

Abstract
We tested correlations between anti-Helicobacter pylori IgG and IgA levels and the urease test, anti-CagA protein antibody, degree of gastritis, and age. In total, 509 children (0–15 years) were enrolled. Subjects were stratified as 0–4 years (n = 132), 5–9 years (n = 274), and 10–15 years (n = 103) and subjected to the urease test, histopathology, ELISA, and western blot using whole-cell lysates of H. pylori strain 51. The positivity rate in the urease test (P = 0.003), the degree of chronic gastritis (P = 0.021), and H. pylori infiltration (P < 0.001) increased with age. The median titer for anti-H. pylori IgG was 732.5 IU/mL at 0–4 years, 689.0 IU/mL at 5–9 years, and 966.0 IU/mL at 10–15 years (P < 0.001); the median titer for anti-H. pylori IgA was 61.0 IU/mL at 0–4 years, 63.5 IU/mL at 5–9 years, and 75.0 IU/mL at 10–15 years (P < 0.001). The CagA-positivity rate was 26.5% at 0–4 years, 36.5% at 5–9 years, and 46.6% at 10–15 years for IgG (P = 0.036), and 11.3% at 0–4 years, 18.6% at 5–9 years, and 23.3% at 10–15 years for IgA (P < 0.001). Anti-H. pylori IgG and IgA titers increased with the urease test grade, chronic gastritis degree, active gastritis, and H. pylori infiltration. Presence of CagA-positivity is well correlated with a high urease test grade and high anti-H. pylori IgG/IgA levels.
Keywords: Antibodies IgG/IgA, Helicobacter pylori, CagA Protein, Urease, Children
Graphical Abstract
INTRODUCTION
Helicobacter pylori is an important etiological factor for acute and chronic gastritis, gastric and duodenal ulcers, and gastric adenocarcinoma (1). The severity of H. pylori infection depends on the strain virulence, host susceptibility, and environmental factors (2). The measurement of specific antibodies in serum has been used as a noninvasive method for detecting H. pylori infection (3) and over 90% of H. pylori-infected patients have detectable serum IgG antibodies (4). Serological tests are commercially available, which are easy to perform and inexpensive, but studies on children indicate a high sensitivity range of 50%–90% and the specificity ranges from 83% to 100% (5,6,7,8).
The number of immunoreactive bands significantly increases with age and reactions to the VacA and CagA antigens are more frequently found in older children (9). In our previous study, we found that more than 80% of the seropositive enzyme-linked immunosorbent assay (ELISA) results were CagA positive, whereas the other 20% of the seropositive results using ELISA could be attributed to its reaction with another H. pylori antigen (10). Therefore, the use of whole-cell lysates of H. pylori strain 51 in ELISA may increase the yield when detecting anti-H. pylori antibodies in the Korean population.
Several studies have investigated the relationship between antibody titers and the pathogenesis of H. pylori, but the results are inconclusive (3,11). Quantitative evaluations of anti-H. pylori antibodies or against H. pylori recombinant purified proteins have been performed in some human diseases where H. pylori infections may play a role in their pathogenesis (9,12,13,14). However, the clinical significance of high antibody levels to H. pylori according to quantitative ELISA has not been established and high anti-H. pylori antibody levels have not been demonstrated to be predictive of the severity of gastroduodenal diseases or the density of H. pylori colonization.
Thus, to help identify factors that correlate with antibody levels in children, we evaluated the correlations between the levels of anti-H. pylori IgG and IgA antibodies and the urease test grade, presence of CagA antigen, degree of gastritis, and age.
MATERIALS AND METHODS
Study population
As a member of the National Biobank of Korea, Gyeongsang National University Hospital (GNUH) collects serum samples from random patients and stores them at −80℃. Among the samples collected over 21 years, we examined those from 509 children who underwent upper gastroduodenoscopy at GNUH during 1991–2010. Thus, we enrolled 509 children and we reviewed the results of urease test and the histopathological findings, and tested the reserved serum. The sera were stratified into three age groups: 0–4 years (n = 132), 5–9 years (n = 274), and 10–15 years (n = 103) (Table 1).
