

Abstract
To confirm the therapeutic importance of hip arthroplasty in athletes whose pain precludes sportive function of the hip joint, being able to minimize it to the extent of helping on the return of sports practice at satisfactory levels. Methods: 49 athlete patients (51 hips) submitted to hip arthroscopy complaining of pain and inability to practice sports were assessed. Follow-up time ranged from 12 to 74 months (mean: 39.0 months). Preoperatively, pain site, severity according to Facial Expression Scale (FES) and the degree of disability using the modified Harris Hip Score (HHS) were assessed. Different diagnoses were provided, which led to the indication of arthroscopy, such as femoralacetabular impact, acetabular lip injury not secondary to femoral-acetabular impact, etc. Postoperatively, the patients were assessed by using the same methods as used at baseline and by the subjective analysis of return to sports activities. Results: Based on pre-and postoperative HHS and FES, the statistical analysis showed significance between values. We found some improvement in all cases and return to sports activities at a satisfactory level in most of the cases. Conclusion: As a result of our study, we confirm that arthroscopy in athletes with local hip injuries is an effective technique, able to promote the return to sports practice in most of the cases, without pain, and with an effective joint function, provided well indicated.
Keywords: Arthroscopy, Acetabular, Hip, Sports
INTRODUCTION
Shoulder and knee arthroscopy in athletes is a common procedure and its indications are well-defined. Over the years, arthroscopy of other joints such as the elbow, ankle, and wrist have become popular. In the hip, this enthusiasm lagged because the joint is deep and access is more difficult due to the anatomy of the joint. Even so, it has become a reality in the United States and Europe, as well as in Brazil and throughout Latin America, with increasingly frequent indications for different conditions(1).
Since Glick(2) published the technique with the patient positioned in lateral recumbency, after discovering that one can visualize the large joint area by the lateral traction vector, hip arthroscopy has gained great momentum, demonstrating itself to be a safe procedure of great diagnostic and therapeutic importance.
With the growing number of sports practitioners seeking a fit body and a healthier life intending to improve their performance, the number of hip conditions related to sports has been increasing(3).
The main cause of hip pain in athletes is injury to the acetabular lip due to acute traumatic causes or, much more frequently, to complex mechanisms that have not been fully elucidated(4). Femoroacetabular impingement (FAI) is one of those causes and has been gaining importance as the main cause of injury to the acetabular lip.
Arthroscopic procedures can help in this context, making a satisfactory recovery possible in order to allow patients to return to sports(5).
The aim of this study is to confirm the therapeutic significance of hip arthroscopy in athletes with pain that is incapacitating in relation to sports.
METHODS
We define sports as the set of regular physical exercises that is performed by an individual or collectively(6). According to this definition, 49 individuals (51 hips) practicing sports who had debilitating pain in the hip joint that prevented them from performing sports were evaluated. Of these, 32 were male (65.3%) and 17 were female (34.7%). Ages ranged from 16 to 51 years (an average of 33.1 years). Among the subjects studied, 42 were White (85.8%), three were Black (6.1%), three were of mixed ethnicity (6.1%), and one person was of Asian descent (2.0%). The right hip was the most affected in 33 subjects (64.7%) and the left hip in 18 (35.3%). The sport that was the most played was soccer in 14 cases (28.5%). The minimum follow-up period was 12 months and maximum 74 months (averaging 39 months). In the preoperative period, we assessed the location of the pain and its intensity according to the Facial Expression Scale (FES)(7), and the degree of disability using the criteria of the Harris Hip Score modified by Bird (HHS)(8).
After surgery, patients were reassessed at various times using the same criteria as in the preoperative period (HHS and FES).
To assess whether there was a difference between the FES values before and after surgery, we performed the Wilcoxon test to test continuous variables. We considered p values < 0.05 for statistically significant differences in the values of FES before and after arthroscopy.
