

Abstract
Introduction:
Vitiligo is a progressive, idiopathic, pigmentation disorder of the skin, characterized by hypopigmented patches. This condition is compared with Shvitra in Ayurveda. Many Ayurvedic drugs are beneficial in such cases and Apamarga Kshara Yoga is one among them.
Aim:
To evaluate the efficacy of Apamarga Kshara Yoga in Lepa and ointment forms in the management of Shvitra.
Materials and Methods:
Total 50 patients of Shvitra were randomly grouped into two. Patients registered in Group A (n = 25) were treated with Apamarga Kshara Yoga Lepa and Group B (n = 25) with Apamarga Kshara Yoga ointment for 2 months. Rasayana Churna (3g) along with Honey and Ghee was given twice daily internally in the both groups.
Results:
Significant improvement was found in the symptoms of Shvitra with treatment in both the groups. The difference in between the groups was statistically insignificant.
Conclusion:
Both forms of Apamraga Kshara Yoga are effective in cases of Shvitra and can be good alternatives for contemporary medicines.
Keywords: Apamarga Kshara, Lepa, Leucoderma, Manahshila, Shvitra, Vitiligo
Introduction
There is a continuous search for better remedies to combat vitiligo (leucoderma) that is characterized by hypopigmented patches over the body. Though, it is not associated with any major systemic illness, such lesions will lead to social stigma, may affect the psychological status of the individual and has a major impact on self-esteem and perception of the self. Vitiligo is one of the oldest and commonest skin disorders affecting approximately 1–2% of the human population.[1] Based on the dermatological outpatient's records, the incidence of vitiligo is found to be 0.25 to 2.5% in India.[2]
All skin disorders in Ayurveda are placed under the name of Kushtha. In Ayurveda, Shvitra is considered as one of the varieties of Kushtha,[3] that can be correlated with vitiligo based on the similarities of signs and symptoms. It is caused due to vitiation of Tridosha and Dhatus like Rasa (lymph), Rakta (blood), Mamsa (muscles) and Meda (fats).[4] According to Harita Samhita, vitiated Vata along with Pitta affects the Rakta Dhatu manifests Pandura Varna (whitish patches) on skin that is called as Shvitra.[5] Depending upon chronicity and involvement of deeper tissue (Dhatus), disease becomes difficult to treat.
A number of topical formulations are mentioned for management of Shvitra. Modern science uses Psoralen + Ultra Violet-A exposure therapy and corticosteroids in the treatment of vitiligo. But they are associated with side effects like burning, itching, nausea, tanning, eye damage, skin aging and skin cancer.[6] Hence, there is a need to develop an effective formulation with less adverse effects. Ayurveda has ample of formulations that can be used safely in Shvitra. Apamarga Kshara Yoga[7] is one of such formulations. In the current study, it is planned to evaluate clinical efficacy of Apamarga Kshara Yoga in two different dosage forms i.e. Lepa and ointment.
Materials and Methods
The study is a randomized single blind one involving 50 patients with vitiligo fulfilling the inclusion criteria. Each patient was examined in detail. Relevant pathological and biochemical investigations were done before and after treatment and informed consent was taken from all the patients before including into the trial [Chart 1]. The study was started after obtaining permission from Institutional Ethics Committee (PGT/7-A/2012-2013/1964/23 dated 21/09/2012) and was registered in Clinical Trial Registry of India (CTRI/2012/11/003157 dated 30/11/2012).
Chart 1.