Table 1. Baseline and clinical characteristics.
| Characteristics | No. (%) of children by age groups | P value | ||
|---|---|---|---|---|
| 0-4 yr | 5-9 yr | 10-15 yr | ||
| Number | 132 | 274 | 103 | 0.509 |
| Sex | 0.999 | |||
| Female | 60 (45.5) | 125 (45.6) | 47 (45.6) | |
| Male | 72 (54.5) | 149 (54.4) | 56 (54.4) | |
| Histopathological findings | 0.021 | |||
| Chronic gastritis | ||||
| Normal | 4 (3.0) | 4 (1.4) | 0 (0) | |
| Mild | 94 (71.2) | 211 (77.0) | 64 (62.1) | |
| Moderate | 28 (21.2) | 46 (16.8) | 28 (27.2) | |
| Severe | 6 (4.5) | 13 (4.7) | 11 (10.7) | |
| Active gastritis | 0.064 | |||
| Normal | 103 (78.0) | 214 (78.1) | 65 (63.1) | |
| Mild | 20 (15.2) | 44 (16.1) | 27 (26.2) | |
| Moderate | 9 (6.8) | 13 (4.7) | 9 (8.7) | |
| Severe | 0 (0) | 3 (1.1) | 2 (1.9) | |
| H. pylori infiltration | < 0.001 | |||
| Normal | 98 (74.2) | 216 (78.8) | 62 (60.2) | |
| Mild | 29 (22.0) | 46 (16.8) | 28 (27.2) | |
| Moderate | 2 (1.5) | 11 (4.0) | 12 (11.7) | |
| Severe | 3 (2.3) | 1 (0.4) | 1 (1.0) | |
| Urease test | 0.003 | |||
| Negative | 83 (62.9) | 170 (62.0) | 62 (60.2) | |
| 6-24 hr | 21 (15.9) | 49 (17.9) | 5 (4.9) | |
| < 6 hr | 28 (21.2) | 55 (20.1) | 36 (35.0) | |
Urease tests and histopathological findings
Three gastric endoscopic biopsies taken from the gastric prepyloric antrum with an Olympus GIF-XP endoscope with pediatric forceps were first subjected to urease tests, which were performed in the endoscopy room. Based on the rapidity of the color change, the subjects were designated as grades 0 (negative, no color change), 1 (color change between 6 and 24 hours), or 2 (color change within 6 hours).
Three biopsy specimens each from the gastric antrum and gastric body were stained with hematoxylin-eosin for the histological analyses. The histology results were interpreted according to the Updated Sydney System. All of the histopathological slides that we reviewed had been prepared and donated by the GNUH.
ELISA and western blot analysis
Anti-H.pylori IgG and IgA titers were measured by ELISA (10) using the coated with the prepared whole cell proteins of H. pylori strain 51 (10 µg/mL and 50 µL per well diluted with coating buffer). Diluted sera (IgG 1:400, and IgA 1:100) were added to antigen-coated wells (50 µL per well).
Anti-CagA IgG and IgA antibodies were evaluated by western blot using whole-cell lysates of H. pylori strain 51 (15). The western blot patterns were assigned to four categories on the basis of CagA (pattern I), urease without CagA (pattern II), other proteins except CagA and urease (pattern III), and no band (pattern IV) (Fig. 1).
Fig. 1.

The immunoblot assay results were classified into four patterns on the basis of immunoreactive bands. Only pattern I, with reactivity against 120-kDa antigens and other H. pylori antigens, was considered to be a specific marker of H. pylori infection in this study. Panel A shows the Ponceau S‐stained nitrocellulose membrane onto which the marker proteins and separated H. pylori antigen were transferred.
