

Abstract
Endometriosis is a complex disease that affects a large number of women worldwide and may cause pain and infertility.
To systematically review published studies evaluating the relationship between menstrual cycle length and risk of endometriosis.
We searched the Cochrane Library, PubMed, Web of Science, and EMBASE in databases in July 2014 using the keywords “case–control studies,” “epidemiologic determinants,” “risk factors,” “menstrual cycle,” “menstrual length,” “menstrual character,” and “endometriosis.”
We included case–control studies published in English that investigated cases of surgically confirmed endometriosis and examined the relationship between endometriosis risk and menstrual cycle.
Eleven articles that met the inclusion criteria included data of 3392 women with endometriosis and 5006 controls. Fixed-effects and random-effects models were used for the evaluation.
For the association of risk of endometriosis and menstrual cycle length shorter than or equal to 27 days (SEQ27) or length longer than or equal to 29 days (LEQ29), the odds ratio was 1.22 (95% confidence interval [CI]: 1.05–1.43) and 0.68 (95% CI: 0.48–0.96), respectively.
In conclusion, this meta-analysis suggests that menstrual cycle length SEQ27 increase the risk of endometriosis and cycle length LEQ29 decrease the risk.
INTRODUCTION
Endometriosis is a complex gynecologic disorder characterized by benign proliferation of ectopic endometrial glands and stroma in the peritoneal cavity, with dysmenorrhea, pelvic pain, and infertility being typical symptoms.1,2 It affects approximately 10% to 15% of women of reproductive age and as many as 50% of women with infertility.3
Genetic predisposition and environmental factors are considered to be closely associated with the development of endometriosis.4–7 However, the pathogenesis of this disease is currently not very clear. Three main theories used to explain the manifestations and invasion are the retrograde menstruation theory, Müllerian metaplasia theory, and lymphatic spread theory.8
Many studies have surveyed the risk factors associated with the disease. It has been shown that age, race, body mass index, alcohol usage, cigarette smoking, and menstrual characters (such as the length and regularity of menstrual cycles, intensity of menstrual flow, and dysmenorrhea) are associated with the incidence of endometriosis.9–12
Menstrual cycle characteristics affecting the frequency of exposure to menstruation may be related to the incidence of endometriosis.13 Thus, several observational studies and a meta-analysis have provided some evidence that early age at menarche increases the risk of endometriosis.14,15 The length of the menstrual cycle varies greatly among women (ranging from 21 to 35 days), with 28 days designated as the average length.16 Accordingly, 28 days was used as the cut-off value for group assignment in a number of studies relevant to endometriosis.17–22 We placed demarcation points at 27 and 29 days and defined menstrual cycle length shorter than or equal to 27 days as SEQ27 and longer than or equal to 29 days as LEQ29. The majority of observational studies have examined the relationship between menstrual cycle length, 1 of the menstrual characteristics, and endometriosis, and some have found an association between a shorter menstrual cycle and the incidence of this disease.20–23 On the contrary, Sangi-Haghpeykar's study24 showed that women with long cycle lengths were 1.8 times more likely to develop endometriosis than those with short cycle lengths. Dramatically, some studies11,23,25 did not find any significant correlation between short menstrual cycle length and endometriosis at all. Therefore, the association between menstrual cycle length and endometriosis needs further confirmed. The aim of the present study is to perform a meta-analysis to examine the association between menstrual cycle length and endometriosis.
METHODS
Search Strategy
A systematic search was performed in the Cochrane Library, PubMed, MEDLINE, and EMBASE databases for all case–control studies published between January 1993 and July 2014 using the following keywords: “Case–control studies,” “epidemiologic determinants,” “risk factors,” “menstrual cycle,” “menstrual length,” “menstrual character,” and “endometriosis.” Reference lists of selected publications were then searched manually by 1 of the authors to identify additional relevant studies. Two authors reviewed the papers and independently selected eligible articles for the systematic review.
