

Abstract
Objectives
To evaluate vocal fatigue by using objective and subjective measurements of dose recorded by the National Center for Voice and Speech (NCVS) Dosimeter™ (Dosimeter).
Study Design and Setting
Seven subjects completed a two-week study period. The Dosimeter recorded vocal load, soft phonation tasks and subjective soft voice ratings. Three vocal doses (time, distance, and cycle) were measured in classical singers' larynges during an intensive practice period.
Results
Spikes in vocal load are reflected as harsher subjective ratings on the same day as well as 24–72 hours later. When at least 48 hours of vocal rest occurred before a vocal load, improved subjective evaluations were seen after the load.
Conclusions
The NCVS Dosimeter appears to be an effective tool for data collection on prolonged use of the voice.
Significance
This is the first multi-day study comparing objective and subjective data on vocal fatigue in a group of professional singers.
Background/Introduction
Vocal loading is defined as the demands placed on the voice organ by voice use needs.1 Acute laryngeal injuries due to high vocal loading, such as submucosal hemorrhages, or chronic changes like nodules can lead to missed performances, lost revenue, and significant rehabilitation periods. Vocal fatigue often presents clinically in the period immediately preceding a major performance as a feeling of laryngeal discomfort, along with an increase in vocal or respiratory effort needed to produce a normal tone. These symptoms likely reflect both neuro-muscular and lamina propria fatigue.2 The question of work-related vocal loads causing vocal injury is increasingly being approached as an occupational safety and health (OSH) issue.1, 3
Most research on vocal fatigue has been conducted on teachers and daycare workers who, due to the vocal demands of their work and acoustically poor environments, injure their voices or acquire compensatory habits. Studies on teachers historically have combined fundamental frequency (F0), voicing time, average sound pressure level (SPL) over a teaching day or a portion of a teaching day, and background noise levels. Amplification and vocal technique instruction to assist teachers with their vocal loading issues have been tested.4, 5 Unfortunately, singers cannot always use amplification due to stylistic considerations or performance hall restrictions. Occupational safety issues will become increasingly important for professional singers and actors. Otolaryngologists will face ever more difficult decisions when working with professional voice patients. As this happens, a means of effectively evaluating vocal fatigue in individual patients will play a crucial role in the treatment and prevention of laryngeal disorders by speech therapists and otolaryngologists.
While perceptual data on vocal fatigue has been collected on actors and singers, better objective measurements have been needed to corroborate these findings.8 Previously recorded objective measures of the effects of vocal loading have included pre/post loading changes in frequency (F0) range, voice range profile, jitter, and changes in sound pressure level (SPL); vocal loading behaviors or factors previously measured include long-term average F0, average SPL, background noise levels, RASTI (rapid speech transmission index) values, signal to noise ratio and total voicing time.3–6, 9 Computer-based recording devices worn by subjects called “voice accumulators”9, 10–11, 14 as well as portable audio recorders with one or more microphones3, 5 have been used to obtain data. Drawbacks of these devices have included a lack of ease of use for the subject, difficulty in eliminating background noise, insufficient memory for data storage, short battery life of the unit, high cost and low availability of the unit, and variable microphone stability. Recently, the NCVS Dosimeter™ (National Center for Voice and Speech, Denver, CO) (Dosimeter) was introduced as an improved device to measure total vocal “dose.” Vocal dose is similar to the vocal load but is measured objectively as three individual values: time, distance, and cycle.12–13, 19 The Dosimeter incorporates a commercially available Pocket PC that has been successfully adapted for voice data collection and real-time processing.
To our knowledge, the current project is the first study to record multi-day vocal dose data on professional and semi-professional singers prior to a performance. We intended our pilot study data to serve as a launching point for future, larger population research. Our objectives were first, to confirm that the Dosimeter is easy to apply by the subject, inconspicuous, easy to wear, eliminates background noise and records the necessary data to calculate vocal doses. Second, we wanted to use this device to examine vocal fatigue by determining if a relationship exists between reported subjective ratings and the objective dose measurements in order to evaluate the performers' perception of their vocal status. We hypothesized that subjective findings would correspond with the dose data – i.e., a higher vocal dose would be reflected subjectively through worsening self-ratings.