Statistical analysis
The statistical analyses were performed using IBM SPSS Statistics 21 (IBM, Chicago, IL, USA). We tested whether the antibody titer had significant correlations with the urease test results, antigen patterns, or age. We used bivariate correlation (Spearman’s rho), paired samples t-tests, and nonparametric tests to analyze the differences in the antibody titers between CagA-positive and-negative sera, among the three urease test grades, and in the three age groups. The numbers and sex ratios in the three age groups were different, so GLM regression analysis was used for correction. Post-hoc analysis using Scheffé’s method was applied when significant differences were detected among three groups. Statistically significant differences were accepted at P < 0.05.
Ethics statement
The study protocol was reviewed and approved by the institutional review board of GNUH (GNUHIRB-2015-08-020). Informed consent was exempted by the board.
RESULTS
Study population
Table 1 shows the number and sex distribution of the subjects according to age. There were no significant differences in the sex distributions among the age groups.
Results of the urease test and histopathological findings
The positivity rates for the urease test were 37.1% at 0–4 years, 38.0% at 5–9 years, and 39.9% at 10–15 years (P = 0.003). The degrees of chronic gastritis (P = 0.021), active gastritis (P = 0.064), and H. pylori infiltration (P < 0.001) increased with age (Table 1).
Anti-H. pylori IgG and IgA titers
The median titers for anti-H. pylori IgG were 732.5 IU/mL at 0–4 years, 689.0 IU/mL at 5–9 years, and 966.0 IU/mL at 10–15 years (P < 0.001). The median titers for anti-H. pylori IgA were 61.0 IU/mL at 0–4 years, 63.5 IU/mL at 5–9 years, and 75.0 IU/mL at 10–15 years (P < 0.001). The anti-H. pylori IgG titers were higher at 10–15 years than those at 1–5 years and 6–10 years (P = 0.006), but there was no significant difference in the anti-H. pylori IgA titers among the three age groups (P = 0.454).
Western blot patterns according to age groups
The proportions of IgG positivity according to the four western blot patterns (I–IV) were 36.0%, 47.7%, 5.5%, and 10.8%, respectively (P = 0.008). The proportions of IgA positivity according to the four patterns were 17.7%, 33.8%, 23.6%, and 25.0%, respectively (P = 0.221). The CagA-positivity rates were 26.5% at 0–4 years, 36.5% at 5–9 years, and 46.6% at 10–15 years for IgG (P = 0.036, Fig. 2), and 11.4% at 0–4 years, 18.6% at 5–9 years, and 23.3% at 10–15 years for IgA (P < 0.001) (Table 2). The western blot negative (no band) rates for IgG were 13.6%, 8.8%, and 12.6% at 0–4 years, 5–9 years, and 10–15 years, respectively. Post-hoc analysis using Scheffé’s method detected no differences in the proportions of the four western blot patterns among the three age groups for IgG (P = 0.094) and for IgA (P = 0.161).
Fig. 2.

Proportions with the four western blot patterns according to age groups. The CagA-positivity rate was 26.5% at 0–4 years, 36.5% at 5–9 years, and 46.6% at 10–15 years for IgG (P = 0.036). Post-hoc analysis using Scheffé’s method detected no differences in the proportions with the four western blot pattern among the three age groups for IgG (P = 0.094).
Table 2. Proportions with the four western blot patterns according to age groups.
