

Abstract
Research has rarely considered criminal offenders’ psychological responses to stigma, but these responses may significantly influence behavior after release from jail/prison. Jail inmates’ perceived and anticipated stigma was assessed prior to release from jail/prison (N = 163), and outcomes were assessed one year post-release (N = 371). We hypothesized that perceived stigma would predict poor adjustment in several domains (i.e. recidivism, substance dependence, mental health symptoms, community adjustment) through anticipated stigma. Results showed that perceived stigma predicted worse community adjustment through anticipated stigma, and this varied by race. Results are explored from an interdisciplinary perspective.
Keywords: inmates, stigma, longitudinal, community
Being labeled as a stigmatized person has substantial effects on the way people think and feel about themselves, as well as how they expect to be treated by others in their environment (Link et al. 1989; Crocker, Major, and Steele 1998). Psychological research shows that such responses to stigma can interfere with functioning, and lead to maladaptive behaviors, poor mental health, and difficulty participating in the community (Inzlicht, Tullett, and Gutsell 2011). Empirical studies consistently show these relationships in non-correctional groups (Livingston and Boyd 2010), but little research has been conducted with offenders. Criminal offenders are a highly stigmatized group, marginalized via temporary and sometimes permanent restrictions on voting rights, housing, financial aid, employment, and other aspects of community involvement (Pogorzelski et al. 2005). The structural barriers affecting criminal offenders’ integration in the community have been described in depth elsewhere (see Winnick and Bodkin 2008; Morani et al. 2011). Offenders’ psychological responses to stigma may be important in understanding their reintegration in the community after release from jail or prison.
This paper draws upon several theoretical and empirical literatures, namely psychology (clinical and social psychology), sociology, and criminology to examine a model of how responses to stigma affect offenders’ behavior. This paper expands upon the few studies conducted on this topic (Winnick and Bodkin 2009; LeBel 2012) by using conceptually clear stigma constructs, constructing a model of how stigma affects behavior, and by using longitudinal data. Understanding criminal offenders’ psychological responses to stigma has the potential to inform correctional services, as responses to stigma are malleable and could be addressed in clinical interventions.
Theoretical Background
Criminal offender stigma has primarily been studied through the lens of Labeling Theory (Scheff 1966; Lemert 1974). Labeling theory in criminology states that being formally labeled as an offender (e.g. being incarcerated, receiving a felony conviction) causes one to internalize stigmatizing attitudes, withdraw from conventional society, and conform to a deviant identity (Lemert 1974). Many empirical studies drawing upon this theory compare naturalistic groups of offenders who were convicted or served time in jail versus those who had charges dropped/dismissed, sometimes showing that the former group (i.e. labeled individuals) recidivate more than those who were not formally labeled (Chiricos et al. 2007; Worrall and Morris 2011). However, psychological research shows that not everyone in a stigmatized group experiences negative outcomes, despite all being formally labeled with a stigmatized identity.
Current stigma research suggests that solely being labeled does not lead to negative outcomes, but instead differences in how people think and feel about being stigmatized, and the degree to which they anticipate future discrimination predicts functioning (Major and O’Brien 2005). Because of this, we draw upon Modified Labeling Theory (Link et al. 1989) to construct a psychological process through which stigma impacts criminal offenders’ behavior. Modified Labeling Theory suggests that when people become part of a stigmatized group (and hence formally labeled), ingrained societal stereotypes may be viewed as personally relevant and cause internalization of stigma (identity changes, negative views of self, etc.), which leads people to anticipate stigma, and in turn develop different ways of coping with their stigmatized identity, some of which may be problematic, exacerbating maladaptive behaviors (Link et al. 1989). While our paper is not a direct test of Modified Labeling Theory (due to missing key coping variables), the proposed relationships between psychological aspects of stigma and subsequent behavior are greatly influenced by this theory.
From Perceived Stigma to Behavior
Research in sociology and psychology shows that stigma affects individual behavior through complex interactions among institutional barriers that marginalize groups (structural factors), stereotypes and discrimination from community members (social factors), and individual responses to these factors (self factors) (Link and Phelan 2001). For a comprehensive model of the different facets of stigma, see Bos et al. 2013. Perceived stigma is considered the initial step in the process through which stigma impacts individual behavior. Perceived stigma refers to individuals’ perceptions of the public’s stigmatizing attitudes/negative stereotypes toward a group (Corrigan, Watson, and Barr 2006). The term perceived stigma originated from Link’s (1987) concept of discrimination/devaluation in people with mental illness, and much of the research on perceived stigma has used Link’s discrimination/devaluation scale (Winnick and Bodkin 2008; Livingston and Boyd 2010). The belief that one’s group is devalued by the public is thought to negatively affect self-esteem and self-efficacy, which ultimately affect expectations about future interactions, coping, mental health, and behavior (Corrigan et al. 2006).
Research across non-correctional stigmatized groups (e.g. people with mental illness, people living with HIV; people who use illegal drugs) shows that the more individuals perceive that their group is devalued by the public, the more they experience negative psychological and social outcomes such as depression (Semple, Patterson, and Grant 2005), poor social interactions (Perlick et al. 2001), and poor perceived community integration (Prince and Prince 2002). Perceived stigma has been linked to actual markers of poor functioning such as unemployment in people with mental illness and people who use illegal drugs (Link 1987; Luoma et al. 2007) and low treatment participation in people with mental illness (Corrigan and Rusch 2002). Further, perceived stigma is linked to increased risk-taking behaviors such as use of illegal drugs (Schomerus et al. 2011).
Researchers have just recently begun to investigate psychological responses to stigma among criminal offenders. In one study, male prisoners’ (N = 450) perceived stigma was correlated with anticipated withdrawal from society (Winnick and Bodkin 2008). Also, former prisoners’ (N = 229) perceived stigma was positively correlated with number of lifetime probation violations and a violent felony conviction (LeBel 2012), suggesting that perceived stigma is linked to maladaptive behaviors in offenders as well as other stigmatized groups.
How does Perceived Stigma affect Behavior?
A key aspect of understanding stigma involves explaining differences in how people respond to perceived stigma, and the downstream effect this has on behavior. The anticipation of experiencing discrimination may explain why perceived stigma leads to maladaptive functioning. Anticipated stigma is defined here as the expectation of personally experiencing discrimination or consequences due to having a stigmatized identity. Although most measures of anticipated stigma appear to assess perceived stigma toward the group (e.g., Winnick and Bodkin 2008) rather than the anticipation of being personally stigmatized and rejected, perceived and anticipated stigma are conceptually distinct (Quinn and Chaudoir 2009). Perceived stigma refers to perceptions that society currently holds negative views of one’s group; anticipated stigma focuses on the future, and more importantly, specifies what an individual personally expects to experience as a result of stigma (Major and Sawyer 2009; Quinn and Chaudoir 2009). This is distinguished from anticipated stigma in the sense of stereotype threat (Aronson and Steele 2005). Stereotype threat involves being primed about one’s stigmatized identity while in a situation involving the potential for discrimination, which interferes cognitively (i.e. anxiety, stress) to the point of decreasing performance (Aronson and Steele 2005).
Anticipated stigma is thought to lead to defensive behavior, distress, fear, and the urge/actual avoidance of situations, which impairs functioning (Link et al. 2001). For example, Ritsher, Otilingam, and Grajales (2003) and Baretto (2014) assert that the anticipation of discrimination may make people especially likely to succumb to behavioral avoidance of stereotyped domains, as well as withdrawal and alienation from others more generally. The few studies that have examined anticipated stigma as a correlate of functioning support these theorized relationships. Quinn and Chaudoir (2009) found that anticipated stigma was correlated with depression and anxiety in people with various concealable stigmatized identities (e.g. mental illness, criminal actions). Also, anticipated stigma was found to be associated with low life satisfaction through perceived stress in people with chronic illnesses (Earnshaw, Quinn, and Park 2012). Anticipated stigma is theorized to predict criminal behavior upon release for offenders (Benson et al. 2011), but this has not been tested. Furthermore, although central to the theory, anticipated stigma has not been tested as a mechanism through which perceived stigma affects subsequent behavior.
Factors that Influence Perceived and Anticipated Stigma
The process through which perceived stigma leads one to anticipate stigma and subsequently experience negative outcomes may depend on individual differences (Frost 2012). Research shows that perceived and anticipated stigma are correlated but theoretically distinct constructs (Moore, Stuewig, and Tangney 2013). Other research shows that perceived stigma is only modestly correlated with internalized stigma (Ritsher, Otilingam, and Grajales 2003). Taken together, this suggests that just because someone perceives stigma, does not mean that they will be personally affected by it. Further, perceived and anticipated stigma most often predict maladaptive behavior (Livingston and Boyd 2010) but could be protective for certain people (Major and Eccleston 2005). We identified four theoretically driven moderators of this process: social identity, personality characteristics (optimism and shame-proneness), and race.
Social identity
Aspects of one’s social identity, including group identification, identity centrality, closeness/connectedness with the group, and attitudes toward the group may influence how one responds to being stigmatized (Steele, Spencer, and Aronson 2002). Having a more central stigmatized identity may increase threat to the self for being part of that group, causing negative reactions to perceived stigma, and possibly the anticipation of discrimination (Major and Sawyer 2009). Identifying strongly with the stigmatized group may strengthen the relationship between perceived and anticipated stigma.
Personality traits
Stigmatization is expected to cause shame responses in stigmatized people (Braithwaite 1989; Benson et al. 2011). Therefore, individuals who are highly prone to experiencing shame may be more likely to experience negative outcomes after perceiving or anticipating stigma. Most research has not focused on shame as a moderator in the stigma process, but has instead focused on variables like internalized stigma, a construct associated with shame (Livingston and Boyd 2010) and often conceptualized as involving shame (Luoma et al. 2007). Research suggests that people who internalize stigma experience more negative outcomes (Livingston and Boyd 2010). Shame-proneness may exert such an influence in the stigma process by increasing the degree to which stigmatized individuals are vulnerable to perceived stigma, and likely to anticipate future stigmatization from the community. It is hypothesized that offenders prone to shame will have a stronger link between perceiving stigma and personally anticipating stigma.
