

Abstract
Objective:
The aim of this study was to evaluate the mean rotation of the upper first molar (U1st M) in cast models from nontreated patients presenting: Class I, skeletal Class II, dental Class II, and skeletal Class III, comparing with Class I orthodontically treated patients.
Materials and Methods:
One hundred cast models were evaluated with five groups, composed of nontreated Class I (n = 20), dental Class II (n = 20), skeletal Class II (n = 20), skeletal Class III (n = 20), and treated Class I (n = 20). Measurements were taken from photocopies of the upper arches. The angle formed between a line crossing the mesiopalatal and the distal-buccalcusps of the U1st M and a line traced on mid palatal junction were measured in all samples.
Results:
One-way variance analysis showed that dental Class II group presented great mean rotation of the 1st molar (x = 78.95°, SD = 6.19) (P < 0.05), and in 85% of the patients from this group this angle was higher than 73°.
Conclusions:
The skeletal Class II and skeletal Class III groups showed similar mean position of the 1st molar, presenting rotation in approximately 50% of the patients. It can be concluded that upper molar rotation occurs mainly in dental Class II patients and shows higher mesial rotation angle.
Keywords: Angle Class II, malocclusion, molar, rotation
INTRODUCTION
Correct positioning of the upper first molar (U1st M) on the arch and its proper relationship to the opposing arch is one of the foundations of successful orthodontic treatment.[1,2,3,4] The rotation of the U1st M can mean a greater need for space in the arch, due to its trapezoidal shape. As a result, failure in interarch engagement may occur.[5]
It is reported that mesio-palatal rotation of the U1st M is present in about 95% of patients with angle Class II, division 1 malocclusion, and in 83% of them as a whole.[6,7]
Some authors[5,8,9,10] reported the frequent need to correct the rotation of U1st M in order to obtain space in the arch and a correct intercuspal engagement. In addition, McDonald et al.[11] observed that in patients with Class II, who used the headgear, there was great influence in rotation correction of the molars associated with distalization. They found that on average, for each 3 mm of distal movement, there is a contribution of 1 mm regarding the correction in the rotation of the molar (average equivalent to 10°).
Given the importance of diagnosing and quantifying molar rotation, this study investigated the average rotation of the U1st M in patients with Class I, II and III, showing patterns of facial profiles I (dental Class I and dental Class II), II (skeletal Class II) and III (skeletal Class III).
MATERIALS AND METHODS
This study was previously approved by the Ethics Committee on Human Research (CEP: 301916-09, CAAE: 0128.0.214.000-09).
This is an analytical observational study of photocopies of plaster models in order to evaluate the rotation of the U1st M in cases of Class I, II, and III malocclusion, with facial patterns I (dental Class I and dental Class II), II (skeletal Class II) or III (skeletal Class III).[12] The sample was selected from the documentation Collection of the Dental Press Educational Center (CEDP) in Maringa, PR, Brazil.
We included 100 patients divided into 5 groups of 20 patients in each: (1) Group Class I, facial pattern I; (2) Group Class II, facial pattern I– that was dental Class II, (3) Group Class II, facial pattern II– that is Skeletal Class II; (4) Group Class III, facial Pattern III; and (5) a treated group Class I, facial pattern I.
The cases were selected consecutively until they reached 20 individuals for each group, according to the CEDP file order for the years 2000–2005 respecting the following inclusion criteria: Presence of the four first molars; 1st upper molar in occlusion and in good condition (cusps without excessive wear and without prosthetic reconstruction); and absence of posterior cross bite. All cases were separated by evaluating profile pictures of respective records.
The average age of patients in skeletal Class II group was 13 years and 2 months; 8 of them were male and 13 female. The group of dental Class II had an average age of 17.2, with 14 males and 9 females. Class III group had mean age of 15 years and 7 months, 10 of them were male and 10 female. Those in the Class I group were 15 years old, and 18 of them were female and 7 male. The patients who had been treated were 20, and the sample was composed of 17 women and 3 men.
