

Abstract
Introduction:
Cissus quadrangularis Linn. is an indigenous medicinal plant, grown in India, which helps to increase healing process of fractured bone. Fracture of maxillofacial skeletal takes reasonably long time to heal. Many attempts have been made till today to reduce the healing period of 6–8 weeks, by means of improved surgical technology or by inhibiting the physiological mechanism of bone healing.
Aim:
To evaluate the effect of C. quadrangularis in healing process of maxillofacial fracture.
Materials and Methods:
All the patients were treated by open reduction internal fixation method and in postoperative management, antibiotics, and analgesics. Patients were divided into two groups. In Group 1, one capsule of C. quadrangularis (500 mg) thrice a day for 6 weeks was administered (n = 5), and in Group 2 (control group), no supplementary medication was administered (n = 4). Pain, swelling, fragment mobility, serum calcium, and serum phosphorus were evaluated pre- and post-operatively on day-1, -21, and -45.
Results:
Pain, swelling, and fragment mobility were low in Group 1 compared to Group 2. Serum calcium and serum phosphorus were also high, and healing of bone was clearly seen in Group 1 on day 21 as compared to control group.
Conclusion:
C. quadrangularis helps in reducing pain, swelling, and fracture mobility and accelerate the healing of fracture jaw bones.
Keywords: Asthisanghata, Cissus quadrangularis, Hadjod, osteogenic agent
Introduction
Ayurveda, the ancient science of medicine describes different types of herbal preparations that achieve the hastening of bone healing.[1] In Ayurveda, most of the names of the plants have been given according to their medicinal values.[2] The plant is known as Harishankar or Hadjod in Hindi and Asthisanghata, Kandavalli, Vajrangi, etc., in Sanskrit. Hadjod means that which joins the bones.[2,3]
Cissus quadrangularis Linn. (Hadjod) is an indigenous medicinal plant grown in India, Sri Lanka, and Africa. It has been prescribed in ancient Ayurveda texts by Bhava Prakasha and Chakra Dutta as a general tonic, especially for the fractured patient. Since then, it has been used as an external application and as an internal medication by bonesetters.[1,2,3]
C. quadrangularis is a shrub, which has slender, fleshy fibrous, smooth stem, with four winged internodes. Stem and root portion of this plant possess antioxidant and antimicrobial activity. C. quadrangularis contains high amount of anabolic steroidal substances, calcium, and phosphorus.[2,3] The extracts from stem of this plant have been used widely for the early repair of fractures, gout, back pain, and irregular menstruation since ancient time. The steroidal substances from C. quadrangularis have shown marked influence on the rate of fracture-healing and quicker mineralization of the callus.[4] C. quadrangularis comes in the form of capsule, tablet, and syrup. The daily adult dose requires 1000–1500 mg.
The maxillofacial fractures take at least 12–16 weeks to heal. This period reduced by means of improved surgical techniques due to recent advances in internal fixation or by inhibiting the physiological mechanism of bone healing.[5] C. quadrangularis contains high amount of Vitamin C, Vitamin A, anabolic steroidal substances, and calcium. The steroidal substances from the C. quadrangularis showed marked influence on early regeneration of all connective tissue of mesenchymal origin, and thereby, improve the bone healing.[2]
The aim of the present study was to evaluate the effect of C. quadrangularis in accelerating healing of facial fracture by reducing postoperative complication such as pain, swelling, and mobility.
Materials and Methods
Nine patients, 8 male and 1 female, age from 20 to 63 years, with maxillofacial fracture, reported to the Oral and Maxillofacial Department, Sangam Multispeciality Hospital, Vadodara were included in the study. Hospital ethical committee approved the study (ref no. B-27/433), and informed consent was obtained from all patients.
Inclusion criteria
Patients with mandibular and maxillary fractures.
Exclusion criteria
Patients on steroid therapy or immune-suppressants and suffering from any other chronic debilitating diseases, fracture with severe head injury, bone loss, and infected fracture were excluded.
