

Abstract
Background:
Selective atrophy of hamstring components may result from muscle strain or graft harvesting for anterior cruciate ligament reconstruction. Assessment and rehabilitation that specifically targets medial (MH) or lateral (LH) hamstring components may improve patient outcomes. The purpose of this study was to evaluate effects of volitional tibial rotation medially (MR) versus laterally (LR) on activation levels of MH versus LH and strength measures during isometric testing of knee flexors.
Hypothesis:
Muscle activation of MH and LH during knee flexor strength testing will be augmented when coupled with MR and LR of the tibia, respectively, without affecting knee flexor strength measures.
Study Design:
Cross-sectional laboratory study.
Level of Evidence:
Level 3.
Methods:
Surface electrodes were used to record neuromuscular activity from MH and LH of the right lower limb in 40 healthy young men and women during isometric knee flexor strength testing at 40° of knee flexion, where participants maintained concurrent volitional MR or LR of the tibia. Statistical analyses of variance included general linear models for repeated measures.
Results:
A significant interaction was found for tibial rotation and hamstring component variables (P < 0.01). When isometric knee flexion was coupled with LR, normalized activation levels were similar for MH and LH. When performed with MR, a significant drop in LH activation led to dissimilar activation levels of the 2 components. Significantly greater strength measures were found when isometric knee flexion was performed with concurrent LR of the tibia (P < 0.01). Both sexes demonstrated the same rotation-dependent differences.
Conclusion:
Coupling tibial rotation with knee flexor activities primarily affects the LH component.
Clinical Relevance:
Strategies involving volitional tibial rotation may be considered for specific assessment/rehabilitation of the MH or LH component.
Keywords: knee, rotation, assessment, rehabilitation, electromyography
The hamstring muscle group collectively functions as a hip extensor and knee flexor and is frequently affected by injury in sports. The hamstrings are among the most frequently injured muscles of the lower extremity,9,15 and the lateral component—biceps femoris—is most commonly affected with respect to both primary muscle strain and reinjury.10 The medial component may also be compromised secondary to an anterior cruciate ligament (ACL) injury when a graft for ligament reconstruction is harvested from the ipsilateral semitendinosus and gracilis.14 The magnitude of their relative activation levels has been related to tibial rotation12,18 and frontal plane knee moments30,31 and discussed within the context of the multiplanar ACL injury mechanism.25
Imaging studies have demonstrated that the muscle/tendon structure and strength of hamstrings are affected by harvesting, although the extent varies between individuals.7,19,23,24,35 The long head of the biceps femoris35 and the semimembranosus11 may hypertrophy while the semitendinosus generally atrophies and demonstrates a proximal migration of the muscle-tendon junction.7,24,35 Altered firing patterns4,6 may explain seemingly selective, persistent muscle weakness of the medial knee flexors.1,2,7,32,36,37 Similarly, prolonged postinjury atrophy of the long head of the biceps femoris with compensatory hypertrophy of the short head34 and postinjury activation deficits of the biceps femoris accompanied by knee flexor weakness may persist in the injured limb.26
Although strength of knee flexors, collectively, is typically well monitored during any rehabilitation,8,21,38 medial hamstring (MH) versus lateral hamstring (LH) muscle activation is not routinely determined. Hamstring fatigue and semitendinosus inhibition have been identified as risk factors in ACL injury.40,42,43 Poor hamstring recovery may also be a contributing factor for the higher rerupture rate of semitendinosus grafts compared with the patellar tendon.28 Moreover, previous hamstring strain is a well-recognized risk factor for reinjury, which may reflect chronic muscle activation deficits or insufficient recovery after rehabilitation.5,8,13 Selective strength testing and rehabilitation that targets the injured component may positively affect recovery and lower the rate of reinjury. Previous studies have demonstrated that tibial rotation does affect relative activation of the MH and LH components18,22 but have not simultaneously controlled for strength output of the knee flexors.
