

Abstract
Repeated fluoroscopically guided nasojejunal tube (NJT) insertions, particularly in children, can pose health risks through increased radiation exposure. We analyzed frequency of NJT reinsertions and associated radiation exposure through retrospective evaluation of children <18 years at our institution who underwent fluoroscopically guided NJT insertions from 2007 to 2012. Age and weight, reinsertion frequency per patient, radiation dose (dose actual percentage [DAP]), time interval between, and indication for reinsertion were recorded. A total of 252 children (3 days to17 years, 11 months) had 449 NJT insertions. Reinsertions occurred in 105 (41.7%) patients with 14 (5.6%) having ≥5 reinsertions, and 67.6% of reinsertions occurring in patients <1 year. Mean DAP increased with frequency of reinsertion, along with age and weight. Most common indication for reinsertion was a pulled NJT (34.0%). Fluoroscopic NJT reinsertion was most frequent in younger, smaller patients. Self-guided, bedside NJT insertion, and/or earlier instigation of definitive nutritional therapy delivery should be considered.
Keywords: nasojejunal tube, radiation dose, fluoroscopy, self-guided technique, children
Introduction
Malnutrition affects approximately 40% to 50% of pediatric patients during their hospital stay, which can contribute to compromised immunity and poor muscle function, leading to slower disease recovery and poor postoperative outcome.1,2 To improve clinical outcome, improving nutrition is integral. This is often achieved by enteral feeding over the short-term if oral feeding fails to provide sufficient nutrition for a patient, and prior to implementing measures of permanent feeding access as indicated (eg, gastrostomy).
Implementing enteral nutrition in a patient typically requires the insertion of a feeding tube into the stomach or jejunum using a nasogastric or nasojejunal tube (NJT).3 Common indications for nasojejunal feeding include gastroesophageal reflux disease, feeding intolerance, gastroparesis, pancreatitis, short bowel syndrome, and neurological or psychiatric disorders.3 NJT insertions often use fluoroscopy or endoscopy to facilitate correct tube placement.4,5Although use of enteral tubes may improve clinical outcome, they are not without complications. Enteral tubes can be dislodged during bouts of vomiting, retching, or coughing, particularly in children.5,6 Hwang et al5 reported that 27% of patients who underwent NJT insertions also underwent subsequent tube insertions to correct tube displacements. Another study reported multiple NJT insertions in 60% of patients between 1 and 195 months (N = 43).7 Multiple tube insertions in the same patient can generate serious concern due to cumulative radiation exposure.8 Children are also more sensitive to radiation damage as they are still developing and undergoing cell division. Cancer risk accumulates across one’s lifespan, so radiation exposure at a younger age typically increases an individual’s risk of developing malignancies later in life.9
The purpose of our retrospective study was to assess the number of NJT insertions and repeat insertions in a single patient, demographics, time interval between and reasons for reinsertions, and the associated radiation exposure at our institution, to identify those most at risk and why. This was to determine need for procedural change in NJT insertion, to identify those who have undergone or are at risk for multiple reinsertions, and implement blind bedside insertion and/or earlier transition to definitive management, for example, fundoplication.
Materials and Methods
The study received approval from the institution’s research ethics board, and waiver for informed consent was obtained.
Patients
A retrospective evaluation of all patients <18 years who underwent fluoroscopic-guided NJT insertion between February 2007 and August 2012 at a tertiary-care pediatric hospital was conducted using Picture Archiving and Communication Systems (PACS; General Electric (GE) Healthcare, Barrington, IL) audit. Demographic information including gender, age, and weight at the time of the procedure was collected using PACS and Electronic Patient Chart (EPC; Microdea Inc, Synergize, Explorer 2006.1).
Fluoroscopic Technique and Procedure Details
Standard technique at our institution is for the NJT insertion to be placed by a pediatric-trained radiologist or radiology fellow in a nonsedated patient in supine position, with right lateral decubitus positioning as needed, usually using a weighted tip catheter (of sizes 6-10 French) with guide-wire or stylet in place. Frame rate for all procedures was 7.5 frames/second. Screening is performed with coning, without magnification and using pulsed fluoroscopy (GE HealthCare, GE Precision 500D) while manipulating the catheter tip transpylorically, preferably in the region of the duodenojejunal flexure. Position is usually confirmed via contrast injection through the NJT.