Grouping and posology
The patients were divided into two groups, a test group and a control group. The control group consisted of four patients, in whom no supplemental drugs were administered. Five patients were included in the test group for whom 500 mg of C. quadrangularis[2] capsule (manufactured by Aeran India Private Limited, Maharashtra, India, and marketed as Capsule Union Date of MFG: August 2012) thrice a day for 6 weeks was prescribed. The capsules of Cissus were free from any pesticides, chemicals, and heavy metals. These capsules were freshly powdered; whole herb part dried to low moisture content of 6–7% and then slowly grinded with grinders at low temperature.[6]
All the patients were treated by open reduction internal fixation under general anesthesia or local anesthesia with miniplates. Immediate postoperative for 3 days same drugs such as antibiotics (combination of injection amoxicillin, with clavulanic acid combination 625 mg intravenous [IV]) and analgesics (injection Dynapar AQ 75 mg IV) were given. After that, patients were shifted to oral antibiotic, with tablet amoxicillin with clavulanic acid 625 mg and combination of tablet diclofenac sodium (50 mg) with paracetamol (500 mg) for next 5 days.
Criteria for assessment
Pain, swelling, fragment mobility, serum calcium, and serum phosphorus were recorded pre- and post-operative.
The pain was graded as mild, moderate, and severe based upon the patient's response to visual analogue scale, wherein the subjective assessment of intensity or magnitude of pain felt by patient was recorded. Scale consists of a straight line of 10 cm in length, signifying 0 - no pain, and 10 - severe pain [Figure 1]. Swelling was measured by the placement of thread from anterior to posterior limit of swelling. Posterior border of ramus, tragus of ear, lateral canthus of eye, corner of mouth, and alas of nose included for the measurement of swelling. Investigator checked fracture mobility manually. Preoperative serum calcium and serum phosphorus levels, as well as two-dimensional computed tomographic scan (2D-CT), were recorded. All the patients had come for follow-up and calcium and phosphorus test on day of 1st, 21st, and 45th day of postoperative days, as well as 2D-CT radiograph, had been taken on 21st and 45th days.
Figure 1.
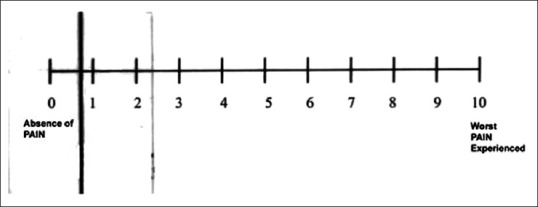
Visual analog scale for pain
Results
Pain and swelling gradually reduced in C. quadrangularis group and was completely absent after 15 days [Table 1] as compare to control group [Table 2]. The mobility was completely absent in Cissus group, but there was slight mobility present in the control group, but it is not so significant (P > 0.001). Serum calcium and phosphorus levels were high or at the adequate level that will help in healing, but in control group, they were at low levels. Apart from the clinical and blood investigation, osteogenesis was evaluated with 2D-CT for all patients. After treatment, there was early periosteum reaction and bridging between the fractures ends at the site of mandibular fracture on the 21st day and complete deposition of bone fragment on 45th day [Figure 2a–c]. As compare to control group, no clinical evidence of bridging between the bony fragment on the 21st postoperative day and minimum bridging at site of fracture on day of the 45th day [Figure 3a–c].
Table 1.
