

Abstract
Objectives
To explore the utility of home and community-based HIV testing and counseling (HTC) to increase detection of undiagnosed HIV among female spouses and children of HIV-positive PWID in Punjab province, Pakistan.
Design
Between March 2014 and March 2015, home-based HTC was provided by a local NGO to spouses of HIV-positive PWID in Lahore, Faisalabad, and Sargodha. Convenience sampling was used to identify 2400 married, HIV-positive men who inject drugs and who were currently registered and receiving harm reduction services from the NGO ‘Roshan Rasta’ and seek consent to approach their wives.
Method
Trained outreach teams conducted HTC and administered a short sociodemographic and behavioral questionnaire to consenting spouses in their homes. HIV-exposed children were also tested with parental consent.
Results
of the 2400 married HIV positive male-injecting drug users, only 1959 spouses were approached and 1896 agreed to HTC (96.8%). HIV prevalence was 5.3% (n = 101) among spouses and they had very low level of HIV-related knowledge and protective behaviors
Conclusion
Home and community-based HTC was effective in identifying undiagnosed HIV among spouses of PWID, the majority of whom reported low rates of prior HIV testing and low HIV-related knowledge. Expansion of HIV prevention services and linkages to treatment and care including PMTCT are urgently needed for this group.
Keywords: HIV, injecting drug users, Pakistan, spouses
INTRODUCTION
The HIV epidemic in Pakistan is driven largely by people who inject drugs (PWID). Current national prevalence among PWID is 27.2%, with higher concentrations in areas such as Punjab where up to 37.8% of PWID are living with HIV [1]. Drug use is illegal in Pakistan and punishable by law; these punitive drug policies lead to stigmatization, and push many users underground and out of reach to HIV prevention, and harm reduction services and providers [2].
Limited access to HIV prevention, treatment, and care services among PWID contributes to the onward transmission of HIV to their sexual partners [3]. The high prevalence of HIV among PWID combined with low levels of protective behaviors, 77.4% of PWID did not use a condom at last sex in 2014 [4]. As in other settings, the spouses of PWID also face substantial stigma and discrimination, which increases their vulnerability to HIV [5,6]. Latest estimates suggest that there are around 104 500 PWID in Pakistan and 60 to 65 thousand in Punjab and as many as 33.8% are married [4].
However, there has been very limited uptake of HIV testing and counseling (HTC) in Pakistan [4] resulting in poor identification of key populations living with HIV and even fewer opportunities for case finding among pregnant women. This hampers prevention of parent to child transmission (PPTCT) efforts [7].
Between 2014 and 2015 March, Roshan Rasta and Punjab AIDS Control Program with support from UNICEF Pakistan, conducted this pilot initiative. The overall objective of this pilot was to explore the utility of home and community-based testing of undiagnosed HIV among spouses and children of HIV-positive PWID.
METHODS
Settings
The pilot program was carried out in Lahore, Faisalabad, and Sargodha, three of the largest cities in Punjab province with high concentrations of HIV-positive PWID [1]. Roshan Rasta, the implementing partner selected for this pilot, is an NGO that has been providing HIV prevention and harm reduction services across Punjab province.
Participant selection and sampling
Sample size was determined based on the current number of registered HIV-positive PWID at each of the three drop-in centers. Fig. 1 displays the target number of spouses and number reached in the three pilot sites.
FIGURE 1.
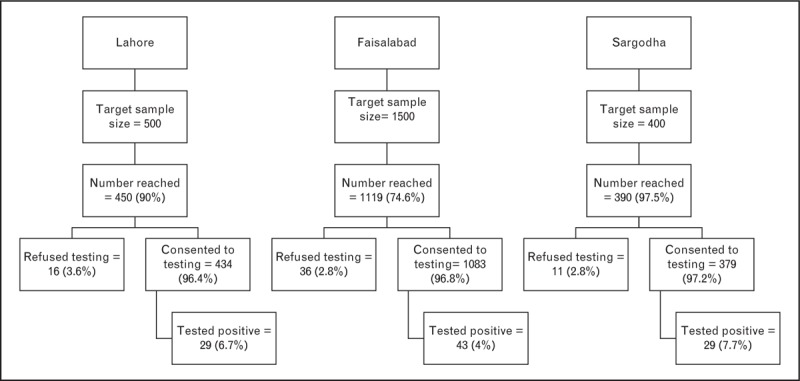
People who inject drugs spouses: targets and reach by pilot site.