The Wilcoxon test was used to test the HHS variable, with p values < 0.05 considered statistically significant differences in relation to the HHS values before and after arthroscopy. To analyze the various diagnoses that led to the indication for surgery, patients were divided into three groups according to the intraoperative diagnosis, namely: group A, those with a diagnosis of femoroacetabular impingement (54.9%), group B, those with lesions of the acetabular lip not secondary to FAI (35.5%) and group C, patients with other diagnoses (9.6%) (Tables 1 and 2). All patients underwent anatomical correction of the anatomical deformities by osteoplasty, both acetabulum (pincer) and femoral (cam) when present.
Table 1.
Diagnostic Frequency of Groups A, B and C.
| Diagnosis | Frequency | Percentage |
|---|---|---|
| Group A – Femoroacetabular impingement | 28 | 54.9% |
| Group B – Labial lesion not secondary to femoroacetabular impingement | 18 | 35.5% |
| Group C – Other diagnoses | 5 | 9.6% |
| Total | 51 | 100% |
Table 2.
Diagnostic Frequency of Group C
| Diagnosis | Frequency | Percentage |
|---|---|---|
| Chronic tendinitis in the iliopsoas muscle tendon | 2 | 3.9% |
| Iliotibial band syndrome | 1 | 1.9% |
| Round ligament lesion | 1 | 1.9% |
| Inflammatory hip disease | 1 | 1.9% |
| Total | 5 | 9.6% |
The HHS and FES values before and after surgery were studied using the Kruskal-Wallis test, in order to assess possible differences between the three groups studied. We considered p values < 0.05 to be statistically significant.
To evaluate the level of return to sports activities in the postoperative period in the most simple manner possible, we used a subjective criterion: whether or not the patient returned to the sport. For those who returned, individuals were asked to categorize their return as satisfactory or unsatisfactory. A return was considered satisfactory if it was asymptomatic, with normal function.
RESULTS
We found that 47 patients (96.0%) returned to the sport in some way. Among them, 36 (73.0%) showed normal, asymptomatic performance, 11 (23.0%) did so in a way that they considered unsatisfactory, and two (4%) left the sport because of experiencing pain in the hip during its practice (Figures 1 and 2). When all 51 cases were analyzed, the HHS variable observed in the preoperative period had an average of 62.3 points, while in the postoperative period the average was 98.3 points, constituting a statistically significant value (p < 0.001). FES, which in the preoperative period was on average 2.16 points, in the postoperative period was 5.86 points, a value that is statistically significant (p < 0.001).
Figure 1.
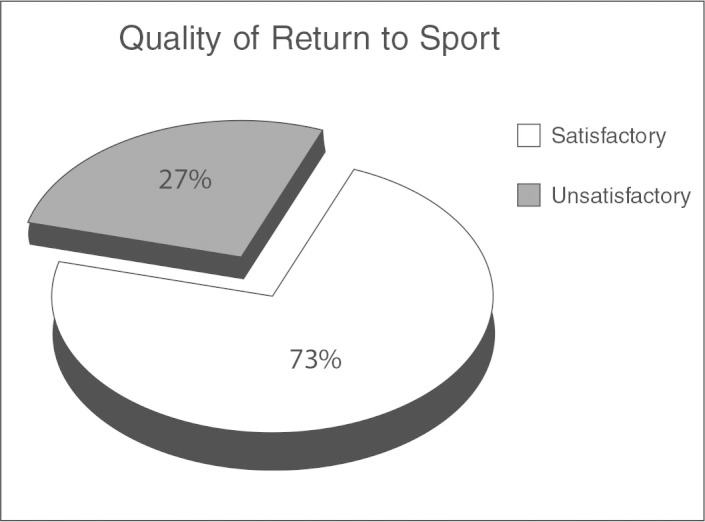
Subjective scale of return to sport.
Figure 2.