Social-cognitive theories suggest that some personality characteristics can buffer the negative effects of stigma (Crocker et al. 1998; Watson and River 2005). Optimism is considered to be a worldview in which people generally expect positive outcomes for themselves, even when faced with adversity (Carver, Scheier, and Segerstrom 2010). Theory asserts that optimism differentiates how people respond to discrimination; it protects the “self” as it reduces the degree to which people feel threatened by discrimination toward their group (Major and Sawyer 2009). Research shows that optimism attenuates the association between perceived prejudice toward one’s gender and self-esteem and depression (Kaiser, Major, and McCoy 2004). It is hypothesized that highly optimistic offenders will be less affected by perceived stigma toward the group, and will therefore anticipate less stigmatization from the community. In addition to being a protective factor for the self, optimism is positively related to many real-world outcomes such as health, educational attainment, and occupational functioning (Carver et al. 2010). Optimism is thought to increase proactive, engagement coping and problem-solving (Carver et al. 2010). It is hypothesized that highly optimistic offenders will be less troubled by anticipated stigma, and may even make adaptive plans for release, causing a weaker relationship between anticipated stigma and subsequent indices of poor functioning.
Race
Research suggests that racial minorities process and cope with stigma differently than non-minorities because they have visible stigma (e.g. skin color, racial features). Having a visible stigma requires one to incorporate it into their identity and adapt to it (Quinn 2006). Cook, Arrow, and Malle (2011) examined the buffering effect of stigma and found that stigmatized people react less strongly to feeling stereotyped than people without stigmas, and those with visible stigmas have less behavioral inhibition and negative affect than people with concealable stigmas during interactions in which they feel stereotyped. They interpreted this as evidence that being stigmatized, especially having a visible stigmatized identity, leads people to adapt and learn to “tolerate, minimize, accept, or ignore stereotypic beliefs directed toward them” (Cook et al. 2011: 175). Research supports this, showing that people with both obvious and concealable stigmas have better mental health than those with solely concealable stigmas (Frable, Platt, and Hooey 1998).
Research on racial minorities who have double stigmas (stigma of being a minority and another stigma) shows again that racial minorities process and cope with having multiple stigmatized identities differently than non-minorities. For example, Caucasians placed more emphasis on hiding their stigmatized identity compared to African Americans living with HIV (Rao et al. 2008). Along these lines, theory on offender stigma suggests that being labeled an offender may be less meaningful for African Americans because they already manage racial minority stigma (Harris 1976). Research has found that Caucasian prisoners are more secretive about criminal offender status than African Americans (Winnick and Bodkin 2009). It is hypothesized that for minority offenders, perceived stigma regarding criminals will not have as much impact on the self because of prior experience with racial stigmatization, causing a weaker relationship between perceived and anticipated stigma. Similarly, it is hypothesized that anticipated stigma will be less predictive of outcomes for minorities, as minorities may have built up strategies to cope with such anticipated stigma through prior experiences with discrimination.
The Present Study
The purpose of this study is to evaluate a longitudinal model of how stigma affects criminal offenders’ functioning in various areas. Research has yet to examine offenders’ perceived stigma with longitudinal data, and has not yet examined potential mediating or moderating factors of the relationship between perceived stigma and indices of functioning. Further, research with correctional and non-correctional groups has yet to include anticipated stigma in models of the stigma process. This paper presents a substantial expansion of Moore, Stuewig, and Tangney’s (2013) examination of stigma among offenders. Moore, Stuewig, and Tangney (2013) found that there are race differences in bivariate relationships of stigma and behavior. Specifically, offenders’ perceived stigma predicted more employment in the year after release for African Americans, but not Caucasian inmates, and anticipated stigma predicted fewer arrests for Caucasian inmates but not African American inmates.
The current paper uses structural equation modeling to test a significantly expanded multivariate theoretical model of how perceived stigma impacts offenders post-release functioning. The primary aim of this study is to examine whether perceived stigma predicts functioning in several domains (i.e. substance dependence, community adjustment, and mental health in addition to employment and recidivism) through anticipated stigma. It is hypothesized that perceived stigma will be positively related to anticipated stigma, which will in turn predict poorer functioning. The second key aim of this paper is to determine how individual differences may influence stigma’s effect on behavior. We examine moderators of the relationship between perceived and anticipated stigma, as well as anticipated stigma and subsequent functioning. It is hypothesized that perceived stigma will be most strongly linked to anticipated stigma for inmates who are highly shame-prone, and those who have a salient social identity as a “criminal” (i.e. identify as a “criminal” and feel more connected to other offenders). It is hypothesized that the relationships between perceived and anticipated stigma, and anticipated stigma and post-release functioning will be attenuated for highly optimistic and minority inmates.
METHOD
Participants
Participants were 163 inmates recruited from June 2002 to May 2007 as part of a larger longitudinal study (Tangney, Mashek, and Stuewig 2007) at an urban adult detention center. Data were collected after entry into the jail (Time 1), again just before release to the community (Time 2), and then one year post-release (Time 3). Inmates were informed that participation was voluntary and that data were confidential, protected by a Certificate of Confidentiality from DHHS. Pre-release assessments (Time 2) were collected from 2002–2010, depending on inmates’ release dates. Post-release assessments (Time 3) were collected from 2003 to 2010. Inmates received a $15–18 honorarium for completing the Time 1 assessment, $25 for the Time 2 assessment, and $50 for the Time 3 assessment.
Of the participants who consented to participate in the parent study (N = 628), 120 were not eligible for longitudinal follow up because they were transferred, released, or bonded out before assessments could be completed. Of the 508 inmates enrolled in the longitudinal study, 86 people were disqualified because there were less than 6 weeks between intake and their release date and 12 people were considered not yet eligible for their pre-release assessment because they are still currently incarcerated. 410 inmates were eligible to be re-interviewed prior to their release from jail/prison (Time 2). Of these participants, we were unable to reach 116 participants in the allotted time frame for their Time 2 assessment (timed out), 5 refused to complete the assessment, 4 withdrew from the study, and one person did not have a release date, so was excluded, leaving 284 participants who completed a Time 2 assessment.
A total of 163 participants completed valid assessments of one or both of the stigma measures prior to release (Time 2). Because the stigma measures were added into the study after data collection had begun, 60 participants did not receive these measures. Due to study design/unexpected release, we collected an abbreviated version for 25 participants, and a missed version for 31 participants after the allotted time frame for the Time 2 assessment. Stigma measures were not included in these versions because they were collected after participants had been released, and therefore the prospective stigma measure did not make sense. An additional 5 people were excluded from analyses for having invalid data. Figure 1 shows a consort diagram for the Time 2 stigma measures. Participants (N = 163) were about 33 years old on average (range = 18.44 – 69.63) and primarily male (71.2%). This sample was racially/ethnically diverse (46.0% African American, 35.6% Caucasian, 6.1% Hispanic, 8.0% Mixed race/other race, 4.3% Asian/Pacific Islander).
Figure 1.

Sample retention from Time 1 to stigma measures. This figure illustrates a consort diagram of sample retention from participants enrolled at Time 1 to those who completed the stigma measures prior to release from jail/prison.
This paper focuses on pre-release (Time 2) and post-release (Time 3) data. Missing data were handled using Full Information Maximum Likelihood (FIML). Thus, we were able to analyze the entire sample of individuals (N = 371) who completed the post-release measures. FIML is highly encouraged when data are Missing at Random, which means that participants are not missing on items/variables for a reason that is relevant to the phenomenon being measured (Schafer and Graham 2002; Little et al. 2013). In our sample, missingness is largely due to factors related to study design. Specifically, missingness was due to unexpected release from the jail, which occurred for various participants throughout the course of the study (N = 56). Also, a proportion of data had already been collected at Time 2 before the stigma measures were introduced in our interview packet, resulting in missing data for 60 participants. In this case, the only identifiable variable related to missingness in our study was the date in which a person’s interview occurred; because participants were recruited into the study randomly, we do not think that this influences our missingness in any consistent way (Schafer and Graham 2002). All participants who had the opportunity to complete the stigma measures completed them; 5 individuals’ stigma data were invalidated because they were erroneously administered outside the allowable timeframe or due to indications of invalidity from the PAI validity scales.
To increase our confidence that our data were missing at random, we analyzed whether participants who completed the stigma measures were different in important ways compared to the participants who did not complete the stigma measures. Specifically, we conducted t-tests comparing participants who completed the stigma measures (N = 163) to those who did not (N = 121), on demographics and outcome variables. Results of t-tests show no significant differences on any demographic variables, suggesting the groups were equivalent in race, age, gender, and years of education completed. There were no significant differences on any outcome variables, suggesting that the groups were equivalent in levels of post-release employment, community functioning, substance dependence, and mental health symptoms. Because missing data was unrelated to the variables being measured in our study, as well as any other consistent variable, it was estimated during analyses.
The FIML technique is considered to be a more accurate approach to missing data than the commonly used listwise deletion method (Schafer and Graham 2002; Little et al. 2013). Listwise deletion of cases can strongly bias results because it deletes people who do not have complete data, which is not representative of the true population. It is almost impossible to predict whether listwise deletion will bias the results of any one study, and experts recommend not using the technique to avoid the possibility of bias (Schafer and Graham 2002). Further, FIML was designed for estimation of entire waves of data when one wave is present and the other is missing, for example, when you estimate Y for people who have X (Little and Rubin 1989). The same premise applies here, where we estimate X for participants who have Y. FIML uses all of the data available about a participant, including other measures at that timepoint (i.e. missing stigma data is estimated using other data on that person at Time 2) and outcome measures to determine the model parameters. Data values are not imputed in this technique, but rather the model parameters are estimated using all available information.
Figure 2 shows a consort diagram for Time 3 outcome measures. The sample analyzed in FIML was descriptively similar to the sample of 163 people (Mean age = 33, range = 18.40 – 69.63; 70.1% male; 45.6% African American, 35.6% Caucasian, 7.0% Mixed race/Other race; 6.5% Hispanic, 3.5% Asian/Pacific Islander, and additionally there were 0.8% Mexican American, 0.5% Middle Eastern, 0.5% Native American participants in this larger sample).
