations were performed with a Philips HD 11 ultrasound system (Philips Healthcare, USA) equipped with a 5- to 12-MHz linear array transducer. The scanning protocol for all cases included both transverse and longitudinal real-time imaging of the thyroid nodules.
Each lesion was described using the sonographic features, including echogenicity, margin, shape, and presence of calcifications. The echogenicity of the tumor was compared with that of adjacent thyroid parenchyma. Malignant sonographic features were defined as marked hypoechogenicity (echogenicity lower than that of the surrounding strap muscle), irregular margins, a taller-than-wide shape (greater in the anteroposterior dimension than the transverse dimension in any plane), and microcalcification (tiny, punctate echogenic foci of 1 mm or less either with or without posterior shadowing). We classified the nodules as malignant even if only one of these suspicious sonographic features was present (16). Clinicopathologic variables such as tumor size, extrathyroidal invasion, and lymph node metastasis were evaluated. PTMC was defined as a tumor that measured ≤ 1 cm in diameter. Follicular neoplasm (FN)-like nodules were defined as having no accepted malignant feature (Fig. 1). PTC-like nodules were defined as having at least one accepted malignant feature (Fig. 2). The tumor-node-metastasis (TNM) stage of the tumor was determined using criteria from the 7th edition of the American Joint Committee on Cancer staging manual (22).
Fig. 1.

Ultrasonographic findings of thyroid in a 35-year-old woman with FN-like follicular variant papillary thyroid cancer. The nodule shows no malignant suspicious US findings in transverse view (A) and longitudinal view (B).
Fig. 2.

Ultrasonographic findings of thyroid in a 55-year-old woman with PTC-like follicular variant papillary thyroid cancer. The nodule shows marked hypoechogenicity and irregular infiltrated margin in transverse view (A) and longitudinal view (B).
Statistical analysis
Comparison of mean values for the two groups was performed with t-test or Mann-Whitney U test, as appropriate. The categorical variables are presented as numbers and percentages, and were compared using the chi-square test or Fisher exact test. P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
Ethics statement
The institutional review board of the Daegu Catholic University Hospital reviewed and approved the protocol of this study (IRB approval number; CR-15-027). The need for informed consent was waived by the board.
RESULTS
Comparisons of clinicopathologic findings of FVPTC and conventional PTC
Clinicopathologic characteristics of FVPTCs and conventional PTCs are summarized in Table 1. A total of 249 patients were included, 83 patients in the FVPTC group and 166 in the conventional PTC group. There was no significant difference in age and gender between the two groups. The size of the tumor was not significantly different between the two groups: 0.90 ± 1.11 cm in FVPTC patients and 0.74 ± 0.67 cm in PTC patients (P = 0.236). Micro- PTC was more common than macro-PTC in both groups (74.7% versus 80.7%, P = 0.274). The conventional PTC group had significantly higher central lymph node metastasis (36.7% versus 9.6%, P < 0.001) and extrathyroidal invasion (24.1% vs. 6.0%, P < 0.001) than the FVPTC group. The majority of FVPTCs (72.3%) were defined as suspicious for PTC by FNA.
Table 1. Comparisons of clinicopathologic findings of FVPTC and conventional PTC.
| Variables | FVPTC (n = 83 ) | Conventional PTC (n = 166 ) | P value |
|---|---|---|---|
| Age (yr) | 46.70 ± 9.42 | 46.93 ± 10.20 | 0.861 |
| Gender (M/F) | 10 (12.0)/73 (88.0) | 24 (14.5)/142 (85.5) | 0.602 |
| Tumor size (cm) | 0.90 ± 1.11 | 0.74 ± 0.67 | 0.236 |
| Micro/Macro PTC | 62 (74.7)/21 (25.3) | 134 (80.7)/32 (19.3) | 0.274 |
| AJCC TNM staging | 0.001 | ||
| Stage I | 74 (89.2%) | 122 (73.5%) | |
| Stage II | 2 (2.4%) | 0 (0.0%) | |
| Stage III | 7 (8.4%) | 44 (26.5%) | |
| FNAC result (follicular lesion or atypical / PTC) | 23 (27.7)/60 (72.3) | 21 (12.7)/145 (87.3) | 0.003 |
| Multiplicity | 16 (19.3) | 36 (21.7) | 0.659 |
| Extrathyroidal invasion | 5 (6.0) | 40 (24.1) | <0.001 |
| Central LN Mets | 8 (9.6) | 61 (36.7) | <0.001 |
| Distant Mets | 0 (0.0) | 0 (0.0) | NA |
| Hashimoto's thyroiditis | 8 (9.6) | 21 (12.7) | 0.485 |
Data are mean ± standard deviation. n, number of patients; AJCC, American Joint Committee on Cancer; FNAC, fine-needle aspiration cytology; LN, lymph node; Mets, metastasis; FV, follicular variant; PTC, papillary thyroid cancer; NA, non available.