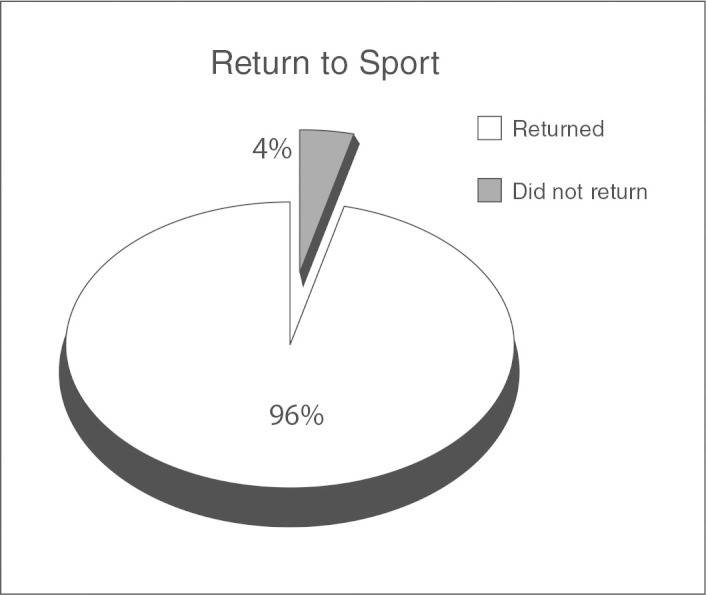
Evaluation of return to sport.
When the groups are studied separately, we observed in group A a variation of 62.2 points from the preoperative HHS to 98.7 points in the postoperative evaluation (p < 0.001), and for FES the preoperative 2.2 points increased to 5.9 points postoperatively (p < 0.001). Group B showed an improvement from 65.5 points to 99.1 in HHS (p < 0.001) and from 2.1 to 5.9 points in FES (p < 0.001), while for group C the variation was from 54.6 points to 94.9 in HHS (p < 0.028) and from 1.5 points to 5.3 points in FES (p < 0.027) (Figures 3 and 4).
Figure 3.
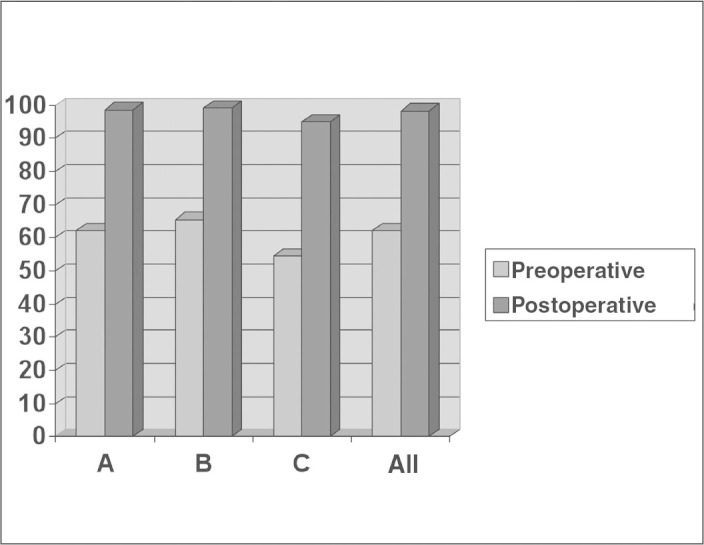
Changes between the pre- and postoperative HHS.
Figure 4.
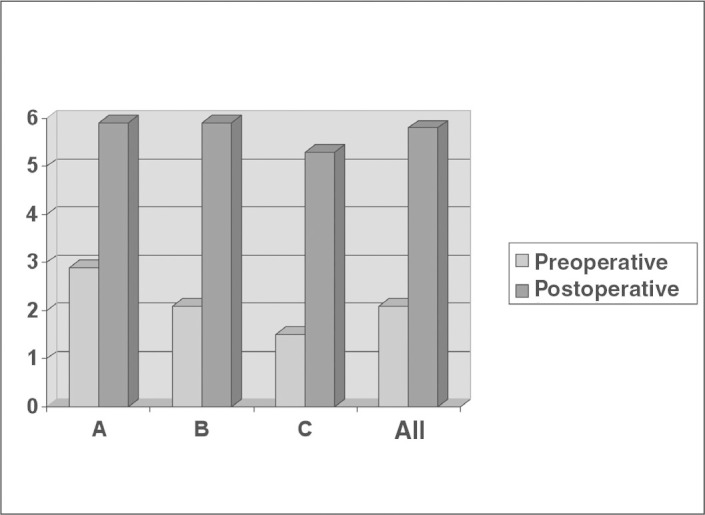
Changes between the pre- and postoperative FES.