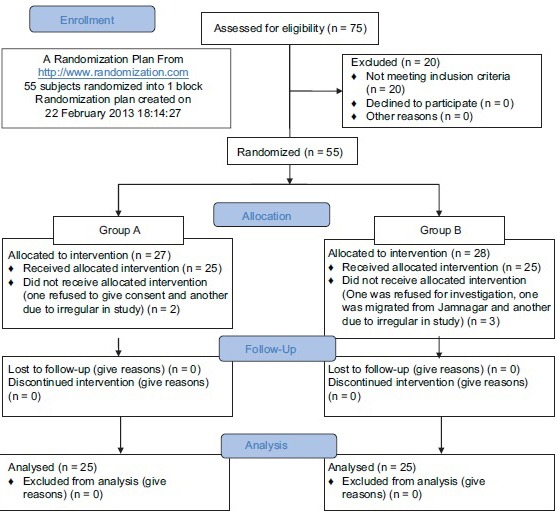
Consort flow diagram
Inclusion criteria
Patients having signs and symptoms of Shvitra (vitiligo)
Patients having age between 16 and 60 years
Patients with chronicity of <10 years
Lesions with positive wood's lamp test.
Exclusion criteria
Chronicity more than 10 years
Patients suffering with chronic cardiac, renal, hepatic ailments, insulin-dependent diabetes mellitus (IDDM), non-IDDM and other serious systemic illness
Patches due to burning, chemical explosion,
Gravid and lactating women
Lesions at Guhyanga (genital organ), Panipadatala (palms and soles), Oshtha (lips), Ekanga (involving an entire organ), Sarvanga (generalized lesions)[8]
Patches with Raktaroma (reddish hair) and Samsakta (coalescent).[9]
Grouping and posology
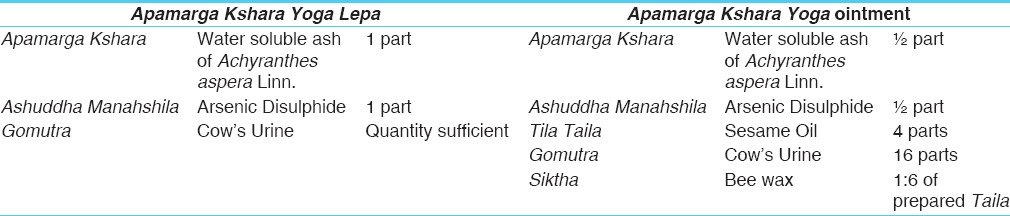
Registered patients were grouped into two by using computer generated randomization plan.[10] Patients of Group A were treated with Apamarga Kshara Yoga Lepa,[7] while patients of Group B were treated with Apamarga Kshara Yoga Ointment[11] [Table 1]. Patients in both the groups were advised to apply quantity sufficient drug locally on patches in the morning followed by 5–10 min. exposure to sunlight in the morning (before 9 AM) for 8 weeks. Besides, 3 g of Rasayana Churna[12] along with Madhu and Ghrita was given twice a day as internal medication in both the groups. Patients were advised dietary restrictions during the treatment period.
Table 1.
Formulation composition of both dosage forms
Criteria for assessment
Scoring pattern was adopted for scrutinizing the symptomatology. The score was given on the basis of Size, Color and Number of patches, Percentage of body area involvement and chronicity of patches [Table 2]. For the assessment of involvement of body surface area, rule of nine was used to calculate the percentage of lesions with certain modifications. Whole body was scored but looking into the nature of the disease; score was further specified to the organs. Total score was obtained from calculation of Table 2. Maximum score was 25. Then obtained score was divided into mild, moderate and severe category.
Table 2.
Criteria for assessment

Severity of disease

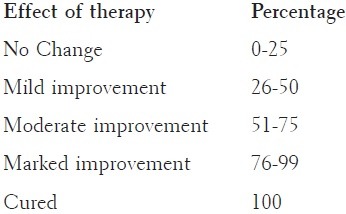
Criteria for assessment of total effect
Observations
Of the registered patients, 26 were in the age group of 16–30 years with chronicity of 1–2 years. Majority of the registered patients (30) were males, 11 had positive family history. Totally, 44 patients had white colored patches while 5 patients had red to white and only one patient had red colored patch. A total of 30 patients had number of patches more than 4; while 12 patients had 4 patches, 2 and 3 patches were found in 6 patients each while only one patient had a single patch. Totally, 12 patients had more than 4 cm size of patches, 4 patients had 4 cm, while 3 patients had 3 cm size of patches, 9 patients had 2 cm and only 2 patients had 1 cm size of patches. Vata-Kaphaja Prakriti was predominant in the majority of the patients. Hematological and biochemical investigations after the treatment were within normal limits.