Comparisons of sonographic findings of FVPTC and conventional PTC
Sonographic features of an irregular margin (40.4% vs. 19.3%, P = 0.001) and marked hypoechogenicity (84.9% vs. 60.2%, P < 0.001) were more frequent in conventional PTCs than FVPTCs (Table 2). An irregular margin was less common in FVPTCs than conventional PTCs (19.3% vs. 40.4%, P = 0.001). Taller-than-wide shape (9.6% vs. 9.6%, P = 0.582) and microcalcification (13.3% vs. 22.9%, P = 0.071) were not significantly different between FVPTCs and conventional PTCs. A total 31 of 83 FVPTCs (37.3%) did not have sonographic malignant features, compared with only 13 of 166 conventional PTCs (7.8%, P = 0.001).
Table 2. Comparisons of sonographic findings of FVPTC and conventional PTC.
| Variables | FVPTC (n = 83) | Conventional PTC(n = 166) | P value |
|---|---|---|---|
| Sonographic | |||
| Marked hypoechogenicity | 50(60.2) | 141 (84.9) | <0.001 |
| Irregular margin | 16(19.3) | 67(40.4) | 0.001 |
| Taller than wide shape | 8(9.6) | 16(9.6) | 0.582 |
| Calcification | 11(13.3) | 38(22.9) | 0.071 |
| FN-like/PTC-like | 31(37.3)/52(62.7) | 13(7.8)/153(92.2) | 0.001 |
n, number of patients; FN, follicular neoplasm; FV, follicular variant; PTC, papillary thyroid cancer.
Ultrasonographic features according to the size of the tumor
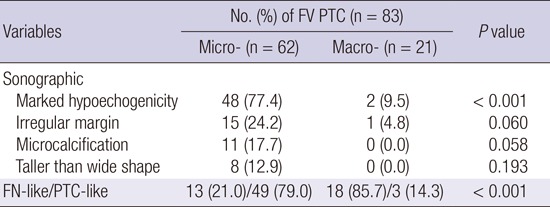
We evaluated the US features of FVPTCs according to the size of the tumor in a pathologic diagnosis. In the patients with macro-FVPTC (i.e., tumors larger than 1 cm) the sonographic feature of marked hypoechogenicity was significantly less common than for micro-FVPTC (9.5% vs. 77.4%, P < 0.001; Table 3-1). Sonographic features of irregular margin (24.2% vs. 4.8%, P = 0.060), microcalcification (17.7% vs. 0.0%, P = 0.058), and taller-than-wide (12.9% vs. 0.0%, P = 0.193) were not significantly different between the groups. Of the 62 micro-FVPTCs, 13 (21%) had FN-like features and 49 (79%) had PTC-like features. Of the 21 macro-FVPTCs, 18 (85.7%) had FN-like features and 3 (14.3%) had PTC-like features. However, in the comparison of US features of PTCs according to the size of the tumor, 124 of the 134 micro-PTCs (81%) and 29 of the 32 macro-PTCs (90.6%) had PTC-like features (Table 3-2). Unlike the results for FVPTCs, the conventional PTC group showed PTC-like features in US regardless of the size of the tumor.
Table 3-1. Sonographic findings of FVPTC according to tumor size.
| Variables | No. (%) of FV PTC (n = 83) | P value | |
|---|---|---|---|
| Micro- (n = 62) | Macro- (n = 21) | ||
| Sonographic | |||
| Marked hypoechogenicity | 48 (77.4) | 2 (9.5) | < 0.001 |
| Irregular margin | 15 (24.2) | 1 (4.8) | 0.060 |
| Microcalcification | 11 (17.7) | 0 (0.0) | 0.058 |
| Taller than wide shape | 8 (12.9) | 0 (0.0) | 0.193 |
| FN-like/PTC-like | 13 (21.0)/49 (79.0) | 18 (85.7)/3 (14.3) | < 0.001 |
n, number of patients; FN, follicular neoplasm; FV, follicular variant; PTC, papillary thyroid cancer.