All selected patient's upper impressions were photocopied (XEROX/Konica Minoltabiz hub 210, Norwalk, CT/United States), with the mesio-palatal cusps and distobuccal of first upper molars carefully marked with pencil graphite 0.5 mm.
On the photocopies, measurements were taken for the angles formed by the intersection of lines going over the tips of the mesio-palatal and distobuccal cusps of each molar (Ricketts line)[13] with a straight line marked over the palatine raphe, as shown in Figure 1. The reference trace was done with graphite pencil 0.5 mm, on the copies.
Figure 1.
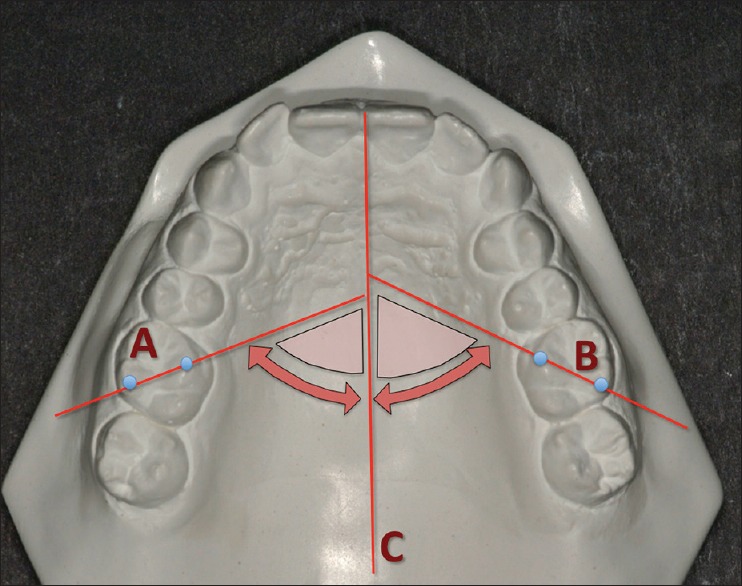
(A and C) Reference Lines drawn on the photocopied model for the angles related to upper first right and left molars; (C) median raphe line. The marked regions illustrate the locations for reading both sides
The angle between those two straight lines was measured with a protractor (Trident/Desetec, Itapui, SP/Brazil), with 0.5° as assigned values for the intermediate readings. The marks and measurements were done by a previously trained examinator.
In order to assess the accuracy of the copies for this purpose, we randomly selected 20 plaster models from the sample. A 2 mm glass plate was placed on these models up on which the angle of interest was reproduced and measured. The values obtained were compared directly with those made on the photocopies. The t-paired test revealed no statistically significant difference between measurements (P < 0.05).
The readings on the photocopies were repeated after an interval of 1 week to test the reproducibility and random error, using the intraclass correlation coefficient and Dalberg's formula, respectively.
RESULTS
The intraclass correlation test showed excellent reproducibility between the repeated measurements (0.91) and Dalberg error was 0.45.
The rotations of the upper right and left molars were not statistically different in any of the groups (P < 0.05), so the means of the left and right angles were used for comparisons between groups.
When comparing the groups [Table 1], there was a different behavior observed for the molars.
Table 1.
Individual values, means, and standard deviations of the molar angulation in each studied groups, compared by one-way analysis of variance
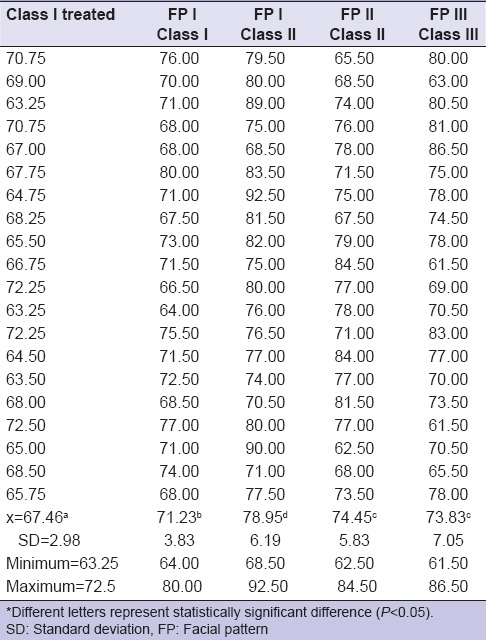
The average angle between the Ricketts line[13] and the median raphe for the treated group was 67.46° (SD = 2.98°) ranging from a minimum of 63.25° to a maximum of 72.5° [Table 1].