Spouses were identified through their husbands; the following selection criteria was used to identify suitable men: known HIV diagnosis; history of injecting drug use, registered with Roshan Rasta at the time of the pilot and had a spouse whose HIV status was unknown. Using convenience sampling eligible HIV-positive PWID who attended the drop-in center during the study period. The consent for spouses was obtained from their husbands. A counselor was available during the study to provide support to the PWID and spouse regarding the importance of HIV testing.
Implementation
Consenting PWID signed a form granting permission for outreach teams to visit their wives at home. Outreach teams comprised one woman counselor and one male outreach worker. During home visits, the objectives of the pilot program/study were described and explained that participation was completely voluntary and confidential; those who agreed signed a consent, a short, quantitative questionnaire was administered by the woman counselor. This questionnaire included sociodemographic status, HIV-related risk factors, access, knowledge and vulnerability in the local language (‘Urdu’). Female counselor provided pretest HIV counseling. Testing was done using three serial rapid test algorithm (‘Alere Determine HIV, followed by Uni-Gold, and SD Bioline’ in the case of a positive, first test) as per national and WHO guidelines [8]. The female counselor was responsible for delivering the results and posttest counseling.
Spouses who tested positive were provided with referrals to local HIV treatment and care facilities. Consent was also sought from HIV-spouses to test any of their children who were aged between 2 and 10 years. There were no PCR facilities available in any of the pilot sites, necessary for detecting HIV among infants. Consequently, all HIV testing was done with rapid test kits which are recommended for use on children aged 2 and over. A decision was made to limit testing to HIV-exposed children aged up to 10 on the assumption that a child infected perinatally would not have survived beyond this age in the absence of HIV diagnosis and treatment.
Ethical considerations
The pilot was conducted as an extension of Roshan Rasta's implementation/programmatic activities. A number of measures were taken to ensure ethical conduct, particularly in regards to confidentiality and consent. Consent was obtained from PWID and their spouses.
During home visits, outreach teams took the utmost care to ensure privacy; if this could not be guaranteed (for example, if the wife lived with extended family members) arrangements were made to conduct the counseling and testing at a Roshan Rasta drop in center or at a arranged place in the community.
Spouses who tested positive during the pilot were provided with referrals to local services for further follow up, treatment and care. A qualified female psychologist was retained on staff throughout the study period and was available to provide support with disclosure and counseling.
Data analysis
Data was transferred to Excel for cleaning and analysis. We use descriptive statistics to describe the findings of this pilot study.
RESULTS
Of 1959 spouses of HIV-positive PWID visited, 1896 (96.7%) consented to home and community-based HIV testing and counseling and participation in pretest questionnaire across Lahore, Faisalabad, and Sargodha.
Sociodemographic characteristics
The average age of the 1896 spouses was 31.5 years (range 17–60 years), with 51% (n = 972) aged between 26 and 35. The majority were illiterate or had not completed any schooling (36.1%; n = 685), whereas 32% (n = 592) had completed between 1 and 5 years of education at the primary level. Only 20% (n = 328) of spouses had more than 9 years of education, the majority of whom were located in Lahore (Table 1).
Table 1.