Insertions were considered successful if the tip was at the duodenojejunal flexure (optimal), but a transpyloric position, including in the duodenum or proximal jejunum, was still considered a successful insertion. Insertions were deemed unsuccessful if the tip of the NJT was described as remaining in the stomach at the termination of the procedure, or the patient did not tolerate the procedure and it was discontinued. Both successful and unsuccessful procedures were included in the number of insertions, as unsuccessful procedures still exposed the patient to radiation, and potentially discomfort.
Procedural details including radiation dose measured as dose area product (DAP) in mGycm2 on an integral DAP meter, fluoroscopy time (minutes), frame rate (frames/second), and size of the NJT were recorded. Corflo NJTs, mostly weighted (1.5 g pediatric weight with stylet were used; Corpak MedSystems). Outcome of the procedure (successful/unsuccessful NJT placement) and the occurrence of complications were obtained using radiology reports in PACS.
Radiation Dose
Mean, minimum, and maximum DAP were determined according to different age and weight categories to capture radiation dose according to body size, as body surface area was not calculated. Patients were divided into different weight groups for standardization, according to the 2008 GE weight-based CT scanning categories.
Indications for Reinsertion
Indications for repeat insertion were recorded from the radiology request form on PACS and grouped into mechanical, positional, symptom-related, and pulled categories. The latter was subdivided into pulled accidentally (unplanned pulled) or intentionally (planned pulled) if necessitated by a procedure (planned pulled), for example, abdominal computed tomography to avoid tip artifact. Reinsertion requests not specifying a particular reason were grouped accordingly.
Referrer Details
Referrer details including the ward, service, and referring physician were also obtained from PACS to identify sources of frequent NJT referrals.
Statistics
Data were analyzed using Microsoft Excel 2007 and Statistical Package for the Social Sciences (SPSS; IBM SPSS Statistics Version 21).
Results
Patients
Four hundred and fifty-four NJT insertions from February 2007 and August 2012 were identified from PACS. Five insertions were excluded from the initial audit due to data entry errors, leaving 449 NJT insertions for study inclusion.
The 449 NJT insertions were performed in 252 patients, 116 (46%) male and 136 (54%) female, with an age range of 3 days to 17 years 11 months (median = 5.3 months) and weight range of 1.23 to 113.5 kg (median = 5.22 kg).
Procedure Details
Of the 449 insertions, 396 (88.2%) were classified as successful, the majority with the tip in the third or fourth parts of the duodenum, only a few in the second part of the duodenum. Mean fluoroscopy time for the procedures was 4.5 ± 4.1 minutes.
Radiation Dose
As anticipated, mean DAP showed an overall increase with age (Table 1) and weight (Table 2).
Table 1.
Radiation Dose per Insertion According to Age.
| Dose Area Product (mGycm2) |
||||
|---|---|---|---|---|
| Age | N (Procedures) | Mean | Minimum | Maximum |
| 0 to 1 months | 39 | 0.23 | 0.14 | 0.89 |
| 1 to 6 months | 203 | 0.30 | 0.01 | 3.28 |
| 6 months to 2.0 years | 78 | 0.46 | 0.01 | 2.04 |
| 2.0 to 7.0 years | 23b | 0.99 | 0.10 | 2.7 |
| 7.0 to 12.0 years | 25 | 2.22 | 0,03 | 17.01 |
| 12.0 to 15.0 years | 37 | 5.60 | 0.15 | 26.98 |
| 15.0 to 18.0 years | 38 | 5.02 | 0.20 | 49.41 |
| Total | 443/449a,b | 2.47 | ||
Abbreviation: DAP, dose area product.
DAP missing for 5 NJT procedures; therefore, DAP data for these procedures were excluded.
An additional procedure was ommitted as DAP data for one patient exceeded 2 standard deviations in the 2.0-7.0 years category.
Table 2.
