

Abstract
Presenting the arthroscopic treatment by Tight Rope - Arthrex® system for acute acromioclavicular dislocation and to evaluate results obtained with this procedure. Methods: Between August 2006 and May 2007, 10 shoulders of 10 patients with acute acromioclavicular dislocation were submitted to arthroscopic repair using the Tight Rope - Arthrex® system. Minimum follow-up was 12 months, with a mean of 15 months. Age ranged from 26 to 42, mean 34 years. All patients were male. Radiology evaluation was made by trauma series x-ray. The patients were assisted in the first month weekly and after three months after the procedure. Clinical evaluation was based on the University of California at Los Angeles (UCLA) criteria. Results: All patients were satisfied after the arthroscopic procedure and the mean UCLA score was 32,5. Conclusion: The arthroscopic treatment by Tight Rope – Arthrex® system for acute acromioclavicular dislocation showed to be an efficient technique.
Keywords: Acromioclavicular dislocation/surgery, Arthroscopy/methods
INTRODUCTION
Acromioclavicular dislocation (ACD) is one of the most common shoulder injuries seen in general orthopedic practice. The most common trauma mechanism for this type of injury is a fall with direct force in the lateral region of the shoulder with the upper limb in an adducted position(1).
This injury can be classified into six types according to the magnitude of the trauma(2). Typically, types I and II are treated conservatively, with most patients returning to pre-injury conditions3, 4, 5, 6. Although the treatment of type III injuries is controversial, high-energy injuries (types IV, V, and VI) with more than 100% posterior and/or inferior displacement are treated surgically7, 8, 9, 10.
Several surgical techniques have been developed seeking to treat acromioclavicular dislocation9, 10. The Weaver-Dunn technique of transferring the coracoacromial ligament to the intramedullary canal of the distal clavicle has been one of the more commonly used procedures for acute as well as chronic cases(11).
The purpose of this study is to evaluate the results obtained with the Arthrex® TightRope arthroscopic surgical technique in the treatment of acute acromioclavicular dislocation.
METHODS
From August 2006 to May 2007, 10 shoulders of 10 patients who underwent arthroscopic treatment of acute ACD using the Arthrex® TightRope technique were operated and reevaluated. The surgeries were performed by the Shoulder and Elbow Surgery Group at the Bahia Institute of Orthopedics and Traumatology (INSBOT – Instituto Baiano de Ortopedia e Traumatologia) and the Hospital Português da Bahia, and evaluated after approval by the Ethics Committees of those institutions.
The follow-up period ranged from 12 to 19 months, with an average of 15 months. The average age was 34 years, ranging from 26 to 42 years. All patients were male (Table 1).
Table 1.
Patient data
| Patient Number | Gender | Age | UCLA | Postoperative follow-up (months) |
|---|---|---|---|---|
| 1 | M | 36 years | 35 | 19 |
| 2 | M | 42 years | 29 | 12 |
| 3 | M | 30 years | 29 | 15 |
| 4 | M | 26 years | 34 | 15 |
| 5 | F | 34 years | 35 | 19 |
| 6 | M | 32 years | 35 | 15 |
| 7 | M | 28 years | 30 | 15 |
| 8 | M | 30 years | 34 | 17 |
| 9 | M | 34 years | 29 | 14 |
| 10 | M | 33 years | 35 | 13 |
UCLA = University of California, Los Angeles – method for evaluating postoperative results.
Source: DOT-INSBOT
Pain and deformity were found in all patients in this study (100% of cases) and the “piano key” sign was present in nine patients (types IV and V).
All patients were seen in the acute phase of injury and were evaluated by simple radiology (trauma series). With this test, three patients were observed to have a type V ACD, five patients had a type IV ACD, and two patients had a type III ACD. None of the patients were regularly performing physical activity. The period of immobilization in the postoperative period was two weeks in all cases. Patients were then sent to physiotherapy procedures and released for their daily activities. Patients were allowed to return to sports after three months of surgery. Patients were monitored weekly during the first month, monthly in the first three months, and every three months after the fourth month after the arthroscopic procedure.
