

Abstract
Objective
To evaluate the prevalence of anal cytology (ACyt) abnormalities among HIV-infected and HIV-uninfected men who have sex with men (MSM)
Design
Multicenter cohort study of 723 HIV-infected and 788 HIV-uninfected MSM with ACyt, with a second ACyt collected two years later. Referral for high-resolution anoscopy (HRA) was suggested for abnormal ACyt.
Methods
ACyt samples were collected using a polyester swab and liquid cytology media, and read in a central laboratory.
Results
Prevalence of any abnormal ACyt was 25% in HIV-uninfected MSM, and increased to 38%, 41%, and 47% among HIV-infected MSM with current CD4+ T-cell counts ≥500, 350–499, and <350 cells/mm3 (p<0.001), respectively. Anal HPV16 DNA was also more common in HIV-infected than HIV uninfected MSM (25% vs 16%, p<0.001). Abnormal baseline ACyt together with prevalent HPV16 DNA detection was present in only 7% of HIV-uninfected MSM compared to 18% of HIV-infected MSM with current CD4<350, p<0.001).
Among HIV-infected men, 56% of the men with low grade squamous intraepithelial lesions ASC-US/LSIL and 81% of men with atypical squamous cells cannot exclude high grade (ASC-H/)/high grade SIL (HSIL) had lower grade ACyt findings 18–30 months later (“regressed”). However, 19% of untreated HIV-infected men with ASC-H/HSIL cytology maintained that same grade of cytology at their second test approximately two years later, and 15% with ASC-US/LSIL “progressed” to ASC-H/HSIL. Abnormal ACyt had high sensitivity (96%) but low specificity (17%) for biopsy proven HSIL.
Conclusions
Prevalence of abnormal ACyt remains elevated in HIV-infected men during the current ART era.
Keywords: anal dysplasia, screening, anal cytology, MSM, HIV, MACS, anal cancer, HPV
Introduction
Although anal cancer is rare in the general U.S. population (1.8 per 100,000)1, its incidence has been increasing since the 1960s.2 Most anal cancers are squamous cell carcinomas causally related to high-risk types of human papillomavirus (hr-HPV), which is most prevalent in populations who practice receptive anal intercourse, such as men who have sex with men (MSM).3 Compared to the general U.S. population, anal cancer risk is 32 times higher in HIV-uninfected MSM and 52 times higher in HIV-infected MSM.4 Between 2001–05, almost one-third of anal cancers in men in the U.S. were diagnosed in HIV-infected individuals.4
Although current anal cancer rates in MSM are comparable to cervical cancer rates in women prior to the introduction of routine screening in the 1950s, anal cancer screening and prevention efforts remain limited. Using similar methods to cervical screening, initial studies suggest anal cytology (ACyt) can detect anal squamous intraepithelial lesions (SIL) with similar sensitivity and specificity to that seen for cervical cytology.5–7 High levels of abnormal ACyt have been uniformly reported among unscreened HIV-uninfected (12%–32%) and HIV-infected (34%–58%) MSM.8–11 In these studies, the majority of abnormalities detected were atypical squamous cells of undetermined significance (ASC-US) or low-grade SIL (LSIL). Although high-grade SIL (HSIL) cytology most likely accurately predicts the presence of true pre-cancer, its prevalence has been lower (≤5%) in both HIV-infected and uninfected MSM,8–11 studies suggest that due to its limited sensitivity12, ACyt likely underestimates HSIL prevalence.9
Given the high anal cancer risk in MSM, effective screening strategies are greatly needed. Prospective studies have demonstrated progression from normal anal epithelium or LSIL to HSIL over 2–4 years. Subsequent studies have also shown presence of high rates of HSIL – the putative anal cancer precursor – particularly among unscreened HIV-infected MSM.8 It had previously been generally accepted that most biopsy proven HSIL (bHSIL) would persist and eventually progress to cancer if not treated; however, recent research has shown that some bHSIL may regress without treatment.13 In HIV-infected individuals with HSIL ACyt, there is an estimated five year progression rate to invasive anal cancer of 1.7%.14
Anal cancer screening is not widely implemented, even among the highest risk groups. This is likely due to several issues including limitations in research, clinical expertise, and practice guidelines. The efficacy of ACyt screening with linkage to treatment for bHSIL to reduce anal cancer rates has not yet been tested in a randomized trial (although such a study is now underway). In addition, there are not enough clinicians trained in high-resolution anoscopy (HRA), a procedure analogous to cervical colposcopy that is needed to evaluate, diagnose and treat bHSIL. Finally, there are not consistent clinical recommendations on how MSM should be screened, either by ACyt or by proceeding directly to HRA. While some U.S. experts currently recommend ACyt for all MSM, others call for a closer examination of relative harms and benefits before treating all bHSIL.15–18
We conducted a study within a longitudinal cohort of HIV-infected and uninfected MSM to better understand the prevalence of abnormal ACyt and anal bHSIL.