The main purpose of this study was to evaluate the effect of volitional medial tibial rotation (MR) versus lateral tibial rotation (LR) on MH and LH muscle activation levels and on knee flexor strength measures. We hypothesized that MR would lead to greater relative activation of MH versus LH while the opposite would be seen when testing knee flexors coupled with LR. We further hypothesized that the magnitude of shift in medial and lateral activation levels would be similar for the 2 components and therefore not affect knee flexor strength measures.
Methods
Study Design and Subjects
The study protocol was approved by the National Bioethics Committee (VSNb2013100007/03.07) and registered with the National Data Protection Authority (S6556). All participants signed an informed consent form prior to data collection. All measurement sessions took place during a 3-week period at the university’s research center.
Twenty men and 20 women meeting inclusion criteria were recruited from the university community for this cross-sectional laboratory study and participated in a single measurement session. Sample size was determined based on the laboratory’s previous research using electromyographic (EMG) measures4,6 where observed power of 2 groups with 20 subjects each ranged from 0.7 to over 0.9 for 2- and 3-way interactions with alpha set at 0.05, also providing adequate power for analysis of strength data. Exclusion criteria consisted of history of knee surgery or any serious neuromusculoskeletal injury of the lower limbs; lesser injury (not leading to modification of activities) of the hamstring, gluteal, or back muscles in the 3 months prior to data collection; knee pain during the 3 previous months; and a body mass index (BMI) of greater than 35 kg/m2.
Data Collection and Processing
After a 5-minute warm-up on a stationary bicycle, isometric knee flexor strength of the right lower limb was tested using a dynamometer (KinCom) in the seated position. Wireless surface EMG (Kine Pro) was used to measure muscle activity of MH and LH during testing. The test was chosen as the setup is standardized and may also be used for rehabilitation purposes to augment hamstring strength.33,41 Preamplified surface electrodes were placed according to SENIAM guidelines,16 that is, midway between the ischial tuberosity and medial versus lateral epicondyle of the tibia for MH and LH, respectively. To further verify optimal placement, muscles were palpated and a visual assessment of the signal was performed prior to testing. A signal bandwidth of 16 to 500 Hz was used, sampling at 1600 Hz, according to manufacturer recommendations. The pelvis and distal thigh were secured to the dynamometer’s chair with straps and the shank to its lever arm, proximal to the malleoli. The axis of rotation was aligned with the lateral femoral epicondyle and the knee positioned in 40° of flexion to allow for rotational movement of the tibia while attaining a relatively comfortable hamstring muscle length for maximal performance (Figure 1). Submaximal isometric tests coupling the desired rotation with knee flexion were performed to familiarize participants with procedures and correct lower limb positioning during performance. In all, four 5-second maximal isometric contractions of knee flexors were then performed and recorded, 2 each with concurrent volitional MR and LR of the tibia, in random order, to favor MH versus LH contraction, respectively.18,22 The order of testing was determined by utilizing a webpage to randomly select either MR then LR, or vice versa. The stronger of 2 tests for each rotation was documented, as was the peak EMG signal during the measurement. All participants received standardized instructions during testing, encouraging them to bend their knee, gradually increasing force to maximal, while actively maintaining the desired maximal tibial rotation without shifting the thigh. The raw EMG data were high-pass filtered at 25 Hz, full wave rectified, and the root mean square of the signal was derived using a moving window of 250 ms according to the laboratory’s protocol.4,6 Maximum values of the smoothened data were then identified within each 5-second measurement and normalized to the maximum signal obtained after warm-up during a standard maximal voluntary isometric contraction obtained in a prone position at 25° of knee flexion with a neutral tibial position.
Figure 1.

Knee flexor strength test. Maximal isometric contraction with the knee positioned in 40° of flexion and maximal volitional lateral rotation of the tibia. Electrodes (not seen) over the medial and lateral hamstring components are connected to each of 2 electromyography recording units held by the participant.