Figure 2.

Sample retention from Time 1 to FIML sample. This figure illustrates a consort diagram of sample retention from those enrolled at Time 1 to those who were analyzed with FIML analyses. The legend provides a detailed description of the sample.
Measures and Procedures
A battery of measures and demographic questionnaires were given at entry into the jail (Time 1); race was the only variable used from this timepoint. Other assessments relevant to this study were given prior to release from jail/prison (Time 2) and one year post-release (Time 3) timepoints. Time 2 assessments were conducted in the privacy of professional visiting rooms or secure classrooms, and included perceived stigma, shame-proneness, optimism, and criminal identity. Perceived and anticipated stigma were assessed with the Inmate Perceptions and Expectations of Stigma measure (IPES; Mashek et al. 2002) containing 12 items. Inmates were asked to indicate on a 7-point scale (“1” “totally disagree” to “7” “totally agree”) their perceptions of how people in society feel toward criminals—e.g. “People on the outside think criminals are bad people” (6 items; alpha = .83). Participants were then asked to indicate how they thought they would be treated once released –e.g. “People in the community will accept me” (4 items; alpha = .88). Previous factor analyses (Moore, Stuewig and Tangney 2013) indicated that this measure contained two factors: perceived stigma and anticipated stigma. Both scales were normally distributed (see Table 1) and significantly correlated (r = .36, p < .001).
Table 1.
Univariate Statistics
| N | Mean | SD | Skew | SE | Kurtosis | SE | Possible Range | Actual Range | |
|---|---|---|---|---|---|---|---|---|---|
|
Variable
| |||||||||
| Perceived Stigma | 162 | 4.30 | 1.20 | −.37 | .19 | .13 | .38 | 1.00–7.00 | 1.00–7.00 |
| Anticipated Stigma | 156 | 3.36 | 1.42 | .36 | .19 | .00 | .39 | 1.00–7.00 | 1.00–7.00 |
|
Moderators
| |||||||||
| Shame-proneness | 218 | 2.11 | .66 | .60 | .17 | −.15 | .33 | 1.00–5.00 | 1.00–4.08 |
| Connected w/Criminal Comm. | 167 | 2.60 | 1.65 | .75 | .19 | −.63 | .37 | 1.00–6.00 | 1.00–6.00 |
| Criminal Identity | 158 | 2.82 | 1.83 | .48 | .19 | −1.22 | .38 | 1.00–6.00 | 1.00–6.00 |
| Optimism | 215 | 3.89 | .61 | −.57 | .17 | 1.13 | .33 | 1.00–5.00 | 1.25–5.00 |
|
DVs
| |||||||||
| Recidivism | |||||||||
| SRa Arrests | 321 | .54 | .93 | 2.13 | .14 | 4.94 | .27 | 0–15.00 | 0–5.00 |
| SR Offenses | 319 | 1.07 | 1.46 | 1.72 | .14 | 3.56 | .27 | 0–15.00 | 0–9.00 |
| Official Arrests | 355 | .71 | 1.16 | 1.84 | .13 | 3.31 | .26 | 0–15.00 | 0–6.00 |
| Substance Dep. Sxs | |||||||||
| Alcohol | 320 | .54 | .92 | 1.95 | .14 | 2.92 | .27 | 0–4.00 | 0–3.78 |
| Marijuana | 318 | .21 | .55 | 3.34 | .14 | 12.19 | .27 | 0–4.00 | 0–3.50 |
| Cocaine | 317 | .57 | 1.18 | 1.95 | .14 | 2.28 | .27 | 0–4.00 | 0–4.00 |
| Opiates | 318 | .24 | .83 | 3.52 | .14 | 11.11 | .27 | 0–4.00 | 0–3.97 |
| Hard drugsb | 318 | .69 | 1.29 | 1.62 | .14 | .97 | .27 | 0–4.00 | 0–4.00 |
| Mental Health Sxs | |||||||||
| Depression | 256 | 54.85 | 11.06 | .69 | .15 | .14 | .30 | 30–110 | 36–90 |
| Anxiety | 256 | 52.77 | 10.93 | .88 | .15 | .62 | .30 | 30–110 | 34–89 |
| BPD Featuresc | 138 | 61.05 | 12.61 | .23 | .21 | −.33 | .41 | 30–110 | 36–94 |
| Stress | 255 | 59.26 | 11.72 | .23 | .15 | −.68 | .30 | 30–110 | 37–91 |
| Community Adjust. | |||||||||
| # Hrs Employed | 270 | 1081.56 | 745.54 | −.22 | .15 | −1.53 | .30 | 0–1920 | 0–1920 |
| Comm.Functioning | 319 | .39 | .18 | .05 | .14 | −.74 | .27 | 0–1 | 0–0.86 |
SR = Self-reported.
Cocaine and opiate variables had low variance and were skewed due to few participants reporting dependency symptoms, so they were combined (hard drugs) and analyzed.
The BPD Features scale was entered into the study late, therefore fewer participants received it.
Note: 163 participants completed either stigma measure; one person who completed anticipated was missing on perceived stigma, 7 people who completed perceived were missing on anticipated stigma.
Shame-proneness was assessed using the Test of Self-Conscious Affect-Socially Deviant (TOSCA-SD; Hanson and Tangney 1996). The TOSCA-SD is composed of 13 scenarios followed by a series of possible responses. Participants rated how likely they would be to respond in ways described (capturing shame and guilt responses). This measure has been shown to be reliable and valid with offenders (Tangney et al. 2011). The shame-combined scale, including negative self-appraisal responses (e.g. “You would think, I’m inconsiderate”) and behavioral avoidance responses (e.g. “You would leave as quickly as you could”), was used for these analyses. The TOSCA-SD shame-proneness scale had acceptable reliability (alpha = .77) and was normally distributed (see Table 1). Optimism was assessed using 6 items from the Values in Action inventory (VIA; Peterson and Seligman 2001). This scale has been shown to be reliable and valid with inmates (Heigel, Stuewig, and Tangney 2010). This scale assessed trait optimism (e.g. “I can always find the positive in what seems negative to others”). Responses were rated on a 5-point Likert scale where “1” was “not at all like me” and “5” was “very much like me” (alpha = .77). This scale was normally distributed (see Table 1).
Two aspects of social identity were assessed. The Inclusion of Community in Self scale (ICS; Mashek, Cannaday, and Tangney 2007) assessed actual and desired connectedness with various target groups including the family, the criminal community, and the community at large. Responses were rated using six figures of circles overlapping to various degrees (representing not at all connected to as connected as possible). The item asking participants about their actual connectedness with the criminal community was used in the current analyses. The ICS has been determined to be valid with inmates, though test-retest data was not available to assess reliability (Mashek et al. 2006). About 37 percent of participants indicated no connectedness to the criminal community, slightly skewing this variable (see Table 1). Participants were also asked to what degree they agreed with the statement “I am a criminal” on a 6-point Likert scale from “1” “totally disagree” to “6” “totally agree.” This variable was slightly kurtotic due to a concentration of data points at the low (especially) and high ends of the scale (see Table 1).
Time 3 assessments were conducted by phone or (for those re-incarcerated) in person one year after inmates were released from jail/prison, and included employment, recidivism, mental health symptoms, substance dependence symptoms, and community functioning. Employment was assessed by asking participants whether they were unemployed, or had odd jobs, part-time (less than 35 hours), or full-time employment (more than 35 hours) in the year after release from jail, and how many weeks they worked in that year. The majority of participants (67.1%) reported having full-time employment in the year after release. A continuous variable (total hours employed) was created by multiplying the number of hours expected for the type of employment (i.e. typical number of hours worked in full-time employment in the U.S. is 40 hours, part-time employment is 20 hours, and odd jobs is 5 hours) by the number of weeks participants were employed in the year after release. The distribution covered the full range and showed minimal skewness and kurtosis (see Table 1), although there were substantial clusters at the extreme ends of the distributions reflecting unemployed and full-time employed participants.
Recidivism was assessed by both self-report and official records. Participants were asked whether they had been arrested for (self-reported arrests) and whether they had committed without being detected (self-reported offenses) each of 16 types of crime (i.e. theft, robbery, assault, murder, domestic violence, weapons offenses, major driving offenses, prostitution, drug offenses, sex offenses, fraud, kidnapping, arson, resisting arrest, miscellaneous, and other) during the year after their release. Official National Crime Information Center (NCIC) criminal records of arrests in the first year after release were collected as well (official arrests); 119 charge codes found on official records were categorized into the 16 types of crimes used for the self-report variables. To capture criminal versatility in these three sources, three variables were created to reflect the number of types of crimes (i.e. 0–16) that participants were arrested for (official arrests and self-reported arrests) and reported committing (self-reported offenses). Versatility (the number of different types of crimes) was employed rather than the frequency of arrest/offense because the latter is confounded by the type of crime, e.g., illegal substance use vs. violent offenses. The actual range for these variables were 0–5 for self-reported arrests, 0–6 for official records of arrest, and 0–9 for self-reported offenses. Because many participants reported/were found to have zero arrests and reported committing zero offenses, each variable was skewed (see Table 1).
Eight items representing community participation/functioning were chosen from a measure of detailed demographic information given at the one year post-release assessment. Items included 1) residential stability, 2) homeownership, 3) current marital status, 4) largest source of support in the past year (i.e. job, family/spouse, friends, illegal activities, unemployment benefits, etc.), 5) valid driver’s license, 6) financial support of children, 7) educational and vocational upgrades (i.e. taking vocational or college courses, graduating high school, getting GED, etc.), and 8) volunteerism in the community. Participant responses on each of the eight items were evaluated in terms of the level of adaptive functioning. We used the criminology literature to indicate certain responses as being adaptive, prosocial behaviors that are particularly useful for offenders’ reintegration in the community. All other behaviors, including maladaptive ones and even neutral ones that could be adaptive or maladaptive depending on the situation, were considered fundamentally different and placed in another category.