Methods
Study Design and Population
The Multicenter AIDS Cohort Study (MACS) is an ongoing prospective study of HIV-infected and uninfected MSM, across four sites (Baltimore, Chicago, Pittsburgh, Los Angeles) over four enrollment periods (1984–85, 1987–1991, 2001–03, and 2010–12). All MACS participants who attended any MACS study visits between June 2010 and July 2011 were eligible to participate in the Anal Health Study (AHS) and were offered a free ACyt test by study staff. Men with an inadequate ACyt were offered another ACyt at their next study visit six months later. The study protocol called for all men who enrolled to have a second ACyt two years later (with additional annual sampling in HIV-infected men, not presented here). The AHS was approved by the institutional review boards of each participating site. Biologic and behavioral covariates of interest are routinely collected every six months in the MACS and were available for this analysis.
ACyt Collection
ACyt samples were collected by MACS clinicians who were trained in proper collection technique. Briefly, a water moistened polyester swab was blindly inserted into the anus to approximately 5 cm proximal to the anal verge and rotated in a spiral motion as it was withdrawn over 10–30 seconds.19–22 After removal, the swab was placed into PreservCyt® (Cytyc Corp., Marlborough, MA) liquid cytology media and vigorously agitated to remove cells. ACyt specimens were stored at room temperature until shipped to the laboratory for analysis.
ACyt Testing
Within two days of receipt, all samples were centrally processed by TriCore Reference Laboratories, Albuquerque, NM. Samples were processed as per manufacturer’s protocol on a Hologic T-2000 instrument (Hologic, Bedford, MA) using a non-gynecologic specimen filter and rehydrated using PreservCyt® to standard volume. A monolayer of cells was placed onto a slide using an automated system and Papanicolau staining was applied to slides before cells were visualized using microscopy. Specimens were initially screened for abnormalities by certified cytotechnologists and each was examined by a board certified cytopathologist.
Results were reported using the Bethesda 2001 system for grading cervical cytology as follows: 1) each sample was coded as adequate (sufficient nucleated squamous epithelial cells present) or inadequate for evaluation; 2) adequate specimens were classified as: negative (normal), or abnormal: ASC-US, LSIL, atypical squamous cells cannot exclude HSIL (ASC-H), or HSIL. Among 235 men whose baseline ACyt was inadequate, 161 men had a second adequate ACyt sample, a median of 11 months later; the results for these second ACyt samples were normal (76%), ASCUS (16%), LSIL (4%), ASC-H/HSIL (3%).
During ongoing study monitoring, the frequency of technically inadequate ACyt results was greater than expected from previous studies.23 To investigate and address this, additional quality assurance steps were introduced including: 1) monitoring and evaluation of the proportion of inadequate ACyt samples at each site; 2) evaluation of whether switching brand of polyester swab changed the proportion of samples deemed inadequate; 3) comparing inadequate rates when sample was collected by the training physician (RDC) or by other MACS clinicians, 4) comparison of ACyt results by individual MACS clinicians, and by how frequently the clinicians collected anal swabs, 5) re-reading of a subset of samples by an outside pathologist with expertise in ACyt interpretation (TMD).
Anal HPV Testing
The same sample used for ACyt was also used to test for anal HPV16 DNA using PCR by Tricore Reference Laboratory. In brief, DNA was extracted from 250 μL of the cytology sample using Qiagen MinElute PCR Purification kit (Qiagen, Valencia, CA), 50 μL was amplified using the PGMY09/11 primer system, and hybridized using Linear Array (Roche Diagnostic Laboratories) for 37 different HPV types.
High Resolution Anoscopy (HRA)
Participants with an abnormal ACyt result were given an educational brochure about HRA with contact information for local HRA providers (the presence of at least one local HRA provider was a site activation requirement) and were referred to their primary care physician to discuss whether to have HRA. Referral thus assessed a more ‘real life’ experience of follow up for both abnormal ACyt and the engagement of an at-risk population and was not a mandated study requirement. At each semi-annual visit all AHS participants, regardless of their ACyt results, were asked if they had a HRA examination and if so, copies of the HRA examination including anal biopsy were obtained.
Participants who had HRA performed for whom no biopsies were collected were considered to have had a finding of “No intraepithelial lesions” (NIL) upon HRA examination. Biopsy confirmed diagnosis of HSIL (bHSIL; also known as anal intraepithelial neoplasia 2+ (AIN2+) as well as biopsy findings of LSIL (bLSIL; also known as AIN1), and NIL were collected and reported using two-tiered Lower Anogenital Squamous Terminology (LAST).24 Participants who had abnormal ACyt and reported not having HRA, were asked to answer a questionnaire to indicate the main reason why they did not have HRA from a list of options which include a text box for ‘other reason’.
Statistical Analysis
Characteristics of enrolled participants were compared by HIV status and by ACyt results (normal versus abnormal, where abnormal was defined as ASC-US or higher) using Chi-square test for categorical and test of medians for continuous data. ACyt results were evaluated as adequate vs. inadequate, and the prevalence of each ACyt grade among adequate samples was reported. Cytologic grade was compared in a subset of samples between the testing laboratory and a confirmatory second laboratory using percent agreement and Kappa statistic.
Serial cytology results were also evaluated among men who had ACyt within 18–30 months after their first adequate study ACyt and had not been treated for anal dysplasia during this time. We evaluated the proportion of men that: “progressed” from any lower to higher cytologic grade, “regressed” (from any higher to lower cytologic grade), or “maintained” the same cytologic finding.