Statistical Analyses
Data were analyzed using IBM SPSS Statistics version 20. A general linear model (GLM) for repeated measures was used to identify differences in normalized muscle activation levels during isometric knee flexor strength testing using muscle component (MH vs LH) and tibial rotation (MR vs LR) as within-subject factors, including sex as a between-group factor. A GLM was also used to identify differences in maximal force output (N) using tibial rotation (MR vs LR) as the within-subject factor and sex as a between-group factor to identify potential interaction between those factors or main effects. Differences between men and women with respect to demographic outcomes were analyzed using an independent Student t test. Additional calculations of normalized MH:LH muscle activation ratios were performed to allow for comparison between relevant published data. Alpha was set at 0.05 for statistical significance.
Results
A significant main effect of rotation was found for knee flexor strength measures as the overall mean force output was significantly greater when isometric knee flexion was coupled with concurrent volitional LR compared with MR across both sexes (P < 0.01) (Table 1). An expected main effect was also found due to greater mean (SD) strength measures of men versus women (P < 0.01).
Table 1.
Participants’ isometric knee flexor strength measures and relative medial (MH) and lateral (LH) muscle activation levelsa
| Men | Women | All | |
|---|---|---|---|
| Age, y | 24.5 (2.8) | 23.7 (2.3) | 24.1 (2.6) |
| Body mass index, kg/m2 | 24.8 (2.8)b | 22.3 (2.4) | 23.5 (2.9) |
| Knee flexor strength with MR, N | 426.3 (90.1)b | 271.9 (86.0) | 349.1 (116.9) |
| Knee flexor strength with LR, N | 456.1 (91.7)b | 305.3 (80.0) | 380.7 (114.2)c |
| MH:LH activation ratio with MR | 1.46 (0.63) | 1.82 (1.06) | 1.64 (0.88)d |
| MH:LH activation ratio with LR | 1.01 (0.31) | 1.02 (0.32) | 1.01 (0.31) |
LH, lateral hamstring; LR, lateral rotation of the tibia; MH, medial hamstring; MR, medial rotation of the tibia.
Data presented as mean (SD). Isometric strength measured at 40° of flexion.
Significantly greater mean value for men than women (P < 0.01).
Significantly greater mean strength value compared with that measured in MR (P < 0.01).
Significantly greater value for MH:LH ratio with tibia in MR than in LR (P < 0.01).
A significant interaction (muscle component by tibial rotation) was found for normalized EMG data obtained during isometric strength testing across both sexes (P < 0.01). On average, muscle activation levels of LH were significantly greater when isometric knee flexion was coupled with volitional LR than with MR (P < 0.01), while levels of MH activation were only slightly greater when isometric knee flexion was coupled with MR compared with LR (P = 0.085) (Figure 2). This led to shifts in relative MH:LH activation and a significant rotation-dependent difference in the calculated ratio (P < 0.01) (Table 1).
Figure 2.
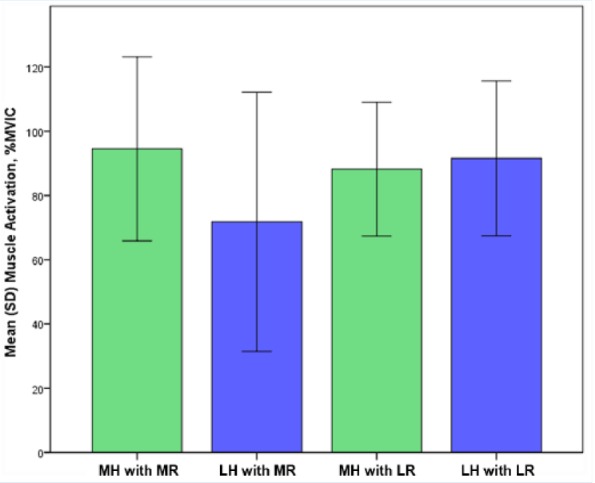
Muscle activation levels of medial (MH) and lateral (LH) hamstrings during knee flexor testing with concurrent medial (MR) and lateral (LR) rotation of the tibia, normalized to a maximal voluntary isometric contraction (MVIC). Statistically significant interaction (muscle component by rotation, P < 0.01).