| Target proteins | No. (%) of children by age group | |||
|---|---|---|---|---|
| 0–4 yr | 5–9 yr | 10–15 yr | ||
| CagA | IgG | 35 (26.5) | 100 (36.5) | 48 (46.6) |
| IgA | 15 (11.4) | 51 (18.6) | 24 (23.3) | |
| Urease | IgG | 72 (54.5) | 133 (48.5) | 38 (36.9) |
| IgA | 39 (29.5) | 97 (35.4) | 36 (35.0) | |
| Other proteins | IgG | 7 (5.3) | 17 (6.2) | 4 (3.9) |
| IgA | 52 (39.4) | 51 (18.6) | 17 (16.5) | |
| No band | IgG | 18 (13.6) | 24 (8.8) | 13 (12.6) |
| IgA | 26 (19.7) | 75 (27.4) | 26 (25.2) | |
Correlations between the urease test grade, degree of histopathological findings, western blot patterns, and antibody titers for IgG and IgA
The titers of anti-H. pylori IgG antibodies increased with the urease test grade (r = 0.527, P < 0.001), chronic gastritis (r = 0.613, P < 0.001), active gastritis (r = 0.545, P < 0.001), and the degree of H. pylori infiltration (r = 0.593, P < 0.001). The anti-H. pylori IgA titers also increased with the urease test grade (r = 0.450, P < 0.001), degree of chronic gastritis (r = 0.523, P < 0.001), active gastritis (r = 0.453, P < 0.001), and H. pylori infiltration (r = 0.480, P < 0.001). In the urease test, the anti-H. pylori IgG (Fig. 3) and IgA (Fig. 4) antibody titers were higher with grade I than the other grades (P < 0.001), regardless of age. According to the four western blot patterns, the anti-H. pylori IgG (Fig. 5) and IgA (Fig. 6) titers were higher with the CagA-positive pattern (P < 0.001), regardless of age.
Fig. 3.

Anti-H. pylori IgG antibody titers according to age groups and the urease test grade. The anti-H. pylori IgG antibody titers were higher with grade I (positive within 6 hours) than the other grades (P < 0.001) in all age groups.
Fig. 4.

Anti-H. pylori IgA antibody titers according to age groups and the urease test grade. The anti-H. pylori IgA antibody titers were higher with grade I (positive within 6 hours) than the other grades (P < 0.001) in all age groups.
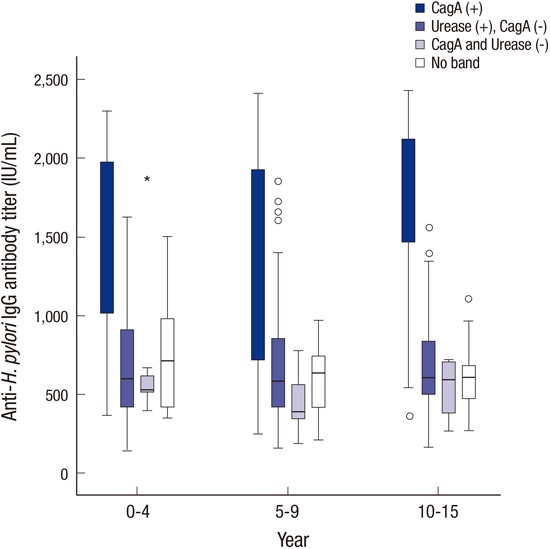
Fig. 5.

Anti-H. pylori IgG antibody titers according to the western blot patterns and age. The anti-H. pylori IgG antibody titers were higher with the CagA-positive pattern (P < 0.001) regardless of age.
Fig. 6.

Anti-H. pylori IgA antibody titers according to the western blot patterns and age. The anti-H. pylori IgA antibody titers were higher with the CagA-positive pattern (P < 0.001) regardless of age.