Study Selection
Studies were included if they investigated cases of surgically confirmed endometriosis; examined the relationship between endometriosis risk and menstrual cycle; were case–control studies; and were full-length articles published in English. Only original publications were included; conference abstracts and dissertations were excluded.
Data Extraction and Quality Assessment
Data were extracted independently by 2 investigators, and discrepancies were resolved by discussion. The following details were collected: first author's last name, year of publication, country of origin, study design, number of subjects, age, length of menstrual cycle in days, and odds ratios (ORs) of endometriosis and corresponding confidence intervals (CIs). The quality of primary studies was evaluated using the Newcastle–Ottawa Scale (NOS) according to 3 criteria: participant selection, comparability of study groups, and assessment of exposure.26
Statistic Analysis
ORs and 95% CIs for menstrual cycle length and endometriosis were calculated in a random-effects model and a fixed-effects model when appropriate. Both the Cochran Q statistic to test for heterogeneity and the I2 statistic to quantify the proportion of the total variation due to heterogeneity were calculated. A P value of more than the nominal level of 0.10 for the Q statistic indicated a lack of heterogeneity across studies, allowing for the use of a fixed-effects model; otherwise, the random-effects model was used. To explore sources of heterogeneity across studies, subgroup analysis was performed. Sensitivity analysis was performed to assess the stability of results. All statistical analyses were performed with the RevMan 5.3 software.
RESULTS
Results of the Literature Search
Of the 631 reports initially identified from the database search, 603 articles were excluded after carefully reviewing the titles and abstracts because of low relevance to the present study (Figure 1). Among the 28 remaining articles, 17 more were excluded after an in-depth examination for the following reasons: 7 were not case–control studies, 7 did not mention menstrual cycle, 2 only presented mean values and not numbers of subjects, and 1 had similarities with 1 of the selected reports. Thus, only 11 studies fulfilled the predefined entry criteria and were ultimately selected for meta-analysis.
FIGURE 1.
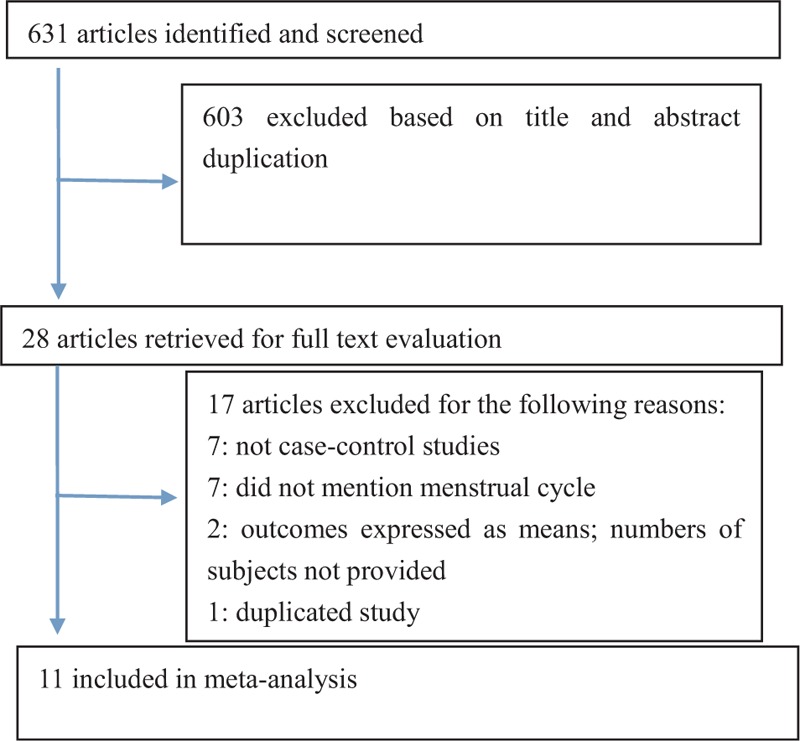
Flow diagram illustrating the study selection process.