Discussion
Isometric knee flexor testing coupled with volitional MR versus LR of the tibia significantly affected relative MH and LH muscle activation levels (Figure 2) as well as knee flexor strength measures (Table 1). This was due to a large extent to changes in LH activation. On average, knee flexor strength measures were 9.1% greater when flexion was coupled with tibial LR than with MR, thus reflecting significantly greater activation levels of LH while MH was largely unaffected by tibial rotation.
Mohamed et al22 measured the effects of maintaining MR versus LR of the tibia on muscle activation levels of all 4 hamstring components during maximal isometric knee flexor activities in healthy young adults. Their results with respect to relative changes in MH and LH activation levels were in agreement with those found in the present study, although there were some methodological differences. They presented no strength outcomes as manual resistance was applied to the knee flexors with the hip in neutral and 70° of knee flexion and thus were arguably testing the knee flexors in a shortened position with suboptimal standardization. Similar changes in synergy between MH and LH during dynamic exercises with MR versus LR tibial rotation were also found by Lynn and Costigan,18 although only MH:LH ratios, not muscle-specific changes in activation levels, were presented, and there were no strength values provided. Despite differences in normalization procedures and exercises performed (submaximal, dynamic tasks), both studies demonstrated significant changes in the MH:LH ratio by altering tibial rotation. Importantly, the present study reveals that this change was mainly due to the effects rotation had on activation of the LH component and that this was accompanied by significant changes in knee flexor strength output. Although statistically significant, the clinical significance of the mean difference in strength measures may be questioned. On average, flexion with MR produced 91.7% of the force seen with LR, and this may be considered an important difference depending on postinjury activities pursued by the individual.38 The results do demonstrate that in a clinical situation when testing knee flexor strength, it is important to standardize tibial rotation. If the uninjured side is tested with IR and the injured limb with ER, strength deficits might be missed.
As noted earlier, the semitendinosus and gracilis may be negatively affected by harvesting for ACL reconstruction (ACLR) as demonstrated by changes in morphology and strength.2,19,20,24 Rotating the tibia medially during select hamstring exercises as part of a comprehensive rehabilitation program lowers LH and thereby augments relative MH contribution for a set load. This approach may be more successful in preventing semitendinosus inhibition and atrophy than nonspecific hamstring rehabilitation after ACLR. Similarly, it may be feasible to decrease or increase activation levels of LH during rehabilitation after a biceps femoris muscle strain while considering both concentric and eccentric contractions specifically during training.26 Particular exercises activate MH versus LH components in different ways,18,43 and fatigue may affect them differently.39
A 15-fold greater risk of a second noncontact ACL injury (in either limb) during the first year after surgery has been reported in comparison with primary injury risk of noninjured athletes.27 In efforts to decrease risk of graft failure, postoperative rehabilitation increasingly focuses on resolving neuromuscular deficits that often persist after ACLR and standard rehabilitation.17 Patients may use compensatory mechanisms, such as tibial rotation, to alter demands on an injured MH or LH component, and the results demonstrated that this not only alters relative activation levels but also influences general knee flexor function, as strength measures were also affected. Patients may compensate after injury by using MR to lessen pain after biceps femoris strain or by using LR after MH injury or ACLR. Therefore, targeting each hamstring component may be indicated for some patient populations.
Limitations to the present study include limited external validity due to a homogenous group of participants. The magnitude of tibial rotation was not standardized as natural anatomic variation is to be expected between individual participants. No testing was performed in the neutral position due to fatigue considerations resulting from repeated maximal outputs. Previous studies have shown that normalized muscle activation levels or relative activation levels in the neutral position generally lie between values obtained with IR and ER.18,22
Conclusion
MR and LR of the tibia specifically favored MH and LH activation, respectively, thereby altering the relative activation ratio of the 2 components in healthy young adults. The degree of change in activation levels was more notable in the LH component and clearly had an impact on knee flexor strength.