Materials and Methods
The Dosimeter
The Dosimeter is a commercially available Compaq iPAQ 3765 Pocket PC (Hewlett-Packard corporation, Palo Alto, CA) that has been modified to measure the frequency (F0), intensity (SPL) and duration (total voicing time or VT) of a subject's vocal activity. It is shown in figure 1. The attached accelerometer, a vibration sensor rather than a microphone, has previously been described in the literature and was chosen for its ability to eliminate background noise in the recordings.14, 18 The integrity of the accelerometer-to-skin connection is crucial to the quality of data collected. The accelerometer attaches to the skin of the sternal notch with Mastisol™ (Ferndale Laboratories, Inc, Ferndale, MI) and a Steri-Strip™ (3M, St. Paul, MN) (figure 2). This is removed at the end of the day with Detachol™ (Ferndale Laboratories, Inc, Ferndale, MI) adhesive remover. This method has been found to be strong enough to withstand an entire day of activity. The Dosimeter is individually calibrated to each subject's F0 and SPL range19 and can record up to 17 hours per charge, allowing data to be collected over an entire day18. The files stored by the Dosimeter on a daily basis (both objective data and self-perceptual tasks) totals approximately 5 MB of memory for 14 hours of use. The Pocket PC is equipped with 32 MB of RAM, and can thus safely store 5 days of data.
FIGURE 1.
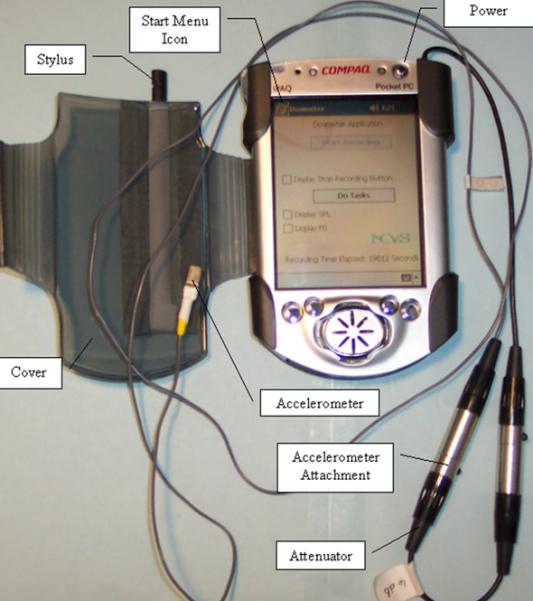
NCVS DOSIMETER
The NCVS Voice Dosimeter consists of a modified Compaq iPAQ PocketPC with an accelerometer and custom software.
FIGURE 2.
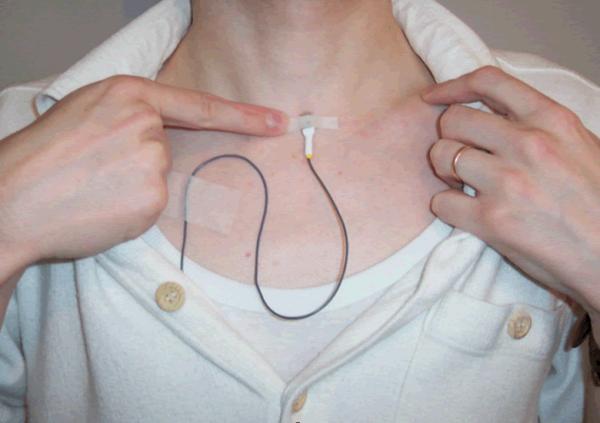
NCVS DOSIMETER
The accelerometer is attached using hypoallergenic medical adhesive and medical tape to the sternal notch. The cabling runs underneath the clothing and the dosimeter is worn in a fanny pack.
Self-perceptual Data
Every two hours, the Dosimeter prompted the wearer to perform five standardized phonation exercises (SPE) and to enter four self-ratings (a.k.a. the “self-perceptual data”). The brief SPE sessions were lead by visual prompts on the Dosimeter screen and included an initial 3-second period of silence during which the Dosimeter recorded a baseline noise floor level. The subject then performed four vocal exercises while the Dosimeter recorded the results. Subjects performed in succession (1) a very low intensity, moderately high-pitched /i/ vowel, (2) a pitch glide from low to high pitch at a low intensity level on /i/, (3) five short /i/ /i/ /i/ /i/ /i/ at a low intensity and moderately high pitch, and (4) the first few phrases of “Happy Birthday” sung at low intensity and high pitch. Subjects were then prompted to rate on a scale of 1(best) to 10 (worst) their inability to produce a soft voice (IPSV). Difficulty producing soft voice would result in a higher rating. Following this, subjects performed the fifth task (5), counting to 3 in a loud voice. Subjects were asked to rate on a scale of 1(best) to 10 (worst) the effort needed to produce this loud voice, and their level of laryngeal discomfort. Finally, the Dosimeter prompted them to record where they physically perceived their laryngeal discomfort: inside the larynx (i.e. intrinsic musculature/mucosal), outside the larynx (i.e. extrinsic/strap musculature), both or neither.