Study Characteristics
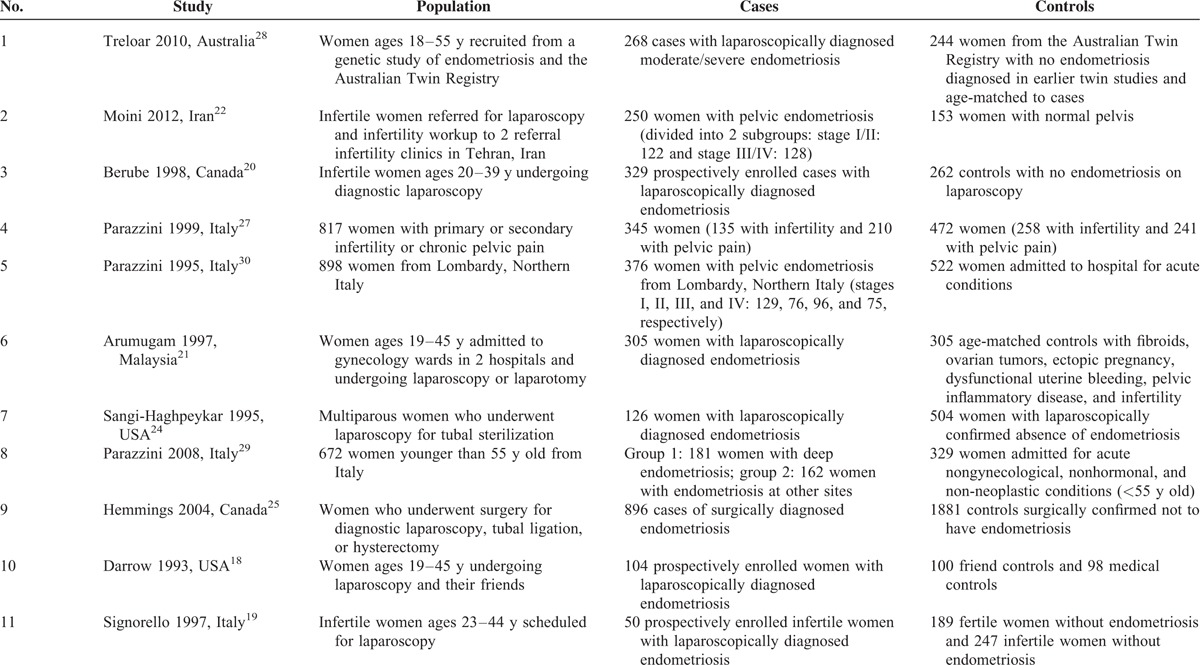
Table 1 summarizes the 11 case–control studies selected for meta-analysis. Numbers of subjects in the studies published between 1993 and 2014 ranged from 186 to 2777, and there were 3392 cases of surgically diagnosed endometriosis and 5006 controls (Table 1).18–22,24,25,27–30 Fortunately, we received the original data from one author of study22 and used them in data analysis. The studies were conducted in Italy (n = 4), the United States (n = 2), Canada (n = 2), Australia (n = 1), Malaysia (n = 1), and Iran (n = 1). Subjects were generally younger than 55 years,18–21,28,29 although women up to 64 years old were included in 1 study.24 Four studies22,25,27,30 did not provide the subjects’ age explicitly but used age ranges. Reports differed with respect to the description of menstrual cycle. Five studies described menstrual cycle as “regular” or “irregular,”19,22,27,29,30 and 2 of them did not mention the duration.29,30 Nine studies18–22,24,25,27,28 used clearly defined intervals for the menstrual cycle length but the intervals in different studies were not the same. Five studies18–20,22,25 provided the numbers of women in case and control with the length SEQ27 and 5 studies19,20,22,24,28 provided the cases numbers with the length LEQ29. Three studies used age-matched controls.21,28,30 In particular, 1 study28 utilized age-matched twins as case and control subjects, whereas another18 employed 2 control groups: 100 controls who were friends of the patients with endometriosis and 98 medical controls (patients from the same medical practice with conditions other than endometriosis).