The rotation mean for the Class I group was 71.23° (SD = 3.83°) ranging from a minimum of 64° up to 80° [Table 1].
For the dental Class II group, it was 78.95° (SD = 6.19°), ranging from a minimum of 68.5° to a maximum of 90° [Table 1].
For groups with skeletal discrepancies, skeletal Cl II and Skeletal Cl III, respectively, had an average rotation of 74.45° (SD 5.83°) and 73.83° (SD 7.05°). Considering that the above values 73° reflect rotation of the molars (based on the treated group) the percentages of the cases with molar rotation are presented by group in Table 2.
Table 2.
Absolute distribution and percentage of cases with molar rotation by groups

DISCUSSION
In 1972 Andrews reported that in order to achieve the six keys for the normal occlusion there should be no dental rotation.[2] In a routine treatment of any malocclusion it can be advisable to correct the rotation of the U1st Ms with a palatal bar, for example, before the alignment and leveling phase with a preadjusted fixed appliance. A leveling wire positioned without prior correction of the molars can promote buccal inclination of the upper second molars and palatal movement of the upper second premolars causing premature contacts in addition to jiggling [Figure 2].[14]
Figure 2.
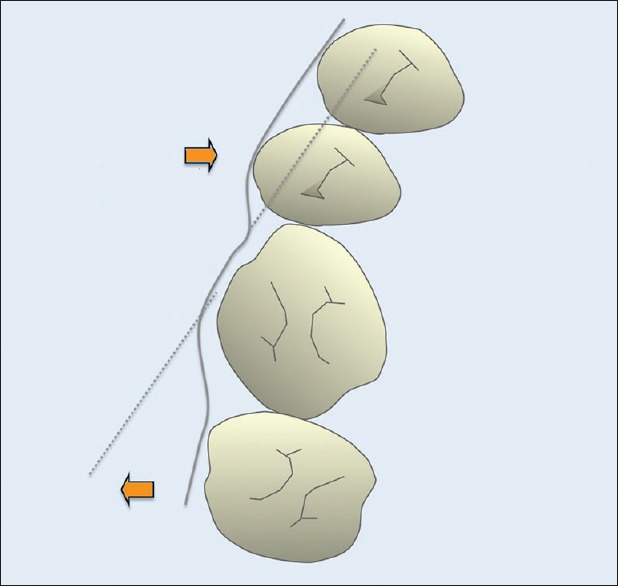
Schematic drawing of the unwanted effect of arch leveling with pre adjusted appliance, without previous correction of rotation of the molars
Considering that, with the correction of the rotation of the molars one can gain space in the arch,[6,8,15] it can be said that especially in dental Class II (Division II Class II) using a palatal bar for example, may assist in space adjustment.
The incidence of mesio-palatal rotation for the U1st M in this study agrees with the results obtained by Henry[6] who had reported this finding in 83% of malocclusions, which is also supported by the study of Lamons and Holmes,[7] who found a frequency of up to 95% of mesio-palatal rotation in Class II patients. These results are very close to the data obtained in this study [Table 2].