Analysis of clinical variables at different follow-up in Group 1 (n=5)
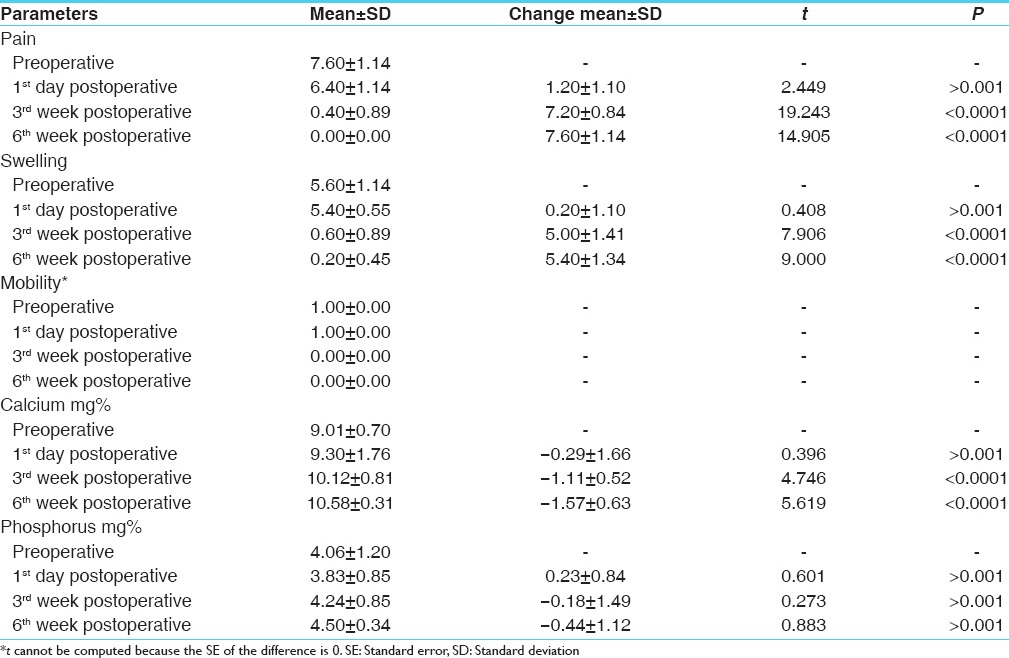
Table 2.
Analysis of clinical variables at different follow-up in Group 2 (n=4)
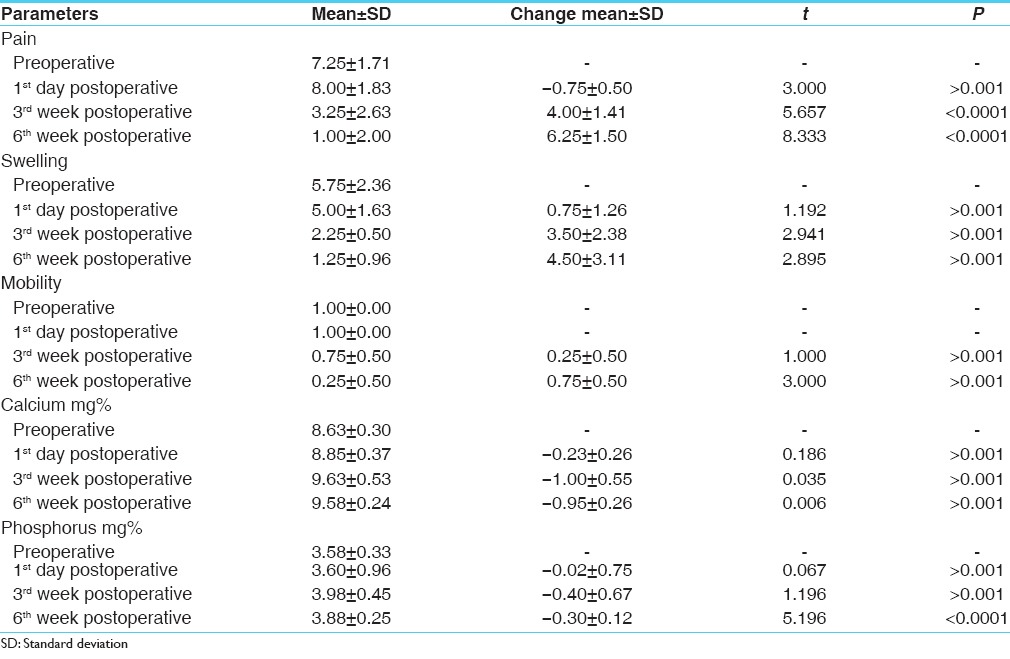
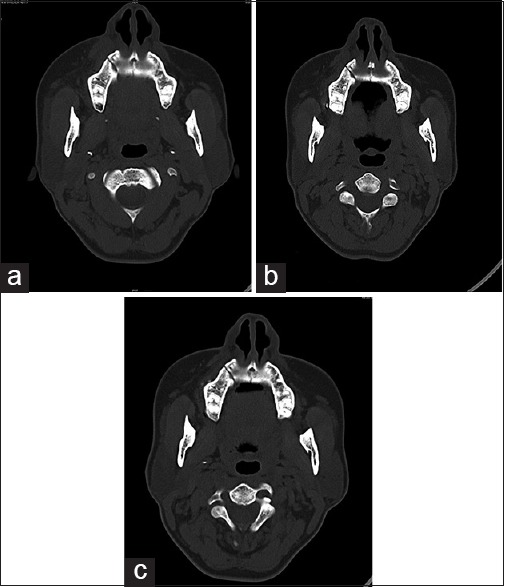
Figure 2.
