

Abstract
Aim:
The aim and purpose of this study was to determine the occlusal fracture resistance of three core buildup materials using the Nayyar technique.
Materials and Methods:
Thirty human extracted maxillary premolars were used for the study. The test samples were decoronated till the cementoenamel junction (CEJ) and proper cleaning and shaping was done with protaper niti files till the F3. Corresponding f3 protaper(Dentysply)gutta pecha cones were selected and obturated. The gutta-percha was removed till the depth of 4 mm from the coronal orifice with Gates Glidden (GG) drills for all the samples; then the samples were randomly divided into three different groups. Group I was restored with universal composite Z350XT, group II was restored with light curable glass ionomer cement (GIC), and group III was restored with miracle mix. The coronal buildup was done using compound supported matrix. The fracture resistance strength of all the specimen groups was tested under a universal testing machine.
Results:
The data of the study were statistically analyzed by one-way analysis of variance (ANOVA) and Bonferroni's comparison test. Results of the study showed that group I that was restored with the universal composite Z350XT showed much higher fracture resistance strength compared to the other two groups. Statistically significant difference was noted between group I and group II and also between group I and group III.
Conclusion:
It can be concluded that the core buildup done with composite offered better occlusal fracture resistance strength compared to light curable GIC and miracle mix.
Keywords: Core buildup materials, corono-radicular build-up, fracture, fracture resistance, materials, Nayyar cores, resistance
INTRODUCTION
The success of root canal therapy depends on the fluid tight seal at the apex and orifice in the pulp chamber. Most of the root canal treated tooth will require a buildup, which may be as simple as closing the access opening or restoring the complete tooth. The optimal core buildup material should have adequate strength, must be biocompatible, exhibit a high level of resistance to bacterial leakage, and be dimensionally stable in the presence of oral fluids.[1]
Many procedures, techniques, and various materials have been suggested for core buildup. However, all of them are based on personal preference and clinical experience with no research evidence for superiority of one over the other.
Nayyar et al. suggested a technique using an amalgam dowel–core. In this technique, retention for the amalgam-core is derived from the remaining pulp chamber and the prepared canals by extending amalgam to these areas.[2] This technique involves the removal of obturated gutta-percha to the depth of 2–4 mm from canal orifice and restoring with amalgam. The quality of root canal treatment and prosthodontic reconstruction are the two key factors which determine the longevity of grossly decayed tooth.[3] This study focuses on the evaluation of occlusal fracture resistance strength of the three different core materials using Nayyar technique.
MATERIALS AND METHODS
Thirty human extracted maxillary premolars were used for the study. All the samples were decoronated till the cementoenamel junction (CEJ) and proper cleaning and shaping were done with (Dentysply) Protaper rotary instruments till F3, prepared samples roots were obturated with the corresponding protaper guttaperch cones (dentysply). The gutta-percha was removed till the depth of 4 mm from the coronal orifice with Gates Glidden (GG) drills for all the samples then randomly grouped into three groups.
Group I—Ten samples were restored with the composite Z350XT. The samples were mounted on a custom-made wax block and t-band was placed around the tooth as shown in Figure 1. Wax compound was heated and placed around the banded sample to secure it firmly. Composite restoration was done incrementally to make sure that the restored material reached till the depth of 4 mm of the radicular space followed by the coronal buildup.
Figure 1.

Compound supported matrix and the restored samples
Group II—Ten samples were restored with light curable glass ionomer cement (GC Fuji) Restoration procedure was followed according to the manufacturer recommendations. The same procedure for coronal buildup was followed for this group as that of group I.
Group III—Ten samples were restored with miracle mix (GC Fuji). The core buildup method as mentioned in group I was followed for all the specimens. All the samples were polished after they were restored. The samples were mounted on acrylic blocks and were inserted into a custom-made metal jig. This metal jig was placed parallel to the long axis of the upper arm of the universal testing machine with tapering tip. A static load with 0.5mm speed was applied on the specimens to the point of fracture and values were noted. The noted [Figure 2] values were analyzed using one-way analysis of variance (ANOVA) and Bonferroni's test to compare between the groups.