When rotation measurements were compared between the groups, there were statistically significant differences between them, highlighting the highest values for the dental Class II (78.95°) (P < 0.05), followed by skeletal Class II (74.45°) and skeletal Class III (73.83°) with no statistical difference, and Class I (71.23°) and treated individuals (67.46°) [Table 1]. However, if we consider the value of 73° as an acceptable value for the position of the first molar, the two groups with skeletal error (skeletal II and III) don’t have a clinically significant expression in behavior, both with regards to intensity as well as frequency of rotation [Tables 1 and 2]. As for tolerance for some rotations of the molars, the literature also reports that Ricketts[13] reference line can be very strict for this evaluation. Dahlquist et al.[16] observed that the molars can have ideal occlusion with this line going through the distal of the opposite canine, or even more, through the mesial of first premolars. In millimeters, on average, they observed 11 mm per distal from the cusp of the canines. However, the patients were studied during the mixed dentition stage.[16]
This value of 73°, as a limit of what is considered an acceptable normal, derives from the minimum value observed in the Class I group treated. This means that with a slight degree of rotation, it is possible to obtain normal occlusion. For this rotation parameter, a more significant and more frequent rotation was evident in the cases of Class II [Tables 1 and 2]. Nery and Barbosa[5] also found a higher prevalence of rotation of the molars (71.4%) in patients with Class II division 1 malocclusion. However, no details were given over the skeletal involvement of the studied Class II sample.
The results illustrate that the Dental Cl II is the one with higher mesial rotation of the molar when compared to Skeletal Cl II. The works which show only the relationship of the molars and do not distinguish the skeletal involvement of malocclusion, probably underestimated the rotation present in the cases of dental Class II only.[5,7,16,17,18] Therefore, in the cases with dental Class II, one may consider a potential space gain in the mesial arch to the first superior molar when it is rotated in the mesio-buccal direction. Molar rotation represents an average situation of ¼ of Class II, in other words around 2 mm.[19] Such a gain in space may mean more conservative procedures in borderline cases.[5] It also seems reasonable to say that Class II with good facial profile (Pattern I sic Capelozza Filho)[12] may require further intervention on the rotation of the molars than those with skeletal involvement (Pattern II).
In this study the average behavior of the molars on both sides was similar, contrary to what was reported by Friel[17] and Dahlquist et al.[16] who found statistically significant difference between the right and left sides with regard to the rotation of the upper molars. Amin[20] found that upper right molar presented more rotation than its contralateral in Class I and II, and more rotation in the upper left molar in Class III. In fact, in some cases in the present study, there were not ably different rotations, however on average the position of the molars was similar on both sides. These results corroborate the data of Lamons and Holmes[7] and Scanavini et al.[19] who also found no statistical difference between the molars on the right and the left. The symmetrical position of the teeth in the arch can facilitate correction and obtain a stable interarch occlusion.[21] Studies have shown great variability in the morphology of the maxillary first molar,[22] thus more studies are needed to identify whether there are greater chances of each specific facial pattern has a more prevalent morphology.
CONCLUSIONS
It was concluded that the Dental Class II group had the highest mean mesio-palatal rotation of the U1st M (78.6°) and more frequency, followed by the skeletal Class II group (74.95°), skeletal Class III group (73.83°), and the Class I group (71.9°).