Responses deemed to be adaptive were given a score of 1, and those that were either neutral or maladaptive were given a score of 0. Specifically, for residential stability, living in 1 or 2 places in the year post-release was considered adaptive and living in more than 2 places or being homeless was considered neutral/maladaptive. There is a general consensus in the literature of measuring residential stability with the number of places lived. For current marital status, being legally married was the only response considered adaptive. Social control theory (in criminology) states that the act of being legally married to someone is a community convention that is fundamentally different from other forms of cohabitation or relationships (Sampson and Laub 1993). It is believed that this represents a prosocial bond to the community that is not observed in cohabitating couples or other types of romantic relationships.
For largest source of financial support, a job or savings was considered adaptive and all other responses were considered neutral (i.e., family, spouse) or maladaptive (i.e. illegal activities). Research in criminology places great importance on the employment of ex-offenders after release from jail, and supporting oneself through a job or savings is considered the primary prosocial form of financial support. For financial support of children, supporting all of their children or more than their own children (i.e. a partner’s children) was considered adaptive, not having children was considered neutral, and failing to financially support all of their children was considered maladaptive. In regards to supporting one’s children, we do not think of it as penalizing those without children, but rather giving credit to those with children who also financially support their children. For educational and vocational upgrades, participating in any of the upgrades was considered adaptive and not participating in any was considered neutral/maladaptive. On yes/no questions, participants who reported owning their own home, having a valid driver’s license, or volunteering in the community in the past year were given a score of 1 (adaptive) on those respective items. Scores were averaged across the eight dichotomous indicators to create a total functioning index. Because this is a formative construct composed of different areas of functioning that are not necessarily expected to be correlated with one another (i.e. having a valid driver’s license may not necessarily be linked to financially supporting one’s children), Cronbach’s alpha was not calculated.
Levels of mental health symptoms were assessed with a shortened version of the Personality Assessment Inventory (PAI; Morey 2007), which included four scales: depression (DEP), anxiety (ANX), borderline features (BPD), and stress (STR). Item responses ranged from 1 = “False, not at all true” to 4 = “Very true.” These scales use T-scores, which are normed on a sample of average adults; the ranges for each scale were 36T–90T for depression (24 items, α = .85), 34T–89T for anxiety (24 items, α = .89), 36T–94T for borderline features (24 items, α = .88), and 37T–91T for stress (8 items, α = .74). The PAI is a widely used, well-validated measure (Morey 2007). These scales were all normally distributed (see Table 1).
Using Simpson and Knight’s (1998) Texas Christian University: Correctional Residential Treatment Form, Initial Assessment (TCU-CRTF), four substance dependence scales were created to capture symptoms of dependency on alcohol, marijuana, cocaine, and opiates in the first year post-release. Each variable was composed of items that assess each of the DSM-IV-TR substance dependence domains. Item responses ranged from 0 = “Never” to 4 = “7 or more times.” Responses were averaged within domain and a total score was computed by taking the mean across the seven domains (six in the case of marijuana because withdrawal is not considered part of the criteria). Each scale had acceptable reliability (alcohol, 7 items, α = .93; marijuana, 6 items, α = .88; opiates, 7 items, α = .97; cocaine, 7 items, α = .98). Given the similarities between cocaine and opiates (illegal, highly addictive) and the low rate of opiate use in our sample, opiates and cocaine were combined into a category of hard drugs. Frequency and dependence of cocaine/opiate use was defined as the higher of the two ratings for either cocaine or opiates. As there were a large number of people with very few dependency symptoms, each variable was skewed (see Table 1). The TCU has been shown to be reliable with jail inmates (Stuewig et al. 2009).
RESULTS
Measurement Model for Post-Release Functioning
Correlations for the independent variables and moderators with the dependent variables are presented in Table 2. Prior to testing the structural model, we examined the measurement model for the outcomes. We created four latent variables (indicated with capital letters) to capture these outcomes: Recidivism was composed of self-reported arrests, official records of arrests, and self-reported undetected offenses; Substance Dependence Symptoms was composed of alcohol dependence, marijuana dependence, and hard drug dependence (cocaine and opiate dependence); and Mental Health Symptoms was composed of depression, anxiety, borderline personality disorder features, and stress scales. Community Adjustment was composed of employment and the community functioning index (i.e. residential stability, homeownership, marital status, driver’s license, volunteerism, educational upgrades, and financial support of children).
Table 2.
Bivariate Relationships.
| Perceived Stigma | Anticipated Stigma | Connected w/ Criminal Community | Criminal Identity | Shame-proneness | Optimism | |
|---|---|---|---|---|---|---|
|
IVs and Moderators
| ||||||
| Perceived Stigma | 1.00 | .33** | .21* | .09 | .01 | −.03 |
| Anticipated Stigma | .33** | 1.00 | .12 | .10 | .12 | −.19* |
| Connected with | ||||||
| Criminal Comm. | .21* | .12 | 1.00 | .17* | .02 | −.04 |
| Criminal Identity | .09 | .10 | .17* | 1.00 | .13 | −.26* |
| Shame-proneness | .01 | .12 | .02 | .13 | 1.00 | −.26** |
| Optimism | −.03 | −.19* | −.04 | −.26** | −.26** | 1.00 |
|
| ||||||
|
DVs
| ||||||
| Recidivism | ||||||
| SR1 Arrests | .12 | −.08 | .14 | .15+ | .05 | −.04 |
| SR Offenses | .05 | −.06 | .12 | −.05 | −.02 | −.10 |
| Official Arrests | −.04 | .02 | .26* | .12 | .03 | −.02 |
| Substance Dep. Sxs | ||||||
| Alcohol | −.05 | .02 | −.14 | .02 | .12 | −.24* |
| Marijuana | −.03 | .09 | .11 | −.08 | −.01 | −.03 |
| Hard drugs | −.15+ | −.13 | −.14 | −.07 | .12 | −.07 |
| Mental Health Sxs | ||||||
| Depression | −.11 | .01 | −.04 | .23* | .33** | −.38** |
| Anxiety | −.26* | −.02 | −.07 | .09 | .38** | −.41** |
| BPD Features | −.28* | .01 | −.15 | .07 | .41** | −.50** |
| Stress | −.12 | .04 | −.04 | .17+ | .23* | −.25* |
| Community Adjust. | ||||||
| # Hrs Employed | .07 | −.10 | −.02 | −.12 | −.24* | .08 |
| Community Functioning | −.16+ | −.23* | −.08 | −.38** | −.17* | .23* |
p < .10,
p < .05,
p < .001, two-tailed tests
SR = Self-reported
Note: Ns range from 63 to 219 due to missing data on IV measures (i.e. BPD Features: N = 65, perceived and anticipated stigma: N = 168).
Note: Only correlations for IVs and moderators with DVs are presented. Correlations among DVs are not shown.
All missing data was assumed to be missing at random. Missing data were handled using the Full Information Maximum Likelihood (FIML) estimation method, a model-based estimation technique that is widely accepted and used in structural equation modeling analyses (Graham, Cumsille, and Shevock 2013). In this study, only 163 participants completed the stigma measures prior to release, and 131 of these participants completed the one-year post-release assessment. Using FIML, we were able to analyze the entire sample of individuals who completed the post-release outcome measures in addition to those participants who completed the stigma measures at pre-release. This total number of participants analyzed was 371.
The measurement model was run with the four latent dependent variables, and included intercorrelations among all latent variables. The latent variables were identified using the marker variable method (Kline 2005). The model fit was acceptable according to model fit criteria (χ 2 (48) = 141.72, p = 0.00; RMSEA = .07 with 90% CI .06 to .09, CFI = .92, SRMR = .07). Factor loadings of indicators ranged from .48 to .89 and all loaded significantly onto the respective latent variables. Examination of residuals and modification indices suggested that model fit would greatly improve with the addition of a correlated residual between official records of arrest and self-reported arrests. This made sense because both share specific/unique variance on arrests as opposed to undetected offenses, and was considered acceptable based on research supporting correlated residuals for shared specific/unique variance among variables (Kline 2005). This correlated residual was added and this model fit the data significantly better than the previous model (χ 2 (47) = 103.82, p < .001; RMSEA = .06 with 90% CI .04 to .07, CFI = .95, SRMR = .06; χ2 (1) Δ = 37.9, p < .001). Based on model fit criteria, this model fit the data well. Factor loadings ranged from .47 to .88 and loaded significantly on their respective latent variables. On Recidivism, Mental Health Symptoms, and Substance Dependence, higher scores indicated worse functioning, whereas higher scores indicated more adaptive functioning on the Community Adjustment latent variable. All latent variables were significantly correlated within the model (see Figure 3); Substance Dependence and Recidivism were very highly correlated (r = .87, p < .001). This was attributed to self-reported undetected offenses, which can heavily reflect illicit drug use, driving the recidivism variable after self-reported arrests and official records of arrest residuals were correlated. The measurement model was also run on the smaller sample of individuals who all completed the stigma measures (N = 163), and there were no significant differences in model fit or factor loadings.1
Figure 3.

Measurement model (N = 367). This figure illustrates the measurement model including the four latent dependent variables of Recidivism, Substance Dependence Symptoms, Mental Health Symptoms, and Community Adjustment. The legend provides information on fit indices in MPLUS.
Mediation through Anticipated Stigma
We tested the structural model, involving a mediated pathway from perceived stigma to all latent variable outcomes, through anticipated stigma. For the same reasons as stated above, we used Full Information Maximum Likelihood (FIML) estimation to utilize the full one year post-release sample (N = 371) in structural analyses. We hypothesized that perceived stigma would be positively related to anticipated stigma, which would in turn predict more Recidivism, Mental Health Symptoms, and Substance Dependence, and lower Community Adjustment.