Table 3-2. Sonographic findings of conventional PTC according to tumor size.
| Variables | No. (%) of conventional PTC (n = 166) | P value | |
|---|---|---|---|
| Micro- (n = 134) | Macro- (n = 32) | ||
| Sonographic | |||
| Marked hypoechogenecity | 118 (88.1) | 23 (71.9) | 0.026 |
| Irregular margin | 48 (35.8) | 19 (59.4) | 0.015 |
| Microcalcification | 25 (18.7) | 13 (34.2) | 0.008 |
| Taller than wide shape | 14 (10.4) | 2 (6.3) | 0.368 |
| FN-like/PTC-like | 10 (19.0)/124 (81.0) | 3 (9.4)/29 (90.6) | 0.475 |
n, number of patients; FN, follicular neoplasm; FV, follicular variant; PTC, papillary thyroid cancer.
Comparisons of clinicopathologic characteristics of FN-like and PTC-like FVPTC
There were 31 patients in the FV-like group and 52 patients in the PTC-like group of FVPTCs (Table 4). Multifocality, extrathyroidal invasion, and lymph node metastasis were not significantly different between PTC-like FVPTCs and FN-like FVPTCs.
Table 4. Comparisons of clinicopathologic of FN-like and PTC-like FVPTC.
| Variables | FN-like (n = 31 ) |
PTC-like (n = 52) |
P value |
|---|---|---|---|
| Multiplicity | 7(22.6) | 9(17.3) | 0.556 |
| Extrathyroidal invasion | 1(3.2) | 4(7.7) | 0.379 |
| Central LN Mets | 2(6.5) | 6(11.6) | 0.364 |
| Distant Mets | 0(0.0) | 0(0.0) | NA |
n, number of patients; LN, lymph node; Mets, metastasis FN, follicular neoplasm; FV, follicular variant; PTC, papillary thyroid cancer; NA, non available.
DISCUSSION
In the present study, FVPTCs showed a lower frequency of sonographically malignant features than conventional PTCs. Especially, FVPTCs larger than 1 cm had a more common benign sonographic appearance. As a very common variant of PTC, FVPTC has been increasingly diagnosed with the dramatic increasing incidence of PTC (1). This may be due to the increased use of neck US and early diagnosis (23). Despite the high incidence, the clinical behavior and outcomes of FVPTC remain controversial, making it challenging to establish a standard treatment strategy (4,6,9,10,11,12,13,14). Most published studies involved a small sample size and a short mean duration of follow-up. In a recent large population-based study, Yu et al. (14) reported that the clinical behavior of FVPTC larger than 1 cm is unique and represents an intermediate entity with clinical features that are between those of conventional PTC and follicular thyroid carcinoma (FTC). Interestingly, despite the variations in clinical behavior, the long-term outcome of these patients remains excellent and similar to that of conventional PTC. In addition, total thyroidectomy and radioiodine ablation significantly improved the disease-specific survival in patients with conventional PTC, but did not benefit the survival of FVPTC and FTC patients (14). Based on current evidence, the overall management and prognosis of FVPTC would be assumed to be similar to that of conventional PTC. However, it is still important to diagnose and differentiate FVPTC clinically and pathologically until any consensus is reached.
As mentioned earlier, FVPTC is known to have a relatively benign appearance on ultrasonography, more similar to that of follicular neoplasm than PTC (19,20,21). However, there are few studies comparing the sonographic characteristics of FVPTC with those of conventional PTC. Yoon et al. (24) attempted to establish the sonographic findings of FVPTC and assess the role of preoperative FNA biopsy. The common sonographic findings of FVPTC were hypoechoic (51.9%), well-defined margins (51.9%), an oval shape (63%), and no microcalcifications (85.2%). Nevertheless, most lesions were correctly classified as malignant by both US and FNA biopsy. In our study, the sonographic findings of FVPTC patients were hypoechoic (60.2%), well-defined margins (80.7%), an oval shape (90.4%), and no microcalcifications (86.7%) (Table 2). Kim et al. (25) reported the sonographic features of FVPTC in comparison with conventional PTCs. The sonographic features of a taller-than-wide shape (5% vs. 22%), a spiculated margin (7% vs. 32%), marked hypoechogenicity (5% vs. 38%), and microcalcification (7% vs. 24%) were less common in FVPTCs than in conventional PTCs (all P < 0.05). In this study, marked hypoechogenicity was observed in the majority of FVPTCs and conventional PTCs (60.2% vs. 84.9%, P < 0.001).