TABLE 1.
Characteristics of the 11 Case–Control Studies Included in the Analysis
Data Quality
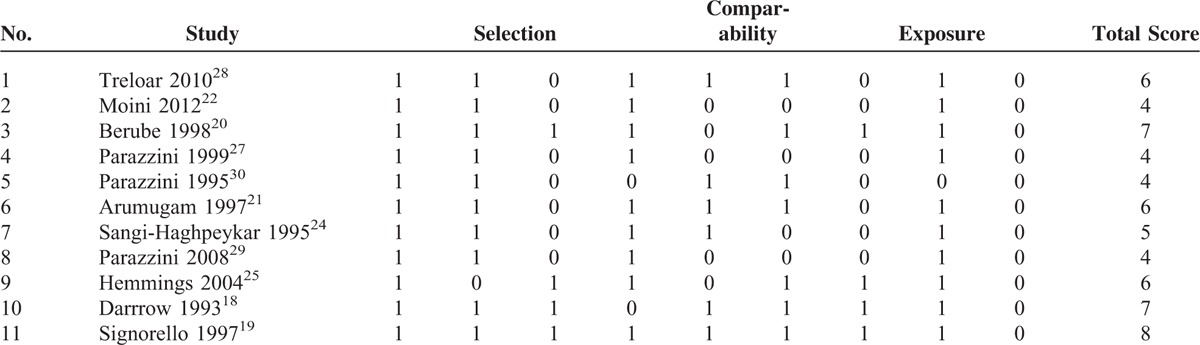
The quality of the studies was assessed by 2 investigators using the NOS, a validated tool for evaluating observational and nonrandomized studies, and the results were scored from 4 to 8. In particular, 1 study19 received a score of 8, 218,20 a score of 7, 321,25,28 a score of 6, 124 a score of 5, and the remaining 422,27,29,30 a score of 4 (Table 2).
TABLE 2.
Quality of the Included Studies Assessed Using the Newcastle–Ottawa Scale
Menstrual Cycle and Risk of Endometriosis
Women with menstrual cycle lengths SEQ27 were at an increased risk of developing endometriosis (OR: 1.22, 95% CI: 1.05–1.43; Figure 2) and those with menstrual cycle lengths LEQ29 were at an approximately 32% lower risk of endometriosis (OR: 0.68, 95% CI: 0.48–0.96; Figure 3).
FIGURE 2.
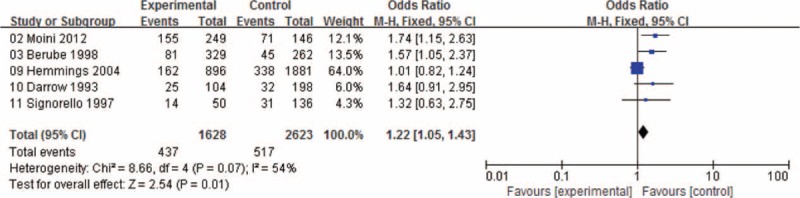
Forest plot of ORs with 95% CIs for menstrual cycle length SEQ27 and risk for endometriosis. CI = confidence interval, OR = odds ratio.
FIGURE 3.
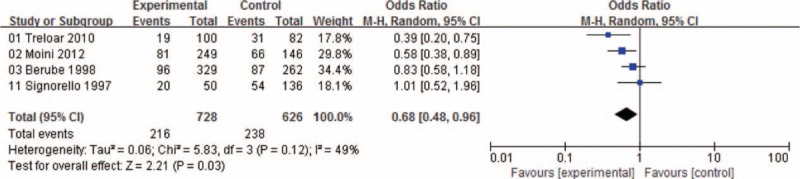
Forest plot of ORs with 95% CIs for menstrual cycle length LEQ29 and risk for endometriosis. CI = confidence interval, OR = odds ratio.