We ran a model where perceived stigma predicted anticipated stigma, and anticipated stigma predicted the four latent outcomes. We tested the indirect relationship from perceived stigma to each latent outcome through anticipated stigma using the model indirect command in MPLUS (see Figure 4). This model had acceptable fit (χ 2(67) = 137.20, p < .001; RMSEA = .05 with 90% CI .04 to .07, CFI = .94, SRMR = .07). Perceived stigma was positively related to anticipated stigma (β = .33, p < .001). Anticipated stigma did not significantly predict Recidivism (β = −.06, p = .56), Substance Dependence Symptoms (β = −.03, p = .78), or Mental Health Symptoms (β = −.01, p = .92), but it did significantly predict Community Adjustment (β = −.23, p = .02). The indirect pathway from perceived stigma to Community Adjustment through anticipated stigma was significant as well (β = −.08, p = .04). This indicates that higher perceived stigma predicted more anticipated stigma, which predicted worse functioning in the community. To investigate whether there was evidence of a true mediating effect, the direct effect from perceived stigma to Community Adjustment was tested. The direct path from perceived stigma to Community Adjustment was nonsignificant (β = −.09, p = .36), therefore, there was not necessarily evidence of a mediating effect (because the exogenous and dependent variables were not significantly related), but rather an indirect effect (Preacher and Hayes 2004). Bias-corrected bootstrapping was used on standard errors and confidence intervals of the indirect effect; the indirect effect after bootstrapping was marginally significant (β = −.01, p = .10) and the 90% confidence interval did not include zero (CI = −.021 to −0.002), meaning that we can confidently conclude that the indirect effect is different from zero (Shrout and Bolger 2002).
Figure 4.
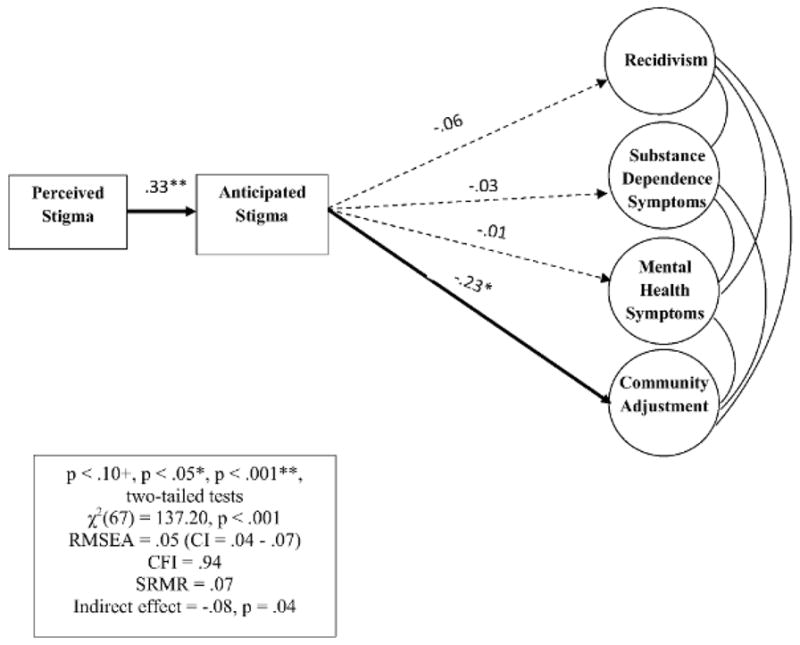
Mediation model (N = 371). This figure illustrates the final mediational model of perceived stigma through anticipated stigma to the four latent outcomes. Latent correlations are not shown for ease of viewing; all were significant. The legend provides information on fit indices in MPLUS.
Overall, perceived stigma accounted for 10.6% of the variance in anticipated stigma, while the model accounted for 0.4% of the variance in Recidivism, 0.0% of the variance in Mental Health Symptoms, 0.1% of the variance in Substance Dependence, and 5.4% of the variance in Community Adjustment. This mediation model was also run for the smaller sample of 163 people who all completed the stigma measures, and there were no significant differences between parameter estimates or model fit.2
Moderators
We hypothesized that perceived stigma and anticipated stigma would be more strongly linked for highly shame-prone inmates, those with a stronger criminal identity, and those highly connected to the criminal community, and less strongly linked for highly optimistic and minority inmates. We hypothesized that anticipated stigma and post-release outcomes would be less strongly linked for highly optimistic and minority inmates. We analyzed continuous moderators (i.e. shame-proneness, criminal identity, connectedness to the criminal community, optimism) by centering each variable and then multiplying it by perceived or anticipated stigma to create an interaction term that was then entered as a predictor. We used a multiple-group test to analyze moderation by race.
Moderators of perceived stigma to anticipated stigma link
We tested moderation of the link between perceived and anticipated stigma. Each continuous moderator of this path was tested in a separate model. Neither connectedness to the criminal community (β = .08, p = .35) nor having a criminal identity (β = .10, p = .21) predicted or interacted with perceived stigma to predict anticipated stigma. There was no significant interaction between perceived stigma and shame-proneness in predicting anticipated stigma (β = −.11, p = .16). Optimism had a significant main effect on anticipated stigma (β = −.18, p = .02), but the interaction was not significant (β = −.02, p = .77).
Moderators of anticipated stigma to outcomes
We hypothesized that even if inmates anticipated stigma, those who were highly optimistic may not experience poor functioning. We multiplied optimism by anticipated stigma to create an interaction term that was entered as a predictor of each latent outcome. Optimism had a significant main effect on Mental Health Symptoms (β = −.46, p < .001) and Community Adjustment (β = .20, p = .02), and a marginal main effect on Substance Dependence (β = −.18, p = .07). In no case was the interaction term significant. The model in Figure 4 generalized across inmates who varied in shame-proneness, criminal identity, connectedness to the criminal community, and optimism.
Multiple group test of race
A multiple group test was conducted to test whether the model varied significantly by race. Race was coded as 0-Caucasian (N = 132), 1-African American (N = 171); there were too few other races to include as a separate group. First, we ran a multiple group test of the measurement model to determine whether factor loadings and intercepts were comparable across races. Chi square difference tests were computed to compare the models. The fully unconstrained model was not positive definite for Caucasians because undetected offenses loaded too highly on the Recidivism latent variable; this parameter was fixed to 1 in order for the model to run properly. Results showed that the model with factor loadings and intercepts constrained to be equal (χ 2 (110) = 187.91, p < .001; RMSEA = .07 with 90% CI .05 to .09, CFI = .93, SRMR = .09) was not significantly different from the unconstrained model (χ 2 (95) = 168.16, p < .001; RMSEA = .07 with 90% CI .05 to .09, CFI = .93, SRMR = .08; χ 2 (15) Δ = 19.75, p > .05), meaning factor loadings and intercepts were comparable across races.
We then included the structural pathways in the multiple group test, while constraining the factor loadings and intercepts of the measurement model (see Figure 5). We used the chi square difference test to compare the model with all structural pathways free to vary, to a model with all structural pathways constrained to be equal across groups. Results showed that the model with all structural pathways free to vary fit the data acceptably (χ 2 (152) = 273.54, p < .001; RMSEA = .07 with 90% CI .06 to .09, CFI = .89, SRMR = .13), but fit was worse when all structural pathways were constrained to be equal (χ 2(157) = 283.01, p < .001; RMSEA = .07 with 90% CI .06 to .09, CFI = .89, SRMR = .14; χ 2 Δ(5) = 9.47, p < .10). This suggests that there are notable differences between Caucasians and African Americans for pathways in the structural model. To determine specific pathway differences, one structural path at a time was made free to vary in the fully constrained model, and chi square differences were calculated comparing each new model to the fully constrained model. Two pathways significantly improved model fit when freed to vary across groups.
Figure 5.

Multiple group test. This figure shows the unconstrained model where all structural pathways were free to vary among Caucasian (N = 132) and African American (N = 169) inmates. This model fit significantly better than the model in which all of the structural pathways were constrained to be equal. The individual pathways that significantly varied between the two groups were from perceived to anticipated stigma, and from anticipated stigma to Community Adjustment. The factor loadings and intercepts of the measurement model are all constrained.
The pathway from perceived to anticipated stigma differed as a function of race, with marginally improved model fit when free to vary (χ 2(156) = 279.76, p < .001; RMSEA = .07 with 90% CI .06 to .09, CFI = .89, SRMR = .13; χ 2 (1) Δ = 3.25, p < .10). For Caucasians, perceived stigma predicted more anticipated stigma (β = .39, p < .001); this pathway accounted for 15% of the variance in anticipated stigma. For African Americans, the pathway from perceived to anticipated stigma was smaller in magnitude (β = .32, p < .001), and accounted for 9.9% of the variance in anticipated stigma.
The pathway from anticipated stigma to Community Adjustment was then freed to vary across groups. It also differed as a function of race, with marginally improved model fit when free to vary (χ 2 (155) = 276.92, p < .001; RMSEA = .07 with 90% CI .06 to .09, CFI = .89, SRMR = .13; (χ 2 (2) Δ = 2.84, p < .10). For Caucasian inmates, anticipated stigma predicted less Community Adjustment (β = −.47, p = .001), and this pathway accounted for 22.2% of the variance in Community Adjustment. The indirect effect from perceived stigma to Community Adjustment was significant (β = −.18, p = .01). When bootstrapped, the indirect effect remained significant (β = −.03, p = .02), and the 90% confidence interval did not include zero (CI = −.08 – −.03), allowing us to conclude that for Caucasian inmates, the indirect effect from perceived stigma to Community Adjustment is different from zero. For African American inmates, the pathway from anticipated stigma to Community Adjustment was nonsignificant (β = −.18, p = .25), and only accounted for 3.1% of the variance in Community Adjustment. The indirect effect from perceived stigma to Community Adjustment for African Americans was also nonsignificant (β = −.06, p = .27). This model, where the pathways from perceived stigma to anticipated stigma, and from anticipated stigma to Community Adjustment were free to vary, fit significantly better than the model in which all pathways were constrained (χ 2 (2) Δ = 6.09, p < .05).
DISCUSSION
Perceived Stigma Predicts Community Adjustment after Release
This study showed that higher perceptions of stigma toward criminals prior to release predicted poorer adjustment in the community (e.g., community functioning, employment) indirectly through anticipated stigma. Thus, perceiving stigma toward criminals impacts offenders’ ability to function in the community via the expectation of personally experiencing discrimination from community members. It is worth noting that there was no direct effect of perceived stigma on Community Adjustment. Current thinking is that the independent variable does not necessarily have to be related to the dependent variable to conclude mediation/indirect effects (MacKinnon, Fairchild, and Fritz 2007). The lack of direct effect suggests that just being aware of stereotypes toward criminals does not in and of itself prevent offenders from engaging in the community. Perceived stigma affects offenders’ community adjustment when it leads to the anticipation of personally experiencing stigmatization.