Results
Effect of therapy shows that in Group A, 57.26% reduction was found in color of patches, in number of patches 43.80% reduction was found while in percentage area of patches 40.58% reduction was found and 42.42% reduction was found in size of patches [Figures 1 and 2]. All these changes were statistically highly significant (P < 0.001) [Table 3].
Figure 1.
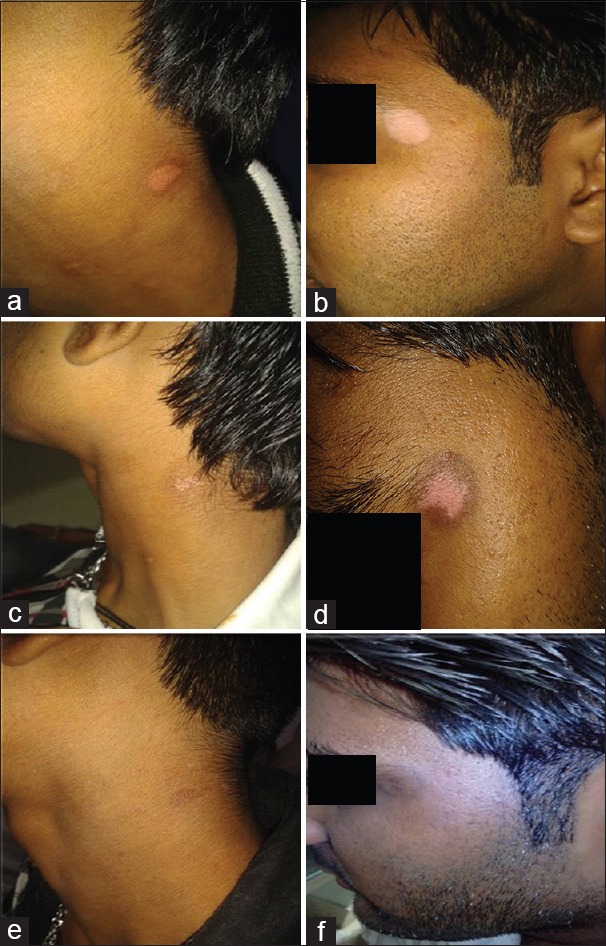
Before treatment (BT) and after treatment (AT) of both Groups; (a) Group B – BT, (b) Group A – BT, (c) Group B – during treatment, (d) Group A – during treatment, (e) Group B – AT, (f) Group A – AT
Figure 2.
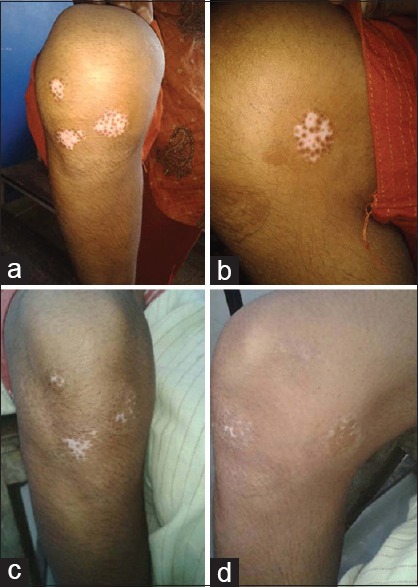
Before treatment (BT) and after treatment (AT) of both Groups (a) Group A – BT, (b) Group A – BT, (c) Group A – AT, (d) Group A – AT
Table 3.