We explored the proportion of men with anal pre-cancer (HSIL) or cancer, diagnosed on biopsy (bHSIL+) within the three years after study baseline follow-up data available to date. This was explored among 220 men who had at least one adequate ACyt sample, had no known history of bHSIL before entry and who had at least one HRA at/after first interpretable ACyt in study (“entry”). Cytologic grade in the baseline ACyt was compared to HRA confirmed histology outcome (among 94 men who had HRA within less than 12 months of ACyt); sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were reported.
Results
There were 1511 men who had ACyt testing as part of this study including 723 HIV-infected and 788 HIV-uninfected men. At initial ACyt the median age was 55 years (IQR=49,61), 72% were white, 21% were current smokers, and 36% of men had receptive anal intercourse in the past six months (Table 1). Median current CD4+ T-cell count among HIV-infected men was 583 cells/mm3. Only 6% (94/1511) of men had ever had an ACyt test before this study, and 1% (15/1511) had a prior confirmed diagnosis of invasive anal squamous cell cancer.
Table 1.
Description of study population at baseline Anal Health Study (AHS) visit, stratified by baseline anal cytology (ACyt) result
| N | Col % | Prevalence of ACyt result (by Row) | ||||
|---|---|---|---|---|---|---|
| Total (N=1511) | Normal (N = 849) | Abnormal (N = 427) | Inadequate (N = 235) | P-value | ||
| HIV Status | <0.001 | |||||
| HIV-Uninfected | 788 | 52% | 62% | 21% | 17% | |
| HIV-Infected | 723 | 48% | 50% | 36% | 14% | |
| Current ART use | 723 | 91% | 50% | 36% | 14% | 0.488 |
| Race | 0.138 | |||||
| White | 1086 | 72% | 58% | 27% | 14% | |
| Black | 271 | 18% | 49% | 32% | 20% | |
| Hispanic | 127 | 8% | 54% | 29% | 17% | |
| Other | 27 | 2% | 63% | 22% | 15% | |
|
| ||||||
| Center | 0.013 | |||||
| Baltimore | 359 | 24% | 56% | 26% | 19% | |
| Chicago | 302 | 20% | 54% | 34% | 12% | |
| Pittsburgh | 368 | 24% | 61% | 27% | 12% | |
| Los Angeles | 482 | 32% | 54% | 27% | 18% | |
|
| ||||||
| Smoking Status | 0.088 | |||||
| Never | 410 | 28% | 61% | 26% | 13% | |
| Former | 742 | 51% | 56% | 28% | 15% | |
| Current | 298 | 21% | 50% | 33% | 17% | |
|
| ||||||
| # of anal receptive partners in 6 months prior to first ACty | 0.004 | |||||
| 0 | 917 | 64% | 58% | 26% | 16% | |
| 1 | 247 | 17% | 55% | 30% | 15% | |
| ≥2 | 270 | 19% | 51% | 37% | 12% | |
|
| ||||||
| Before the baseline ACyt | ||||||
| Ever had ACyt? | ||||||
| No | 1417 | 94% | 56% | 28% | 16% | 0.89 |
| Yes | 94 | 6% | 59% | 31% | 10% | |
| Ever had HRA? | 88 | 6% | 47% | 45% | 8% | <0.001 |
| Ever diagnosed with invasive anal cancer? | 15 | 1% | 40% | 27% | 33% | 0.150 |
|
| ||||||
| HIV viral lead, copies/mL (among HIV-infected) | ||||||
| Undetectable (≤40) | 561 | 78% | 51% | 34% | 15% | 0.148 |
| Detectable (>40) | 161 | 22% | 47% | 42% | 11% | |
|
| ||||||
| N | Median | Median (IQR) | ||||
|
| ||||||
| Age, years | 1511 | 55 | 56 (50, 61) | 55 (48, 60) | 55 (49, 61) | 0.162 |
|
| ||||||
| Current CD4 T cell count, cells/mm3 | 723 | 583 | 595 (431, 769) | 565 (401, 747) | 599 (461, 808) | <0.001 |
ACyt
At baseline, 28% (427/1511) of men had abnormal ACyt, and in 16% (235/1511) of men the cytologic specimen was inadequate (Table 1). Of the 1276 men with adequate baseline ACyt, 33% had abnormal ACyt. We did not identify any differences in the proportion of inadequate samples by provider characteristics (study sites, clinicians, swab type used), or patient characteristics (HIV status, age), data not shown. Men with abnormal ACyt were more likely to be HIV-infected, to be current smokers, and to have more recent receptive anal intercourse partners, but were similar in terms of age and race, when compared to men with normal or inadequate ACyt results (Table 1).
Among the 1437 men with an adequate ACyt (Figure 1), abnormal ACyt was common (32%), and more frequent among HIV-infected (276/687, 40%) than HIV-uninfected men (189/750, 25%; p<0.001). The proportion of HIV-infected men with abnormal ACyt increased with lower CD4+ T-cell count, with 38%, 41%, and 47% among men with current CD4+ T-cell counts ≥500, 350–499, and <350 cells/mm3, respectively (p<0.001, Table 2). HSIL (1.5%) and ASC-H (2.4%) ACyt were uncommon overall. This difference was most notable for LSIL cytology, which was three-fold more common in HIV-infected than HIV-uninfected men (13.2% vs. 4.5%, p<0.001).
Figure 1.