DISCUSSION
In the present study, we found that the presence of the CagA antigen was the major factor related to high levels of anti-H. pylori IgG and IgA antibodies, regardless of age. CagA is known to be an important virulence factor in H. pylori (14) and antibodies against CagA have been observed in gastritis, gastroduodenal ulcer, and gastric cancer patients (13,16,17). In the early 2000s, 80%–100% of H. pylori strains possessed the cagA gene in East Asia (18,19) and 94% were cagA-positive in H. pylori DNA extracts from 33 Korean children (20). In Japan, the CagA was the most reactive antigen recognized by all the H. pylori positive sera even from children under the age of 3 year (21). Therefore, the regional CagA antigens for serodiagnosis of H. pylori would be important, which could affect the rate of seropositivity (21). Thus, a positive test result for anti-CagA antibody was regarded as an H. pylori infection in Korean studies (15,22). In the present study, the highest positivity rate for CagA was 46.6% among the 10–15 years group, although this CagA-positivity rate is lower than the seroprevalence (59.6%) of H. pylori infections in a recent study of the general population in Korea (23), as well as the seroprevalence rate (68.0% CagA-positive) in children aged 6–15 years using the same immunoblot analysis during 1998–1999 (17). Recent seroprevalence studies of H. pylori infection suggest that the decrease in the seroprevalence of H. pylori may be related to the improved socioeconomic status of Koreans (23,24)
Young children may have a different immune response to H. pylori, with preferences for specific antigens, as well as lower titers than adults (8). A lower sensitivity has been reported based on serological H. pylori tests in children compared with adults (25). Using commercial ELISA kits, false-negative results were found more often in children aged younger than 5 years (8,26). In our previous study, we showed that the Genedia IgG ELISA kit, which uses H. pylori antigen obtained from a Korean H. pylori strain, achieved a higher seropositivity rate than other ELISA kits (e.g., GAP IgG, HM-CAP, and Pyloriset EIA-G obtained from USA and Finland) (17). There are differences in the antigenicity of multiple H. pylori strains and even among different antigens in the same strain (9). In the present study, the median levels of anti-H. pylori IgG and IgA antibody also increased with age but the antibody titers were higher in the CagA-positive cases than those in the CagA-negative cases, even in children aged under 5 years.
Age is strongly related to H. pylori infections (27). In the present study, the degree of chronic gastritis, active gastritis, and H. pylori infiltration and the positive urease test rate increased significantly with age. The CagA-positivity rate increased with age but not significantly. Previously, the grades of active and chronic inflammation, atrophy, lymphoid follicles, and H. pylori density were correlated with the IgG antibody levels in the antral mucosa (3,11,28). The serum antibody response to H. pylori also depends on the severity of H. pylori-associated diseases (29). In the present study, the anti-H. pylori IgG and IgA antibody levels were correlated with the degree of chronic gastritis and H. pylori infiltration. The degrees of the histopathological findings and the anti-H. pylori IgG and IgA antibody titers were also correlated with the ages of the children.
A positive urease test within 6 h was another factor that affected the anti-H. pylori IgG and IgA antibody levels regardless of age. Buffered urease tests require at least 1000 organisms to generate a positive reaction (30) and a higher degree of H. pylori infiltration is correlated with a faster positive reaction in the urease test (31,32). Therefore, a rapid reaction in the urease test may be related to a high density of bacteria. In the present study, there was no significant correlation between the presence of anti-urease antibody, the titer of anti-H. pylori antibodies, and the urease test grade. The change in H. pylori strains from CagA-positive to CagA-negative in Korea should be considered when evaluating the seroepidemiology of H. pylori infections.
The current study had some limitations as follows. We conducted the current study with a retrospective design. We simply analyzed the results of urease tests and histopathological findings in this study, and we did not evaluate the clinical histories of the children.
In summary, we found that the anti-H. pylori IgG and IgA antibody titers were higher in the CagA-positive sera of children regardless of age, while higher IgG and IgA titers were observed with a higher degree of active gastritis and H. pylori infiltration, higher urease test grade, and greater age. In conclusion, the presence of CagA antigen is the main factor that affects the levels of anti-H. pylori IgG and IgA antibodies regardless of age. The ELISA test is a valuable diagnostic tool for diagnosing CagA-positive H. pylori infections in children. However, further studies are needed of CagA-negative strain infections and the levels of anti-H. pylori IgG and IgA antibodies.
ACKNOWLEDGMENT
The serum samples used in this study were provided by the Gyeongsang National University Hospital, which is a member of the National Biobank of Korea, which is supported by the Ministry of Health, Welfare and Family Affairs. All samples derived from the National Biobank of Korea were obtained with informed consent under institutional review board approved protocols.
Footnotes
Funding: This study was supported by a grant from the National R&D Program for Cancer Control of the Ministry of Health & Welfare of the Republic of Korea (0820050).