When we compared clinical improvement between the groups, that is, if a group had better results than the others, we found no statistically significant differences, with p < 0.126 for HHS and p < 0.918 for FES.
DISCUSSION
In the pursuit of health and quality of life, people are increasingly seeking sports as the solution. The number of people who regularly practice sports increases every year. Amateur and professional athletes undergo great exertion, which can affect their joints, making them conducive to injury(5). As a result of this sports bevahior, shocks and traumas to skeletal structures are increasingly more frequent, increasing the risk of joint injury and damage. Similarly, the increasing demands of physical capacity increases the risk of these lesions(9). The evolution of medical technology in recent decades has had an impact on sports with major advances in the physical preparation of athletes and the consequent requirement for maximum performance(10). The mechanism of injury may be due to direct trauma or repetitive strain(5). In regards to the topography of the lesions, there is greater involvement of the lower limbs, a finding that is probably explained by the fact that soccer is the most practiced sport in our country10, 11, 12.
Byrde and Ganz et al. consider the combination of flexion, adduction, and internal rotation of the hip causing pain in the groin (FADIR-test) as the most sensitive test for intra-articular hip injury13, 14. McCarthy et al.(15) reported that hip arthroscopy is a valuable and feasible procedure, and indicate it for patients with refractory hip pain to clinical treatment for more than six months.
Femoroacetabular impingement is gaining importance as the main cause of injury to the acetabular lip. It is defined as abnormal contact between the acetabulum and the femoral neck during mobilization of the hip, especially in flexion and internal rotation, limiting the range of motion(16).
Londers et al. analyzed 56 cases of hip arthroscopies performed in patients complaining of pain in the joint for more than six months, pain that was refractory to clinical treatment and positive on the FADIR-test(17). They found 80% good results with return to the activities of daily living and sports; 2% of patients reported worsening of pain and could not return to sports activities. Acetabular lip injury was identified in 62% of cases and poor results correlated with the degree of these cartilaginous lesions (Outerbridge III and IV(18)), but no mention was made of femoroacetabular impingement as a possible cause of injury to the lip, and the arthroscopic treatment procedures performed were not described as we have in this study. Londers et al. demonstrated that in 11% of cases improvement was temporary, with a return of previous symptoms, and that all cases had mild (Outerbridge I and II) or no damage to the cartilage, suggesting a structural cause for the return of symptoms(17).
Heyworth et al. reviewed 24 cases of hip arthroscopy that had evolved to poor results in an average period of six months and found that 19 of them (79%) had femoroacetabular impingement that was identifiable on preoperative radiographs but was not treated during the arthroscopic procedure(19). They suggest that lesions of the acetabular lip may show underdiagnosed structural changes of the hip and that FAI that is not adequately treated is the main cause of persistent symptoms after debridement of acetabular lip lesions(19).
Byrd et al. observed that in 42 athletes (44 hips), 27 (61.3%) had acetabular lip injury, but the authors did not state whether the injuries were isolated or describe their possible causes(20). The percentage index was at variance with that observed in our series (18 cases – 35.5%). This is probably due to the separation of cases of labial lesion caused by femoroacetabular impingement from cases that were secondary to other conditions.
Philippon reported HHS improvements in all of his athletes, and noted that 84.8% of cases returned to sports and 15.2% were unable to resume a previous level of sports activity(5). Our series showed that most patients returned to sports in some way, 76% in an asymptomatic manner.