Sociodemographic characteristics of spouses of people who inject drugs, by location
| Total (n = 1896) | Lahore (434) | Faisalabad (1083) | Sargodha (379) | |
| n (%) | n (%) | n (%) | n (%) | |
| Age group | ||||
| Average (range) | 31.5 (17 – 60) | |||
| 18–25 years | 436 (23) | 108 (24.9) | 260 (24) | 69 (18.2) |
| 26–35 years | 972 (51.3) | 192 (44.3) | 597 (55.1) | 182 (48) |
| 36–45 years | 432 (22.8) | 117 (27) | 208 (19.2) | 106 (28) |
| 45 and over | 56 (3) | 16 (3.7) | 18 (1.7) | 22 (5.8) |
| Level of education | ||||
| Illiterate/none | 685 (36.1) | 0 (0) | 440 (40.6) | 245 (64.8) |
| Primary (1–5 years) | 592 (32.2) | 80 (18.4) | 420 (38.8) | 92 (24.3) |
| Middle (6–8 years) | 237 (12.5) | 68 (15.7) | 138 (12.7) | 31 (8.2) |
| Matric and above (9+ years) | 382 (20.2) | 286 (65.9) | 85 (7.9) | 11 (2.9) |
| Monthly household expenditurea | ||||
| Average expenditure (range) | 8980 PKR (2000–14 000) | |||
| Less than 5000 PKR (Less than US $47) | 213 (14.5) | 15 (3.5) | 181 (27.5) | 17 (4.5) |
| 5001–10 000 PKR (US $48–95) | 950 (64.9) | 311 (71.7) | 429 (65.2) | 210 (55.4) |
| 10 001–15 000 PKR (US $96–143) | 265 (18.1) | 100 (23) | 35 (5.4) | 130 (34.3) |
| 15 001 and above (US $144 and above) | 37 (2.5) | 8 (1.8) | 7 (1.1) | 22 (5.8) |
| Age at marriage | ||||
| Average (range) | 21 (10–35) | |||
| 18 and under | 513 (27.1) | 247 (56.9) | 130 (12) | 136 (35.9) |
| 19–25 years | 1201 (63.4) | 180 (41.5) | 786 (72.6) | 237 (62.5) |
| 26 and above | 180 (9.5) | 7 (1.6) | 167 (15.4) | 6 (1.6) |
| Number of children | ||||
| None | 177 (9.3) | 41 (9.5) | 103 (9.5) | 33 (8.7) |
| 1–3 | 1287 (67.9) | 254 (58.3) | 786 (72.7) | 246 (64.9) |
| 4–6 | 410 (21.6) | 132 (30.4) | 186 (17.2) | 92 (24.3) |
| More than 6 | 22 (1.2) | 7 (1.6) | 7 (0.6) | 8 (2.1) |
aMissing = 431 due to this subset of questions being unintentionally omitted by some outreach teams in Faisalabad. Surveys were not completed correctly in Faisalabad.
Question about monthly household expenditure was administered. Spouses typically had spent around US $88 per month on household expenses (PKR. 8980), ranging from US $19 to 187 (range PKR. 2000–14 000). Spouses in Sargodha reported the highest monthly household expenditure, with 34% (n = 130) spending between US $134 and 200 (PKR. 10 000–15 000) per month compared to 23% (n = 100) in Lahore and 5.4% (n = 35) in Faisalabad. The average monthly household expenditure found considerably lower than the average expenditure of lowest quintile households in Punjab (US $119 or NPR. 12, 131 in 2014) [9] (Table 1).
The majority of spouses were married young, with nearly two thirds (63.4%; n = 1201) married between the ages of 19 and 25 years. The youngest age at marriage was 10 years and the oldest was 35. On average, spouses were married around age 21 (Table 1).
The group had 4673 children in total, with the number of children per woman ranging from 0 to 10 (data not reported). The majority had between 1 and 3 children (63.5%) (Table 1).
The majority of spouses were housewives (58%; n = 970) whereas 13% (n = 217) worked as a domestic or garment/factory worker, respectively. Other occupations include ‘dancer’ (n = 5), ‘female sex worker’ (n = 2), and beggar (n = 17; data not reported).