The method chosen for the postoperative clinical evaluation of the patients was based on the UCLA (University of California, Los Angeles) criteria(12).
SURGICAL TECHNIQUE
In all cases, surgery was performed with the patient in the beach-chair position. The arthroscope is introduced through the posterior portal to inspect the shoulder joint. A 1.5-cm incision is made above the clavicle to the level of the coracoid process under direct vision (Figure 1). At this point, a stirrup-type guide is placed under the coracoid process (larger arrow) and over the clavicle through the anterior portal and tunnels (smaller arrows) are created into the clavicle at the clavicular incision and into the coracoid process (Figure 2). A flexible guide wire (larger arrow) is then passed through these tunnels from top to bottom, and is captured through the anterior portal by a grasper (smaller arrow) (Figure 3). The Arthrex® TightRope system, consisting of two metal buttons joined by four segments of the same Arthrex® No. 5 Fiberwire (Figure 4), is attached to the upper end of the flexible guide wire, which is pulled through the anterior portal, passing a subcoracoid metal button (arrows), while another button is adjusted under tension on the clavicle (arrows) after reduction of the acromioclavicular joint (Figures 5 and 6).
Figure 1.

Incision over the clavicle
Figure 2.
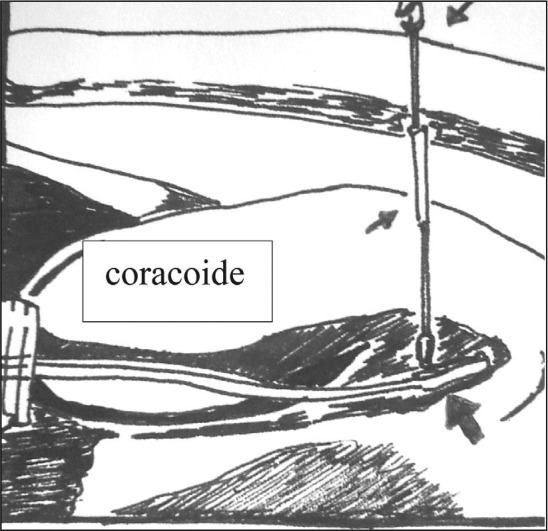
Creating the bone tunnels
Figure 3.

Capturing the flexible guide wire
Figure 4.
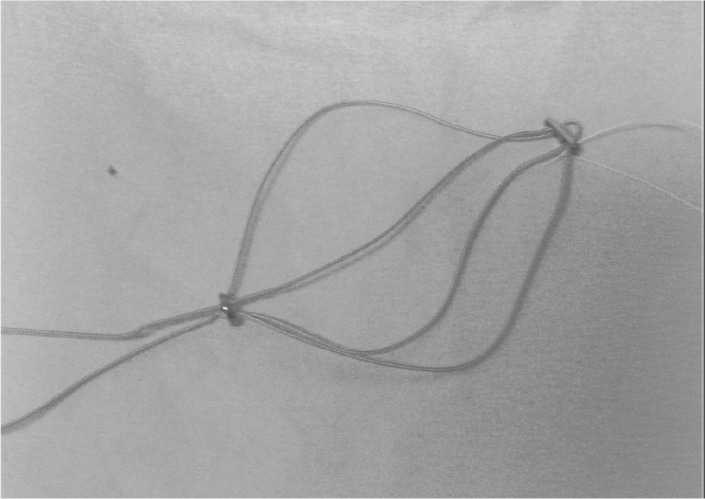
Arthrex® TightRope system
Figures 5 and 6.

Passage of the system and fixation of the it after joint reduction
RESULTS
The mean postoperative follow-up period was 15 months, ranging from 12 to 19 months (Table 1).
Using the UCLA scale(12) as the method for evaluation, we found good and excellent results in all cases with an average of 32.5 points (Table 1).
After one week postoperatively, one of the patients suffered another fall on the operated shoulder, and suffered no damage to the implanted system, with the acromioclavicular joint remaining clinical and radiologically reduced (Figure 7).
Figure 7.