McCarthy et al., reviewing 170 cases of arthroscopy in dysplastic hips, found acetabular lip lesions in 42% of them, of which 85% showed good results after arthroscopic debridement(4). In our study we found the lesion of the acetabular lip to be the main cause of pain for those who underwent hip arthroscopy, similar to the literature(4). We chose to separate injuries secondary to FAI in order to establish the importance of this condition, which is often underdiagnosed and suggested as the main cause of symptoms persisting after arthroscopy(19). We have attempted to find differences between patients undergoing suturing and debridement of the lesions, but this was not possible due to the sample size and length of follow-up. Instead of resection, we opted for the suture based on studies such as Ikeda et al. that compare acetabular lip injuries to meniscal injuries(21). Ferguson et al. cite the functions of the acetabular lip as important, justifying its repair: impact absorption, impact distribution, pressure distribution, and joint stabilization and sealing(22). Other authors have cited that acetabular lip lesion sutures achieve better outcomes than resections of acetabular lip(23). We did not correlate the degree of cartilage damage with functional results in our patients, since none of the cases had patients with loss of joint space, but this seems to be a point of strong association and should be taken into consideration17, 19. We found that 96% of cases resumed sports after arthroscopy, of which 76% were satisfactory, that is, asymptomatic and similar to pre-injury. This finding is similar to that found in the literature and desmontrates the good results of the arthroscopic technique5, 17.
Good treatment results of any disease are always secondary to the good indication of the procedure adopted and good patient selection. Thus, patients with hip osteoarthritis radiographically evidenced by loss of joint space and osteophyte formation are not good candidates for any arthroscopic procedure in this joint, whether athletes or not(13).
Byrd et al. believe that clinical improvement reaches its maximum at three months of postoperative follow-up, and that these results tend to be better in younger patients and tend to remain stable over at least five years(20).
A direct comparison of all diagnoses was not possible due to the small number of cases of patients with other injuries, which required the grouping of these into one group (five cases – 9.8%). Thus, comparing them, we did not observe better results for the arthroscopic technique between the different diagnoses found in our athletes, which is not a prognostic criterion of arthroscopy.
HHS is an imperfect scale for the evaluation of the hip, but it is well-known, standardized, validated, and the orthopedist is familiar with it. This allows for an objective and reliable assessment of pain and functionality of this joint1 . We do not have a standardized qualitative scale to specifically assess resuming sports, but as we deem it important to analyze the data we obtained, we used a subjective scale of return to sports. Most patients reported the asymptomatic resumption of sports activities, which reflects the good results of the arthroscopic technique in this group of athletes.
CONCLUSION
Given what has been studied, we confirm that arthroscopy is an effective technique in athletes with lesions located in the hip, capable of promoting their return to sports, with effective and painless joint function in most cases.
ACKNOWLEDGEMENTS
We thank the Publication Support Nucleus for technical and scientific support in the publication of this manuscript.
Footnotes
We declare no conflict of interest in this article.
Study conducted at the Department of Orthopedics and Traumatology, School of Medical Sciences, Santa Casa de São Paulo (FCMSCSP)
Polesello GC, Honda E, Ono N, Guimarães R, Aristide RSA. Artroscopia do Quadril – Atualização. Educação continuada/SBOT 25:32 Junho 2005.
Contributor Information
Giancarlo Cavalli Polesello, Email: giancarlopolesello@hotmail.com.
Guilherme Do Val Sella, Email: hladefin@fmrp.usp.br.
REFERENCES
- 1.Kelly BT, Williams RJ, 3rd, Philippon MJ. Hip arthroscopy: current indications, treatment options, and management issues. Am J Sports Med. 2003;31(6):1020–1037. doi: 10.1177/03635465030310060701. [DOI] [PubMed] [Google Scholar]
- 2.Glick JM. Hip arthroscopy. The lateral approach. Clin Sports Med. 2001;20(4):733–747. doi: 10.1016/s0278-5919(05)70281-7. [DOI] [PubMed] [Google Scholar]
- 3.Raymundo JLP, Reckers LJ, Locks R, Silva L, Hallal PC. Perfil das lesões e evolução da capacidade física em atletas profissionais de futebol durante uma temporada. Rev Bras Ortop. 2005;40(6):341–348. [Google Scholar]
- 4.McCarthy JC, Lee JA. Hip arthroscopy: indications, outcomes, and complications. J Bone Joint Surg Am. 2005;87(5):1138–1145. [Google Scholar]
- 5.Philippon MJ. Arthroscopy of the hip in the management of the athlete. In: McGinty JB, editor. Operative arthroscopy. 3rd ed. Lippincott, Williams & Wilkins; Philadelphia: 2003. pp. 879–883. [Google Scholar]
- 6.Ferreira ABH. Novo Dicionário da Língua Portuguesa. 2a ed. Nova Fronteira; Rio de Janeiro: 1986. p. 708. [Google Scholar]
- 7.Pimenta CAM, Teixeira MJ. Avaliação da dor. Rev Med (São Paulo). 1997; 76(edição especial):27-35.