Effect of therapy of patches on Group A (n=25)

In Group B, 55.46% reduction was found in color of patches and 40.42% in number of patches was found. In area of patches 35.53% reduction and 42.45% reduction was found in size of patches that all changes were statistically highly significant (P < 0.001) [Table 4 and Figure 1].
Table 4.
Effect of therapy on Group B (n=25)

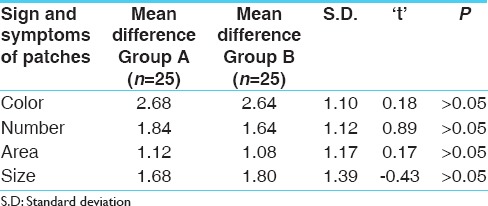
In comparison of both groups, statistically insignificant difference (P < 0.05) was found in the effect of therapies on size, color, number of patches and area of body. Based on this, it can be said that both the dosage forms have similar effect on Shvitra (Vitiligo) [Table 5].
Table 5.
Comparative effect of therapies on chief complaints
Discussion
Incompatible diet is emphasized to be an important etiological factor in manifestation of Shvitra. Charaka also stated that Papakarma (Sinful acts), Guruninda (Insult of the preceptors)[13] Such psychological factors may induce stress in the patients and become Vyanjaka Hetu (triggering factor) that triggers disease manifestation mechanism. Sudden emotional trauma and depression have been noted to be responsible for sudden onset or rapid spread of lesion.[14]
In the present study, 47.27% of patients are from the age group of 16–30 years. Though, there is no significance of age with Shvitra, but, younger age individuals are more prone to psychological stress and consumption of Virudhdha Ahara. According to modern science, it may appear at any age.[15] As Shvitra is Pittapradhana Tridoshaja Vyadhi, hence, may be prevalent in the age group of 16-30 years, which is Pittapradhana.[5] 54.55% of patients were males and 45.45% of patients were females. Gender has no role in manifestation of disease.[15] It is observed that, 80% patients were having negative family history while remaining 20% were having positive family history. It has been mentioned that hereditary diseases (Sahaja Vyadhi) are difficult to cure. Modern science says that the occurrence of vitiligo is in ratio of 1:3 when it comes to inheritance.[15]
Apamarga Kshara Yoga has Apamarga Kshara, Ashuddha Manahshila and Gomutra as ingredients. Ksharas have qualities like Ushna (hot), Tikshna (irritant), Pachana (digestive), Vilayana (corrosive), Shodhana (purification), Ropana (closure of wound), Shoshana (absorbing), Sthambhana (restrain), and Lekhana (scarificant) etc.[16] Apamarga Kshara has Tikshna Guna[17] so it can remove Kleda, Ama and Kapha and also can clear Srotodushti especially Sanga. Manahshila has Katu (pungent), Tikta Rasa (bitter taste), Ushna Virya and Singdha (unctuous), Guru Guna (heaviness), Vata-Kapha Shamana Karma and also has Rasayana and Varnya Karma.[18] It acts on Bhrajaka Pitta and helps in restoring normal color of skin. So, may be helpful in vitiligo. Hematological and biochemical parameters of both groups were not affected with the treatment.
Both trial drugs have shown highly significant results in symptoms of Shvitra. Comparison in between the groups is statistically insignificant. As complete remission was not found; the duration was increased to 4–6 months in few cases, where the patients were responded significantly. This infers that, there is a need to increase the study period.