Dose Data
The data points recorded by the Dosimeter used to calculate the vocal dose include the voicing time (VT), F0, and root mean squared (RMS) skin acceleration level (SAL), from which SPL is calculated.15, 19 Once SPL, F0 and VT were known (figure 3), individual vocal doses were determined. Five doses have previously been discussed in the literature: time dose (Dt), cycle dose (Dc), radiated energy dose (Dr), energy dissipation dose (De), and the distance dose (Dd). The three potentially most useful doses in the calculation of total vocal dose are Dt, Dd, and Dc.12–13
FIGURE 3.

NCVS DOSIMETER
What the NCVS Voice Dosimeter records. Top: skin acceleration level in dB which has been correlated to dB SPL (each subject has their own correlation curve); Middle: fundamental frequency contour; Bottom: duty ratio of voicing/non-voicing (1 for voice, 0 for no voice).
The doses are calculated from F0 and empirical data on vocal fold tissue as described previously.12–13 Dt, measured in seconds, is the voicing time, and quantifies the time the vocal folds spend vibrating by summing voicing instances. The concept of Dc was originally introduced under the name vocal loading index (VLI).12 Dc, measured in cycles, quantifies the total number of oscillatory periods completed by the vocal folds over time. Dc is obtained by a calculation using a subject's measured F0 and the duration of a voicing segment. Finally, Dd totals the approximate vibrational distance the vocal folds move as a cumulative “distance traveled.” This dose is measured in meters. This is calculated from a formula using an approximated measurement of amplitude (from normative data on F0 and SPL) as well as the subject's individual F0 over voiced instances, e.g. one vibration cycle would result in a distance of four times the approximate vibrational amplitude.12–13
It may be instructive to briefly discuss what each of the doses means in practical terms. On a day where a subject speaks extensively, but does not sing a great deal, nor sing high, nor talk loudly for extended periods, phonation time (Dt) would be high, and the number of cycles fairly high (Dc), but the amplitude of vibration and thus the distance the vocal folds would travel back and forth (Dd) would not be as high relative to the other doses. An example of this can be found on Figure 6, day 8.
FIGURE 6.

Subject 5. Normalized dose values. Dt (time dose). Dc (cycle dose). Dd (distance dose)
Data Collection
Institutional IRB approval was obtained. Eight subjects were recruited in Denver, Colorado for the study. Seven subjects completed the study (5 males and 2 females). Information on the subjects is included in Table I. All participants wore the dosimeter during the two weeks preceding (and in some cases including) a major performance.
Table I.
Study period information by subject.
| Second letter denotes gender; O denotes operatic; C denotes choral | |||||||
|---|---|---|---|---|---|---|---|
| SUBJECT NUMBER | S1M1O1 | S2M2O2 | S3M3O3 | S5F2O5 | S6F3C1 | S7M4C2 | S8M5C3 |
| Voice type | Bass | Tenor | Baritone | Soprano | Mezzo-soprano | Baritone | Baritone |
| Age | 36 | 32 | 32 | 41 | 46 | 43 | 52 |
| Years of training | 15 | 14 | 15 | 22 yrs | 15 | 15 | 5 |
| Singing commitments during study period | Singing Baron Douphol in La Traviata with regional opera company | Singing Gastone in La Traviata with regional opera company | Singing Fiorello in Barber of Seville with regional opera company | Outreach performances with regional opera company plus Beethoven 9 Symphony | Church choir | Church choir; barbershop quartet; symphony chorus | Church choir; rehearsals for Little Shop of Horrors musical |
Before participating in dosimetry, each participant underwent a complete laryngeal examination (including videostroboscopy with the senior author MA), the administration of a self-perceptual vocal health questionnaire, adapted with permission20, and an individual accelerometer calibration session.19 Subjects were asked to wear the Dosimeter from waking until bed each day during the two-week study period. They were instructed to attach the accelerometer, start the recording and perform their normal daily activities. A member of the research team met subjects every 24–48 hours for a 10 to 15 minute session to gather the data. They were instructed to maintain a paper diary (provided) of all daily activities including unusual events. One author (JN) was responsible for all interactions with the subjects throughout the study period.
