

Abstract
Introduction:
The nutritional profile of the Brazilian population has changed in recent years. Therefore, this study aimed to assess the prevalence of nutritional status among Brazilian school adolescents during the period from January 2014 to December 2014.
Methods:
This study employed an observational design with a cohort of school adolescents. Anthropometric measurement was assessed by nutritionists in government schools. The cut-off points for body mass index according to Brazilian criteria for adolescents of both sexes between 10 years and 19 years old were underweight (≤17.5 kg/m2), overweigh (≥25.0 kg/m2), and obesity (≥30.0 kg/m2).
Results:
The number of students included in the analysis was 2162, of which 71.0% were males and 29% were females (P = 0.00001). The mean age (years) was 13.14 ± 2.17 for boys and 12.66 ± 1.85 for girls (P = 0.0001). The prevalence of underweight, overweight, and obesity observed in our population of school adolescents according to the Brazilian criteria was 2.8%, 8.1%, and 2.4% for males, respectively, and 23.0%, 10.7%, and 3.6% for females, respectively. For both sexes, there was no statistically significant difference between overweight (P = 0.5469) and obesity (P = 0.7863), but there was for underweight (P = 0.001).
Conclusions:
The occurrence of excess weight among Brazilian school adolescents is similar to the international prevalence, but the prevalence of underweight was very high among girls. The nutritional status of adolescents must be considered a public health problem in Brazil.
Keywords: Adolescent, nutrition, nutritional status, obesity
INTRODUCTION
The nutritional profile of the Brazilian population has changed in recent years.[1] Overweight and obesity are present among all age groups.[1,2] Controlling overweight and obesity in adolescence is a challenge for physicians and nutritionists. Eating habits in this age group are characterized by a preference for fast foods with a high fat and carbohydrate composition, with an increased rate of calories and low nutritional value. The food preferences of adolescents can lead to obesity and overweight when combined with a sedentary lifestyle represented by long time periods dispensed to low-intensity physical activities, such as watching television and using the computer. Most Brazilian adolescents are students and are also fed in their schools. Therefore, responsible nutritional habits should also be incorporated in official guidelines for school nutrition.[3,4,5]
Nutritional assessment can determine the nutritional status. Nutritional status is the result of a balance between nutrient intake and nutrient loss.[6] The nutritional status of a population is an indicator of its quality of life. The assessment of nutritional status is an important step in evaluating a child. Here, the nutritionist or pediatrician makes a diagnosis if growth is moving away from the standard expected of disease and/or unfavorable social conditions. The main objective of the nutritional assessment is to determine the growth and body proportions in an individual or community. As a consequence, the secondary objective is to establish interventions. Hence, that more individuals are assessed from a nutritional point of view. Earlier interventions may be imposed by improving the quality of life of the population in general. There is no way to reduce malnutrition and obesity if they are not diagnosed correctly.[7,8,9,10]
Currently, anthropometry is still the best method to evaluate nutritional status.[11] Body mass index (BMI) or Quetelet index has been established as an important diagnostic method for nutritional profile assessment in several populations. The importance of BMI has been recognized by the World Health Organization (WHO).[11]
What is already known about this topic? First, childhood obesity is difficult to conceptualize; and second, there is not an international consensus on the best anthropometric criteria to be used for the evaluation of overweight and obesity in adolescents.[12,13] Therefore, this study aimed to evaluate the prevalence rate of underweight, overweight, and obesity among Brazilian school adolescents using the cut-off points for BMI according to Brazilian reference during the period between January 2014 and December 2014.
METHODS
To prevent errors in this epidemiologic study, we applied the methodological criteria recommended by the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.[14]
Study design and sample size
This epidemiological design was an observational, descriptive, cross-sectional and population-based study with a cohort of school adolescents. All evaluations were performed by graduate nutritionists. The sample consisted of 2162 school adolescents enrolled in all 20 government schools during the period from January 2014 to December 2014. A chief responsible for the institution signed a consent form to analyze the database. All ethical procedures were followed.
Assessment of anthropometric measurements body weight and height were assessed by nutritionists in schools, according to rules established by the Brazilian Institute of Geography and Statistics Manual.[15] The height was measured using a tape attached to the wall. Students were placed against the wall, barefoot, with the heels touching the wall, and the value was recorded in centimeters with one decimal place. Body weight was measured using a portable scale, with resolution up to 500 g. The students wore light clothes and were barefoot. The value was reported in kilograms to one decimal place, and BMI was calculated as the ratio between body weight (kilograms) and the square of height (m).