Heterogeneity Analysis and Sensitivity Analysis
There was heterogeneity among studies in overall comparisons. We assessed all of the comparison models by country, and study sample size (≤300 subjects or >300 subjects) to explore sources of heterogeneity across studies. However, none of these variables could explain the heterogeneity. In the sensitivity analysis, we repeat the meta-analysis by omitting each study 1 by 1 to exam the influence of each study on the pooled OR. The result proved that our results were reliable. In addition, when excluding 1 study24 simultaneously, the I2 significantly decreased from 79% to 49% which was not so high as before. Therefore, the study24 was considered as the source of heterogeneity and finally excluded when analyzed.
Publication Bias
Funnel plots for the association between menstrual cycle length SEQ27 or menstrual cycle length LEQ29 and risk for endometriosis were shown in the Figures 4 and 5. Visual inspection of funnel plot asymmetry was conducted to assess the potential publication bias. Obviously, no indication of asymmetry was observed in the funnel plots.
FIGURE 4.
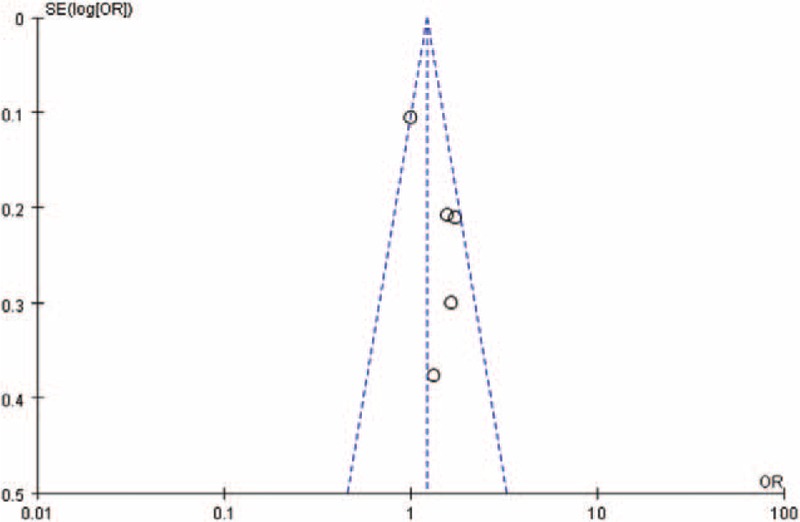
Funnel plot for the association between menstrual cycle length SEQ27 and risk for endometriosis.
FIGURE 5.
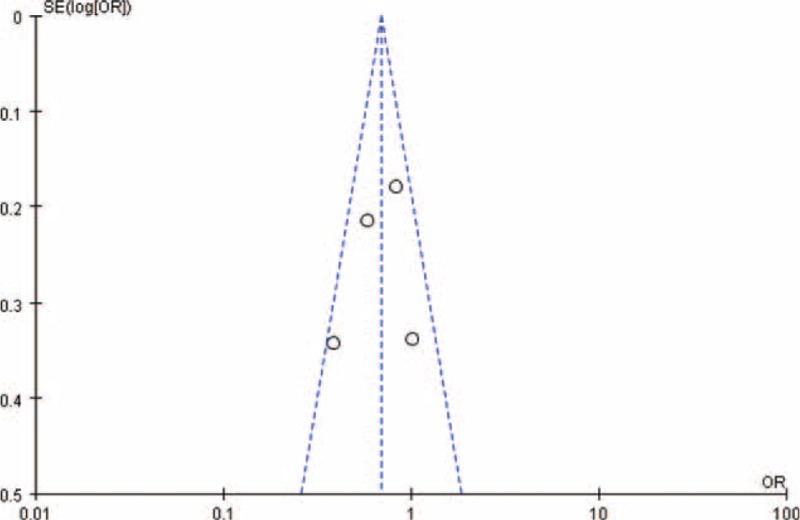
Funnel plot for the association between menstrual cycle length LEQ29 and risk for endometriosis.