Researchers in criminology and psychology can further investigate psychological aspects of the stigma process among offenders to better understand its effect on behavior. Specifically, it may be useful to consider coping strategies (as is specified in Modified Labeling Theory); research has shown that perceived stigma predicts negative outcomes through social withdrawal/avoidance (Perlick et al. 2001). It could be that recently released inmates who perceive a great deal of stigma and personally expect stigmatization withdraw from community activities, leading to poor community functioning and lower employment. Similarly, former inmates who anticipate a great deal of stigma may have less motivation/self-efficacy to attain employment and be involved in their communities (i.e. own a home, volunteer). This may reflect the “why try?” effect, such that anticipating stigma discourages people from trying to integrate in society (Corrigan et al. 2010: 56). Future research should incorporate social withdrawal and motivation/perseverance into the model tested here.
Race Differences in the Implications of Stigma
The pathway from perceived to anticipated stigma, and anticipated stigma to Community Adjustment significantly varied by race. For Caucasian inmates, perceived stigma predicted more anticipated stigma, which predicted worse community adjustment. For African Americans, perceived stigma was less predictive of anticipated stigma, and anticipated stigma did not significantly predict community adjustment. This suggests that when Caucasian and African American inmates perceive stigma toward criminals, they are both likely to expect stigmatization, but that these expectations have different implications for adjustment.
These race differences are consistent with criminology and psychology theories suggesting that African Americans and other minorities, having had to manage racial discrimination, do not experience as many negative effects resulting from the perception of additional stigmas (Winnick and Bodkin 2009). It may be that people with multiple stigmas have developed skills for coping with stigma; Crocker and Major (1989) argue that racial minorities and certain other stigmatized people can protect their self-esteem, for instance, by attributing rejection experiences to discrimination rather than an internal quality of themselves. So, when African American inmates anticipate stigma for having a criminal record, it may have minimal effect on their cognitions, emotions, or behavior if they attribute fault to the outgroup or to discrimination. This, then, may not lead to difficulties adjusting to the community after release.
Research also supports the idea that non-minority groups experience more negative effects from stigma compared to minority groups because solely having a concealable stigmatized identity is thought to cause more distress in people than having an obvious identity, or both an obvious and concealable identity causes (Frable et al. 1998). Specifically, people with concealable identities (i.e. mental illness, criminal record) must manage the anxiety of whether to disclose their identity to others, a decision that must be made in various contexts, some of which could seriously impact life opportunities (Quinn 2006; Pachankis 2007). Caucasian inmates who anticipate a great deal of stigma may be especially at risk for difficulties adjusting to the community after release, as decisions about disclosure of their criminal record may inhibit them more than African American inmates from engaging in their community.
One alternative explanation for these findings is that on average, African American inmates perceive and anticipate less stigma than Caucasian inmates, and therefore do not experience as many negative outcomes. However, we examined mean differences in perceived and anticipated stigma for gender, race, years of education, and age, and found no significant differences (Moore et al. 2013). Another alternative explanation for these findings may be that African American offenders are functioning worse at the one year post-release timepoint than Caucasian offenders on average, and have less variance in the outcomes, causing no relationship between African Americans’ perceived stigma and outcomes (i.e. floor effect). Research does show that Caucasians with a criminal record are more likely to be employed over African Americans with a criminal record (Pager, Western, and Sugie 2009). We examined this by conducting t-tests by race to assess for differences in the outcome variables. There were no instances of unequal variance, mean differences, or differences in actual range on any outcome variable. African American and Caucasian inmates were functioning at the same level on average across domains, and had equal variance in the outcomes, lending more support to differential effects of stigma on post-release community adjustment found in this study.
Stigma and Recidivism, Substance Dependence, and Mental Health Symptoms
Perceived stigma did not predict recidivism, substance dependence symptoms, or mental health symptoms through anticipated stigma. This suggests that perceived and anticipated stigma have a unique relationship with different indices of functioning for offenders, and may not be robustly associated with negative outcomes in all areas. Offenders are a diverse group of individuals, some of whom may not identify as “criminals.” This may be especially true of people incarcerated for drug offenses or for crimes influenced by symptoms of mental illness (e.g. manic or psychotic episode). For these people, perceiving stigma toward criminals may not create or exacerbate existing mental health symptoms.
Alternatively, criminal offenders may be a unique stigmatized population in that the self may somehow be more protected from stigma compared to other stigmatized groups. For example, offenders who are highly connected to other offenders (i.e. antisocial friends/family, antisocial values) may perceive and anticipate stigma, but not care about it and not experience resulting distress. Ingroup cohesion/connectedness is in fact thought to act as a protective factor for stigmatized people’s mental health, as there is a sense of safety and belonging with the ingroup, providing people with self-esteem and less ambiguity about their place in society (Eccleston and Major 2006). To test this post-hoc hypothesis, we created an interaction term between anticipated stigma and connectedness to the criminal community, and entered this into the pathway from anticipated stigma to Mental Health Symptoms. Connectedness to the criminal community did not significantly predict Mental Health Symptoms (B = −.08, p = .43), nor did the interaction (β = −.01, p = .95). This highlights the importance of understanding the impact (or lack thereof) that stigma has on the self in offenders. Future research should examine internalized stigma and self-esteem in this population to understand how stigma is related to offenders’ mental health.
Perceived and anticipated stigma did not predict substance dependence or recidivism. Again, we post-hoc hypothesized that offenders who are highly connected with other offenders may perceive and anticipate stigma, and subsequently engage in more antisocial behavior. Criminology researchers suggest that for highly antisocial networks, stigma may push these individuals farther away from the community at large, and closer to other offenders (Braithwaite 1989), which may cause further criminal behavior. Further, strong group identification with other offenders is linked to more anticipated stigma and perceived stigma (Benson et al. 2011; LeBel 2012). To test this, we created another interaction term of anticipated stigma and connectedness to the criminal community to predict Recidivism. Connectedness to the criminal community did significantly predict higher recidivism (β = .32, p = .002), but the interaction was not significant (β = .051, p = .65). Aside from this, it is very likely that other coping and identity variables can explain these relationships.
It is worth mentioning that our substance dependence outcome variables were created based on the presence of DSM-IV symptoms for substance dependence disorders, and therefore did not include symptoms of substance abuse, which are now combined into a single category with dependence symptoms in DSM-V. That is, our variables captured the degree to which individuals had experienced each possible symptom of tolerance, withdrawal, consuming larger amounts of the substance than usual, persistent desire to cut down on use, spending a great deal of time obtaining/using the substance, giving up important activities in order to use the substance, and persistent substance use despite the problems it causes. DSM-V symptoms of substance abuse (which we did not include) involve failing to fulfill major roles, engaging in physically hazardous behavior, interpersonal/social problems caused by substance use, and cravings for the substance. Therefore, our substance use outcome variables capture more severe substance use issues than would be captured using the new, more inclusive criteria for these disorders. We think this is appropriate for our sample, given the generally high rates of substance use in incarcerated populations. Further, substance abuse and dependence are correlated at .87 for alcohol, .73 for marijuana, .90 for cocaine, and .90 for opiates in our sample. Therefore, our results would most likely generalize under DSM-V criteria.
Summary of Key Findings
In sum, perceived stigma prior to release can have serious implications for offenders’ functioning once released from jail/prison. Participation as a member of one’s community (i.e. residential stability, owning a home, having a driver’s license, supporting children, volunteering) is essential for the successful reentry of offenders after release from jail. The dynamics of stigma and adjustment are complex and appear to vary by race/ethnicity. For African Americans, who have coped with the visible stigma of being a minority, recognition that they may be further stigmatized by the (often concealable) stigma of having a criminal record may not carry the same negative consequences as it does for Caucasian inmates who may not have previous experience with stigma. African Americans may be inoculated to the impact of additional stigma, and may have developed positive coping strategies that Caucasians are less likely to draw upon. This underscores the importance of race in future research with any stigmatized group.
Limitations
Data were provided by inmates held on felony charges in one jail, potentially limiting generalizability to inmates who are charged with less serious crimes, incarcerated in other geographic locations, and incarcerated in state and federal prisons. Although perceived stigma theoretically occurs before anticipated stigma, temporal precedence was not obtained, as these variables were both measured prior to release. Because of this, results must be interpreted with some caution. This study suffered from limited power to test more complex moderator hypotheses. For example, because race is an important factor in how stigma is managed, shame-proneness, optimism, and criminal identity may operate differently for Caucasians and African Americans (i.e. optimism is important for one race but not the other). This sample size did not allow tests of such complex interactions. Because coping variables were not measured, we were unable to test whether coping might mediate the relationship between anticipated stigma and indices of post-release functioning, as is suggested by stigma theory (Link et al. 1989). These are directions for future research.
Criminal offenders are a diverse group and may possess multiple stigmatized identities in addition to that of being a criminal offender. For example, criminal offenders may possess stigmatized identities related to race, disability, mental illness, addiction, or HIV status. The study of having multiple stigmatized identities, referred to as intersectionality, is in the early stages and therefore the implications for behavior are not well understood. We did not have assessments of other stigmatized identities in this study, and therefore, could not examine perceived and anticipated stigma related to any other stigmatized identity. This is a limitation of our paper, as possessing multiple stigmatized identities may certainly affect how one feels about being a criminal offender. Intersectionality is an important direction for future research when examining criminal offender stigma.
Social Policy and Clinical Implications
Broadly, society would benefit from careful reconsideration of structural, stigma-inducing state and federal policies (e.g. prohibitions on voting, ineligibility for tuition assistance, housing and employment restrictions), which not only limit positive community opportunities for ex-offenders, but also communicate that ex-offenders remain excluded from the law-abiding community at large. That said, the reality is that many offenders will face significant structural and social barriers to community involvement after release, and they must learn to modulate psychological responses to these barriers in order to be successful in the community. Regarding clinical interventions, post-release success may be enhanced by providing correctional treatment services for inmates targeted at reducing anticipated stigma and adjusting expectations for community reentry. Interventions have just begun to target the harmful effects of stigma, such as self-stigma/internalized stigma. For example, acceptance and commitment therapy has been used in self-stigma interventions, and seems promising (Livingston et al. 2012). Group interventions drawing upon cognitive-behavioral principles that challenge discrimination expectancies and increase community involvement (among other skills) have shown significant decreases in internalized stigma (Lucksted et al. 2011). Programs that target negative expectancies and aim to enhance prosocial community ties could be adapted for correctional facilities; such programs would likely be beneficial in preparing offenders to reenter the community.