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Research conception & design: Seo JH, Youn HS, Cho MJ, Rhee KH. Performing the experiments: Lim CW, Jun JS, Baik SC, Lee WK. Data acquisition: Seo JH, Park JS, Yeom JS, Lim JY, Woo HO, Youn HS. Data analysis and interpretation: Seo JH, Cho MJ. Statistical analysis: Seo JH, Youn HS. Drafting of the manuscript: Seo JH, Lim CW, Jun JS, Youn HS. Critical revision of the manuscript: Seo JH, Woo HO, Youn HS. Receiving grant: Youn HS. Approval of final manuscript: all authors.
References
- 1.McColl KE. Clinical practice. Helicobacter pylori infection. N Engl J Med. 2010;362:1597–1604. doi: 10.1056/NEJMcp1001110. [DOI] [PubMed] [Google Scholar]
- 2.Malaty HM. Epidemiology of Helicobacter pylori infection. Best Pract Res Clin Gastroenterol. 2007;21:205–214. doi: 10.1016/j.bpg.2006.10.005. [DOI] [PubMed] [Google Scholar]
- 3.Chen TS, Li FY, Chang FY, Lee SD. Immunoglobulin G antibody against Helicobacter pylori: clinical implications of levels found in serum. Clin Diagn Lab Immunol. 2002;9:1044–1048. doi: 10.1128/CDLI.9.5.1044-1048.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schumann C, Triantafilou K, Rasche FM, Möricke A, Vogt K, Triantafilou M, Hahn P, Schneider EM, Lepper PM. Serum antibody positivity for distinct Helicobacter pylori antigens in benign and malignant gastroduodenal disease. Int J Med Microbiol. 2006;296:223–228. doi: 10.1016/j.ijmm.2006.02.009. [DOI] [PubMed] [Google Scholar]
- 5.de Oliveira AM, Rocha GA, Queiroz DM, Mendes EN, de Carvalho AS, Ferrari TC, Nogueira AM. Evaluation of enzyme-linked immunosorbent assay for the diagnosis of Helicobacter pylori infection in children from different age groups with and without duodenal ulcer. J Pediatr Gastroenterol Nutr. 1999;28:157–161. doi: 10.1097/00005176-199902000-00012. [DOI] [PubMed] [Google Scholar]
- 6.Raymond J, Kalach N, Bergeret M, Barbet JP, Benhamou PH, Gendrel D, Dupont C. Evaluation of a serological test for diagnosis of Helicobacter pylori infection in children. Eur J Clin Microbiol Infect Dis. 1996;15:415–417. doi: 10.1007/BF01690102. [DOI] [PubMed] [Google Scholar]
- 7.Raymond J, Sauvestre C, Kalach N, Bergeret M, Dupont C. Immunoblotting and serology for diagnosis of Helicobacter pylori infection in children. Pediatr Infect Dis J. 2000;19:118–121. doi: 10.1097/00006454-200002000-00008. [DOI] [PubMed] [Google Scholar]
- 8.Kindermann A, Konstantopoulos N, Lehn N, Demmelmair H, Koletzko S. Evaluation of two commercial enzyme immunoassays, testing immunoglobulin G (IgG) and IgA responses, for diagnosis of Helicobacter pylori infection in children. J Clin Microbiol. 2001;39:3591–3596. doi: 10.1128/JCM.39.10.3591-3596.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rocha GA, Oliveira AM, Queiroz DM, Carvalho AS, Nogueira AM. Immunoblot analysis of humoral immune response to Helicobacter pylori in children with and without duodenal ulcer. J Clin Microbiol. 2000;38:1777–1781. doi: 10.1128/jcm.38.5.1777-1781.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Seo JH, Jun JS, Youn HS, Yeom JS, Park JS, Park CH, Woo HO, Lee WK, Cho MJ, Rhee KH. Development of an ELISA for quantitative detection of immunoglobulin G (IgG) and IgA antibodies to Helicobacter pylori for use in Korean pediatric patients with H. pylori-associated diseases. Gut Liver. 2013;7:437–442. doi: 10.5009/gnl.2013.7.4.437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sheu BS, Shiesh SC, Yang HB, Su IJ, Chen CY, Lin XZ. Implications of Helicobacter pylori serological titer for the histological severity of antral gastritis. Endoscopy. 1997;29:27–30. doi: 10.1055/s-2007-1004057. [DOI] [PubMed] [Google Scholar]