At the present time, the incidence of PTMC (defined as thyroid tumor ≤ 1 cm in diameter) has increased. Therefore, we performed a comparison of US features between micro- and macro-FVPTC. Among the patients with FVPTC, the sonographic feature of marked hypoechogenicity was significantly less frequent in macro- than micro-FVPTCs (9.5% vs. 77.4%, P < 0.001). In the patients with macro-FVPTC, the FVPTCs were relatively lower when malignant components are present (14.3% vs. 79.0%, P < 0.001). In contrast, the conventional PTC group showed PTC-like features in US regardless of the size of the tumor (81% in micro-PTC vs. 90.6% in macro-PTC, P = 0.475). Based on this result, it may be hard to find differences among FVPTCs on US in cases of microcarcinoma.
In the most recent study, Rhee et al. (26) reported that patients with FVPTC with malignant US features (taller-than-wide shape, infiltrative margin, marked hypoechogenicity, and micro- or macrocalcifications) have a worse prognosis (e.g., lymph node metastasis, higher stage) than patients with FVPTC without malignant US features. FVPTCs were divided into PTC-like and FN-like groups based on US findings. PTC-like nodules were defined as having at least one accepted malignant feature. These authors suggested that US might help to predict the behavior of FVPTC. However, in our data, multifocality, extrathyroidal invasion, and lymph node metastasis were not significantly different between PTC-like FVPTCs and FN-like FVPTCs.
Our study had some limitations. First, this retrospective analysis was limited by the small sample size. In addition, the prevalence of PTC variants in Korea was previously reported as 6.7% (27,28). A large-scale prospective study would overcome these limitations. Second, although cytology specimens were evaluated by experienced pathologists, they did not use the defined criteria of the Bethesda System for Reporting Thyroid Cytopathology (29). This system can promote uniformity in the reporting of thyroid aspirates and is associated with defined risks of malignancy, allowing standardized management algorithms for each diagnosis. Third, FVPTCs were not divided into encapsulated and unencapsulated groups. It may differ from characteristics between two groups on US. Two distinct types of FVPTC are the common (or encapsulated) follicular variant with a less aggressive course and prognosis apparently similar to classical PTC, and the widely invasive (diffuse or multinodular) follicular variant (diffuse FVPTC) with a more aggressive course (30). Therefore, further distinction of US findings of the tumor may be helpful in order to define the clinical management strategy and prognosis.
In conclusion, FVPTCs showed fewer sonographically malignant features compared with conventional PTCs. In particular, FVPTCs larger than 1 cm had a more common benign sonographic appearance. Our data suggest that the possibility of FVPTC should be considered if the FNA result is suspicious for PTC in a nodule larger than 1 cm with no suspicious US features.
Footnotes
DISCLOSURE: There are no potential conflicts of interest relevant to this article to report.
AUTHOR CONTRIBUTION: Conception and coordination of the study: Jung ED. Consideration of ethical issues: Jeon EJ, Cho CH. Data collection and analysis: Jung ED, Shon HS, Park SW. Statistical analysis: Jeon EJ, Jung YJ. Manuscript approval: all authors.
