

Sir,
Cataract surgery in cases of persistent fetal vasculature (PFV) is challenging despite the recent advances in the surgical technique, particularly if the diagnosis is made intraoperatively. We describe salmon pink patch sign in eyes with PFV. It is the presence of pink hue emerging from within the lens substance indicating the possibility of patent blood flow within the mass.
A 10-month-old child presented with unilateral cataract OD noticed by the parents since 5 months of age. There was no family history of cataract or trauma. There was evidence of mild exodeviation of the right eye (Hirshberg 15°). Gross examination showed a well dilating pupil; on indirect ophthalmoscopy, visualized peripheral fundus was within normal limits. Ultrasonography for the posterior segment was anechoic, and axial lengths were 20.5 mm OD and 20.6 mm OS. On examination under anesthesia, corneal diameters measured 10.5 mm × 11 mm each eye. Lamellar cataract was observed with an eccentric posterior capsular mass reflecting a pink hue [Figure 1a]. As phacoaspiration was performed, the mass was found to be retrolenticular, and a stalk emerging from posterior lens surface could be identified [Figure 1b]. With the confirmation of PFV, plasma blade was arranged. Primary posterior capsulorhexis was performed by manual peeling with Internal limiting membrane (ILM) peeling forceps after giving capsular nick using a bent 26 gauge needle [Figure 1c]. Vascular stalk was coagulated using Fugo plasma blade (MediSURG R and MC). The coagulated avascular retrolenticular mass was removed with a 23 gauge vitrectomy probe as limited anterior vitrectomy was performed [Figure 1d]. A single piece acrylic foldable IOL (Acrysof SN60AT, Alcon Laboratories Inc.) was implanted in the bag.
Figure 1.
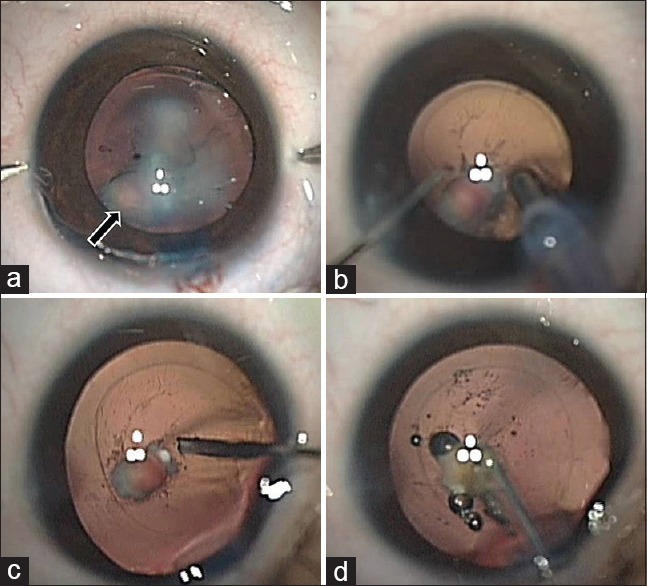
(a) A congenital cataract showing the presence of an eccentric salmon pink sign intraoperatively (arrow). (b) Irrigation aspiration of the lens matter further enhances the pinkish hue from the retrocapsular plaque. (c) Posterior capsulorhexis is being performed with a bent 26 gauge needle. (d) The vascularized mass is coagulated with Fugo plasma blade
Cataract-associated with PFV may be associated with a high risk of intraoperative bleeding if associated with a patent hyaloid artery passing through the posterior capsule. Cutting the capsule during posterior capsulorhexis unknowingly may avulse the vascular stalk resulting in nonsalvageable intraocular hemorrhage. This may sometimes require abandoning the surgery.[1,2] Fugo plasma blade is recommended for coagulating the active vascular stalk before cutting it.[3,4] However, in certain situations, one may not be aware of the diagnosis preoperatively. The thin avascular stalk may be missed out completely on ultrasonography, and the eye may be normal in size as seen in this case. Doppler ultrasonography helps in ascertaining the patency of blood flow noninvasively;[5] however, is performed only in suspected cases. Mass with a pinkish hue, especially if eccentric, a sign which we label as the salmon pink patch is suggestive of active vasculature within PFV. When visualized, it should alarm the surgeon of the possibility of patent vasculature.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Tartarella MB, Takahagi RU, Braga AP, Fortes Filho JB. Persistent fetal vasculature: Ocular features, management of cataract and outcomes. Arq Bras Oftalmol. 2013;76:185–8. doi: 10.1590/s0004-27492013000300011. [DOI] [PubMed] [Google Scholar]
- 2.Onder F, Cossar CB, Gültan E, Kural G. Vitreous hemorrhage from the persistent hyaloid artery. J AAPOS. 2000;4:190–1. doi: 10.1016/s1091-8531(00)70014-0. [DOI] [PubMed] [Google Scholar]
- 3.Khokhar S, Tejwani LK, Kumar G, Kushmesh R. Approach to cataract with persistent hyperplastic primary vitreous. J Cataract Refract Surg. 2011;37:1382–5. doi: 10.1016/j.jcrs.2011.06.012. [DOI] [PubMed] [Google Scholar]
- 4.Sinha R, Bali SJ, Kumar C, Shekhar H, Sharma N, Titiyal JS, et al. Results of cataract surgery and plasma ablation posterior capsulotomy in anterior persistent hyperplastic primary vitreous. Middle East Afr J Ophthalmol. 2013;20:217–20. doi: 10.4103/0974-9233.114794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Neudorfer M, Waisbourd M, Buzi S, Wygnanski-Jaffe T, Stolovitch C, Barak A, et al. Color Doppler imaging of eyes with persistent fetal vasculature. Pediatr Radiol. 2012;42:1229–34. doi: 10.1007/s00247-012-2432-0. [DOI] [PubMed] [Google Scholar]