Once the data was downloaded, MATLAB® algorithms created by the authors were used to calculate doses and present the dose and rating information in table format. These tables were saved as Microsoft Excel® files. Converting the numerical values for each dose to a percentage value of the highest result in each category over the 2-week period “normalized” the daily totals for Dt, Dd, and Dc. This was done in order to compare the dose values, which have different units, to each other on one graph (figure 4). Discomfort, effort and IPSV, initially recorded at approximately two-hour intervals during each day, were averaged separately for each day during the study period. These average values were also normalized against the highest value for the study period and then plotted as a percentage for ease of graphical data evaluation (figure 7). The final result was normalized self-perceptual rating and dose data. These plots, along with the subjects' paper diaries, allowed us to examine the data for any trends.
FIGURE 4.

Subject 6. Normalized dose values. Dt (time dose). Dc (cycle dose). Dd (distance dose)
FIGURE 7.

Subject 5. Normalized subjective values. IPSV (inability to produce soft voice rating). Discomfort (discomfort rating). Effort (effort rating).
Results
Five trends were observed between normalized doses and self-perceptual ratings (figures 4, 5, 6 and 7). First, subjects' IPSV and vocal effort often increased the same day as a large vocal dose. Second, there was a trend for all subjects to have a 24-72 hour time lag between most large vocal doses and a further worsening of subjective ratings. Often, before the ratings deteriorated to reflect the preceding vocal load, there was a period when both the doses and effort decreased and the soft voice quality improved. When a deterioration in soft voice quality occurred and an increase in effort was observed 24-72 hours after exposure to a high vocal dose, but the vocal dose had remained low throughout this “lag” period, this change was believed to not be a reflection of re-injury. Third, there was often less deterioration in the subjective ratings following a large vocal dose when the dose was preceded by at least a 48-hour period of vocal rest. Fourth, after a day with a high vocal dose in four of our five low-voice subjects (i.e. mezzo, baritone and bass), we observed that their ratings of vocal effort had a tendency to increase one day ahead of any subjective deterioration in soft voice quality. Finally, when singers experienced 2 or more days of high doses separated by only 24 hours of a lower dose, there appeared to be a cumulative effect on subjective ratings. This occurred in two of our seven subjects who had more demanding two-week study periods. The IPSV and the effort remained fairly constant at an elevated level, rather than recovering to lower ratings. We refer to this as the “multi-hit phenomenon” (figures 6 and 7).
FIGURE 5.

Subject 6. Normalized subjective values. IPSV (inability to produce soft voice rating). Discomfort (discomfort rating). Effort (effort rating).
Discussion
Vocal folds experience significant daily vibration-related stresses. Titze16 has estimated the mechanical stresses in vocal fold tissues and concluded that while tensile stress in the anterior-posterior direction placed on the vocal ligament by the cricothyroid muscle is the greatest, the stresses that cause the most damage are the collision and acceleration forces associated with vibration that are directed perpendicular to the vocal ligament. His hypothesis is that the vocal ligament serves to protect the other tissues in the vocal fold from rupture. Studies estimate a safety threshold would be met after approximately 17 minutes of continuous phonation12; however, phonation is never continuous for more than a few seconds. Pauses between phonation episodes (breathing, swallowing, etc.) may allow for some immediate muscular and LP recovery, but quantifying these short-term recovery effects continues to be an ongoing research challenge. Also, as a general rule, it should be noted that females experience a higher raw cycle dose due to their higher natural F0.1, 4–5 It is possible that female vocal fold tissue structure is somewhat adapted for these higher vibration doses.2