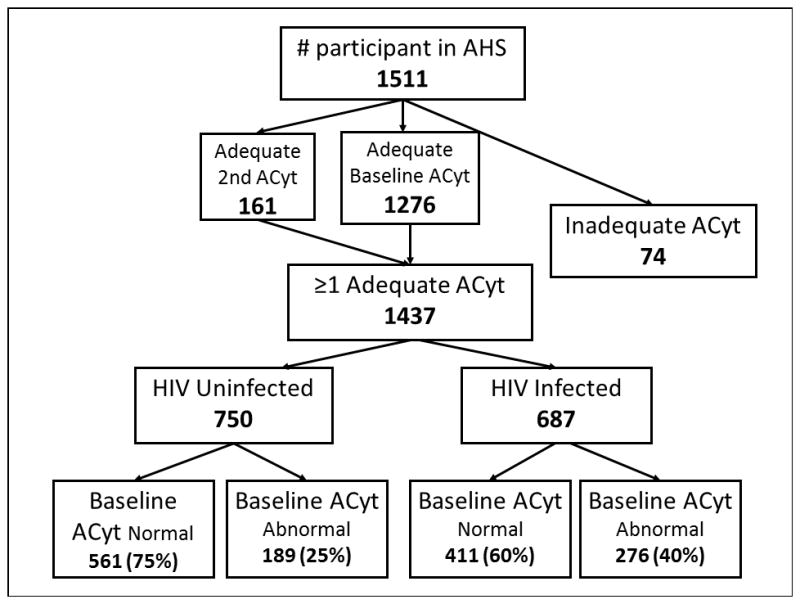
Study flowchart of the 1511 men enrolled in the MACS Anal Health Study (AHS), showing number of men with any adequate ACyt, and describing number with normal vs. abnormal ACyt by HIV status.
Table 2.
First Adequate ACyt result among 1437 men with adequate ACyt, by HIV status and current CD4+ T-cell count
| Baseline ACyt | HIV-uninfected N = 750 |
N (%) HIV-infected |
Total N = 1437 |
||
|---|---|---|---|---|---|
| CD4+ ≥ 500 N = 421 |
350≤ CD4+ <500 N = 151 |
CD4+ <350 N = 115 |
|||
| Normal ACyt | 561 (75) | 261 (62) | 89 (59) | 61 (53) | 972 (68) |
| Abnormal ACyt | 189 (25) | 160 (38) | 62 (41) | 54 (47) | 465 (32) |
|
| |||||
| ASC-US/ LSIL | 165 (22) | 140 (33) | 54 (36) | 50 (43) | 409 (28) |
| ASC-H / HSIL | 24 (3) | 19 (5) | 8 (5) | 4 (3) | 55 (4) |
|
| |||||
| N positive (%) | |||||
|
| |||||
| HPV16 DNA detected^ | 117 (16) | 96 (23) | 37 (25) | 31 (27) | 281 (20) |
|
| |||||
| Abnormal ACyt and HPV16 detected | 50 (7) | 48 (12) | 21 (14) | 21 (18) | 140 (10) |
Among 1423 participants consented to testing for HPV16 DNA.
Anal HPV16 DNA was more common in HIV-infected than HIV-uninfected men (25% vs 16%, p<0.001). Ten percent of all men had both prevalent HPV16 DNA and abnormal ACyt at baseline (abnACyt/16+), and the frequency of this abnACyt/16+ profile increased significantly with HIV-infection and immunosuppression (p<0.001, Table 2). Indeed, 18% of HIV-infected men with current CD4<350 had both abnormal ACyt and prevalent HPV16 DNA detected at baseline, compared to only 7% of HIV-uninfected men.
ACyt Interpretation Reproducibility
To evaluate the reproducibility of ACyt findings, a subset of selected ACyt samples (oversampled for inadequate and abnormal ACyt) was sent from the central testing laboratory for blinded re-read at a second laboratory with ACyt expertise (TMD).25 Agreement of classification of any abnormal ACyt between the two labs was 82%, Kappa=0.61. Of those ACyt classified as negative (n=59), LSIL (n=20), HSIL/ASC-H (n=24), and inadequate (n=30) by the confirming laboratory, the percent agreement for ACyt grade read by the central testing laboratory was: 70%, 60%, 67%, and 73%, respectively.
Comparison of ACyt 2 years Apart
We compared the cytologic classification of repeat ACyt among 447 HIV-infected and 409 HIV-uninfected men who had two adequate ACyt tests within 18–30 months and had no treatment of anal SIL during that time period (Table 3). Among men with normal baseline cytology, 29% and 16% of subsequent ACyt specimens from HIV-infected and HIV–uninfected men, respectively, showed abnormalities of a higher grade (”progressed”) 18–30 months later (Table 3). Among men with baseline ASC-US/LSIL cytology, 61% “regressed” to normal cytology, while 15% of HIV-infected and 5% of HV-uninfected men “progressed” to a higher-grade cytologic classification.
Table 3.