DISCUSSION
The consistency of the results of this meta-analysis indicates that menstrual cycle length SEQ27 is inversely associated with the risk of endometriosis and menstrual cycle length LEQ29 decreases the risk.
The retrograde bleeding hypothesis can be 1 explanation for these findings. Sampson's theory of retrograde menstruation,31 which is supported by the anatomical distribution of endometriotic implants32 and higher prevalence of the disease in women with obstructive Müllerian anomalies, is currently considered to describe the main causal mechanism of endometriosis.15,33 A short menstrual cycle usually means an increased menstrual frequency and higher risk of exposure to menstruation. Menstrual cycle length SEQ27, which is shorter than average cycle length, could potentially increase the frequency and the risk of retrograde bleeding and finally increase the incidence of endometriosis. However, the cycle length LEQ29 influences the endometriosis in a contrary way.
The other potential explanation for our study results may be the fact that endometrial-like tissues of short-cycle-length (SEQ27) women are at a relatively higher frequency of exposure to higher levels of estrogen than that of long-cycle-length women. Several studies have already found that the ectopic growth of endometrial-like tissue was depended upon sex steroid hormones34 and local growth factors35 such as insulin-like growth factor 1 (IGF-1)36 or vascular endothelial growth factor (VEGF).37 Commonly, short cycle length comes along with punctually ovulation and the estrogen level sharply increasing in a short period of time before ovulation. Estrogen has synergistic effects with IGF-1/VEGF and sometimes enhance the effects of IGF-1/VEGF on ectopic endometrial cells proliferation and mitosis,38 which possibly ended with endometriosis.
Consistent with our conclusion, some studies20–23 concluded that short menstrual cycle length increases the risk of endometriosis. Oppositely, Sangi-Haghpeykar's study24 draw a conclusion that long cycle length is a risk factor. The opposite conclusion may result from the differences in the subjects’ source population, race, geographical region, and age. In summary, findings of our study can be used to guide the diagnostic and therapeutic strategies of endometriosis in clinical practices. For instance, the artificial menstrual cycle can be tried to manage the development of endometriosis in terms of delaying the menstruation or ovulatory phase. There are some limitations in our studies: only studies published in English between 1993 and 2014 were included; and the number of included studies and the total sample size were relatively small. More well-designed studies should be conducted.
CONCLUSIONS
In conclusion, this meta-analysis suggests that menstrual cycle length SEQ27 increase the risk of endometriosis and length LEQ29 decrease the risk.
Acknowledgments
Here we thank professor Chunquan Yu gave us much help on meta-analysis methodology. We also thank Mrs Jia Fu provided valuable revised advices.
Footnotes
Abbreviations: BMI = body mass index, CI = confidence interval, IGF-1 = insulin like growth factor 1, LEQ29 = longer than or equal to 29 days, NOS = Newcastle–Ottawa Scale, OR = odds ratio, SE = standard error, SEQ27 = shorter than or equal to 27 days, VEGF = vascular endothelial growth factor.
MW and YC have contributed equally to this study.
MW and WLZ conceived and designed the experiments, YFC and YZ performed the experiments, WLZ and HEB analyzed the data, YZ Contributed reagents/materials/analysis tools, and MW, YFC and YZ wrote the paper.
The authors have no funding and conflicts of interest to disclose.