References
- 1.Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–1214. doi: 10.1089/thy.2009.0110. [DOI] [PubMed] [Google Scholar]
- 2.Jossart GH, Clark OH. Well-differentiated thyroid cancer. Curr Probl Surg. 1994;31:933–1012. doi: 10.1016/0011-3840(94)90063-9. [DOI] [PubMed] [Google Scholar]
- 3.Kumar PV, Talei AR, Malekhusseini SA, Monabati A, Vasei M. Follicular variant of papillary carcinoma of the thyroid. A cytologic study of 15 cases. Acta Cytol. 1999;43:139–142. doi: 10.1159/000330967. [DOI] [PubMed] [Google Scholar]
- 4.Zidan J, Karen D, Stein M, Rosenblatt E, Basher W, Kuten A. Pure versus follicular variant of papillary thyroid carcinoma: clinical features, prognostic factors, treatment, and survival. Cancer. 2003;97:1181–1185. doi: 10.1002/cncr.11175. [DOI] [PubMed] [Google Scholar]
- 5.Tielens ET, Sherman SI, Hruban RH, Ladenson PW. Follicular variant of papillary thyroid carcinoma. A clinicopathologic study. Cancer. 1994;73:424–431. doi: 10.1002/1097-0142(19940115)73:2<424::aid-cncr2820730230>3.0.co;2-i. [DOI] [PubMed] [Google Scholar]
- 6.Lang BH, Lo CY, Chan WF, Lam AK, Wan KY. Classical and follicular variant of papillary thyroid carcinoma: a comparative study on clinicopathologic features and long-term outcome. World J Surg. 2006;30:752–758. doi: 10.1007/s00268-005-0356-7. [DOI] [PubMed] [Google Scholar]
- 7.Rosai J, Carcangiu ML, Delellis RA, editors. Atlas of tumor pathology. Tumors of the thyroid gland. Washington, D.C.: Armed Forces Institute of Pathology; 1992. pp. 42–121. [Google Scholar]
- 8.Hedinger C, Williams ED, Sobin LH, editors. Histological typing of thyroid tumours: World Health Organization international histological classification of tumours. 2nd ed. Berlin: Springer-Verlag; 1988. Papillary carcinoma; pp. 9–10. [Google Scholar]
- 9.Chang HY, Lin JD, Chou SC, Chao TC, Hsueh C. Clinical presentations and outcomes of surgical treatment of follicular variant of the papillary thyroid carcinomas. Jpn J Clin Oncol. 2006;36:688–693. doi: 10.1093/jjco/hyl093. [DOI] [PubMed] [Google Scholar]
- 10.Cardenas MG, Kini S, Wisgerhof M. Two patients with highly aggressive macrofollicular variant of papillary thyroid carcinoma. Thyroid. 2009;19:413–416. doi: 10.1089/thy.2008.0178. [DOI] [PubMed] [Google Scholar]
- 11.Liu L, Venkataraman G, Salhadar A. Follicular variant of papillary thyroid carcinoma with unusual late metastasis to the mandible and the scapula. Pathol Int. 2007;57:296–298. doi: 10.1111/j.1440-1827.2007.02092.x. [DOI] [PubMed] [Google Scholar]
- 12.Passler C, Prager G, Scheuba C, Niederle BE, Kaserer K, Zettinig G, Niederle B. Follicular variant of papillary thyroid carcinoma: a long-term follow-up. Arch Surg. 2003;138:1362–1366. doi: 10.1001/archsurg.138.12.1362. [DOI] [PubMed] [Google Scholar]
- 13.Burningham AR, Krishnan J, Davidson BJ, Ringel MD, Burman KD. Papillary and follicular variant of papillary carcinoma of the thyroid: initial presentation and response to therapy. Otolaryngol Head Neck Surg. 2005;132:840–844. doi: 10.1016/j.otohns.2005.02.002. [DOI] [PubMed] [Google Scholar]
- 14.Yu XM, Schneider DF, Leverson G, Chen H, Sippel RS. Follicular variant of papillary thyroid carcinoma is a unique clinical entity: a population-based study of 10,740 cases. Thyroid. 2013;23:1263–1268. doi: 10.1089/thy.2012.0453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Baloch ZW, Gupta PK, Yu GH, Sack MJ. LiVolsi VA. Follicular variant of papillary carcinoma. Cytologic and histologic correlation. Am J Clin Pathol. 1999;111:216–222. doi: 10.1093/ajcp/111.2.216. [DOI] [PubMed] [Google Scholar]
- 16.Moon WJ, Jung SL, Lee JH, Na DG, Baek JH, Lee YH, Kim J, Kim HS, Byun JS, Lee DH. Benign and malignant thyroid nodules: US differentiation--multicenter retrospective study. Radiology. 2008;247:762–770. doi: 10.1148/radiol.2473070944. [DOI] [PubMed] [Google Scholar]