Figure 2.

Samples testing under a universal testing machine
RESULTS
One-way ANOVA and Bonferroni's comparison test revealed significant differences in the fracture resistance of the core materials. The results of the study showed higher occlusal fracture resistance in group I. The mean fracture resistance of group I is 1.213 kN, which is much higher and statistically significant compared to that of the other groups. The mean fracture resistance of group 2 was 0.76 Kn and group III showed mean fracture resistance of 0.30 kN, which is lowest of all the three groups [Graph 1]. Comparatively statistically significant difference was observed between group I and group II and also between group I and group III [Graph 2].
Graph 1.
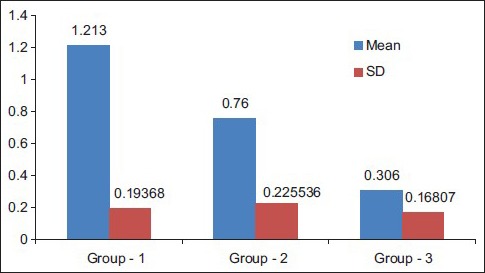
Bar chart shows difference between mean and standard deviation of three groups
Graph 2.
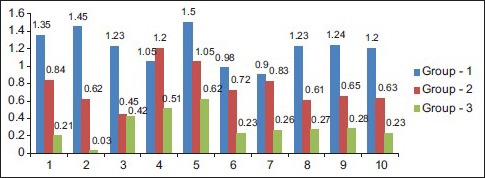
Bar chart between group- 1,2,3
DISCUSSION
Appropriate reconstruction of the tooth structure is important for the success of good root canal treatment.[4] It has been suggested that placing a post in a root-treated-tooth would pose extra risks to the fracture of the tooth itself.[5] Hence, the Nayyar technique was preferred in this study. However, at the same time, the superiority of the Nayyar core is also unclear. Therefore, proper understanding and knowing about the restorative techniques that could ensure the longevity of an already weakened tooth would prove beneficial for the dentist as well as the patient. This study made an attempt to provide new knowledge regarding the clinical efficacy of these restorative modalities of the lost coronal structure of endo-treated teeth before placing crowns on them. It was determined whether placing a conventional post-core or a corono-radicular restoration (Nayyar core) was preferable for endodontically treated premolars.
Root canal treated teeth are susceptible to fracture as the tooth undergoes coronal and radicular structural loss due to caries, endodontic treatment, and/or restorative procedures. Various studies have shown that root canal treated tooth has reduced proprioception, which could impair the normal reflexes and lead to fracture of the tooth.[6]
Ideal requirement for a core buildup should exhibit satisfactory mechanical and physical properties to resist intraoral forces. All the three materials used in the study are core buildup materials.
Group I restored with composite exhibited higher fracture resistance strength compared with other two materials. The mean fracture resistance strength of group I is 1.213 kN, which is much higher when compared to those of the other two groups. The advantage of composite material is that it can be directly placed in the pulp chamber and it has better control over the setting. They show better bonding to the tooth structure by micromechanical bonding.[7,8] Composites have shown to exhibit higher mechanical and physical properties compared to various core buildup materials.[9] Hence, the use of composite as core materials increased rapidly.
Group II showed mean fracture resistance of 0.76 Kn. This value was comparatively lower than group I. However when compared to group III it was higher, suggesting that this could be due to the material composition of light curable gic. The pressance of Urethrene Dimethacrylate[10] (UDMA) in the liquid of group II might be the reason for higher fracture resistance. UDMA contains hydroxyl groups that enable the formation of strong hydrogen bonds resulting in higher resistance to fracture in group II.