Inclusion and exclusion criteria
In this research, as reference values for BMI in Brazilian adolescents, we used the cut-off point recommended by Conde and Monteiro for anthropometric measurements in the Brazilian population.[16] The age limits of adolescence are 10 years old and 19 years old according to the WHO.[17] The exclusion criteria included some conditions present in the medical reports of adolescents, such as thyroid, renal, and liver diseases, use of oral corticosteroids, anabolic steroids, and beta-blockers. Other exclusion criteria were adolescents who refused to participate in the study, student younger than 10 years and older than 19 years, pregnancy, and adolescents with special needs.[18]
Cut-off values for body mass index
The cut-off points for BMI according to Conde and Monteiro (Brazilian criteria) for students of both sexes between 10 years old and 19 years old were as follows: Underweight (BMI ≤17.5 kg/m2), overweight (BMI ≥25.0 kg/m2), and obesity (BMI ≥ 30.0 kg/m2).[16]
Statistical analysis
We defined period prevalence as the number of school adolescents with underweight, overweight, and obesity, divided by the total number of school adolescents in the sample. The period spanned January 2014 to December 2014. The anthropometric evaluations were entered into Microsoft Office Excel 2010® and exported from the database to the following software programs: GraphPad Prism, version 2015 (GraphPad Software, Inc. San Diego, California, USA); NCSS10 software, version 2015 (NCSS, LLC, Kaysville, Utah, USA); WHO AnthroPlus software, version 3.2.2 (Freely distributed and copied by WHO, Geneva, Switzerland) to determine BMI; and EpiTools epidemiological calculators, (copyright 2015 by AusVet Animal Health Services).[19] The data were analyzed using univariate analysis. The following statistical tests were performed: (1) Central limit theorem, in which very large sample size had a normal distribution. The general rule of greater or equal to 30 observations was applied. (2) Continuous data are reported as the arithmetic mean ± standard deviation. Categorical data are reported as percentages of the total population. (3) Student's t-test was used with the aim of comparing differences in the arithmetic means of the normally distributed continuous variables. (4) The Z-test was used to compare proportions for categorical variables. (5) The Chi-square test with a trend line was used for associations among obesity and age in a contingency table, with two columns and ten rows for both sexes. (6) P < 0.05 (two-tailed) was considered to be statistically significant and sufficient enough to reject the null hypothesis and define a type I error.
RESULTS
The number of students included in the analysis was 2162, of which 1527 were males (71.0%) and 635 were females (29.0%), with a Z = 18.0 (P = 0.00001). The arithmetic mean of age (in years) was 13.14 ± 2.17 for males and 12.66 ± 1.85 for females, with an unpaired t-test equal to 4.74 (P = 0.0001). The coefficient of variation (CV) for the age of the students was 16.52% and 14.65%, respectively. This value for age signified that the sample was homogeneous (CV ≤20%).
The anthropometric characteristics of all school adolescents of both sexes are shown in Table 1. The height (cm), body mass (kg), and BMI (kg/m2) for males were 1.60 ± 0.14, 52.0 ± 15.0, and 20.0 ± 4.0, respectively. The height (cm), body mass (kg), and BMI (kg/m2) for females were 1.50 ± 0.09, 50.0 ± 13.0, and 21.0 ± 4.6, respectively. When both sexes were compared for height, body mass, and BMI, the t values, were 7.57 (P = 0.0001), 2.47 (P = 0.0136), and 3.82 (P = 0.0001), respectively. The CV was higher than 20% for only BMI in males and females, with values between 20.02% and 22.36%, respectively.
Table 1.
Anthropometric characteristics of all school adolescents of both sexes (n=2162)

Table 2 shows a comparison of the BMI of underweight, overweight, and obesity in Brazilian school adolescents. According to Student's t-test, there was not a statistically significant difference between the arithmetic means in both sexes for underweight (P = 1.00) and obesity (P = 0.089). However, the comparison of overweight for both sexes was statistically significant (P = 0.044).
Table 2.