- 17.Chan BK, Desser TS, McDougall IR, Weigel RJ, Jeffrey RB., Jr Common and uncommon sonographic features of papillary thyroid carcinoma. J Ultrasound Med. 2003;22:1083–1090. doi: 10.7863/jum.2003.22.10.1083. [DOI] [PubMed] [Google Scholar]
- 18.Hoang JK, Lee WK, Lee M, Johnson D, Farrell SU. Features of thyroid malignancy: pearls and pitfalls. Radiographics. 2007;27:847–860. doi: 10.1148/rg.273065038. [DOI] [PubMed] [Google Scholar]
- 19.Komatsu M, Hanamura N, Tsuchiya S, Seki T, Kuroda T. Preoperative diagnosis of the follicular variant of papillary carcinoma of the thyroid: discrepancy between image and cytologic diagnoses. Radiat Med. 1994;12:293–299. [PubMed] [Google Scholar]
- 20.Rago T, Di Coscio G, Basolo F, Scutari M, Elisei R, Berti P, Miccoli P, Romani R, Faviana P, Pinchera A, et al. Combined clinical, thyroid ultrasound and cytological features help to predict thyroid malignancy in follicular and Hupsilonrthle cell thyroid lesions: results from a series of 505 consecutive patients. Clin Endocrinol (Oxf) 2007;66:13–20. doi: 10.1111/j.1365-2265.2006.02677.x. [DOI] [PubMed] [Google Scholar]
- 21.Baloch ZW, Tam D, Langer J, Mandel S. LiVolsi VA, Gupta PK. Ultrasound-guided fine-needle aspiration biopsy of the thyroid: role of on-site assessment and multiple cytologic preparations. Diagn Cytopathol. 2000;23:425–429. doi: 10.1002/1097-0339(200012)23:6<425::aid-dc14>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 22.Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A 3rd, editors. AJCC cancer staging manual. 7th ed. New York, NY: Springer; 2010. [Google Scholar]
- 23.Leenhardt L, Bernier MO, Boin-Pineau MH, Conte Devolx B, Maréchaud R, Niccoli-Sire P, Nocaudie M, Orgiazzi J, Schlumberger M, Wémeau JL, et al. Advances in diagnostic practices affect thyroid cancer incidence in France. Eur J Endocrinol. 2004;150:133–139. doi: 10.1530/eje.0.1500133. [DOI] [PubMed] [Google Scholar]
- 24.Yoon JH, Kim EK, Hong SW, Kwak JY, Kim MJ. Sonographic features of the follicular variant of papillary thyroid carcinoma. J Ultrasound Med. 2008;27:1431–1437. doi: 10.7863/jum.2008.27.10.1431. [DOI] [PubMed] [Google Scholar]
- 25.Kim DS, Kim JH, Na DG, Park SH, Kim E, Chang KH, Sohn CH, Choi YH. Sonographic features of follicular variant papillary thyroid carcinomas in comparison with conventional papillary thyroid carcinomas. J Ultrasound Med. 2009;28:1685–1692. doi: 10.7863/jum.2009.28.12.1685. [DOI] [PubMed] [Google Scholar]
- 26.Rhee SJ, Hahn SY, Ko ES, Ryu JW, Ko EY, Shin JH. Follicular variant of papillary thyroid carcinoma: distinct biologic behavior based on ultrasonographic features. Thyroid. 2014;24:683–688. doi: 10.1089/thy.2013.0351. [DOI] [PubMed] [Google Scholar]
- 27.Park JY, Lee JI, Tan AH, Jang HW, Shin HW, Oh YL, Shin JH, Kim JH, Kim JS, Son YL, et al. Clinical differences between classic papillary thyroid carcinoma and variants. J Korean Endocr Soc. 2009;24:165–173. [Google Scholar]
- 28.Kim KW. Clinical characteristics of papillary thyroid cancer in Korea. J Korean Thyroid Assoc. 2010;3:111–115. [Google Scholar]
- 29.Cibas ES, Ali SZ. The Bethesda system for reporting thyroid cytopathology. Thyroid. 2009;19:1159–1165. doi: 10.1089/thy.2009.0274. [DOI] [PubMed] [Google Scholar]
- 30.Ivanova R, Soares P, Castro P, Sobrinho-Simões M. Diffuse (or multinodular) follicular variant of papillary thyroid carcinoma: a clinicopathologic and immunohistochemical analysis of ten cases of an aggressive form of differentiated thyroid carcinoma. Virchows Arch. 2002;440:418–424. doi: 10.1007/s00428-001-0543-3. [DOI] [PubMed] [Google Scholar]