Radiation Dose per Insertion According to Weight.
| Dose Area Product (mGycm2) |
||||
|---|---|---|---|---|
| Weight (kg)a | N (Procedures) | Mean | Minimum | Maximum |
| 0-3 | 28 | 0.17 | 0.01 | 1.35 |
| 3-6 | 135 | 0.28 | 0.01 | 2.00 |
| 6-7.5 | 23 | 0.52 | 0.05 | 1.16 |
| 7.5-9.5 | 20 | 0.51 | 001 | 2.00 |
| 9.5-11.5 | 13b | 0.65 | 0.07 | 2.04 |
| 11.5-14.5 | 13 | 0.98 | 0.15 | 2.70 |
| 14.5-18.5 | 9 | 0.94 | 0.10 | 1.88 |
| 18.5-22.5 | 7 | 2.76 | 0.30 | 7.57 |
| 22 5-31.5 | 24 | 1.70 | 0.03 | 7.95 |
| 31.5-40.5 | 17 | 5.38 | 0.27 | 26.98 |
| 40.5+ | 46 | 6.29 | 0.20 | 49.41 |
| Total | 335/449 | 2.22 | ||
Weight divisions based on GE weight-based CT scanning categories (2008).
One procedure was ommitted as DAP data for one patient exceeded 2 standard deviations in the 9.5-11.5 kg category.
Radiation Dose Comparison
Radiation dose comparisons between conventional abdominal radiographs, low-dose radiographs, fluorospot, and conventional fluoroscopy are illustrated in Table 3. Mean DAP using our fluoroscopic NJT technique is comparable to low-dose radiographs and higher than fluorospot technique as expected, but lower than conventional radiographs in sample age ranges according to data from Magistrelli et al.10
Table 3.
Radiation Dose (DAP) Comparison Between Conventional Abdominal Radiographs, Low-Dose Radiographs, Fluorospot, and Conventional Fluoroscopy.
| Mean DAP (per age in years) | 1 | 5 | 10 |
| Conventional abdominal radiographa,b | 6.23 | 8.94 | 11.98 |
| Low-dose radiographa,c | 0.43 | 0.49 | 1.20 |
| Fluorospota | 0.08 | 0.25 | 0.16 |
| Fluoroscopyd (our study) | 0.52 | 0.66 | 1.93 |
Abbreviation: DAP, dose area product.
Mean DAP for these procedures taken from Magistrelli et al.10
Standard plain-radiography (abdominal) with kid-size presets.
Fixed parameters (121 kV/<0.5 mA).
For comparison purposes, the mean DAP for fluoroscopy was calculated based on a smaller sample size, as the number of our patients in the reference age categories was small.
Reinsertion Frequency and Timing
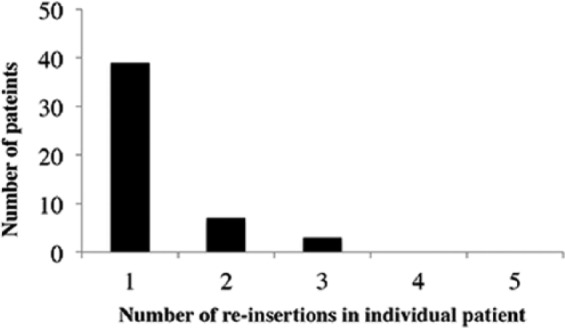
A total of 105 of 252 (41.7%) patients underwent multiple reinsertions. Of these, the majority had between 2 to 4 insertions; very few had 5 or more (Figure 1). Of the 449 NJT procedures examined, 197/449 (43.9%) were repeat insertions excluding the first insertion, 302/449 (67.3%) if the first was included (Figure 2). Reinsertions occurred most commonly in patients <1 year of age (Figure 3), with 43.1% of reinsertions occurring within 1 week and 82.7% occurred within 1 month (Figure 4).
Figure 1.
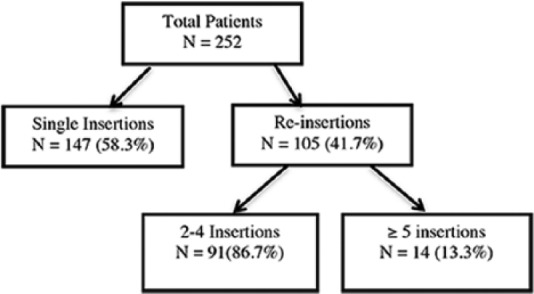
Number of patients having single and multiple insertions.
Figure 2.