Anecdotally, some singers report returning to their subjective baseline quickly from episodes of vocal fatigue while others do not. This phenomenon is not completely understood. Technique and training, reflected in how aware singers are of subtle changes in the way their laryngeal tissues feel, likely plays a large role in the ability to compensate for mild dysfunction. This may allow them to recover rapidly and avoid further injury.7 Respiration, which is but one aspect of vocal production and singing training, is frequently observed as being different between singers of different musical genres and between genders of singers. Classical singers may use most of their vital capacity while singing a long phrase, simultaneously employing a lower laryngeal position and a more efficient glottal closure than non-classically trained individuals.17 Genetics, environment, and hormonal changes are also factors that contribute to why some singers can recover more easily from a given vocal load; in the final analysis, though, even the best trained singers do experience fatigue and injury from time to time.1
This research, from its inception, was intended to be a pilot study to aid in the future direction of larger population studies with statistical evaluation. Due to our small sample size, we present our findings as trends rather than statistical data. These findings lead us to consider what may actually be occurring within the fatiguing laryngeal tissues. We speculate that LP fatigue and muscular fatigue are represented in different ways by the subjective ratings. Muscular fatigue seems to occur on the same day that doses are high. This is comparable to the discomfort an athlete feels while actively exercising and muscle chemistry is being broken down. The delayed IPSV seen 24-72 hours after a large dose may represent LP injury and healing. When the subject's IPSV rating is high, edema may be present in the LP, preventing a normal mucosal wave. Changes in effort are presumed to represent both muscular and LP injury. As stated above, in 4 out of 5 of our low voice subjects, effort actually increased a day before the increase in IPSV. This might reflect muscle tissue inflammation and rebuilding as well as LP edema that may not have peaked. The IPSV and effort plateau seen with the “multi-hit” phenomenon may represent a period of time where the laryngeal musculature is continuously being warmed and exercised. It is not until a period of true rest has occurred that the LP becomes fully affected (i.e. edematous) by the previous dose and the musculature can begin to repair.
The questions of immediate interest raised by this study are: How do these findings compare between different subpopulations that have different genetic make-ups, different training/experiences and different hormonal changes? Specifically, future studies could compare male and female voices, search for variations or similarities between operatic, choral and musical theatre singers, as well as compare those with formal training versus those who are self-taught. Can vocal recovery be quantified in classical singers, and is this recovery the same as is found in other populations of less-formally trained heavy voice users, such as teachers? How do illnesses, menstruation and sleep affect vocal fatigue and recovery? Most of these questions can only be addressed with larger study populations and more frequent videostroboscopic examinations. More frequent exams might enable our team to link changes in IPSV ratings with visible changes in the short-term condition of the lamina propria and enable us to discern the difference between what is lamina propria fatigue (as revealed by changes in the appearance of the folds themselves) and what is intrinsic muscle fatigue (as shown by changes in vocal fold posturing). Finally, one means to improve our data set and deepen our overall understanding of how sleep plays a role in vocal recovery might be to have the singers wear the Dosimeter at all times within reason.
Conclusion
The NCVS Voice Dosimeter is an effective tool for the collection of prolonged voice use data. It is relatively easy to use and avoids many of the pitfalls seen with previous vocal accumulators. While not all of the shortcomings are worked out with the device, this preliminary research will guide the design of future projects. We observed several trends in the way objective vocal dose data was reflected in subjective vocal rating changes. We plan to design larger studies to evaluate vocal recovery time based on collected dose data. The application of the Dosimeter in the clinical setting is still several years in the future. Eventually, we envision a unit that will be available to otolaryngologists, speech therapists or voice teachers as a tool to objectively evaluate the vocal load placed on a patient's or student's larynx and to act as an adjunct in guiding medication, therapy and artistic training.
Acknowledgement
This research was funded by a grant from The Recording Academy. The research protocol employed equipment and software developed as a part of grant R01 DC04224 from the National Institute on Deafness and other Communication Disorders.
Footnotes
Presentation: This paper's content was presented at the 2005 AAOHNS meeting in Los Angeles, California and was presented as a poster at the 2005 ICVT meeting in Vancouver, BC Canada.