Comparison of first and second adequate ACyt results in 856 participants, taken 18–30 months apart, among HIV-infected and uninfected men with no anal squamous intraepithelial lesion treatment
| Baseline ACyt | %
|
P-value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HIV-uninfected | HIV-infected | ||||||||
|
| |||||||||
| N | Lower grade | Same grade | Higher grade | N | Lower grade | Same grade | Higher grade | ||
| Normal | 305 | -- | 84% | 16% | 277 | -- | 71% | 29% | <0.001 |
| ASC-US/ LSIL | 91 | 66% | 29% | 5% | 149 | 56% | 29% | 15% | 0.075 |
| ASC-H / HSIL | 13 | 92% | 8% | 0% | 21 | 81% | 19% | 0% | 0.364 |
| Overall | 409 | 18% | 69% | 13% | 447 | 23% | 54% | 23% | <0.001 |
Among HIV-infected men, 56% the men with ASC-US/LSIL and 81% of men with ASC-H/HSIL had lower grade cytologic findings 18–30 months later (“regressed”). However, 19% of untreated HIV-infected men with ASC-H/HSIL cytology maintained that same grade of cytology at their second test approximately two years later (Table 3), and 15% with ASC-US/LSIL “progressed” to ASC-H/HSIL. Among HIV-uninfected men, findings were similar but the proportion of men with ASC-US/LSIL who maintained the same cytologic grade was 29% and only 5% “progressed” to ASC-H/HSIL (Table 3).
Identification of bHSIL and utility of abnormal ACyt in identifying men with bHSIL
Of the 1437 men in the AHS with adequate ACyt, 45 men were known to have had bHSIL before their first ACyt, including 12 men with a history of invasive anal squamous cell cancer. Among the remaining 1392 men at risk for first bHSIL diagnosis during the study, 16% (220/1392) elected to have evaluation using HRA and biopsy during study follow-up (June 2010 – January 2015). Median time from baseline ACyt to first HRA in study was 0.5 years in those with abnormal ACyt and 2.4 years in those with normal ACyt.
Among 220 men with HRA during study follow-up, 87 (40%) were confirmed to have bHSIL+ during study follow-up (at/after first sufficient ACyt). The proportion of men confirmed to have bHSIL+ was high among both HIV-infected (38/79; 48%) and HIV-uninfected (22/61; 36%) men with abnormal baseline ACyt. Only 80 men with normal baseline ACyt had HRA during follow-up, but among these men bHSIL+ was diagnosed in HIV-infected (18/53, 34%) and HIV-uninfected (9/27, 33%) men.
Ninety-four men had HRA and anal biopsy within 12 months of baseline ACyt and we restricted analysis of utility of ACyt in identifying men with bHSIL to these men. Although there was a limited population with follow up HRA and biopsy that was based on local standard of care, abnormal ACyt had high sensitivity (96%) but low specificity (17%) for bHSIL (Table 4). The positive predictive value (PPV) of abnormal ACyt for bHSIL was only 27% but the negative predictive value (NPV) was 92%. If all 220 men with HRA and anal biopsy were considered, sensitivity was lower at 67% and specificity was higher at 38%.
Table 4.
Comparison of first adequate anal cytology result with the biopsy result from subsequent high resolution anoscopy (HRA), among 94 men who had HRA within less than 12 months after anal cytology.
| HRA Outcome/Biopsy | ||||
|---|---|---|---|---|
| Cytology | No intraepithelial lesions | bLSIL | bHSIL | Total |
| Normal (negative) | 8 | 4 | 1 | 13 |
| ASC-US+ | 43 | 16 | 22 | 81 |
| Total | 51 | 20 | 23 | 94 |
|
| ||||
| Utility of any abnormal ACyt for bHSIL | % | n/N | ||
|
| ||||
| Sensitivity | 96% | (22/23) | ||
| Specificity | 17% | (12/71) | ||
| Positive Predictive Value | 27% | (22/81) | ||
| Negative Predictive Value | 92% | (12/13) | ||
ASC-H/HSIL: Atypical squamous cells-cannot exclude high grade/High-grade intraepithelial lesion on anal cytology
bLSIL: Low-grade squamous intraepithelial lesion on biopsy
bHSIL: High-grade squamous intraepithelial lesion on biopsy
Follow-up for abnormal ACyt
Interview follow-up data for men with abnormal cytology showed many did not undergo diagnostic follow-up using HRA. Among 465 men with abnormal baseline cytology, 139 (30%) had HRA during the study, and 326 did not (of whom 68% [223/326] completed the follow-up survey). Thirty-seven percent of these men reported the primary reason for not undergoing HRA was that they were unaware HRA was recommended or that they had insufficient information to act on the diagnostic follow-up recommendation. Another 22% stated no reason or reported not being interested in a diagnostic HRA, and 11% reported that they discussed it with their doctor who said HRA was not needed. Nearly 8% of men reported forgetting or being unaware of an abnormal ACyt finding. Additional reasons reported for not getting HRA included having had ≥1 normal prior cytology finding (4%), having had HRA previously (2%), deciding to have a follow-up cytology (3%) or colonoscopy (4%) instead of HRA, financial constraints (4%), and 5% reported other reasons, including not remembering whether they had HRA.
Discussion
This report demonstrates a high prevalence of abnormal ACyt among MSM in a multi-site U.S. study. Abnormal ACyt and anal HPV16 DNA were more common among HIV-infected than HIV-uninfected MSM, and increased with immunosuppression. Most ASC-US and LSIL ACyt was no longer detected (“regressed”) on ACyt two years later. bHSIL was primarily detected among HIV-infected and HIV-uninfected men with abnormal ACyt, but was also detected in men with normal ACyt. Prevalence of abnormal ACyt remains elevated in HIV-infected men during the current ART era, although this was primarily due in higher prevalence of LSIL cytology.