Body mass index of underweight, overweight, and obesity in Brazilian school adolescents of both sexes
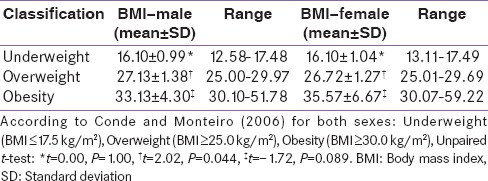
Table 3 shows the prevalence of nutritional status among the population studied using a Brazilian reference for adolescents. There was no statistically significant difference in both sexes for overweight (Z = 0.60, P = 0.5469) and obesity (Z = 0.30, P = 0.7863). However, the comparison of underweight for both sexes was statistically significant (Z = 7.80, P = 0.001).
Table 3.
Prevalence of nutritional status in Brazilian school adolescents in both sexes
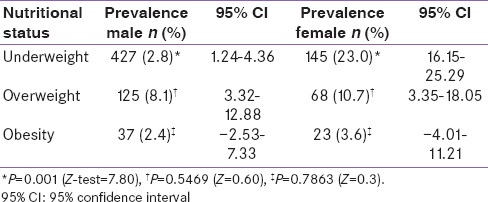
Figure 1 shows a histogram representing the prevalence rate distribution and association with obesity and age of the school adolescents (n = 60). The trend line shows an inverse relationship between obesity and age among the school adolescents of both sexes. The association with a Chi-square test for a linear trend was 30.95 (P = 0.01).
Figure 1.
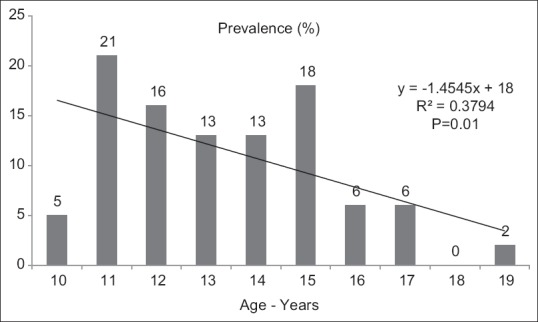
Histogram representing the prevalence distribution and association of obesity and age of the school adolescents (n = 60). The trend line shows an inverse relationship between obesity and age among the school adolescents for both sexes. Chi-square test for linear trend = 30.92 (P = 0.01)
DISCUSSION
Adolescence can be considered a transitional stage from puberty to adulthood. However, adolescence has stages of development according to different ages within this age range. Many authors have described such physical, intellectual, emotional, and social development.[12,13,16] Considering these different stages, the WHO mentioned many causes of illness and disability among adolescents, such as asthma and lower respiratory infections, use of alcohol, HIV/AIDS, anxiety, and depression, among others. Endocrine disorders were among ten top causes of death in adolescents in 2012.[17]
In high complexity centers for diagnosis, endocrine disorders are present in less than 1% of those with childhood obesity. Other secondary causes are less frequently observed.[13] Thus, the main cause of obesity in adolescents and other children is exogenous factors or increased caloric intake and decreased physical activity.[13] Adolescent obesity is a public health problem. It is associated with a variety of risk factors for type 2 diabetes, insulin resistance, metabolic syndrome, dyslipidemia, systemic arterial hypertension, and atherosclerosis.[12,18]
The BMI correlates with direct measures of total body fat.[20] The use of BMI is justified by its simplicity and low cost. There is consensus that BMI should be used in the collective assessment and perhaps individual for assessment of nutritional status in adolescents.[21] However, BMI does not always relate to central obesity. It cannot differentiate muscle mass and fat mass.[20]
The height and body mass for both the sexes among school adolescents in our study [Table 1] was in accordance with data from Brazilian Institute of Geography and Statistics. In a government report from 2008 to 2009, the median range of height among Brazilian adolescents was 1.39–1.72 m for males and 1.4 m to 1.61 for females. The median of body mass was reported with a range of 33.4–65.9 kg in males and a range of 34.3–56.2 kg for females.[15]
The Conde and Monteiro criteria[16] for the diagnosis of nutritional status by BMI in adolescents are shown in Table 2. However, these authors also agree that the adoption of the proposed cut-off point for underweight requires further analysis and discussion. However, the method used in Brazilian references was basically the same as that used in the calculation of the value of the international BMI standard.[12]
In this study, the prevalence rates of underweight, overweight, and obesity observed in our population of school adolescents according to the Brazilian BMI criteria were 2.8%, 8.1%, and 2.4% for males, respectively, and 23%, 10.7%, and 3.6% for females, respectively [Table 3]. The prevalence rates for both sexes were similar to those of other studies that used the Conde and Monteiro criteria.[22] Different from our results and those of other researchers, the prevalence of overweight and obesity was 14% and 23%, respectively, among girls in a district school in Bangladesh.[23]