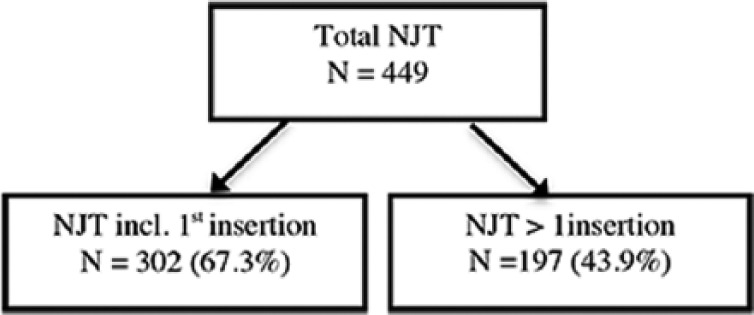
Number of NJT single and multiple insertions.
Figure 3.
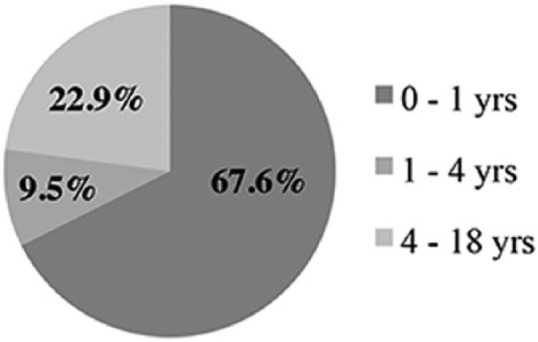
NJT reinsertion frequency according to age.
Figure 4.

Frequency of reinsertion in each time interval.
(n = number of NJT procedures included in specific time interval; total = 197).
Indications for Reinsertion
The majority of reinsertions were due to NJTs being pulled out (34.0%) either accidentally (unplanned; 31.5%) or intentionally for a specified procedure (planned; 2.5%; Figure 5). Reinsertion frequency by age in the unplanned group was similar to the overall group (Figure 3), again most occurring under 1 year of age (median 6 months), within 1 month, similar to the overall group, and most having only undergone one reinsertion (Figure 6). A smaller proportion of reinsertions were a consequence of mechanical issues, such as blocked, leaking or broken tubes or tubes due for replacement, and positional issues, including tubes reverting to a nasoduodenal or nasogastric position, rarely too distal. Fewer were due to patient symptoms, including but not limited to vomiting and intussusception, with indication in a similar number unspecified.
Figure 5.
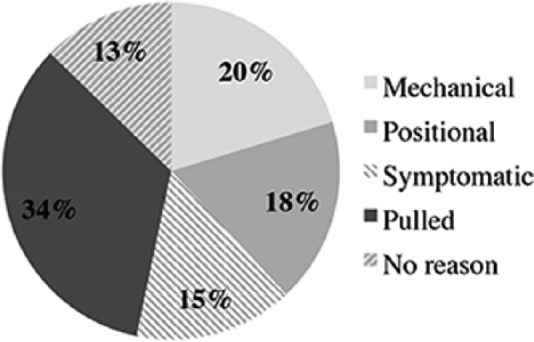
Indications for repeat insertions (N = 197).
Figure 6.
Reinsertion frequency in patients in unplanned pulled group.
Referral Details
Most frequent referrals were from general pediatrics (17.2%), neonatal (16.5%) and pediatric (11.9%) intensive care, and gastroenterology (12.4%), with the remaining referral groups each less than 10%.
Discussion
Fluoroscopic NJT insertions, despite having high success rates as reported in previous studies,8,11 can expose a child to commensurately higher radiation exposure if multiple insertions are required. In our study, radiation dose demonstrated an overall increasing trend with age and weight as we had expected. However, when comparing against reported but unpublished DAP values from Magistrelli et al,10 alternative imaging techniques, such as use of low-dose radiography or fluorospot to confirm NJT tip positions, become viable options to minimize radiation exposure, the latter a third or less of the mean DAP when compared with fluoroscopy. By procedure modification, reducing exposure to ionizing radiation and anticipated stochastic effects can potentially be better achieved.9
Vitta et al reported a reinsertion frequency of 60% with an average of 4.3 fluoroscopic NJT insertions occurring in children who underwent multiple insertions under a 4-month time period; however, 2 had more than 20 insertions in a 14-month period corresponding to a cumulative DAP of 50 cGycm2 and 31.2 cGycm2, respectively.7 This is comparable to our results with a reinsertion frequency of 67.3% with a lower average of 2.9 insertions in children undergoing multiple insertions. Moreover, the majority of our reinsertions occurred in patients aged less than 1 year and within 1 week of prior insertion. Of those patients that underwent multiple reinsertions, 86.7% underwent 2 to 4 insertions, while 13.3% represented exceptional cases where patients underwent 5 or more insertions. In our study, the greatest number of insertions in a single patient was 9 insertions within 3 months. The high reinsertion frequency, the short time interval within which the majority of reinsertions occurred, the overrepresentation of younger and smaller patients, and the exceptionally high number of reinsertions in a subset of our patients warrants serious consideration of alternate techniques to minimize radiation dose.