The prevalence of abnormal ACyt observed among MSM in this study was similar to previous reports of frequent cytologic abnormality (ASC-US+; 41–68%) but low (≤5%) prevalence of HSIL ACyt,10,26,27 although this is not consistent with some smaller older studies reporting higher prevalence of HSIL ACyt.28–30 The high proportion of MSM tested who had anal bHSIL in this study is comparable to another study of MSM which reported 16% two year cumulative incidence31, and supports the need for effective screening methods in this population.
Rates of cytological inadequacy vary by study, and despite investigation into potentially contributing variables, none were identified as causal. It should be noted that although the rate of inadequacy was higher than expected, there are reports with similar rates in the literature.10,27 However, lower rates (<5% insufficiency) are also in the literature.23,30 This has implications for the utility of ACyt testing, as a high insufficiency rate can decrease patient interest in testing due to the need for repetition and so decrease screening efficacy. The interpretation of ACyt varies between cytopathologists, and to enhance reporting uniformity we elected to have all ACyt read centrally for men from all study sites over the duration of the study.
As HRA was not required as part of this study, this study provides information on a more ‘real life’ clinical referral pathway where patient and provider factors contribute to HRA referral. Although only 15% of participants had HRA data available, this data includes participants from each study site including some participants with negative ACyt that also underwent HRA. Sensitivity and specificity of any abnormal ACyt to detect bHSIL in this study was comparable to that reported in previous ACyt studies,5,23,32,33 and comparable to that of a single cervical cytology for cervical bHSIL.34,35 Only a small proportion of men with normal ACyt had HRA during this study, and this group is likely not representative.
This is one of the largest studies to describe ACyt prevalence among HIV-infected MSM in the recent anti-retroviral treatment era, and to compare prevalence with HIV-uninfected MSM. This study underscores the increased risk of anal disease among MSM in general and especially among HIV-infected MSM. Despite this risk, the research suggests that issues of inadequate ACyt samples and low specificity of ACyt may limit the utility of this method for anal cancer screening. This study contributes to our understanding of anal pre-cancer risk among MSM. It is clear that MSM are at high and continuing risk of anal pre-cancer and cancer. The challenge now is how to best screen for and manage pre-cancer in order to reduce the progression to invasive disease.
Supplementary Material
Acknowledgments
Sources of Support: Data in this manuscript were collected by the Multicenter AIDS Cohort Study (MACS), with funding from the National Cancer Institute (NCI). MACS (Principal Investigators): Johns Hopkins University Bloomberg School of Public Health (Joseph Margolick), U01-AI35042; Northwestern University (Steven Wolinsky), U01-AI35039; University of California, Los Angeles (Roger Detels), U01-AI35040; University of Pittsburgh (Charles Rinaldo), U01-AI35041; the Center for Analysis and Management of MACS, Johns Hopkins University Bloomberg School of Public Health (Lisa Jacobson), UM1-AI35043. The MACS is funded primarily by the National Institute of Allergy and Infectious Diseases (NIAID), with additional co-funding from the National Cancer Institute (NCI), the National Institute on Drug Abuse (NIDA), and the National Institute of Mental Health (NIMH). MACS data collection is also supported by UL1-TR001079 (JHU ICTR) from the National Center for Advancing Translational Sciences (NCATS) a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research.
Footnotes
Meetings at which data was presented: August, 2014 International Papillomavirus Meeting in Seattle, WA, USA.
The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH), Johns Hopkins ICTR, or NCATS. The MACS website is located at http://aidscohortstudy.org.
Conflicts of Interests: GD, AW, NS, FB, MP, SR, NJ, EB have no conflicts of interest. DW has speaker bureau fees and research support from Merck & Co. SY is a member of the Scientific Advisory Boards for Roche Diagnostic Corporation and Quidel Corporation. TMD has received research supplies from Hologic for anal cytology. RDC has institutional research support from Merck & Co. (IISP 38548)
References
- 1.Surveillance E, and End Results (SEER) Program. [Accessed August 12, 2015];SEER Stat Fact Sheets: Anal Cancer. http://seer.cancer.gov/statfacts/html/anus.html.