Acknowledgments
The authors would like to acknowledge the assistance of Dr Thorarinn Sveinsson in processing and analysis of EMG data.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Ahlen M, Liden M, Bovaller A, Sernert N, Kartus J. Bilateral magnetic resonance imaging and functional assessment of the semitendinosus and gracilis tendons a minimum of 6 years after ipsilateral harvest for anterior cruciate ligament reconstruction. Am J Sports Med. 2012;40:1735-1741. [DOI] [PubMed] [Google Scholar]
- 2. Armour T, Forwell L, Litchfield R, Kirkley A, Amendola N, Fowler PJ. Isokinetic evaluation of internal/external tibial rotation strength after the use of hamstring tendons for anterior cruciate ligament reconstruction. Am J Sports Med. 2004;32:1639-1643. [DOI] [PubMed] [Google Scholar]
- 3. Arnason A, Andersen TE, Holme I, Engebretsen L, Bahr R. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports. 2008;18:40-48. [DOI] [PubMed] [Google Scholar]
- 4. Arnason SM, Birnir B, Gudmundsson TE, Gudnason G, Briem K. Medial hamstring muscle activation patterns are affected 1-6 years after ACL reconstruction using hamstring autograft. Knee Surg Sports Traumatol Arthrosc. 2014;22:1024-1029. [DOI] [PubMed] [Google Scholar]
- 5. Bourne MN, Opar DA, Williams MD, Al Najjar A, Shield AJ. Muscle activation patterns in the Nordic hamstring exercise: impact of prior strain injury [published online June 9, 2015]. Scand J Med Sci Sports. doi: 10.1111/sms.12494. [DOI] [PubMed] [Google Scholar]
- 6. Briem K, Ragnarsdóttir AM, Arnason SI, Sveinsson T. Altered medial versus lateral hamstring muscle activity during hop testing in female athletes 1-6 years after anterior cruciate ligament reconstruction [published online September 24, 2014]. Knee Surg Sports Traumatol Arthrosc. doi: 10.1007/s00167-014-3333-6. [DOI] [PubMed] [Google Scholar]
- 7. Choi JY, Ha JK, Kim YW, Shim JC, Yang SJ, Kim JG. Relationships among tendon regeneration on MRI, flexor strength, and functional performance after anterior cruciate ligament reconstruction with hamstring autograft. Am J Sports Med. 2012;40:152-162. [DOI] [PubMed] [Google Scholar]
- 8. De Vos RJ, Reurink G, Goudswaard GJ, Moen MH, Weir A, Tol JL. Clinical findings just after return to play predict hamstring re-injury, but baseline MRI findings do not. Br J Sports Med. 2014;48:1377-1384. [DOI] [PubMed] [Google Scholar]
- 9. Ekstrand J, Hagglund M, Walden M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med. 2011;39:1226-1232. [DOI] [PubMed] [Google Scholar]
- 10. Ekstrand J, Healy JC, Walden M, Lee JC, English B, Hagglund M. Hamstring muscle injuries in professional football: the correlation of MRI findings with return to play. Br J Sports Med. 2012;46:112-117. [DOI] [PubMed] [Google Scholar]
- 11. Eriksson K, Hamberg P, Jansson E, Larsson H, Shalabi A, Wredmark T. Semitendinosus muscle in anterior cruciate ligament surgery: morphology and function. Arthroscopy. 2001;17:808-817. [DOI] [PubMed] [Google Scholar]
- 12. Fiebert IM, Spielholz NI, Applegate EB, et al. Comparison of EMG activity of medial and lateral hamstrings during isometric contractions at various cuff weight loads. Knee. 2001;8:145-150. [DOI] [PubMed] [Google Scholar]
- 13. Fyfe JJ, Opar DA, Williams MD, Shield AJ. The role of neuromuscular inhibition in hamstring strain injury recurrence. J Electromyogr Kinesiol. 2013;23:523-530. [DOI] [PubMed] [Google Scholar]