The prevalence rate of excess weight (overweight and obesity) in our school adolescents was 10.5% for boys and 14.3% for girls. Krinski et al. found similar results with the national criteria in a sample of 3118 school adolescents in the northern region of Brazil, i.e., 11.6% and 14.6% prevalence of excess weight for boys and girls, respectively.[24] Other Brazilian studies showed different results concerning excess weight with Brazilian references. Flores et al. showed a prevalence rate of 27.6% for boys and 33.8% for girls.[25]
Our results in Figure 1 show a statistically significant inverse association between obesity prevalence and age in school adolescents. Other authors drew the same conclusion.[24]
The choice of the Brazilian reference for the calculation of prevalence rates of anthropometric status in adolescents can be compared to other international criteria.[22]
International references for comparisons of the prevalence rate are 5–18% for overweight and 0.1–4% for obesity at 2–18 years old.[12] The results of our study are in the international reference range as shown in Table 3. However, the prevalence rate of underweight in our population was very high among girls (23.0%) compared to boys (2.8%) and was statistically significant (P = 0.001), as shown in Table 3. An international study of the trends of obesity and underweight in many countries showed that the prevalence rate of underweight was 6.5% among girls in 1997 in Brazil.[26]
In 12 schools of Bhubaneswar, State of Odisha, India, the prevalence of overweight and obesity among adolescents in private schools was significantly higher (45.2%) than those in government schools (10.5%).[27]
CONCLUSIONS
In summary, what does this study add to this research field? What are the limitations? What are the implications? We recommend BMI as the best procedure for monitoring and diagnosing obesity in health campaigns. This study concludes that the occurrence of excess weight among our school adolescents was similar to the international prevalence. However, the prevalence rate of underweight in our population was very high among girls (23.0%). The results of the diagnosis of nutritional status of every adolescent were sent with knowledge of the parents. The current study cannot be extrapolated to the entire population of Brazilian adolescent students because this research was conducted with a specific population group. The nutritional status of adolescents must be considered to be a public health problem in Brazil.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We wish to acknowledge the support of all the students and teachers of the schools who participated in this research during the year 2014. The manuscript was edited for the proper English language, grammar, punctuation, spelling, and overall style by one or more of the highly qualified native English speaking editors at American Journal Experts. Certificate verification key: A3EF-A557-BF3C-2Ec2-962D. The authors thank two American native English speakers who reviewed this manuscript.
REFERENCES
- 1.Anjos LA. Diagnosis of obesity and determination of nutritional requirements: Challenges for the area of nutrition. Cien Saude Colet. 2013;18:295. doi: 10.1590/s1413-81232013000200001. [DOI] [PubMed] [Google Scholar]
- 2.Kranz S, Findeis JL, Shrestha SS. Use of the revised children's diet quality index to assess preschooler's diet quality, its sociodemographic predictors, and its association with body weight status. J Pediatr (Rio J) 2008;84:26–34. doi: 10.2223/JPED.1745. [DOI] [PubMed] [Google Scholar]
- 3.Assis CM, Qui VR, Rasseli JG, Cunha FG, Salaroli LB. Eating habits and nutritional status of the youth: A comparative study. Nutrire. 2009;34:13–27. [Google Scholar]
- 4.Hernades F, Valentini MP. Obesity: A concern each day more common for children and teenagers. Rev Educ Fisica UNICAMP. 2010;8:47–63. [Google Scholar]
- 5.Freitas CG, Santos RS, Carreiro DL, Coutinho LT, Martins AM, Coutinho WL. Factors associated with perception of healthy habits among adolescentes. Adolesc Saude. 2014;11:23–35. [Google Scholar]
- 6.Albano RD, Souza SB. Nutrient and energy intake in adolescents from a public school. J Pediatr (Rio J) 2001;77:512–6. doi: 10.2223/jped.359. [DOI] [PubMed] [Google Scholar]