References
- 1.Vilkman E. Occupational safety and health aspects of voice and speech professions. Folia Phoniatr Logop. 2004;56:220–53. doi: 10.1159/000078344. [DOI] [PubMed] [Google Scholar]
- 2.Titze IR, McCabe DJ. Chant therapy for treating vocal fatigue among public school teachers: a preliminary study. Am J Speech Lang Pathol. 2002;11:356–369. [Google Scholar]
- 3.Sala E, Airo E, Olkinuora P, et al. Vocal loading among day care center teachers. Logoped Phoniatr Vocol. 2002;27:21–8. doi: 10.1080/140154302760146943. [DOI] [PubMed] [Google Scholar]
- 4.Jonsdottir V, Laukkanen A, Vilkman E. Changes in teachers' speech during a working day with and without electric sound amplification. Folia Phoniatr Logop. 2002;54:282–7. doi: 10.1159/000066149. [DOI] [PubMed] [Google Scholar]
- 5.Sodersten M, Granqvist S, Hammarberg B, et al. Vocal behavior and vocal loading factors for preschool teachers at work studied with binaural DAT recordings. J Voice. 2002;16(3):356–371. doi: 10.1016/s0892-1997(02)00107-8. [DOI] [PubMed] [Google Scholar]
- 6.Stemple JC, Stanley J, Lee L. Objective measures of voice production in normal subjects following prolonged voice use. J Voice. 1995;9(2):127–33. doi: 10.1016/s0892-1997(05)80245-0. [DOI] [PubMed] [Google Scholar]
- 7.Gelfer MP, Andrews ML, Schmidt CP. Effects of loud reading on selected Measures of vocal function in trained and untrained singers. J Voice. 1991;5(2):158–67. [Google Scholar]
- 8.Kitch JA, Oates J. The perceptual features of vocal fatigue as self-reported by a group of actors and singers. J Voice. 1994;8(3):207–14. doi: 10.1016/s0892-1997(05)80291-7. [DOI] [PubMed] [Google Scholar]
- 9.Szabo A, Hammarberg B, Hakansson A, et al. A voice accumulator device: Evaluation based on studio and field recordings. Logoped Phoniatr Vocol. 2001;26:102–17. doi: 10.1080/14015430152728016. [DOI] [PubMed] [Google Scholar]
- 10.Ohlsen A, Brink O, Lofqvist A. A voice accumulator - validation and application. J Speech Hear Res. 1989;32:451–7. doi: 10.1044/jshr.3202.451. [DOI] [PubMed] [Google Scholar]
- 11.Buekers R, Bierens E, Kingma H, et al. Vocal load as measured by the voice accumulator. Folia Phoniatr Logop. 1995;47:252–61. doi: 10.1159/000266359. [DOI] [PubMed] [Google Scholar]
- 12.Titze IR, Svec JG, Popolo PS. Vocal dose measures: Quantifying accumulated vibration exposure in vocal fold tissues. J Speech Lang Hear Res. 2003;46:922–35. doi: 10.1044/1092-4388(2003/072). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Svec JG, Popolo PS, Titze IR. Measurement of vocal doses in speech: experimental procedure and signal processing. Logoped Phoniatr Vocol. 2003;28:181–92. doi: 10.1080/14015430310018892. [DOI] [PubMed] [Google Scholar]
- 14.Cheyne HA, Hanson HM, Genereux RP, et al. Development and testing of a portable vocal accumulator. J Speech Lang Hear Res. 2003;46:1457–67. doi: 10.1044/1092-4388(2003/113). [DOI] [PubMed] [Google Scholar]
- 15.Titze IR. Principles of Voice Production. Prentice-Hall; Englewood Cliffs, NJ: 1994. p. 120.p. 233. [Google Scholar]
- 16.Titze IR. Mechanical stressing phonation. J Voice. 1994;8(2):99–105. doi: 10.1016/s0892-1997(05)80302-9. [DOI] [PubMed] [Google Scholar]
- 17.Cleveland TF. An Overview of Laryngeal Function in Different Singing Styles. Journal of Singing. 1994 Nov-Dec;51:37–38. [Google Scholar]
- 18.Popolo PS, Rogge-Miller K, Svec JG, et al. NCVS Online Technical Memo 2002. Denver, Co: 2004. NCVS Memo No05. Technical Considerations in the Design of a Wearable Voice Dosimeter. www.ncvs.org/ncvs/library/tech. [Google Scholar]
- 19.Svec JG, Hunter EJ, Popolo PS, et al. NCVS Online Technical Memo April 2004. Denver, Co: 2004. NCVS Memo No 02. The Calibration and Setup of the NCVS Dosimeter. www.ncvs.org/ncvs/library/tech. [Google Scholar]
- 20.Sapir S, Mathers-Schmidt B, Larson GW. Singers' and non-singers vocal health, vocal behaviors, and attitudes toward voice and singing: indirect findings from a questionnaire. Eur J Disord Commun. 1996;31(2):193–209. doi: 10.3109/13682829609042221. [DOI] [PubMed] [Google Scholar]