- 14. Granan LP, Bahr R, Lie SA, Engebretsen L. Timing of anterior cruciate ligament reconstructive surgery and risk of cartilage lesions and meniscal tears: a cohort study based on the Norwegian National Knee Ligament Registry. Am J Sports Med. 2009;37:955-961. [DOI] [PubMed] [Google Scholar]
- 15. Hagglund M, Walden M, Ekstrand J. Risk factors for lower extremity muscle injury in professional soccer: the UEFA Injury Study. Am J Sports Med. 2013;41:327-335. [DOI] [PubMed] [Google Scholar]
- 16. Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. 2000;10:361-374. [DOI] [PubMed] [Google Scholar]
- 17. Hewett TE, Di Stasi SL, Myer GD. Current concepts for injury prevention in athletes after anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41:216-224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Lynn SK, Costigan PA. Changes in the medial-lateral hamstring activation ratio with foot rotation during lower limb exercise. J Electromyogr Kinesiol. 2009;19:e197-e205. [DOI] [PubMed] [Google Scholar]
- 19. Macleod TD, Snyder-Mackler L, Axe MJ, Buchanan TS. Early regeneration determines long-term graft site morphology and function after reconstruction of the anterior cruciate ligament with semitendinosus-gracilis autograft: a case series. Int J Sports Phys Ther. 2013;8:256-268. [PMC free article] [PubMed] [Google Scholar]
- 20. Makihara Y, Nishino A, Fukubayashi T, Kanamori A. Decrease of knee flexion torque in patients with ACL reconstruction: combined analysis of the architecture and function of the knee flexor muscles. Knee Surg Sports Traumatol Arthrosc. 2006;14:310-317. [DOI] [PubMed] [Google Scholar]
- 21. Mendiguchia J, Brughelli M. A return-to-sport algorithm for acute hamstring injuries. Phys Ther Sport. 2011;12:2-14. [DOI] [PubMed] [Google Scholar]
- 22. Mohamed O, Perry J, Hislop H. Synergy of medial and lateral hamstrings at three positions of tibial rotation during maximum isometric knee flexion. Knee. 2003;10:277-281. [DOI] [PubMed] [Google Scholar]
- 23. Nikolaou VS, Efstathopoulos N, Wredmark T. Hamstring tendons regeneration after ACL reconstruction: an overview. Knee Surg Sports Traumatol Arthrosc. 2007;15:153-160. [DOI] [PubMed] [Google Scholar]
- 24. Nomura Y, Kuramochi R, Fukubayashi T. Evaluation of hamstring muscle strength and morphology after anterior cruciate ligament reconstruction. Scand J Med Sci Sports. 2015;25:301-307. [DOI] [PubMed] [Google Scholar]
- 25. Opar DA, Serpell BG. Is there a potential relationship between prior hamstring strain injury and increased risk for future anterior cruciate ligament injury? Arch Phys Med Rehabil. 2014;95:401-405. [DOI] [PubMed] [Google Scholar]
- 26. Opar DA, Williams MD, Timmins RG, Dear NM, Shield AJ. Knee flexor strength and bicep femoris electromyographical activity is lower in previously strained hamstrings. J Electromyogr Kinesiol. 2013;23:696-703. [DOI] [PubMed] [Google Scholar]
- 27. Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of contralateral and ipsilateral anterior cruciate ligament (ACL) injury after primary ACL reconstruction and return to sport. Clin J Sport Med. 2012;22:116-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Persson A, Fjeldsgaard K, Gjertsen JE, et al. Increased risk of revision with hamstring tendon grafts compared with patellar tendon grafts after anterior cruciate ligament reconstruction: a study of 12,643 patients from the Norwegian Cruciate Ligament Registry, 2004-2012. Am J Sports Med. 2014;42:285-291. [DOI] [PubMed] [Google Scholar]
- 29. Petersen J, Thorborg K, Nielsen MB, Budtz-Jørgensen E, Hölmich P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39:2296-2303. [DOI] [PubMed] [Google Scholar]