Simple X-ray with TightRope® system implanted and acromioclavicular joint reduced
All acutely operated patients were satisfied with the results of arthroscopic surgery (Figures 8 and 9).
Figures 8 and 9.

Clinical appearance after TightRope® system implantation with reduced acromioclavicular joint
The degree of range of motion of the glenohumeral joint of all patients returned to the pre-injury range of motion – 135° to 140° of flexion and 90° of abduction – according to information gathered from the patients in comparison to the contralateral side. Patients with UCLA scores of 29 and 30 were due to residual pain at the level of the acromioclavicular joint with some limitation in the range of motion due to this residual pain. However, all reported being satisfied with the final postoperative results when compared with the preoperative clinical picture.
DISCUSSION
The treatment of acromioclavicular dislocation types I and II is managed conservatively with most patients returning to pre-injury conditions3, 4, 5, 6, 7, whereas types IV, V and VI are typically treated surgically8, 9, 10, 11, 12. Although the treatment of type III ACD is controversial(13), many recommend conservative treatment with the use of a sling without concern for the reduction of the dislocation(14), while others believe surgery is necessary(15). We observed better results through subjective clinical evaluation, assessing the range of motion and the muscle strength using a Cybex device when treating these patients surgically, and therefore advocate the latter.
Surgical treatment of acromioclavicular dislocation is typically reserved for full displacements. In acute dislocation of the acromioclavicular joint, reconstruction of the coracoclavicular ligaments has also been employed16, 17, 18. Surgical options are numerous; surgeons can choose from dozens of techniques(11). We currently opted for the Arthrex® TightRope system which seeks to substitute the coracoclavicular ligaments through four Arthrex® No. 5 Fiberwires so that they are supported in tension through supraclavicular and infracoracoid metal buttons, by vision under arthroscopy. To our knowledge, the first reported experience of the use of this arthroscopic technique was published in 2006(19).
The literature confirms the effectiveness of the Arthrex® TightRope system with results similar to ours, which reinforces the effectiveness of the method and thus encourages the application of this minimally invasive procedure19, 20.
Veado et al. note that surgery should not be performed in the acute phase if there is excoriation/abrasion at the location or presence of blistering or infected skin in the region of the shoulder girdle(16). We support this course of action, since even employing a minimally invasive procedure, we believe that not correcting such problems beforehand poses an unnecessary risk that compromises surgery.
CONCLUSION
The application of the Arthrex® TightRope system in the arthroscopic treatment of acromioclavicular dislocation proved to be a less surgically aggressive technique that is efficient in promoting pain relief with deformity correction and restoration of the range of motion within a short time. It is a procedure with low morbidity and is easy to use after the technique is mastered.
Footnotes
We declare no conflict of interest in this article.
Study completed at the Bahia Institute of Orthopedics and Traumatology (INSBOT – Instituto Baiano de Ortopedia e Traumatologia) and the Hospital Portugués da Bahia, Salvador, Bahia, Brazil
REFERENCES
- 1.Mazzocca AD, Santangelo SA, Johnson ST, Rios CG, Dumonski ML, Arciero RA. A biomechanical evaluation of an anatomical coracoclavicular ligament reconstruction. Am J Sports Med. 2006;34(2):236–246. doi: 10.1177/0363546505281795. [DOI] [PubMed] [Google Scholar]