Acknowledgments
This research was supported by Grant #R01 DA14694 from the National Institute on Drug Abuse to June P. Tangney and Grant #5F31DA035037-02 from the National Institute on Drug Abuse to Kelly E. Moore. Many thanks to the members of the Human Emotions Research Lab for their assistance with this research, and the inmates who participated in this research.
Biographies
Kelly Moore is a graduate student in the Clinical Psychology Ph.D. program at George Mason University. Her research interests include offender populations, the psychological and behavioral implications of being in a stigmatized group, and barriers to community reentry after incarceration.
Jeff Stuewig is a research associate professor in psychology at George Mason University. His research interests include shame, guilt, substance abuse, violence, and risky behavior over the life course.
June Tangney is a University Professor and Professor of Psychology at George Mason University. Her research interests include moral emotions and cognitions, strengths and virtues, and interventions with offenders.
Footnotes
To assess for considerable differences obtained with FIML analysis, this measurement model was also run with the original sample of individuals who completed the stigma measures (N = 163). Similar fit was obtained (χ 2 (47) = 87.66, p < .001; RMSEA = .07 with 90% CI .05 to 1.0, CFI = .91, SRMR = .08) and there were no large differences in factor loadings between the two samples. In the analysis of the smaller sample, only one factor loading noticeably decreased (marijuana dependence on Substance Dependence factor was .39 in sample of 163, but was .47 in FIML sample). Somewhat lower loadings are to be expected given the reduced power available in the smaller sample. Further, this loading was the lowest among factor loadings in both samples. Otherwise, loadings ranged from .48 to .90 and all loaded significantly onto their respective factors. All factor correlations were in the same direction as those in the FIML sample and remained significant in the smaller sample.
To assess any differences obtained with FMIL analysis, the mediation model was run on the smaller sample of people who all completed the stigma measures (N = 163). Model fit was consistent (χ 2(67) = 120.77, p < .001; RMSEA = .07 with 90% CI .05 to .09, CFI = .89, SRMR = .08) with that obtained in FIML and there were no large differences in parameter estimates. Replicating what was found with FIML analyses, perceived stigma significantly predicted anticipated stigma (β = .33, p < .001), and anticipated stigma significantly predicted Community Adjustment (β = −.24, p = .02). The indirect effect was still significant (β = −.17, p = .02), and this effect was also marginally significant with bootstrapping (β = −.01, p = .09). Also, the indirect effect’s 90% confidence interval did not include zero (CI = −.022 to −.002). Anticipated stigma did not significantly predict any of the other latent outcomes in the smaller sample, consistent with FIML analyses.
Contributor Information
Kelly E. Moore, Department of Psychology, George Mason University
Jeffrey B. Stuewig, Department of Psychology, George Mason University
June P. Tangney, Department of Psychology, George Mason University
References
- Aronson Joshua, Steele Claude M. Stereotypes and the Fragility of Academic Competence, Motivation, and Self-Concept. In: Elliot AJ, Dweck CS, editors. Handbook of Competence and Motivation. New York, NY: Guilford Publications; 2005. pp. 436–456. [Google Scholar]
- Benson Michael L, Alarid Leanne F, Burton Velmer S, Cullen Francis T. Reintegration or Stigmatization? Offenders’ Expectations of Community ReEntry. Journal of Criminal Justice. 2011;39:385–393. [Google Scholar]
- Bos Arjan ER, Pryor Johan B, Reeder Glenn D, Stutterheim Sarah E. Stigma: Advances in Theory and Research. Basic and Applied Social Psychology. 2013;35:1–9. [Google Scholar]
- Braithwaite John. Crime, Shame, and Reintegration. New York: Cambridge University Press; 1989. [Google Scholar]
- Carver Charles S, Scheier Michael F, Segerstrom Suzanne C. Optimism. Clinical Psychology Review. 2010;30:879–889. doi: 10.1016/j.cpr.2010.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chiricos Ted, Barrick Kelle, Bales William. The Labeling of Convicted Felons and its Consequences for Recidivism. Criminology. 2007;45:547–581. [Google Scholar]
- Corrigan Patrick W, Larson Jonathon E, Kuwabara Sachiko A. Social Psychology of the Stigma of Mental Illness: Public and Self-Stigma Models. In: Maddux JE, Tangney JP, editors. Social Psychological Foundations of Clinical Psychology. New York, NY: Guilford Press; 2010. pp. 51–68. [Google Scholar]
- Corrigan Patrick W, Rusch Nicolas. Mental Illness Stereotypes and Clinical Care: Do People Avoid Treatment Because of Stigma? Psychiatric Rehabilitation Skills. 2002;6:312–334. [Google Scholar]
- Corrigan Patrick W, Watson Amy C, Barr Leah. The Self-Stigma of Mental Illness: Implications for Self-Esteem and Self-Efficacy. Journal of Social and Clinical Psychology. 2006;25:875–884. [Google Scholar]
- Crocker Jennifer, Major Brenda. Social Stigma and Self-Esteem: The Self-Protective Properties of Stigma. Psychological Review. 1989;96:608–630. [Google Scholar]
- Crocker Jennifer, Major Brenda, Steele Claude. Social stigma. In: Gilbert DT, Fiske ST, Lindzey G, editors. The handbook of social psychology. 4. New York, NY: McGraw-Hill; 1998. pp. 504–553. [Google Scholar]
- Earnshaw Valerie A, Quinn Diane M, Park Crystal L. Anticipated Stigma and Quality of Life Among People Living with Chronic Illnesses. Chronic Illness. 2012;8:79–88. doi: 10.1177/1742395311429393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eccleston Collette P, Major Brenda N. Attributions to Discrimination and Self-Esteem: The Role of Group Identification and Appraisals. Group Processes & Intergroup Relations. 2006;9:147–162. [Google Scholar]
- Frable Deborah ES, Platt Linda, Hoey Steve. Concealable Stigmas and Positive Self-Perceptions: Feeling Better Around Similar Others. Journal of Personality and Social Psychology. 1998;74:909–922. doi: 10.1037//0022-3514.74.4.909. [DOI] [PubMed] [Google Scholar]
- Frost David M. Social Stigma and its Consequences for the Socially Stigmatized. Social and Personality Psychology Compass. 2011;11:824–839. [Google Scholar]
- Graham John W, Cumsille Patricio E, Elek-Fisk Elvira. Methods for Handling Missing Data. In: Schinka WF, Velicer WF, Weiner IB, editors. Handbook of Psychology Volume 2: Research Methods in Psychology. Hoboken, NJ: John Wiley & Sons Inc; 2013. pp. 109–141. [Google Scholar]
- Hanson Karl R, Tangney June P. Corrections Research. Department of the Solicitor General of Canada; Ottawa: 1996. The Test of Self-Conscious Affect-Socially Deviant Populations (TOSCA-SD) [Google Scholar]
- Harris Anthony R. Race, Commitment to Deviance, and Spoiled Identity. American Sociological Review. 1976;41:432–442. [Google Scholar]
- Heigel Caron P, Stuewig Jeffrey, Tangney June P. Self-Reported Physical Health of Inmates: Impact of Incarceration and Relation to Optimism. Journal of Correctional Health Care. 2010;16:106–116. doi: 10.1177/1078345809356523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Inzlicht Michael, Tullett Alexa M, Gutsell Jennifer N. Stereotype threat spillover: The short- and long-term effects of coping with threats to social identity. In: Inzlicht M, Schmader T, editors. Stereotype Threat: Theory, Process, and Application. New York, NY: Oxford University Press; 2012. pp. 107–123. [Google Scholar]
- Kaiser Cheryl R, Major Brenda, McCoy Shannon K. Expectations About the Future and the Emotional Consequences of Perceiving Prejudice. Personality and Social Psychology Bulletin. 2004;30:173–184. doi: 10.1177/0146167203259927. [DOI] [PubMed] [Google Scholar]
- Kline Rex B. Principles and Practice of Structural Equation Modeling. New York, NY: Guilford Press; 2005. [Google Scholar]
- Laub John H, Nagin Daniel, Sampson Robert J. Trajectories of Change in Criminal Offending: Good Marriages and the Desistance Process. American Sociological Review. 1993;63:225–238. [Google Scholar]
- LeBel Thomas P. Invisible stripes? Formerly Incarcerated Person’s Perceptions of Stigma. Deviant Behavior. 2012;33:89–107. [Google Scholar]
- Lemert Edwin M. Beyond Mead: The Societal Reaction to Deviance. Social Problems. 1974;21:457–468. [Google Scholar]
- Link Bruce G. Understanding Labeling Effects in the Area of Mental Disorders: An Assessment of the Effects of Expectations of Rejection. American Sociological Review. 1987;52:96–112. [Google Scholar]
- Link Bruce G, Cullen Frances T, Struening Elmer L, Shrout Patrick E, Dohrenwend Bruce P. A Modified Labeling Theory Approach to Mental Disorders: An Empirical Assessment. American Sociological Review. 1989;54:400–423. [Google Scholar]
- Link Bruce G, Phelan Jo C. Conceptualizing Stigma. Annual Review of Sociology. 2001;27:363–385. [Google Scholar]
- Little Roderick JA, Donald Rubin B. The Analysis of Social Science Data with Missing Values. Sociological Methods and Research. 1989;18:292–326. [Google Scholar]