- 12.Yokota S, Amano K, Fujii N, Yokochi T. Comparison of serum antibody titers to Helicobacter pylori lipopolysaccharides, CagA, VacA and partially purified cellular extracts in a Japanese population. FEMS Microbiol Lett. 2000;185:193–198. doi: 10.1111/j.1574-6968.2000.tb09061.x. [DOI] [PubMed] [Google Scholar]
- 13.Gao L, Michel A, Weck MN, Arndt V, Pawlita M, Brenner H. Helicobacter pylori infection and gastric cancer risk: evaluation of 15 H. pylori proteins determined by novel multiplex serology. Cancer Res. 2009;69:6164–6170. doi: 10.1158/0008-5472.CAN-09-0596. [DOI] [PubMed] [Google Scholar]
- 14.Satomi S, Yamakawa A, Matsunaga S, Masaki R, Inagaki T, Okuda T, Suto H, Ito Y, Yamazaki Y, Kuriyama M, et al. Relationship between the diversity of the cagA gene of Helicobacter pylori and gastric cancer in Okinawa, Japan. J Gastroenterol. 2006;41:668–673. doi: 10.1007/s00535-006-1838-6. [DOI] [PubMed] [Google Scholar]
- 15.Jeong HL, Jung YS, Jun JS, Yeom JS, Park JS, Seo JH, Lim JY, Park CH, Woo HO, Youn HS, et al. Comparison of four commercial ELISA kits and in-house immunoblotting for diagnosis of Helicobacter pylori infection. Pediatr Gastroenterol Hepatol Nutr. 2012;15:85–90. [Google Scholar]
- 16.Holtmann G, Talley NJ, Mitchell H, Hazell S. Antibody response to specific H. pylori antigens in functional dyspepsia, duodenal ulcer disease, and health. Am J Gastroenterol. 1998;93:1222–1227. doi: 10.1111/j.1572-0241.1998.00399.x. [DOI] [PubMed] [Google Scholar]
- 17.Blaser MJ, Perez-Perez GI, Kleanthous H, Cover TL, Peek RM, Chyou PH, Stemmermann GN, Nomura A. Infection with Helicobacter pylori strains possessing cagA is associated with an increased risk of developing adenocarcinoma of the stomach. Cancer Res. 1995;55:2111–2115. [PubMed] [Google Scholar]
- 18.Yamazaki S, Yamakawa A, Okuda T, Ohtani M, Suto H, Ito Y, Yamazaki Y, Keida Y, Higashi H, Hatakeyama M, et al. Distinct diversity of vacA, cagA, and cagE genes of Helicobacter pylori associated with peptic ulcer in Japan. J Clin Microbiol. 2005;43:3906–3916. doi: 10.1128/JCM.43.8.3906-3916.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wong BC, Yin Y, Berg DE, Xia HH, Zhang JZ, Wang WH, Wong WM, Huang XR, Tang VS, Lam SK. Distribution of distinct vacA, cagA and iceA alleles in Helicobacter pylori in Hong Kong. Helicobacter. 2001;6:317–324. doi: 10.1046/j.1523-5378.2001.00040.x. [DOI] [PubMed] [Google Scholar]
- 20.Ko JS, Kim KM, Oh YL, Seo JK. cagA, vacA, and iceA genotypes of Helicobacter pylori in Korean children. Pediatr Int. 2008;50:628–631. doi: 10.1111/j.1442-200X.2008.02641.x. [DOI] [PubMed] [Google Scholar]