HIV-related knowledge
HIV-related knowledge was low among spouses. Only 12.8% (n = 109) provided correct answers to all seven items (Fig. 2). Individually, nearly all could correctly identify ‘unprotected sex and sharing of needles’ as major routes of transmission (93.6 and 92.5% respectively), but half failed to reject ‘sharing meals, sharing toilets, and mosquito bites’ as possible routes of HIV transmission (correctly answered by 58.7, 56.1, and 56.1% respectively). Furthermore, one-third of spouses were unable to identity ‘mother to child transmission and breastfeeding’ as possible sources of HIV transmission (33.5 and 33.4%, respectively; Fig. 2).
FIGURE 2.
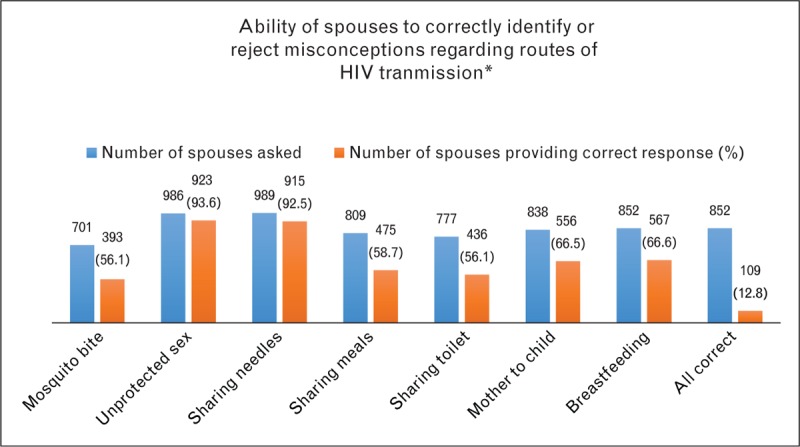
Ability of spouses to either identify correct responses or reject misconceptions regarding routes of HIV transmission. ∗There was some confusion about how to administer this question in the survey by field teams, resulting in a substantial amount of incomplete data, which was subsequently excluded. Consequently, the number of respondents for each mode of transmission varies. We calculate ‘all correct’ based only on spouses that provided a response to all seven modes.
More than half of spouses demonstrated comprehensive knowledge of HIV prevention with 53.7% (n = 786) of spouses correctly identifying three main ways to prevent transmission of HIV (‘Using condoms; using clean needles and syringes, and knowing your HIV status/testing’) (Table 2).
Table 2.
HIV knowledge and risk behaviors among spouses of people who inject drugs
| Total | % | |
| Has ever heard of HIV and AIDS (n = 1851)a | ||
| Yes | 955 | 51.6 |
| No | 896 | 48.4 |
| Has comprehensive knowledge of HIV preventionb (n = 1851)a | ||
| Yes | 786 | 42.5 |
| No | 1065 | 57.5 |
| Has self-reported knowledge of HIV transmission (n = 1836)a | ||
| (Do you know how a person becomes infected with HIV?) | ||
| Yes | 925 | 50.4 |
| No | 911 | 49.6 |
| Lifetime history of injection drug use (any) (n = 1893)a | 48 | 2.5 |
| Has ever shared needles with husband | 35 | 72.9 |
| Currently injecting | 42 | 87.5 |
| Consistent condom use with husband past 6 months (n = 1895)a | ||
| Yes | 254 | 13.4 |
| No | 1641 | 86.6 |
aOwing to some errors in the ways these questions were asked and recorded in Faisalabad, a number of incomplete responses were excluded from this final aggregation.
bDefined as those correctly identifying using condoms, using clean needles, and knowing your HIV status as ways to prevent HIV transmission.
HIV risk behaviors
Forty eight spouses (2.5%) reported a lifetime history of injection drug use. Among them most were injecting at time of survey (n = 42) and reported ever sharing a needle with their husbands (n = 35) (Table 2). Findings were lower than rates of drug using behaviors among PWID spouses reported elsewhere where it was found to be as high as 23 and 19% respectively [3]. Spouses reported very low levels of condom use, only 13% (n = 254) used condoms consistently with their husbands during the past six months (Table 2).