- 7.Lukaski HC. Methods for the assessment of human body composition: Traditional and new. Am J Clin Nutr. 1987;46:537–56. doi: 10.1093/ajcn/46.4.537. [DOI] [PubMed] [Google Scholar]
- 8.De Mello ED. The meaning of nutritional status assessment. J Pediatr (Rio J) 2002;78:357–8. doi: 10.2223/jped.875. [DOI] [PubMed] [Google Scholar]
- 9.Sigulem DM, Devincenzi MU, Lessa AC. Diagnosis of child and adolescent nutritional status. J Pediatr (Rio J) 2000;76(Suppl 3):S275–84. doi: 10.2223/jped.164. [DOI] [PubMed] [Google Scholar]
- 10.Eisenstein E, Coelho KS, Coelho SC, Coelho MA. Nutrition in adolescence. J Pediatr (Rio J) 2000;76(Suppl 3):S263–74. doi: 10.2223/jped.163. [DOI] [PubMed] [Google Scholar]
- 11.Geneva: World Health Organization; [Last updated on 2015 Aug 13]. World Health Organization. The World Health Report 1995: Physical Status: The Use and Interpretation of Anthropometry. Available from: http://www.who.int/childgrowth/publications/physical_status/en/ [Google Scholar]
- 12.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ. 2000;320:1240–3. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Godoy-Matos AF, Guedes EP, Souza LL, Martins MF. Management of obesity in adolescents: State of art. Arq Bras Endocrinol Metabol. 2009;53:252–61. doi: 10.1590/s0004-27302009000200017. [DOI] [PubMed] [Google Scholar]
- 14.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. BMJ. 2007;335:806–8. doi: 10.1136/bmj.39335.541782.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rio de Janeiro: IBGE; 2010. Brazilian Institute of Geography and Statistics. Survey of family budgets 2008-2009: Anthropometry and nutritional status of children, adolescents, and adults in Brazil. [Google Scholar]
- 16.Conde WL, Monteiro CA. Body mass index cutoff points for evaluation of nutritional status in Brazilian children and adolescents. J Pediatr (Rio J) 2006;82:266–72. doi: 10.2223/JPED.1502. [DOI] [PubMed] [Google Scholar]
- 17.Geneva: WHO; 2015. World Health Organization. Adolescent Health Epidemiology. [Google Scholar]
- 18.Lima MC, Romaldini CC, Romaldini JH. Frequency of obesity and related risk factors among school children and adolescents in a low-income community. A cross-sectional study. Sao Paulo Med J. 2015;133:125–30. doi: 10.1590/1516-3180.2014.8960412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sergeant ES. Epitools Epidemiological Calculators. AusVet Animal Health Services and Australian Biosecurity Cooperative Research Centre for Emerging Infectious Disease. [Last updated on 2015 Sep 25]. Available from: http://www.epitools.ausvet.com.au .
- 20.Hall DM, Cole TJ. What use is the BMI? Arch Dis Child. 2006;91:283–6. doi: 10.1136/adc.2005.077339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gomes FS, Anjos LA, Vasconcellos MT. Anthropometry as a tool for assessing the nutritional status of adolescents. Rev Nutr Camp. 2010;23:591–605. [Google Scholar]
- 22.Barbosa RM, Soares EA, Lanzillotti HS. Nutritional status evaluation in schoolchildren according to three references. Rev Paul Pediatr. 2009;27:243–50. [Google Scholar]
- 23.Zabeen B, Tayyeb S, Naz F, Ahmed F, Rahman M, Nahar J, et al. Prevalence of obesity and central obesity among adolescent girls in a district school in Bangladesh. Indian J Endocrinol Metab. 2015;19:649–52. doi: 10.4103/2230-8210.163193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Krinski K, Elsangedy HM, Hora S, Rech CR, Legnani E, Santos BV, et al. Nutritional status and association of overweight with gender and age in children and adolescents. Rev Bras Cineantropom Desempenho Hum. 2011;13:29–35. [Google Scholar]
- 25.Flores LS, Gaya AR, Petersen RD, Gaya A. Trends of underweight, overweight, and obesity in Brazilian children and adolescents. J Pediatr (Rio J) 2013;89:456–61. doi: 10.1016/j.jped.2013.02.021. [DOI] [PubMed] [Google Scholar]
- 26.Wang Y, Monteiro C, Popkin BM. Trends of obesity and underweight in older children and adolescents in the United States, Brazil, China, and Russia. Am J Clin Nutr. 2002;75:971–7. doi: 10.1093/ajcn/75.6.971. [DOI] [PubMed] [Google Scholar]
- 27.Patnaik L, Pattanaik S, Sahu T, Rao EV. Overweight and obesity among adolescents, a comparative study between government and private schools. Indian Pediatr. 2015;52:779–81. doi: 10.1007/s13312-015-0716-9. [DOI] [PubMed] [Google Scholar]