- 2.Jemal A, Simard EP, Dorell C, et al. Annual Report to the Nation on the Status of Cancer, 1975–2009, Featuring the Burden and Trends in Human Papillomavirus (HPV)-Associated Cancers and HPV Vaccination Coverage Levels. J Natl Cancer Inst. 2013 Jan 7;105(3):175–201. doi: 10.1093/jnci/djs491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.D’Souza G, Wiley DJ, Li X, et al. Incidence and epidemiology of anal cancer in the multicenter AIDS cohort study. J Acquir Immune Defic Syndr. 2008 Aug 1;48(4):491–499. doi: 10.1097/QAI.0b013e31817aebfe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shiels MS, Pfeiffer RM, Chaturvedi AK, Kreimer AR, Engels EA. Impact of the HIV epidemic on the incidence rates of anal cancer in the United States. J Natl Cancer Inst. 2012 Oct 17;104(20):1591–1598. doi: 10.1093/jnci/djs371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Berry JM, Palefsky JM, Jay N, Cheng SC, Darragh TM, Chin-Hong PV. Performance characteristics of anal cytology and human papillomavirus testing in patients with high-resolution anoscopy-guided biopsy of high-grade anal intraepithelial neoplasia. Diseases of the colon and rectum. 2009 Feb;52(2):239–247. doi: 10.1007/DCR.0b013e31819793d9. [DOI] [PubMed] [Google Scholar]
- 6.Palefsky JM, Holly EA, Hogeboom CJ, Berry JM, Jay N, Darragh TM. Anal cytology as a screening tool for anal squamous intraepithelial lesions. Journal of acquired immune deficiency syndromes and human retrovirology : official publication of the International Retrovirology Association. 1997 Apr 15;14(5):415–422. doi: 10.1097/00042560-199704150-00004. [DOI] [PubMed] [Google Scholar]
- 7.Cranston RD, Hart SD, Gornbein JA, Hirschowitz SL, Cortina G, Moe AA. The prevalence, and predictive value, of abnormal anal cytology to diagnose anal dysplasia in a population of HIV-positive men who have sex with men. Int J STD AIDS. 2007;18(2):77–80. doi: 10.1258/095646207779949772. [DOI] [PubMed] [Google Scholar]
- 8.Chin-Hong PV, Vittinghoff E, Cranston RD, et al. Age-related prevalence of anal cancer precursors in homosexual men: the EXPLORE study. J Natl Cancer Inst. 2005 Jun 15;97(12):896–905. doi: 10.1093/jnci/dji163. [DOI] [PubMed] [Google Scholar]
- 9.Hillman RJ, van Leeuwen MT, Vajdic CM, et al. Prevalence and predictors of high-grade anal intraepithelial neoplasia in a community-based sample of homosexual men. Sex Health. 2012 Dec;9(6):574–579. doi: 10.1071/SH11139. [DOI] [PubMed] [Google Scholar]
- 10.Gaisa M, Sigel K, Hand J, Goldstone S. High rates of anal dysplasia in HIV-infected men who have sex with men, women, and heterosexual men. AIDS. 2014 Jan 14;28(2):215–222. doi: 10.1097/QAD.0000000000000062. [DOI] [PubMed] [Google Scholar]
- 11.Dona MG, Benevolo M, Vocaturo A, et al. Anal cytological abnormalities and epidemiological correlates among men who have sex with men at risk for HIV-1 infection. BMC cancer. 2012;12:476. doi: 10.1186/1471-2407-12-476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee EQ, Goldstone SE. Predictors of anal dysplasia in men who have sex with men with benign cytology. Dis Colon Rectum. 2011 Mar;54(3):347–351. doi: 10.1007/DCR.0b013e3181f46dc4. [DOI] [PubMed] [Google Scholar]
- 13.Tong WW, Jin F, McHugh LC, et al. Progression to and spontaneous regression of high-grade anal squamous intraepithelial lesions in HIV-infected and uninfected men. AIDS. 2013 Sep 10;27(14):2233–2243. doi: 10.1097/QAD.0b013e3283633111. [DOI] [PubMed] [Google Scholar]
- 14.Cachay E, Agmas W, Mathews C. Five-year cumulative incidence of invasive anal cancer among HIV-infected patients according to baseline anal cytology results: an inception cohort analysis. HIV medicine. 2015 Mar;16(3):191–195. doi: 10.1111/hiv.12190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Anderson JS, Vajdic C, Grulich AE. Is screening for anal cancer warranted in homosexual men? Sex Health. 2004;1(3):137–140. doi: 10.1071/sh03019. [DOI] [PubMed] [Google Scholar]
- 16.Pineda CE, Welton ML. Controversies in the management of anal high-grade squamous intraepithelial lesions. Minerva chirurgica. 2008 Oct;63(5):389–399. [PubMed] [Google Scholar]
- 17.Machalek DA, Poynten M, Jin F, et al. Anal human papillomavirus infection and associated neoplastic lesions in men who have sex with men: a systematic review and meta-analysis. Lancet Oncol. 2012 May;13(5):487–500. doi: 10.1016/S1470-2045(12)70080-3. [DOI] [PubMed] [Google Scholar]
- 18.Park IU, Palefsky JM. Evaluation and Management of Anal Intraepithelial Neoplasia in HIV-Negative and HIV-Positive Men Who Have Sex with Men. Current infectious disease reports. 2010 Mar;12(2):126–133. doi: 10.1007/s11908-010-0090-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Palefsky JM, Holly EA, Ralston ML, Arthur SP, Hogeboom CJ, Darragh TM. Anal cytological abnormalities and anal HPV infection in men with Centers for Disease Control group IV HIV disease. Genitourinary Medicine. 1997;73(3):174–180. doi: 10.1136/sti.73.3.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Palefsky JM, Holly EA, Ralston ML, et al. Anal squamous intraepithelial lesions in HIV-positive and HIV-negative homosexual and bisexual men: prevalence and risk factors. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology. 1998;17(4):320–326. doi: 10.1097/00042560-199804010-00005. [DOI] [PubMed] [Google Scholar]