Conclusion
Both the trial drugs provided significant results against size, color and number of patches. The difference in between the groups is statistically insignificant. Considering the encouraging results, it can be said that both the drugs can be successfully used in cases of Shvitra. However, the observations can be revalidated through well-designed clinical trials involving larger sample size. Experiments also can be made to identify responsible factors of the efficacy.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
IPGT and RA, Gujarat Ayurved University, Jamnagar.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Lerner AB. Vitiligo. J Invest Dermatol. 1959;32:285–310. [PubMed] [Google Scholar]
- 2.Shajil EM, Agarwal D, Vagadia K, Marfatia YS, Begum R. Vitiligo: Clinical profiles in Vadodara, Gujrat. Indian J Dermatol. 2006;51:100–4. [Google Scholar]
- 3.Acharya JT, editor. Ch. 7, Ver 178 Reprint. Varanasi: Chaukhamba Surbharti Prakashan; 2005. Charak Samhita of Agnivesha, Chikitsa Sthana; p. 459. [Google Scholar]
- 4.Acharya JT, editor. , Ch.7, Ver. 173-74 Reprint. Varanasi: Chaukhamba Surbharti Prakashan; 2005. Charak Samhita of Agnivesha, Chikitsa Sthana; p. 458. [Google Scholar]
- 5.Tripathi H, editor. Ch.39, Ver 50 Reprint. Varanasi: Chaukhambha Krushnadas Academy; 2009. Harita Samhita of Harita, Tritiya Sthana; p. 421. [Google Scholar]
- 6.dermnetnz.org. New Zealand Trust: Facts about the skin from DermNet. [Created on 1997; Last modified 29 Dec 2013, © 2014]. Available from: http://www.dermnetnz.org/procedures/puva.html .
- 7.Shastri H, editor. 1st ed. Ch.14, Ver. 71. Delhi: Motilal Banarasidas; 1986. Rasa Tarangini of Sadananda Sharma; p. 339. [Google Scholar]
- 8.Tripathi B, editor. Ch.14, Ver. 41. Reprint ed. Delhi: Chaukhamba Sanskrit Pratishthan; 2009. Asthanga Hridaya of Vagbhata, Nidana Sthana; p. 533. [Google Scholar]
- 9.Tripathi B, editor. Ch.7, Ver. 175. Vol. 2. Varanasi: Chaukhamba Surbharti Prakashan; 2009. Charak Samhita of Agnivesha, Chikitsa Sthana; p. 334. Reprint ed. [Google Scholar]
- 10. [22 February 2013 18:14:27]. www.randomization.com . Homepage on the Internet. Available from: http://www.randomization.com .
- 11.Jadav HR, Galib, Prajapati PK. Pharmaceutical standardisation of Apamarga Kshara Yoga. Journal of Drug Delivery and Therapeutics. 2015;5(6):31–34. [Google Scholar]
- 12.Tripathi I, Tripathi S, editors. Ch.39, Ver. 160 Reprint ed. Varanasi: Krishnadas Acadamy; 1994. Astanga Hridaya of Vagbhata, Uttara Sthana; p. 637. [Google Scholar]
- 13.Acharya JT, editor. Ch.7, Ver. 177 Reprint ed. Varanasi: Chaukhamba Surbharti Prakashan; 2005. Charaka Samhita of Agnivesha, Chikitsa Sthana; p. 458. [Google Scholar]
- 14.Valia RG. 1st ed. Ch 22. Vol. 1. Bombay: Bhalani Publishing House; 1994. Text Book and Atlas of Dermatology; pp. 518–9. [Google Scholar]
- 15.Lotti T, Hercogova J, editors. 1st ed. New York: Marcel Dekker, Inc; 2004. Vitiligo – Problems and Solutions; p. 3. [Google Scholar]
- 16.Shastri AD, editor. Ch.11, Ver. 5. Vol. 1. Varanasi: Chaukhambha Sanskrit Sansthan; 2010. Sushruta Samhita of Sushruta, Sutra Sthana; p. 45. Reprint ed. [Google Scholar]
- 17.Shastri H, editor. 1st ed. Ch.14, Ver. 66. Delhi: Motilal Banarasi Das; 1986. Rasa Tarangini of Sadanand Sharma; p. 336. [Google Scholar]
- 18.Shastri H, editor. 1st ed. Ch.11, Ver. 115-116. Delhi: Motilal Banarasi Das; 1986. Rasa Tarangini of Sadanand Sharma; p. 263. [Google Scholar]