Most reinsertions resulted from an NJT being pulled out, the majority of these unintentionally (31.5%), although in this unplanned pulled group most underwent only one reinsertion. Timing between reinsertions for this group was comparable to the overall group, the majority occurring under a 1-month time period, and in patients under 1 year of age. Since the majority of reinsertions were required due to instances of pulled tubes, particularly in our younger patients, spending more time securing the tube on initial placement may help reduce the frequency and need for multiple reinsertions in cases where tubes are accidentally pulled by patients or caregivers.
Our high reinsertion rate can likely be attributed to a number of other factors. First, 1.5-g weighted tips were used at the time these procedures were conducted, which are different from the 1-g weighted tips currently used at our institution. Anecdotally, the shorter length of the 1-g weighted tip makes it easier to maneuver the NJT around the duodenal loop, better facilitating insertion. Tube insertions are also typically more difficult in pediatric patients due to their smaller size and decreased compliance. Two thirds of our patients were less than a year and less than 6 kg, making insertion of NJTs challenging. Concomitantly, although these data were not formally collected, many were likely to be performed in complex care patients or patients with comorbidities, further contributing to the challenging nature of these insertions.
Operator proficiency may have also had a contributory effect on our high reinsertion rate. Although all procedures were conducted by pediatric-fellowship-trained radiologists and fellows, technique of insertion may have varied between radiologists, with possible effect on the success of the procedure.
An analysis of referrer details demonstrated that general pediatrics and the neonatal and pediatric intensive care units were the most frequent NJT referrers, constituting one-half of all NJT referrals during the 5-year time period. Capturing this information is imperative to identifying those groups most likely to benefit from improving or modifying strategies for NJT insertion, particularly in patients who have or are at risk for undergoing multiple insertions. This will allow more targeted education of referring physicians when implementing procedure modification.
Limitations of our study include the retrospective nature of our study and that data were collected from a single institution only. Inconsistencies in the availability of procedural details such as inclusion of radiation dose (DAP) and type of NJT inserted were also encountered. Additionally, NJT tip position was confirmed by details contained within the radiology report and not by direct assessment of images in PACS. This may have contributed to slight discrepancies between the described and actual positioning of the tip between different practitioners and subsequent determination of procedural success. For instance, whether a loop was left in the stomach would not have been evaluated but may have been cause for a reinsertion.
A high NJT reinsertion frequency strongly suggests the need to adopt a policy change reducing the number of reinsertions. This could include more standardized techniques for insertion and securing of NJTs continuing with the current approach, or using lower dose techniques such as blind insertion at the bedside with a fluorospot to check position.
An approach to flagging a patient undergoing, for example, a third insertion may allow for the referring physician to become aware of a patient’s difficulty in tolerating an NJT, particularly if in short time frames, and if referred for reinsertions without awareness of the primary physician. This could serve as a time point to reassess and potentially hasten definitive management, such as fundoplication or gastrostomy tube, or consider an alternative lower dose technique, such as a bedside placement of an NJT.
One aspect of NJT insertion this study did not address but is considered an important consideration is patient acceptance or tolerance of the fluoroscopically guided procedure. In our experience, there is a distinct benefit of the self-guided approach over the fluoroscopically guided technique, as the self-guided approach requires no or minimal catheter manipulation beyond initial insertion of the catheter tip into the stomach in most instances. Few studies address NJT patient tolerance, rather they refer more to rate of feeding tolerance than acceptance.4,12 Qualitatively evaluating one or both techniques in older patients could be undertaken prospectively.
It is also worth mentioning that data regarding the anchoring technique of the NJT at the nares was not captured in this study as this information was not always available in the radiology report. This could be a point of special attention for patients where reinsertions are common.
Future directions should also involve interdisciplinary collaboration to optimize the NJT referral process and establish policies to address patients undergoing multiple insertions.