- 21.Palefsky JM, Holly EA, Hogeboom CJ, Berry JM, Jay N, Darragh TM. Anal cytology as a screening tool for anal squamous intraepithelial lesions. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology. 1997;14(5):415–422. doi: 10.1097/00042560-199704150-00004. [DOI] [PubMed] [Google Scholar]
- 22.Palefsky JM, Holly EA, Ralston ML, Jay N, Berry JM, Darragh TM. High incidence of anal high-grade squamous intra-epithelial lesions among HIV-positive and HIV-negative homosexual and bisexual men. AIDS. 1998 Mar 26;12(5):495–503. doi: 10.1097/00002030-199805000-00011. [DOI] [PubMed] [Google Scholar]
- 23.Nathan M, Singh N, Garrett N, Hickey N, Prevost T, Sheaff M. Performance of anal cytology in a clinical setting when measured against histology and high-resolution anoscopy findings. AIDS. 2010 Jan 28;24(3):373–379. doi: 10.1097/QAD.0b013e328333ab8e. [DOI] [PubMed] [Google Scholar]
- 24.Darragh TM, Colgan TJ, Thomas Cox J, et al. The Lower Anogenital Squamous Terminology Standardization project for HPV-associated lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. International journal of gynecological pathology : official journal of the International Society of Gynecological Pathologists. 2013 Jan;32(1):76–115. doi: 10.1097/PGP.0b013e31826916c7. [DOI] [PubMed] [Google Scholar]
- 25.Darragh TM, Winkler B, Souers RJ, Laucirica R, Zhao C, Moriarty AT. Room for improvement: initial experience with anal cytology: observations from the College of American Pathologists interlaboratory comparison program in nongynecologic cytology. Archives of pathology & laboratory medicine. 2013 Nov;137(11):1550–1554. doi: 10.5858/arpa.2012-0574-CP. [DOI] [PubMed] [Google Scholar]
- 26.Sendagorta E, Herranz P, Guadalajara H, et al. Prevalence of abnormal anal cytology and high-grade squamous intraepithelial lesions among a cohort of HIV-infected men who have sex with men. Dis Colon Rectum. 2014 Apr;57(4):475–481. doi: 10.1097/DCR.0000000000000095. [DOI] [PubMed] [Google Scholar]
- 27.Botes LP, Pett S, Carr A, et al. Anal cytological abnormalities are poor predictors of high-grade intraepithelial neoplasia amongst HIV-positive men who have sex with men. Sex Health. 2013 Mar;10(1):9–17. doi: 10.1071/SH11135. [DOI] [PubMed] [Google Scholar]
- 28.Piketty C, Darragh TM, Heard I, et al. High prevalence of anal squamous intraepithelial lesions in HIV-positive men despite the use of highly active antiretroviral therapy. Sex Transm Dis. 2004 Feb;31(2):96–99. doi: 10.1097/01.OLQ.0000109515.75864.2B. [DOI] [PubMed] [Google Scholar]
- 29.Wilkin TJ, Palmer S, Brudney KF, Chiasson MA, Wright TC. Anal intraepithelial neoplasia in heterosexual and homosexual HIV-positive men with access to antiretroviral therapy. J Infect Dis. 2004 Nov 1;190(9):1685–1691. doi: 10.1086/424599. [DOI] [PubMed] [Google Scholar]
- 30.Palefsky JM, Holly EA, Efirdc JT, et al. Anal intraepithelial neoplasia in the highly active antiretroviral therapy era among HIV-positive men who have sex with men. AIDS. 2005 Sep 2;19(13):1407–1414. doi: 10.1097/01.aids.0000181012.62385.4a. [DOI] [PubMed] [Google Scholar]
- 31.Burgos J, Curran A, Tallada N, et al. Risk of progression to high-grade anal intraepithelial neoplasia in HIV-infected MSM. AIDS. 2015 Mar 27;29(6):695–702. doi: 10.1097/QAD.0000000000000603. [DOI] [PubMed] [Google Scholar]
- 32.Nahas CS, da Silva Filho EV, Segurado AA, et al. Screening anal dysplasia in HIV-infected patients: is there an agreement between anal pap smear and high-resolution anoscopy-guided biopsy? Dis Colon Rectum. 2009 Nov;52(11):1854–1860. doi: 10.1007/DCR.0b013e3181b98f36. [DOI] [PubMed] [Google Scholar]
- 33.Goldstone SE, Enyinna CS, Davis TW. Detection of oncogenic human papillomavirus and other predictors of anal high-grade dysplasia in men who have sex with men with abnormal cytology. Dis Colon Rectum. 2009 Jan;52(1):31–39. doi: 10.1007/DCR.0b013e31819736aa. [DOI] [PubMed] [Google Scholar]
- 34.Wright TC, Jr, Cox JT, Massad LS, Twiggs LB, Wilkinson EJ. 2001 Consensus Guidelines for the management of women with cervical cytological abnormalities. Jama. 2002 Apr 24;287(16):2120–2129. doi: 10.1001/jama.287.16.2120. [DOI] [PubMed] [Google Scholar]
- 35.Luu HN, Dahlstrom KR, Mullen PD, VonVille HM, Scheurer ME. Comparison of the accuracy of Hybrid Capture II and polymerase chain reaction in detecting clinically important cervical dysplasia: a systematic review and meta-analysis. Cancer medicine. 2013 Jun;2(3):367–390. doi: 10.1002/cam4.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.