REFERENCES
- 1.Donnez J, Van Langendonckt A, Casanas-Roux F, et al. Current thinking on the pathogenesis of endometriosis. Gynecol Obstet Invest 2002; 54 Suppl 1:52–58. [DOI] [PubMed] [Google Scholar]
- 2.Zondervan KT, Cardon LR, Kennedy SH. The genetic basis of endometriosis. Curr Opin Obstet Gynecol 2001; 13:309–314. [DOI] [PubMed] [Google Scholar]
- 3.Fuentes A, Escalona J, Cespedes P, et al. Prevalence of endometriosis in 287 women undergoing surgical sterilization in Santiago Chile. Rev Med Chil 2014; 142:16–19. [DOI] [PubMed] [Google Scholar]
- 4.Shubina AN, Egorova AA, Baranov VS, et al. Recent advances in gene therapy of endometriosis. Recent Pat DNA Gene Seq 2013; 7:169–178. [DOI] [PubMed] [Google Scholar]
- 5.Ma Y, He YL. Study of an antiangiogenesis gene therapy with endostatin on endometriosis in the nude mouse model. Clin Exp Obstet Gynecol 2014; 41:328–334. [PubMed] [Google Scholar]
- 6.Giudice LC, Kao LC. Endometriosis. Lancet 2004; 364:1789–1799. [DOI] [PubMed] [Google Scholar]
- 7.Ballester M, Dehan P, Beliard A, et al. Role of genetic and environmental factors in the development of endometriosis. Rev Med Liege 2012; 67:374–380. [PubMed] [Google Scholar]
- 8.Gazvani R, Templeton A. Peritoneal environment, cytokines and angiogenesis in the pathophysiology of endometriosis. Reproduction 2002; 123:217–226. [DOI] [PubMed] [Google Scholar]
- 9.Guo SW, Wang Y. Sources of heterogeneities in estimating the prevalence of endometriosis in infertile and previously fertile women. Fertil Steril 2006; 86:1584–1595. [DOI] [PubMed] [Google Scholar]
- 10.Missmer SA, Hankinson SE, Spiegelman D, et al. Incidence of laparoscopically confirmed endometriosis by demographic, anthropometric, and lifestyle factors. Am J Epidemiol 2004; 160:784–796. [DOI] [PubMed] [Google Scholar]
- 11.Calhaz-Jorge C, Mol BW, Nunes J, et al. Clinical predictive factors for endometriosis in a Portuguese infertile population. Hum Reprod 2004; 19:2126–2131. [DOI] [PubMed] [Google Scholar]
- 12.Parazzini F, Cipriani S, Bravi F, et al. A meta analysis on alcohol consumption and risk of endometriosis. Am J Obstet Gynecol 2013; 209:106e1–110e1. [DOI] [PubMed] [Google Scholar]
- 13.Matalliotakis IM, Cakmak H, Fragouli YG, et al. Epidemiological characteristics in women with and without endometriosis in the Yale Series. Arch Gynecol Obstet 2008; 277:389–393. [DOI] [PubMed] [Google Scholar]
- 14.Buck LG, Hediger ML, Pena JB. Intrauterine exposures and risk of endometriosis. Hum Reprod 2007; 22:3232–3236. [DOI] [PubMed] [Google Scholar]
- 15.Nnoaham KE, Webster P, Kumbang J, et al. Is early age at menarche a risk factor for endometriosis? A Systematic review and meta-analysis of case–control studies. Fertil Steril 2012; 98:702–712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Widmaier EP, Raff H, Strang KT. Vander's Human Physiology: The Mechanism of Body Function. 12th ed2010; New York: McGraw-Hill, [555-631.]. [Google Scholar]
- 17.Tolossa FW, Bekele ML. Prevalence, impacts and medical managements of premenstrual syndrome among female students: cross-sectional study in College of Health Sciences, Mekelle University, Mekelle, Northern Ethiopia. BMC Womens Health 2014; 14:52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Darrow SL, Vena JE, Batt RE, et al. Menstrual cycle characteristics and the risk of endometriosis. Epidemiology 1993; 4:135–142. [DOI] [PubMed] [Google Scholar]
- 19.Signorello LB, Harlow BL, Cramer DW, et al. Epidemiologic determinants of endometriosis: a hospital-based case–control study. Ann Epidemiol 1997; 7:267–741. [DOI] [PubMed] [Google Scholar]