- Little Todd D, Jorgensen Terrence D, Lang Kyle M, Whitney G Moore. On the Joys of Missing Data. Journal of Pediatric Psychology. 2013;39:151–162. doi: 10.1093/jpepsy/jst048. [DOI] [PubMed] [Google Scholar]
- Livingston James D, Boyd Jennifer E. Correlates and Consequences of Internalized Stigma for People Living with Mental Illness: A Systematic Review and Meta-Analysis. Social Sciences and Medicine. 2010;71:2150–2161. doi: 10.1016/j.socscimed.2010.09.030. [DOI] [PubMed] [Google Scholar]
- Livingston James D, Milne Teresa, Fang Mei Lan, Amari Erica. The Effectiveness of Interventions for Reducing Stigma Related to Substance Use Disorders: A Systematic Review. Addiction. 2012;107:39–50. doi: 10.1111/j.1360-0443.2011.03601.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lucksted Alicia, Drapalski Amy, Calmes Christine, Forbes Courtney, Deforge Bruce, Boyd Jennifer. Ending Self-Stigma: Pilot Evaluation of a New Intervention to Reduce Internalized Stigma Among People with Mental Illnesses. Psychiatric Rehabilitation Journal. 2011;35:51–54. doi: 10.2975/35.1.2011.51.54. [DOI] [PubMed] [Google Scholar]
- Luoma Jason B, Twohig Michael P, Waltz Thomas, Hayes Steven C, Roget Nancy, Padilla Michelle, Fisher Gary. An Investigation of Stigma in Individuals Receiving Treatment for Substance Abuse. Addictive Behaviors. 2007;32:1331–1346. doi: 10.1016/j.addbeh.2006.09.008. [DOI] [PubMed] [Google Scholar]
- MacKinnon David P, Fairchild Amanda J, Fritz Matthew S. Mediation Analysis. Annual Review of Psychology. 2007;58:593–614. doi: 10.1146/annurev.psych.58.110405.085542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Major Brenda, Eccleston Collette P. Stigma and Social Exclusion. In: Abrams D, Hogg MA, Marques JM, editors. The Social Psychology of Inclusion and Exclusion. New York, NY: Psychology Press; 2005. pp. 63–87. [Google Scholar]
- Major Brenda, O’Brien Laurei T. The Social Psychology of Stigma. Annual Review of Psychology. 2005;56:393–421. doi: 10.1146/annurev.psych.56.091103.070137. [DOI] [PubMed] [Google Scholar]
- Major Brenda, Sawyer Pamela J. Attributions to Discrimination: Antecedents and Consequences. In: Nelson TD, editor. Handbook of Prejudice, Stereotyping, and Discrimination. New York, NY: Psychology Press; 2009. pp. 89–110. [Google Scholar]
- Mashek Debra, Cannaday Lisa W, Tangney June P. Inclusion of Community in Self Scale: A Single Item Pictorial Measure of Community Connectedness. Journal of Community Psychology. 2007;54:257–275. [Google Scholar]
- Mashek Debra, Meyer P, McGrath J, Stuewig Jeffrey, Tangney June P. Inmate Perceptions and Expectations of Stigma (IPES) George Mason University; Fairfax, VA: 2002. [Google Scholar]
- Mashek Debra, Stuewig Jeffrey, Furukawa Emi, Tangney June P. Psychological and Behavioral Implications of Connectedness to Communities with Opposing Values and Beliefs. Journal of Social and Clinical Psychology. 2006;25:404–428. doi: 10.1521/jscp.2006.25.4.404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore Kelly, Stuewig Jeffrey, Tangney June P. Jail Inmates’ Perceived and Anticipated Stigma: Implications for Post-Release Functioning. Self and Identity. 2013;12:527–547. doi: 10.1080/15298868.2012.702425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morani Nicole M, Wikoff Nora, Linhorst Donald M, Bratton Sheila. A Description of the Self-Identified Needs, Service Expenditures, and Social Outcomes of Participants of a Prison-Reentry Program. The Prison Journal. 2011;91:347–365. [Google Scholar]
- Morey Les C. Personality Assessment Inventory: Professional Manual. 2. Odessa, FL: Psychological Assessment Resources; 2007. [Google Scholar]
- Pager Devah, Western Bruce, Sugie Naomi. Sequencing Disadvantage: Barriers to Employment Facing Young Black and White Men with Criminal Records. Annals of the American Academy of Political and Social Science. 2009;623:195–213. doi: 10.1177/0002716208330793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perlick Deborah A, Rosenheck Robert A, Clarkin John F, Sirey Jo Anne, Salahi Jamelah, Struening Elmer L, Link Bruce G. Stigma as a Barrier to Recovery: Adverse Effects of Perceived Stigma on Social Adaptation of Persons Diagnosed with Bipolar Affective Disorder. Psychiatric Services. 2001;52:1627–1632. doi: 10.1176/appi.ps.52.12.1627. [DOI] [PubMed] [Google Scholar]
- Peterson C, Seligman MEP. Values in Action Inventory of Strengths (VIA-IS) University of Pennsylvania; 2001. [Google Scholar]
- Pogorzelski Wendy, Wolff Nancy, Pan Ko-Yu, Blitz Cynthia L. Behavioral Health Problems, Ex-offender Reentry Policies, and the “Second Chance Act”. Public Health Consequences of Imprisonment. 2005;95:1718–1724. doi: 10.2105/AJPH.2005.065805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prince Pamela N, Prince Christopher R. Perceived Stigma and Community Integration Among Clients of Assertive Community Treatment. Psychiatric Rehabilitation Journal. 2002;25:323–331. doi: 10.1037/h0095005. [DOI] [PubMed] [Google Scholar]
- Preacher Kristopher J, Hayes Andrew F. SPSS and SAS Procedures for Estimating Indirect Effects in Simple Mediation Models. Behavior Research Methods, Instruments, & Computers. 2004;36:717–731. doi: 10.3758/bf03206553. [DOI] [PubMed] [Google Scholar]
- Quinn Diane M. Concealable Versus Conspicuous Stigmatized Identities. In: Levin S, van Laar C, editors. Stigma and Group Inequality: Social Psychological Perspectives. Mahwah, NJ: Lawrence Erlbaum Associates Publishers; 2006. pp. 83–103. [Google Scholar]
- Quinn Diane M, Chaudoir Stephenie R. Living with a Concealable Stigmatized Identity: The Impact of Anticipated Stigma, Centrality, Salience, and Cultural Stigma on Psychological Distress and Health. Journal of Personality and Social Psychology. 2009;97:634–651. doi: 10.1037/a0015815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rao Deepa, Pryor John B, Gaddist Bambi W. Stigma, Secrecy, and Discrimination: Ethnic/Racial Differences in the Concerns of People Living with HIV/AIDS. AIDS and Behavior. 2008;12:265–271. doi: 10.1007/s10461-007-9268-x. [DOI] [PubMed] [Google Scholar]
- Ritsher Jennifer B, Otilingam Poorni G, Grajales Monica. Internalized Stigma of Mental Illness: Psychometric Properties of a New Measure. Psychiatry Research. 2003;121:31–49. doi: 10.1016/j.psychres.2003.08.008. [DOI] [PubMed] [Google Scholar]
- Sampson Robert J, Laub John. A Life-Course Theory of Cumulative Disadvantage and the Stability of Delinquency. Advances in Criminological Theory. 1997;7:133–161. [Google Scholar]
- Schafer Joseph L, Graham John W. Missing Data: Our View of the State of the Art. Psychological Methods. 2002;7:147–177. [PubMed] [Google Scholar]
- Scheff Thomas. Being Mentally Ill. Chicago: Adine; 1966. [Google Scholar]
- Schomerus Georg, Corrigan Patrick W, Kaluer Thomas, Kuwert Phillip, Freyberger Harald J, Lucht Michael. Self-Stigma in Alcohol Dependence: Consequences for Drinking Refusal Self-Efficacy. Drug and Alcohol Dependence. 2011;114:12–17. doi: 10.1016/j.drugalcdep.2010.08.013. [DOI] [PubMed] [Google Scholar]
- Semple Shriley J, Patterson Thomas L, Rant Igor. Methamphetamine Use and Depressive Symptoms Among Heterosexual Men and Women. Journal of Substance Use. 2005;10:31–47. [Google Scholar]
- Shrout Patrick E, Bolger Niall. Mediation in Experimental and Nonexperimental Studies: New Procedures and Recommendations. Psychological Methods. 2002;7:422–445. [PubMed] [Google Scholar]
- Simpson DD, Knight Kevin. TCU Data Collection Forms for Correctional Residential Treatment (TCU-CRTF) Fort Worth, TX: Texas Christian University, Institute of Behavioral Research; 1998. [Google Scholar]
- Steele Claude M, Spencer Steven J, Aronson Joshua. Contending with Group Image: The Psychology of Stereotype and Social Identity Threat. In: Zanna MP, editor. Advances in experimental social psychology. San Diego, CA: Academic Press; 2002. pp. 379–440. [Google Scholar]
- Stuewig Jeffrey, Tangney June P, Mashek Debra, Forkner Peter, Dearing Ronda. The Moral Emotions, Alcohol Dependence, and HIV Risk Behavior in an Incarcerated Sample. Substance Use and Misuse. 2009;44:449–471. doi: 10.1080/10826080802421274. [DOI] [PubMed] [Google Scholar]
- Tangney June P, Mashek Debra, Stuewig Jeffrey. Working at the Social-Clinical-Community-Criminology Interface: The George Mason University Inmate Study. Journal of Social and Clinical Psychology. 2007;26:1–21. doi: 10.1521/jscp.2007.26.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tangney June P, Stuewig Jeffrey, Mashek Debra, Hastings Mark. ‘Assessing Jail Inmates’ Proneness to Shame and Guilt: Feeling Bad About the Behavior or the Self? Criminal Justice and Behavior. 2011;38:710–734. doi: 10.1177/0093854811405762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson Amy C, River Phillip L. A Social-Cognitive Model of Personal Responses to Stigma. In: Corrigan PW, editor. On the Stigma of Mental Illness: Practical Strategies for Research and Social Change. Washington, D.C: American Psychological Association; 2005. pp. 145–164. [Google Scholar]
- Winnick Terri A, Bodkin Mark. Anticipated Stigma and Stigma Management Among Those to be Labeled “Ex-Con. Deviant Behavior. 2008;29:295–333. [Google Scholar]
- Worrall John L, Morris Robert. Inmate custody levels and prison rule violations. The Prison Journal. 2011;91:131–157. [Google Scholar]