- 2.Rockwood CA, Jr, Williams GR, Young DC. Disorders of the acromioclavicular joint. In: Rockwood CA, Matsen FA, editors. The shoulder. 2nd ed. Saunders; Philadelphia: 1998. pp. 483–553. [Google Scholar]
- 3.Cox JS. The fate of the acromioclavicular joint in athletic injuries. Am J Sports Med. 1981;9:50–53. doi: 10.1177/036354658100900111. [DOI] [PubMed] [Google Scholar]
- 4.Dias JJ, Steingold RF, Richardson RA, Tesfayohannes B, Gregg PJ. The conservative treatment of acromioclavicular joint dislocation: review after five years. J Bone Joint Surg Br. 1987;69:719–722. doi: 10.1302/0301-620X.69B5.3680330. [DOI] [PubMed] [Google Scholar]
- 5.Galpin RD, Haekins RJ, Grainger RW. A comparative analysis of operative versus non-operative treatment of grade III acromioclavicular separations. Clin Orthop Relat Res. 1985;193:150–155. [PubMed] [Google Scholar]
- 6.Lemos MJ. The evaluation and treatment of the injured acromioclavicular joint in athletes. Am J Sports Med. 1998;26:137–144. doi: 10.1177/03635465980260010801. [DOI] [PubMed] [Google Scholar]
- 7.Bannister GC, Wallace WA, Stableforth PG, Hutson MA. The management of acute acromioclavicular dislocation: a randomized prospective controlled trial. J Bone Joint Surg Br. 1989;71:848–850. doi: 10.1302/0301-620X.71B5.2684990. [DOI] [PubMed] [Google Scholar]
- 8.Larsen E, Berg-Nielsen A, Christensen P. Conservative or surgical treatment of acromioclavicular dislocation: a prospective, controlled, randomized study. J Bone Joint Surg Am. 1986;68:552–555. [PubMed] [Google Scholar]
- 9.Sloan SM, Budoff JE, Hipp JA, Nguyen L. Coracoclavicular ligament reconstruction using the lateral half of the conjoined tendon. J Shoulder Elbow Surg. 2004;13:186–190. doi: 10.1016/j.jse.2003.12.002. [DOI] [PubMed] [Google Scholar]
- 10.Tienen TG, Oyen JF, Eggen P. A modified technique of reconstruction for complete acromioclavicular dislocation: a prospective study. Am J Sports Med. 2003;31:655–659. doi: 10.1177/03635465030310050401. [DOI] [PubMed] [Google Scholar]
- 11.Weaver JK, Dunn HK. Treatment of acromioclavicular injuries, especially complete acromioclavicular separation. J Bone Joint Surg Am. 1972;54:1187–1194. [PubMed] [Google Scholar]
- 12.Ellman H, Hanker G, Bayer M. Repair of the rotator cuff. End-result study of factors influencing reconstruction. J Bone Joint Surg Am. 1986;68(8):1136–1144. [PubMed] [Google Scholar]
- 13.Bailey RW. A dynamic repair for complete acromioclavicular joint dislocation. J Bone Joint Surg Am. 1965;47:858. [Google Scholar]
- 14.Veado MAC, Paiva AA, Pinto MS. Tratamento cirúrgico da luxação acromioclavicular completa. Rev Bras Ortop. 2000;35(8):309–313. [Google Scholar]
- 15.Galpin RD, Hawkins RJ, Grainer RW. A comparative analysis of operative versus nonoperative treatment of grade III acromioclavicular reparations. Clin Orthop Relat Res. 1985;193:150–155. [PubMed] [Google Scholar]
- 16.Harris RI, Wallace AL, Harper GD, Goldberg JA, Sonnabend DH, Walsh WR. Structural properties of the intact and the reconstructed coracoclavicular ligament complex. Am J Sports Med. 2000;28:103–108. doi: 10.1177/03635465000280010201. [DOI] [PubMed] [Google Scholar]
- 17.Tsou PM. Percutaneous cannulated screw coracoclavicular fixation for acute acromioclavicular dislocations. Clin Orthop Relat Res. 1989;243:112–121. [PubMed] [Google Scholar]
- 18.Weinstein DM, McCann PD, Mcllveen SJ, Flatow EL, Bigliani LU. Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med. 1995;23:324–331. doi: 10.1177/036354659502300313. [DOI] [PubMed] [Google Scholar]
- 19.Hernegger GS, Kadletz R. Tight rope – the revolutionary anatomical fixation in acromioclavicular joint dislocation – a case report. Tech Shoulder Elbow Surg. 2006;7(2):86–88. [Google Scholar]
- 20.Richards A, Duncan TT. Arthroscopic stabilization of acute acromioclavicular joint dislocation using the tightrope system. Tech Shoulder Elbow Surg. 2008;9(2):51–54. [Google Scholar]