- 20.Berube S, Marcoux S, Maheux R. Characteristics related to the prevalence of minimal or mild endometriosis in infertile women. Epidemiology 1998; 9:504–510. [DOI] [PubMed] [Google Scholar]
- 21.Arumugam K, Lim JM. Menstrual characteristics associated with endometriosis. Br J Obstet Gynaecol 1997; 104:948–950. [DOI] [PubMed] [Google Scholar]
- 22.Moini A, Malekzadeh F, Amirchaghmaghi E, et al. Risk factors associated with endometriosis among infertile Iranian women. Arch Med Sci 2013; 9:506–514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cramer DW, Wilson E, Stillman RJ, et al. The relation of endometriosis to menstrual characteristics, smoking, and exercise. JAMA 1986; 255:1904–1908. [PubMed] [Google Scholar]
- 24.Sangi-Haghpeykar H, Poindexter AR. Epidemiology of endometriosis among parous women. Obstet Gynecol 1995; 85:983–992. [DOI] [PubMed] [Google Scholar]
- 25.Hemmings R, Rivard M, Olive DL, et al. Evaluation of risk factors associated with endometriosis. Fertil Steril 2004; 81:1513–1521. [DOI] [PubMed] [Google Scholar]
- 26.Ottawa Hospital Research Institute. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp Accessed February 4, 2015. [Google Scholar]
- 27.Parazzini F, Di Cintio E, Chatenoud L, et al. Oral contraceptive use and risk of endometriosis. Br J Obstet Gynaecol 1999; 106:695–699. [PubMed] [Google Scholar]
- 28.Treloar SA, Bell TA, Nagle CM, et al. Early menstrual characteristics associated with subsequent diagnosis of endometriosis. Am J Obstet Gynecol 2010; 202:531–534. [DOI] [PubMed] [Google Scholar]
- 29.Parazzini F, Cipriani S, Bianchi S, et al. Risk factors for deep endometriosis: a comparison with pelvic and ovarian endometriosis. Fertil Steril 2008; 90:174–179. [DOI] [PubMed] [Google Scholar]
- 30.Parazzini F, Ferraroni M, Fedele L, et al. Pelvic endometriosis: reproductive and menstrual risk factors at different stages in Lombardy, Northern Italy. J Epidemiol Community Health 1995; 49:61–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.van der Linden PJ. Theories on the pathogenesis of endometriosis. Hum Reprod 1996; 11 Suppl 3:53–65. [DOI] [PubMed] [Google Scholar]
- 32.Parazzini F, Luchini L, Vezzoli F, et al. Prevalence and anatomical distribution of endometriosis in women with selected gynaecological conditions: Results from a multicentric Italian study. Hum Reprod 1994; 9:1158–1162. [PubMed] [Google Scholar]
- 33.Eskenazi B, Warner ML. Epidemiology of endometriosis. Obstet Gynecol Clin North Am 1997; 24:235–258. [DOI] [PubMed] [Google Scholar]
- 34.Sharpe-Timms KL. Basic research in endometriosis. Obstet Gynecol Clin North Am 1997; 24:269–290. [DOI] [PubMed] [Google Scholar]
- 35.Giudice LC. Growth factors and growth modulations in human uterine endometrium: their potential relevance to reproductive medicine. Fertil Steril 1994; 61:1–17. [DOI] [PubMed] [Google Scholar]
- 36.Kim H, Ku SY, Kim SH, et al. Association between endometriosis and polymorphisms in insulin-like growth factor binding protein genes in Korean women. Eur Obstet Gynecol Reprod Biol 2012; 162:96–101. [DOI] [PubMed] [Google Scholar]
- 37.Rathore N, Kriplani A, Yadav RK, et al. Distinct peritoneal fluid ghrelin and leptin in infertile women with endometriosis and their correlation with interleukin-6 and vascular endothelial growth factor. Gynecol Endocrinol 2014; 30:671–675. [DOI] [PubMed] [Google Scholar]
- 38.Maruo T, Matsuo H, Shimomura Y, et al. Effects of progesterone on growth factor expression in human uterine leiomyoma. Steroids 2003; 68:817–824. [DOI] [PubMed] [Google Scholar]