STI symptoms
Of the 605 nearly 31.9% of spouses reported a lifetime history of STIs, among them 270 (44.7%) were experiencing one or more STI symptom at the time of the study. The most commonly reported symptoms among these spouses were ‘vaginal discharge (n = 231), vaginal itching (n = 177), and lower abdominal pain’ (n = 129) (Table 3).
Table 3.
STI symptoms and HIV status among spouses of people who inject drugs
| n (n = 1896) | % | |
| Reported lifetime history of STIs | 605 | 31.9 |
| Currently experiencing STI symptoms (any) | 270 | 44.7 |
| Type of symptom experienceda | ||
| Discharge | 231 | 85.6 |
| Vaginal itching | 177 | 65.6 |
| Lower abdominal pain | 129 | 47.8 |
| Spouses testing HIV-positive | 101 | 5.3 |
| Lahore (n = 434) | 29 | 6.7 |
| Faisalabad (n = 1083) | 43 | 4 |
| Sargodha (n = 379) | 29 | 7.7 |
| Number of HIV-positive spouses with history of injection drug use | 35 | 34.7 |
| Total number of children of HIV exposed childrenb | 191 | |
| HIV-exposed children testedc | 74 | 38.7 |
| HIV-positive | 7 | 9.5 |
aMultiple responses possible.
bDefined as children of mothers who returned HIV positive test results.
cOwing to the difficulties with obtaining consent from mothers, we were only able to test a small proportion of HIV-exposed children. We discuss the implications of this in or discussion.
HIV status
Of 1896 spouses tested for HIV, 101 were diagnosed positive (prevalence of 5.3%). Sargodha had the highest of positive results at 7.7% (n = 29) followed by Lahore at 6.7% (n = 29) and Faisalabad at 4% (n = 43). A total of 35 of the 101 (35%) spouses who were positive reported a lifetime history of injecting drugs (Table 3). Women (n = 101) had 191 children between the ages of 2–10. Owing to difficulties in obtaining consent from their mothers, only 74 children were screened (38.7%) and seven were found to be positive (9.5%) (Table 3).
In the study period, 23 HIV-positive spouses had been successfully linked to a treatment center (22.3%), as well as with community home-based care program.
CONCLUSION
Overall, we found that home and community-based HIV testing was an effective way of expanding access and identifying cases of undiagnosed HIV among spouses of PWID, particularly those who are hard to reach by HIV prevention services. The findings identified PWID spouses as a particularly vulnerable group: one third reported a lifetime history of STIs, and approximately one fifth were experiencing one or more STI symptom at the time of the study. Not only does this corroborate the high rates of inconsistent condom use between spouses, it also indicates the unmet need for STI prevention and treatment and other medical care.
Home and community-based HIV testing was also an effective means of accessing children of PWID. Despite only screening around two-fifths of HIV-exposed children aged 2–10 years, seven were found HIV positive. The majority of spouses who were diagnosed positive were reluctant to consent to testing for their children.
Although found positive results, we faced substantial challenges in engaging spouses in HIV treatment and care. Many spouses and children who were positive were referred to HIV treatment and care centers, however, less than half who tested positive attended an HIV treatment center and most did not return for follow-up.
Real and perceived discrimination by healthcare providers at HIV treatment and care facilities were key barriers to uptake of HIV testing and care services. Poverty was also presented as a major barrier to treatment and care. Those motivated to start HIV treatment had limited options for HIV treatment facilities that were nearby and easily accessible for this target population.
The study also demonstrated the feasibility of reaching PWID spouses through men already engaged in services. Through existing HIV prevention and harm reduction program, we were able to reach spouses with HTC services. This study has identified a number of areas and priorities for future action. Firstly, efforts are needed to improve the HIV-related knowledge among PWID spouses, including development of information materials that are easily accessible to target population. There is need to promote PPTCT, including the importance of HIV testing for children and early initiation of treatment to ensure long-term survival of children living with HIV.