Group III restored with miracle mix showed least occlusal fracture resistance. The mean fracture resistance strength of this group is 0.30 kN, which is very low compared to that of other two groups. The reason for least resistance could be due to incorporation of metallic fillers. These fillers do not provide additional advantages over conventional GIC.[7] Restoration with miracle mix has shown poor adhesion to the tooth structure, but the only advantage was that release of fluoride ions.[11]
Limitations of this study were as follows:
Minimal sample size
This being in vitro study could not mimic the exact intraoral condition
Direction of the force of the universal testing machine was only toward occlusal surface.
Despite these limitations, the results provided the valuable information of fracture resistance strength of the three core materials tested. Further clinical studies have to be done to know the suitability of these materials for clinical use.
CONCLUSION
According to this study, it can be concluded that core buildup done with composite offered better fracture resistance in root canal treated tooth using Nayyar technique when compared to other two test materials.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
Lenora Dental College and Hospital, Rajahmundry, Andhra Pradesh, is acknowledged for providing us an opportunity to conduct the study.
REFERENCES
- 1.Nayyar A, Walton RE, Leonard LA. An amalgam coronal-radicular dowel and core technique for endodontically treated posterior teeth. J Prosthet Dent. 1980;43:511–5. doi: 10.1016/0022-3913(80)90322-4. [DOI] [PubMed] [Google Scholar]
- 2.Eakle WS, Maxwell EH, Braly BV. Fractures of posterior teeth in adults. J Am Dent Assoc. 1986;112:215–8. doi: 10.14219/jada.archive.1986.0344. [DOI] [PubMed] [Google Scholar]
- 3.Cheung W. A review of the management of endodontically treated teeth. Post, core and the final restoration. J Am Dent Assoc. 2005;136:611–9. doi: 10.14219/jada.archive.2005.0232. [DOI] [PubMed] [Google Scholar]
- 4.Heydecke G, Butdz F, Strub JR. Fracture strength and survival rate of endodontically treated maxillary incisors with approximal cavities after restoration with different post and core systems: An in-vitro study. J Dent. 2001;29:427–33. doi: 10.1016/s0300-5712(01)00038-0. [DOI] [PubMed] [Google Scholar]
- 5.Kishen A. Mechanisms and risk factors for fracture predilection in endodontically treated teeth. Endod Topics. 2006;13:57–83. [Google Scholar]
- 6.Anusavice KJ. 11th ed. St Louis USA: Saunders; 2003. Physical Properties of Dental Materials in Phillips Science of Dental Materials; pp. 100–134. [Google Scholar]
- 7.Craig RG, Powers JM, Wataha JC. Properties of Materials in Dental Materials. St Louis USA: Mosby; 2004. pp. 51–32. [Google Scholar]
- 8.Chutinan S, Platt JA, Cochran MA, Moore BK. Volumetric dimensional change of six direct core materials. Dent Mater. 2004;20:345–51. doi: 10.1016/S0109-5641(03)00127-1. [DOI] [PubMed] [Google Scholar]
- 9.Asmussen E, Peutzfeldt A. Influence of UEDMA, BisGMA and TEGDMA on selected mechanical properties of experimental resin composites. Dent Mater. 1998;14:51–6. doi: 10.1016/s0109-5641(98)00009-8. [DOI] [PubMed] [Google Scholar]
- 10.Bapna MS, Gadia CM, Drummond JL. Effects of aging and cyclic loading on the mechanical properties of glass ionomer cements. Eur J Oral Sci. 2002;110:330–4. doi: 10.1034/j.1600-0722.2002.21225.x. [DOI] [PubMed] [Google Scholar]
- 11.Helfer AR, Melnick S, Schilder H. Determination of the moisture content of vital and pulpless teeth. Oral Surg Oral Med Oral Pathol. 1972;34:661–70. doi: 10.1016/0030-4220(72)90351-9. [DOI] [PubMed] [Google Scholar]