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Angle EH. Classification of malocclusion. Dent Cosm. 1899;41:248–64. [Google Scholar]
- 2.Andrews LF. The six keys to normal occlusion. Am J Orthod. 1972;62:296–309. doi: 10.1016/s0002-9416(72)90268-0. [DOI] [PubMed] [Google Scholar]
- 3.Nalcaci R, Topcuoglu T, Ozturk F. Comparison of Bolton analysis and tooth size measurements obtained using conventional and three-dimensional orthodontic models. Eur J Dent. 2013;7(Suppl 1):S66–70. doi: 10.4103/1305-7456.119077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Al-Zubair NM. Dental arch asymmetry. Eur J Dent. 2014;8:224–8. doi: 10.4103/1305-7456.130608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nery PC, Barbosa JA. Upper first molar rotation in normal occlusion and Angle's class II division 1. Rev Dent Press Ortod Ortop Facial. 2003;8:101–12. [Google Scholar]
- 6.Henry RG. Relationship of the maxillary first molar normal occlusion and malocclusion. Am J Orthod. 1956;42:288–306. [Google Scholar]
- 7.Lamons FF, Holmes CW. The problem of the rotated maxillary first permanent molar. Am J Orthod. 1961;47:246–72. [Google Scholar]
- 8.Orton HS. An evaluation of five methods of derotating upper molar teeth. Dent Pract. 1966;16:279–86. [PubMed] [Google Scholar]
- 9.Cooke MS, Wreakes G. Molar derotation with a modified palatal arch: An improved technique. Br J Orthod. 1978;5:201–3. doi: 10.1179/bjo.5.4.201. [DOI] [PubMed] [Google Scholar]
- 10.McNamara J., Jr . Integrated treatment of the orthodontic patient-diagnosis, treatment planning and clinical management. Tokyo: Rocky Mountain Morita; 1986. [Google Scholar]
- 11.McDonald JL, Shofer FS, Ghafari J. Effect of molar rotation on arch length. Clin Orthod Res. 2001;4:79–85. doi: 10.1034/j.1600-0544.2001.040204.x. [DOI] [PubMed] [Google Scholar]
- 12.Capelozza Filho L. Diagnosis in Orthodontics. Maringá: Dental Press; 2012. p. 544. [Google Scholar]
- 13.Ricketts RM. Occlusion – The medium of dentistry. J Prosthet Dent. 1969;21:39–60. doi: 10.1016/0022-3913(69)90030-4. [DOI] [PubMed] [Google Scholar]
- 14.Ramos AL, Sakima MT. Mechanics with palatal arch. In: Almeida MR, editor. Ortodontia Cliánica e Biomecânica. 1st ed. Maringá: Dental Press; 2010. pp. 475–99. [Google Scholar]
- 15.Ramos AL, Sakima MT, Santos-Pinto A, Martins LP, Raveli DB. Palatal Arch, Barra palatina. Rev Dent Press Ortod Ortop Facial 2000. Barra palatina. Rev Dent Press Ortod Ortop Facial. 2000;5:75–100. [Google Scholar]
- 16.Dahlquist A, Gebauer U, Ingervall B. The effect of a transpalatal arch for the correction of first molar rotation. Eur J Orthod. 1996;18:257–67. doi: 10.1093/ejo/18.3.257. [DOI] [PubMed] [Google Scholar]
- 17.Friel S. Determination of the angle of rotation of the upper first permanent molar to the median raphe of the palate in different types of malocclusion. Dent Pract. 1959;9:72–8. [Google Scholar]
- 18.Junqueira MH, Valle-Corotti KM, Garib DG, Vieira RB, Ferreira FV. Analysis of the rotational position of the maxillary first permanent molar in normal occlusion and class II, division 1 malocclusion. Dent Press J Orthod. 2011;16:90–8. [Google Scholar]
- 19.Scanavini PE, Jóias RP, Vasconcelos MH, Scanavini MA, Paranhos LR. Assessment of first molars sagittal and rotational position in Class II, division 1 malocclusion. Dental Press J Orthod. 2013;18:106–11. doi: 10.1590/s2176-94512013000600016. [DOI] [PubMed] [Google Scholar]
- 20.Amin F. Assessment of maxillary first molar rotation in skeletal class II, and their comparison with class I and class III subjects. Pak Oral Dent J. 2012;32:430–5. [Google Scholar]
- 21.Quaglio CL, de Freitas KM, de Freitas MR, Janson G, Henriques JF. Stability and relapse of maxillary anterior crowding treatment in class I and class II division 1 malocclusions. Am J Orthod Dentofacial Orthop. 2011;139:768–74. doi: 10.1016/j.ajodo.2009.10.044. [DOI] [PubMed] [Google Scholar]
- 22.Kim HK, Kwon HB, Hyun HK, Jung MH, Han SH, Park YS. Submorphotypes of the maxillary first molar and their effects on alignment and rotation. Am J Orthod Dentofacial Orthop. 2014;146:286–93. doi: 10.1016/j.ajodo.2014.05.029. [DOI] [PubMed] [Google Scholar]