Secondly, adopting a family centered approach would help to reinforce these health promoting messages and protective behaviors. Working with PWID to help them disclose their HIV status to their spouses can establish an open environment in which conversations can be held on importance of PPTCT services. Engaging both husbands and wives together could also result in higher rates of testing. The reluctance observed among spouses to consent to testing for their children underpins the need to joint decision making and benefits of early testing and treatment. Consistent condom use should be prioritized as a way to prevent further sexual transmission of HIV among this group.
Lastly, while HIV was seen as a significant concern among spouses, their immediate concerns was survival. Linkages to other services like social and nutritional support, income-generating activities and skills development, and educational opportunities for their children should be sought. Overall, utilizing existing harm reduction programs for PWID enabled easy access to underserved spouses and mothers in Pakistan. This study demonstrated the feasibility of using to home and community-based rapid testing as a way of improving active case finding among spouses of PWID and HIV-exposed children. Systematically incorporating spouses into PWID programs would provide a setting in which routine and regular testing of partners could enable early detection of HIV, early initiation of treatment, and timely entry into the PPTCT cascade. The high-risk of HIV faced by spouses of PWID combined with the challenges associated with reaching them calls for new approaches to delivering HTC services to this group.
Acknowledgements
The authors gratefully acknowledge the staff of Roshan Rasta who were involved in this pilot project and assisted with the data collection. We also wish to acknowledge the guidance of Dr Annefrida Kisesa-Mkusa and Nattasha Dawa from UNICEF Regional Office for South Asia (ROSA).
N.S., S.S., and M.F.M. conceptualized and designed the project and provided technical assistance and oversight during its implementation, A.B.A. and H.M. collected and analysed the data and V.V. provided additional analysis and planned and drafted the manuscript.
We confirm that all authors listed above have read, reviewed, and approved this manuscript.
Financial support and sponsorship
Funding for this pilot project was provided by UNICEF Pakistan.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.National AIDS Control Program. HIV/AIDS Second Generation Surveillance in Pakistan: National Report Round IV. Islamabad: National AIDS Control Program; 2011. [Google Scholar]
- 2.UNAIDS. The Gap report: People who inject drugs [Internet]. Geneva: UNAIDS; 2014. http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/documents/unaidspublication/2014/UNAIDS_Gap_report_en.pdf. [Google Scholar]
- 3.Ahmad S, Mehmood J, Awan AB, et al. Female spouses of injection drug users in Pakistan: a bridge population of the HIV epidemic? East Mediterr Health J 2011; 17:271–276. [PubMed] [Google Scholar]
- 4.National AIDS Control Program. Global AIDS Progress Report, Pakistan 2014. Islamabad: National AIDS Control Program of Pakistan; 2014. [Google Scholar]
- 5.UNODC. Supporting access to HIV services for the female spouses of male IDU [Internet]. Islamabad: UNODC; http://www.o3interfaces.com/unodc/info_briefs_pdf/unodc_info_brief_3.pdf. [Google Scholar]
- 6.Sharma V, Sarna A, Luchters S, et al. ‘Women at risk’: the health and social vulnerabilities of the regular female partners of men who inject drugs in Delhi, India. Cult Health Sex 2014; 17:623–637. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organisation. Antiretroviral drugs for treating pregnant women and preventing HIV infections in infants: recommendations for a public health approach. Geneva: WHO; 2010. [PubMed] [Google Scholar]
- 8.National AIDS Control Program. Pakistan country strategy for HIV testing and counselling based on situation and response analysis [Internet]. Islamabad: National AIDS Control Program; 2013. http://www.nacp.gov.pk/library/reports/Technical%20Guidelines/Pakistan%20Country%20Strategy%20for%20HTC.pdf. [Google Scholar]
- 9.Pakistan Bureau of Statistics. Household Integrated Economic Survey 2011-12 [Internet]. Islamabad: Government of Pakistan; 2012. http://www.pbs.gov.pk/sites/default/files/pslm/publications/hies11_12/tables/table25.pdf. [Google Scholar]