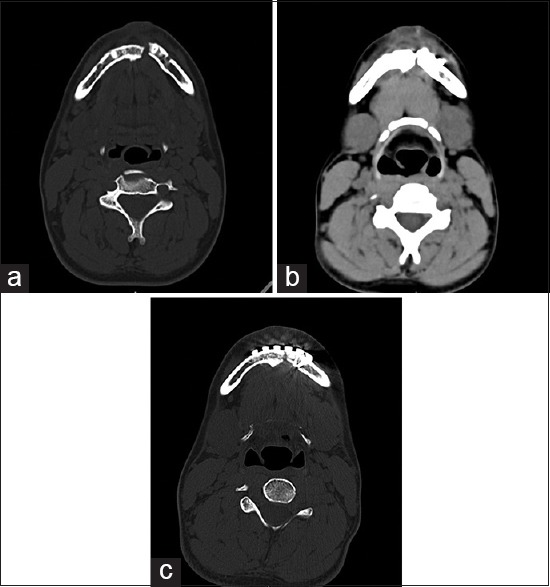
(a) Preoperative malunited of fracture site. (b) After 21 days, bone formation in other site of computed tomography in fracture line. (c) After 45 days, even in malunited fracture well-defined bone formation in between the fracture bone
Figure 3.
(a) Preoperative X-ray shows fracture in right maxilla. (b) After 21 days, there is no evidence of bone formation seen on the radiographs. (c) After 45 days, evidence of very little callus formation on the bone fracture site
Discussion
Nutrition supply is an important factor for bone healing. Calcium is one of the substances, which helps in healing of bone, but only increased intake of calcium does not improve the rate of new bone formation. The ability for absorption and utilization of calcium should be increased for the hastening of healing. C. quadrangularis acts by the stimulation of metabolism and increased uptake of the minerals calcium, sulfur, and strontium by the osteoblasts in fracture healing. Certain amino acids such as lysine help in absorption of calcium. Cissus also contains Vitamin A and C that is effective in the formation of collagen.[2,4,7]
The pharmacological properties of C. quadrangularis are antioxidant, free radical scavenging potential, antibacterial activity, antiosteoporosis activity, antitumor activity, antiulcer activity, analgesic activity, antiobesity activity, antipyretic activity, and bone fracture healing activity.[2,3,8]
In clinical trials, based on radiological and clinical observations, it was found that C. quadrangularis will cause considerable reduction in the healing time of fractures.[5] Radiologically one of study suggested an early callus formation as well as clinical pain, tenderness, and swelling were significantly absent in Cissus group.[4] It was observed that C. quadrangularis neutralizes the antianabolic effect of steroids such as cortisone in healing of fractures. Inhibition of tissue regeneration and repair and retarding formation of the specific skeletal are antianabolic effects of cortisone. This will stimulate the cells of mesenchymal origin, namely the fibroblasts, the chondroblasts, and the osteoblasts by C. quadrangularis. These cells have greater impact on osteoblastic proliferation than other cellular responses.[2,4,9]
It causes less amount of tissue reaction in the fractured region, which leads to optimum decalcification in the early stage with minimum of callus formation. Therefore, deposition of calcium is just enough to join two broken segments of bone, and that is why its remodeling takes much less time.[10] Cissus is also shown to cause early gain in the tensile strength of fractured bones of its normal strength at the end of 6 weeks.[11] C. quadrangularis builds up the skeletal of the fractured bone, namely its mucopolysaccharides, collagen, phosphorus, calcium, and others. Mucopolysaccharides supplies raw materials for repair. Rapid the utilization of these raw materials earlier will be completion of healing process. C. quadrangularis not only causes the greater accumulation of mucopolysaccharides but also an early disappearance of mucopolysaccharides from the fractured area, associated with the earlier calcification and firm callus formation.[2,3,11]
In this study, radiograph of the Cissus group shows the early callus formation and complete new bone formation at the 7–8 weeks. Various studies have mentioned that C. quadrangularis reduces the usual fracture healing time from 14–16 to 8–10 weeks.[5,8,11] We also noted early reduction in pain and swelling with decreased mobility at fracture site, which could be attributed to increased serum calcium and serum phosphorus levels because of administration of C. quadrangularis in test (Cissus) Group.