- 21.Akada J, Okuda M, Hiramoto N, Kitagawa T, Zhang X, Kamei S, Ito A, Nakamura M, Uchida T, Hiwatani T, et al. Proteomic characterization of Helicobacter pylori CagA antigen recognized by child serum antibodies and its epitope mapping by peptide array. PLoS One. 2014;9:e104611. doi: 10.1371/journal.pone.0104611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kim EA, Kim YO, Lim JY, Jung YS, Park CH, Woo HO, Youn HS, Ko GH, Baik SC, Lee WK, et al. Antibody response of infants to Helicobacter pylori infection. Korean J Gastroenterol. 2000;35:704–715. [Google Scholar]
- 23.Yim JY, Kim N, Choi SH, Kim YS, Cho KR, Kim SS, Seo GS, Kim HU, Baik GH, Sin CS, et al. Seroprevalence of Helicobacter pylori in South Korea. Helicobacter. 2007;12:333–340. doi: 10.1111/j.1523-5378.2007.00504.x. [DOI] [PubMed] [Google Scholar]
- 24.Kim HY, Kim N, Kim SM, Seo JH, Park EH, Lee DH. Seroprevalence of Helicobacter pylori infection in Korean health personnel. Gut Liver. 2013;7:648–654. doi: 10.5009/gnl.2013.7.6.648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Crabtree JE, Mahony MJ, Taylor JD, Heatley RV, Littlewood JM, Tompkins DS. Immune responses to Helicobacter pylori in children with recurrent abdominal pain. J Clin Pathol. 1991;44:768–771. doi: 10.1136/jcp.44.9.768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Corvaglia L, Bontems P, Devaster JM, Heimann P, Glupczynski Y, Keppens E, Cadranel S. Accuracy of serology and 13C-urea breath test for detection of Helicobacter pylori in children. Pediatr Infect Dis J. 1999;18:976–979. doi: 10.1097/00006454-199911000-00008. [DOI] [PubMed] [Google Scholar]
- 27.Pounder RE, Ng D. The prevalence of Helicobacter pylori infection in different countries. Aliment Pharmacol Ther. 1995;9(Suppl 2):33–39. [PubMed] [Google Scholar]
- 28.Hsu PI, Lai KH, Tseng HH, Liu YC, Yen MY, Lin CK, Lo GH, Huang RL, Huang JS, Cheng JS, et al. Correlation of serum immunoglobulin G Helicobacter pylori antibody titers with histologic and endoscopic findings in patients with dyspepsia. J Clin Gastroenterol. 1997;25:587–591. doi: 10.1097/00004836-199712000-00007. [DOI] [PubMed] [Google Scholar]
- 29.Chomvarin C, Ottiwet O, Hahnvajanawong C, Intapan PM, Wongwajana S. Seroreactivity to specific antigens of Helicobacter pylori infection is associated with an increased risk of the dyspeptic gastrointestinal diseases. Int J Infect Dis. 2009;13:647–654. doi: 10.1016/j.ijid.2008.12.013. [DOI] [PubMed] [Google Scholar]
- 30.Graham DY. Helicobacter pylori and the endoscopist: whether to diagnose. Gastrointest Endosc. 1991;37:577–579. doi: 10.1016/s0016-5107(91)70838-9. [DOI] [PubMed] [Google Scholar]
- 31.Seo JH, Youn HS, Park JJ, Yeom JS, Park JS, Jun JS, Lim JY, Park CH, Woo HO, Ko GH, et al. Influencing factors to results of the urease test: age, sampling site, histopahtologic findings, and density of Helicobacter pylori . Pediatr Gastroenterol Hepatol Nutr. 2013;16:34–40. doi: 10.5223/pghn.2013.16.1.34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Seo JH, Park JS, Yeom JS, Lim JY, Park CH, Woo HO, Baik SC, Lee WK, Cho MJ, Rhee KH, et al. Correlation between positive rate and number of biopsy samples on urease test in childhood Helicobacter pylori infection. J Korean Med Sci. 2014;29:106–109. doi: 10.3346/jkms.2014.29.1.106. [DOI] [PMC free article] [PubMed] [Google Scholar]