- 8.Byrd JW, Jones KS. Prospective analysis of hip arthroscopy with 2-year follow-up. Arthroscopy. 2000;16(6):578–587. doi: 10.1053/jars.2000.7683. [DOI] [PubMed] [Google Scholar]
- 9.Bjordal JM, Arnly F, Hannestad B, Strand T. Epidemiology of anterior cruciate ligament injuries in soccer. Am J Sports Med. 1997;25(3):341–345. doi: 10.1177/036354659702500312. [DOI] [PubMed] [Google Scholar]
- 10.Cohen M, Abdalla RJ, Ejnisman B, Amaro JT. Lesões ortopédicas no futebol. Rev Bras Ortop. 1997;32(11):940–944. [Google Scholar]
- 11.Pedrinelli A. Incidência de lesões traumáticas em atletas de futebol [dissertação] Faculdade de Medicina da Universidade de São Paulo; São Paulo: 1994. [Google Scholar]
- 12.Ladeira CE. Incidência de lesões no futebol: um estudo prospectivo com jogadores masculinos adultos amadores canadenses. Rev Bras Fisioter. 1999;4(1):39–47. [Google Scholar]
- 13.Byrd JW. Hip arthroscopy: pacients assessment and indications. Instr Course Lect. 2003;52:711–719. [PubMed] [Google Scholar]
- 14.Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;(417):112–120. doi: 10.1097/01.blo.0000096804.78689.c2. [DOI] [PubMed] [Google Scholar]
- 15.McCarthy JC, Busconi B. The role of hip arthroscopy in the diagnosis and treatment of hip disease. Orthopedics. 1995;18(8):753–756. doi: 10.3928/0147-7447-19950801-12. [DOI] [PubMed] [Google Scholar]
- 16.Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis–what the radiologist should know. AJR Am J Roentgenol. 2007;188(6):1540–1552. doi: 10.2214/AJR.06.0921. [DOI] [PubMed] [Google Scholar]
- 17.Londers J, Van Melkebeek J. Hip arthroscopy: outcome and patient satisfaction after 5 to 10 years. Acta Orthop Belg. 2007;73(4):478–483. [PubMed] [Google Scholar]
- 18.Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br. 1961;43:752–757. doi: 10.1302/0301-620X.43B4.752. [DOI] [PubMed] [Google Scholar]
- 19.Heyworth BE, Shindle MK, Voos JE, Rudzki JR, Kelly BT. Radiologic and intraoperative findings in revision hip arthroscopy. Arthroscopy. 2007;23(12):1295–1302. doi: 10.1016/j.arthro.2007.09.015. [DOI] [PubMed] [Google Scholar]
- 20.Byrd JW, Jones KS. Hip arthroscopy in athletes. Clin Sports Med. 2001;20(4):749–761. [PubMed] [Google Scholar]
- 21.Ikeda T, Awaya G, Suzuki S, Okada Y, Tada H. Torn acetabular labrum in yung patients: arthroscopic diagnosis and management. J Bone Joint Surg Br. 1988;70(1):13–16. doi: 10.1302/0301-620X.70B1.3339044. [DOI] [PubMed] [Google Scholar]
- 22.Ferguson SJ, Bryant JT, Ganz R, Ito K. The influence of the acetabular labrum on hip joint cartilage consolidation: a poroelastic finite element model. J Biomech. 2000;33(8):953–960. doi: 10.1016/s0021-9290(00)00042-7. [DOI] [PubMed] [Google Scholar]
- 23.Espinosa N, Rothenfluh DA, Beck M, Ganz R, Leunig M. Treatment of femoro-acetabular impingement: preliminary results of labral refixation. J Bone Joint Surg Am. 2006;88(5):925–935. doi: 10.2106/JBJS.E.00290. [DOI] [PubMed] [Google Scholar]