Conclusion
C. quadrangularis has drawn much attention now-a-days for its medicinal uses because of its efficacy and safety for human use. It does not produce any toxic effects when used orally and due to its various inherent pharmacognostic properties, C. quadrangularis is recommended as a supplementary drug to aid in healing of fractures.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Sanyal A, Ahmad A, Sastry M. Calcite growth in Cissus quadrangularis plant extract, a traditional Indian bone healing aid. Curr Sci. 2005;89:1742–5. [Google Scholar]
- 2.Justin SR, Baby J. Pharmacognostic and traditional properties of Cissus quadrangularis Linn – An overview. Int J Pharm Bio Sci. 2011;2:131–9. [Google Scholar]
- 3.Nayar M. Pharmalogical study of the stem of Cissus quadrangularis Linn. J Sci Ind Res. 1959;18:253. [Google Scholar]
- 4.Deka DK, Lahon LC, Saikia J, Mukit A. Effect of Cissus quandriagularis in accelerating healing process of experimentally fractured radius-ulna of dog: A preliminary study. Indian J Pharmacol. 1994;26:44–5. [Google Scholar]
- 5.Singh V, Singh N, Pal US, Dhasmana S, Mohammad S, Singh N. Clinical evaluation of Cissus quadrangularis and Moringa oleifera and osteoseal as osteogenic agents in mandibular fracture. Natl J Maxillofac Surg. 2011;2:132–6. doi: 10.4103/0975-5950.94466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Srivastava GM, Saurabh S, Nagori BP. Pharmacological and therapeutic activity of Cissus quadrangularis: An overview. Int J PharmTech Res. 2010;2:1298–310. [Google Scholar]
- 7.Kalfas IH. Principles of bone healing. Neurosurg Focus. 2001;10:E1. doi: 10.3171/foc.2001.10.4.2. [DOI] [PubMed] [Google Scholar]
- 8.Udupa KN, Prasad G. Biomechanical and calcium-45 studies on the effect of Cissus quadrangularis in fracture repair. Indian J Med Res. 1964;52:480–7. [PubMed] [Google Scholar]
- 9.Jain A, Dixit J, Prakash D. Modulatory effects of Cissus quadrangularis on periodontal regeneration by bovine-derived hydroxyapatite in intrabony defects: Exploratory clinical trial. J Int Acad Periodontol. 2008;10:59–65. [PubMed] [Google Scholar]
- 10.Teware K, Singh P, Mehta R. In vitro callus induction from stem explants of Cissus quadrangularis L. (Hadjod) Int J Ayurvedic Herb Med. 2012;2:135–8. [Google Scholar]
- 11.Mohammad S, Pal US, Pradhan R, Singh N. Herbal remedies for mandibular fracture healing. Natl J Maxillofac Surg. 2014;5:35–8. doi: 10.4103/0975-5950.140167. [DOI] [PMC free article] [PubMed] [Google Scholar]