Conclusion
High NJT reinsertion frequency in our patient population and associated radiation exposure with fluoroscopically guided NJT insertions suggests implementing a policy change, which would enable a patient to receive a definitive treatment earlier or an alternative lower dose blind bedside insertion.
Footnotes
Authors’ Note: All relevant data have been included in the article, but access to any source material sought by the reader including individual de-identified patient results can be obtained directly from the corresponding author.
Author Contributions: NS: Assisted with data collection, data analyses, data interpretation, drafted the initial manuscript, and approved the final manuscript as submitted.
MF: Assisted with the study design, data collection, analysis, provided ongoing input throughout manuscript preparation, and approved the final manuscript as submitted.
M-LG: Conceptualized and designed the study, assisted in data analyses, critically reviewed the manuscript, and approved the final manuscript as submitted. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Prieto MB, Cid JLH. Malnutrition in the critically ill child: the importance of enteral nutrition. Int J Environ Res Public Health. 2011;8:4353-4366. doi: 10.3390/ijerph8114353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Holmes S. Enteral nutrition: an overview. Nurs Stand. 2012;26(39):41-46. doi: 10.7748/ns2012.05.26.39.41.c9133. [DOI] [PubMed] [Google Scholar]
- 3. Pearce CB, Duncan HD. Enteral feeding. Nasogastric, nasojejunal, percutaneous endoscopic gastrostomy, or jejunostomy: its indications and limitations. Postgrad Med J. 2002;78:198-204. doi: 10.1136/pmj.78.918.198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Phipps LM, Weber MD, Ginder BR, Hulse MA, Thomas NJ. A randomized controlled trial comparing three different techniques of nasojejunal feeding tube placement in critically ill children. J Parenter Enteral Nutr. 2005;29:420-424. doi: 10.1177/0148607105029006420. [DOI] [PubMed] [Google Scholar]
- 5. Hwang JY, Shin JH, Lee YJ, et al. Fluoroscopically guided nasojejunal enteral tube placement in infants and young children. AJR Am J Roentgenol. 2009;193:545-548. doi: 10.2214/AJR.08.1341. [DOI] [PubMed] [Google Scholar]
- 6. Gopalan S, Khanna S. Enteral nutrition delivery technique. Curr Opin Clin Nutr Metab Care. 2003;6:313-317. doi: 10.1097/01.mco.0000068968.34812.14. [DOI] [PubMed] [Google Scholar]
- 7. Vitta L, Raghavan A, Morrell R, Sprigg A. Fluoroscopy-guided insertion of nasojejunal tubes in children—setting local diagnostic reference levels. Pediatr Radiol. 2009;39:1203-1208. doi: 10.1007/s00247-009-1362-y. [DOI] [PubMed] [Google Scholar]
- 8. Puustinen L, Numminen K, Uusi-Simola J, Sipponen T. Radiation exposure during nasojejunal intubation for MRI enteroclysis. Scand J Gastroenterol. 2012;47:658-661. doi: 10.3109/00365521.2012.674971. [DOI] [PubMed] [Google Scholar]
- 9. Hricak H, Brenner DJ, Adelstein SJ, et al. Managing radiation use in medical imaging: a multi-faceted challenge. Radiology. 2011;258:889-905. doi: 10.1148/radiol.10101157. [DOI] [PubMed] [Google Scholar]
- 10. Magistrelli A, Schnigo PMS, Corneli T, et al. , et al. Foreign body ingestion in pediatric population: is there a role for low-dose radiography and fluoroscopy? Poster session presented at: 50th annual meeting of the European Society of Pediatric Radiology; June 5-7, 2013; Budapest, Hungary. [Google Scholar]
- 11. Pobiel RS, Bisset GS, 3rd, Pobiel MS. Nasojejunal feeding tube placement in children: four-year cumulative experience. Radiology. 1994;190:127-129. doi: 10.1148/radiology.190.1.825-9389. [DOI] [PubMed] [Google Scholar]
- 12. Chang Y, Fu H, Xiao Y, Liu J. Nasogastric or nasojejunal feeding in predicted severe acute pancreatitis: a meta-analysis. Crit Care. 2013;17:R118. doi: 10.1186/cc12790. [DOI] [PMC free article] [PubMed] [Google Scholar]