- 30. Ramsey DK, Briem K, Axe MJ, Snyder-Mackler L. A mechanical theory for the effectiveness of bracing for medial compartment osteoarthritis of the knee. J Bone Joint Surg Am. 2007;89:2398-2407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Ramsey DK, Snyder-Mackler L, Lewek M, Newcomb W, Rudolph KS. Effect of anatomic realignment on muscle function during gait in patients with medial compartment knee osteoarthritis. Arthritis Rheum. 2007;57:389-397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Segawa H, Omori G, Koga Y, Kameo T, Iida S, Tanaka M. Rotational muscle strength of the limb after anterior cruciate ligament reconstruction using semitendinosus and gracilis tendon. Arthroscopy. 2002;18:177-182. [DOI] [PubMed] [Google Scholar]
- 33. Sekir U, Gur H, Akova B. Early versus late start of isokinetic hamstring-strengthening exercise after anterior cruciate ligament reconstruction with patellar tendon graft. Am J Sports Med. 2010;38:492-500. [DOI] [PubMed] [Google Scholar]
- 34. Silder A, Heiderscheit BC, Thelen DG, Enright T, Tuite MJ. MR observations of long-term musculotendon remodeling following a hamstring strain injury. Skeletal Radiol. 2008;37:1101-1109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Snow BJ, Wilcox JJ, Burks RT, Greis PE. Evaluation of muscle size and fatty infiltration with MRI nine to eleven years following hamstring harvest for ACL reconstruction. J Bone Joint Surg Am. 2012;94:1274-1282. [DOI] [PubMed] [Google Scholar]
- 36. Tadokoro K, Matsui N, Yagi M, Kuroda R, Kurosaka M, Yoshiya S. Evaluation of hamstring strength and tendon regrowth after harvesting for anterior cruciate ligament reconstruction. Am J Sports Med. 2004;32:1644-1650. [DOI] [PubMed] [Google Scholar]
- 37. Tashiro T, Kurosawa H, Kawakami A, Hikita A, Fukui N. Influence of medial hamstring tendon harvest on knee flexor strength after anterior cruciate ligament reconstruction. A detailed evaluation with comparison of single- and double-tendon harvest. Am J Sports Med. 2003;31:522-529. [DOI] [PubMed] [Google Scholar]
- 38. Thomee R, Kaplan Y, Kvist J, et al. Muscle strength and hop performance criteria prior to return to sports after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2011;19:1798-1805. [DOI] [PubMed] [Google Scholar]
- 39. Timmins RG, Opar DA, Williams MD, Schache AG, Dear NM, Shield AJ. Reduced biceps femoris myoelectrical activity influences eccentric knee flexor weakness after repeat sprint running. Scand J Med Sci Sports. 2014;24:e299-e305. [DOI] [PubMed] [Google Scholar]
- 40. Weinhandl JT, Earl-Boehm JE, Ebersole KT, Huddleston WE, Armstrong BS, O’Connor KM. Reduced hamstring strength increases anterior cruciate ligament loading during anticipated sidestep cutting. Clin Biomech (Bristol, Avon). 2014;29:752-759. [DOI] [PubMed] [Google Scholar]
- 41. White K, Di Stasi SL, Smith AH, Snyder-Mackler L. Anterior cruciate ligament- specialized post-operative return-to-sports (ACL-SPORTS) training: a randomized control trial. BMC Musculoskel Disord. 2013;14:108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Zebis MK, Bencke J, Andersen LL, et al. Acute fatigue impairs neuromuscular activity of anterior cruciate ligament-agonist muscles in female team handball players. Scand J Med Sci Sports. 2011;21:833-840. [DOI] [PubMed] [Google Scholar]
- 43. Zebis MK, Skotte J, Andersen CH, et al. Kettlebell swing targets semitendinosus and supine leg curl targets biceps femoris: an EMG study with rehabilitation implications. Br J Sports Med. 2013;47:1192-1198. [DOI] [PubMed] [Google Scholar]